#migraine pain treatment
Text
Migration nowadays is not an unknown thing, it is highly popular especially the teenage students due to high mental pressure. Sometimes the migration can stay up to four to five hours a day
Almost 50% of people are facing the same trouble all over the world.
Bad headaches are only one aspect of a migraine. This neurological condition may leave you bedridden for days due to excruciating throbbing pain. Movement, light, sound, and other triggers may result in symptoms including brief loss of vision, irritation, difficulty speaking, pain, nausea, and visual abnormalities.
#migraine pain treatment#migraine pain treatment in Sharjah#migraine pain treatment in King Faisal Road#migraine pain treatment in AbuShagara#migraine specialist#migraine specialist in Sharjah
0 notes
Text
I think if we try hard enough we could sexualize migraines
#like. my body is weak and my brain is slow and easily suggestable#the meds make me a little dizzy#i have to be naked because the texture of clothes is too much#curled up in bed in the dark only half conscious#itd be soooooo easy to take advantage of me#plus#yknow#orgasms are actually a really helpful treatment for migraines because of the flood of seratonin#similar to how triptan meds work#to make a long story short im home from work with a migraine and am both in pain and horny. clearly
64 notes
·
View notes
Text
Does Anyone out there happen to know chiropractic therapy, but like reallyy reallyyy poorly (moreso than usuall)) + is willing to just simplyy/entirelyy snap my neck/end my life, in a Singular, Swift motion, Once & for All ??!
#bc am sooo tireddd of these migraines/neck/spinal pain ((yesss i knoww that effective treatment ((mostlyy administered via injection exists.#but Shushhhh..))))
11 notes
·
View notes
Text
finally tried hydrocodone for my back pain and THIS is the ~big scary opioids~ they've been talking about?! i know they're still ykno, serious medication but. i. feel. fine! i even took my other medication todayy!? i'd be angry but im honestly just. WHAT. i'm not in pain! yall coulda gave me this YEARS ago but you just didnt! i shouldnt have had to have figured this out all on my own especially with how it coulda easily gone sideways if i didnt have some awareness of what im doing?? fuckkk the war on drugs man. fuck it. shit.
edit: to be clear no i am not prescribed this i found some in the house it aint mine
#in terms of euphoria and anxiolysis this is equivalent to the barbiturate i got prescribed for migraines. which.#granted i drained the bottle in a few days but#STILL.#i feel like i deserve to choose between severe ending pain that makes me near housebound and stuck in this recliner all day#and potential addiction#like i feel like i should have that choice#especially since they're coming out with more treatments and safety measures for opioid addiction#ALSO especially because denying me adequate pain management is leading me to abuse other shit in ways that have nearly Killed Me#fuck the medical system so hard#fuck#julian rants#opioids tw#drugs tw
37 notes
·
View notes
Text
hate hate hate when people tell me how to deal with my own symptoms that i have had for literal years
like yeah maybe some fresh air right this moment would do me some good but have you considered that the light would be excruciatingly painful for my eyes and the cold would hurt my joints and i'd be just swapping one pain for another
please for the love of god i am begging to be trusted to handle myself. unless i ask for help or advice explicitly i. i do not want it. thank you very much.
#chronic pain#chronic illness#chronically ill#chronic fatigue#migraine#joint pain#brain fog#idk#disability#it's really frustrating#pretty sure my dad is giving me the silent treatment rn#like i get that you might think that i'm doing more harm than good but like#can you try and please trust me for once#sigh
27 notes
·
View notes
Text
WAITLIST APPOINTMENT WENT THRU I SEE THE RHEUMATOLOGIST ON MONDAY. MAYBE WE ARE NOT IN HELL AFTER ALL.
#FIVE WEEKS EARLIER THAN I WAS SUPPOSED TO#it's a different provider who's less versed in My Specific Shit#(the rheum i was seeing in september is specifically an expert in my rare-ass diseases)#but he has Excellent reviews and can easily refer my case back to the specialist rheum if he feels it's outside his purview.#in the meantime. FUCKING PREDNISONE AND/OR HYDROXYCHLOROQUINE IT'S WITHIN REACH#IN LESS THAN 72 HOURS HOPEFULLY MY MIGRAINE CHEST PAIN WHEEZING STOMACH ISSUES AND SKIN ULCERS WILL ALLLLL GO AWAAAAYYYY#please god. please god sir be so nice to me and give me treatment. please#autoimmune tag
22 notes
·
View notes
Text
idk I just want to scream at my doctor really bad. she's done nothing but cost me thousands of dollars and I'm worse off than when I started going to her. why should I be nice yk
#'you need to completely quit pain medication!!' what am i supposed to do instead?? i have treatment resistant headaches and migraines#and have since i was TEN that gave me suicidal depression#you want me to take absolutely fucking nothing? you want me to become a danger to others on the road because i can't see??#if she offered any fucking alternative--and ive asked her dozens of times what the fuck she expects me to do--#i would try#but she doesnt#atp i would rather save my money and just kill myself from otc pain meds instead. who cares#says kenna
2 notes
·
View notes
Text
Well I'm on day four of a migraine and took myself to medcheck. Sitting here in the waiting room anxious they're going to think I'm a drug seeker because I have a pain issue even though I KNOW opioids don't help migraines (typically) and don't want them.
#i have this deep phobia that I'm going to get 'drug seeker' in my permanent file or something#and then get cancer or whatever and jot be able to get pain treatment#i know it's not rational but it's so deep seated I've put up with a migraine for four days so#but like there's part of me CONVINCED there is a finite amout of pain treatment I will be permitted in my life#and I have to be careful not to waste it on trivial things
9 notes
·
View notes
Text
In my feelings...
[Video description: a TikTok by and of the user @/hannah.mae.sutherland. They're a feminine presenting person with long brown hair, light skin and green eyes, sitting in front of the camera in a red hoodie. As they are looking off to the right, a female voice says "Okay, why did you run away?". A line of white text in the middle of the frame reads "wait so you're going to be sick forever?". The next words spoken by the voice over are also being mouthed by the user themselves. They say "Can we not talk about that?" as the person starts tearing up. The video ends with them covering their face with one hand while turning their head away from the camera. In the background, you can also hear soft instrumental music. /VD end]
#chronically ill#chronic illness#disability#disabled#spoonie#lgbtq+#iih#ehlers danlos#diabetes#epilepsy#pots#hypermobility#recovery#mental illness#mentally ill#treatment resistant depression#chronic pain#migraines#rant#vent#cw negative#idiopathic intracranial hypertension#🦓
10 notes
·
View notes
Text
Knowing about migraine disorder can be intimidating. According to researchers and professional doctors, the reason of migraine pain is still a mystery and no one has achieved it’s genuine causes.
The exact cause of migraines is unknown, but they’re thought to be the result of abnormal brain activity temporarily affecting nerve signals, chemicals and blood vessels in the brain.
0 notes
Note
I’m so sorry to hear about your chronic migraines! You might mention to your doctors [if you think it would help at all] that you have a friend who was telling you about the white matter lesions she has in various parts of her brain from chronic, severe migraines. White matter indicates actual brain damage and it’s not something I can heal from. I’m still bitter about how I was treated by the medical community. I pray you eventually find someone who can help you and who’ll really listen. 💙
Hey! Thank you so much for the advice! I've had MRIs and CTs done and I never heard that those were seen (they also weren't looking for those as far as I know, and the medical system can't look past the end of its nose lol) but yeah it's definitely something to look into. And I hope the same to you! I'm glad there's a community out here, it makes it feel much less lonely <3
#chronic migraine#migraine#chronically ill#chronic illness#chronic pain#medical conditions#medical treatment#recovery#pain management#pain treatment#american healthcare
5 notes
·
View notes
Text
Migraine isn’t a Headache Part Six: make it stop
We looked at medication and treatment for acute attacks of migraines. Things that you can do to treat the pain when you're having it.
This is also probably the first line of help you'll get from a GP or pharmacist or whoever you approach for help.
Some people have success with acute treatments. Maybe the migraine was a one-off, or is a rare occurrence, maybe it was just really responsive to acute meds.
Some people have migraines that don't respond to acute meds, or don't respond well enough to be considered effective treatment.
When you get to this stage, you need to start looking at stopping the migraines before they start, instead of constantly taking acute meds that a) don't work and b) can cause rebound headaches and other problems.
It sucks, because you want to reach for the painkillers when you have pain, but doing so is not sustainable.
Getting into preventative meds ties in a lot with how you go about getting a diagnosis, but I'm going to try to speak about the meds and complimentary treatments AROUND being under a neurologist. On that note, GPs are rarely going to work with you on preventative meds.
There are a few they can prescribe, but you'll probably get better treatment under a neurologist or headache specialist. Sorry.
GPs are useless.
Sorry, bit of my bias there, but I don't use GP's unless I need a referral or quick acute treatment, and EVEN THEN.
It's worth noting as well that you'll usually only get to this stage if your migraines have become chronic, that is:
for over 3 months
you've had 15 headache days a month minimum
of which 8 have migraine features
Some of the treatments aren't indicated for episodic migraines.
((As previously mentioned, this definition might be changing to take into account the impact migraines are having on your life, and not a somewhat arbitrary number; fingers crossed this happens soon))
My list of attempted treatments includes:
amitriptyline (this is one the GP might prescribe for you) (also prescribed for abdominal discomfort and major depressive disorder, although it's fallen out of favour due to increased risk of fatality in overdose)
propranalol (and this) - beta blocker
flunarizine (calcium channel blocker, used to treat high blood pressure and certain heart conditions)
lamotrigine (usually prescribed for epilepsy and bipolar disorder)
topiramate (usually prescribed for seizures)
candesartan (usually prescribed for hypertension)
pregabalin (usually prescribed for seizures and anxiety)
gabapentin (usually prescribed as an anticonvulsant and for nerve pain)
Botox injections
greater occipital nerve blocks
Magnesium/CoenzymeQ10/Vitamin B trio
Aimovig (erenumab, CGRP injection, one of the first migraine-only treatments)
Ajovy (fremanezumab, another CGRP injection, one of the first migraine-only treatments)
sTMS machine (single pulse transcranial magnetic stimulation)
Vyepti (eptinezumab-jjmr IV infusion, another CGRP drug)
I don't think I've had EVERY drug available for migraine prophylaxis, but judging by the increasingly surrendering tone of the letters from my neurologist, I'm just about there.
As you can see, apart from the last CGRP drugs, almost every drug listed is used off licence for migraines, and none of them were developed to treat migraine at all.
You can group most of these drugs into treatment for blood pressure, epilepsy and mental health issues.
The idea that migraines are mainly caused by blood pressure has kind of aged out with advances in research, but the fact remains that some medication that acts on blood pressure still helps migraines.
I think, bearing in mind that a migraine is a neurological storm, that it makes sense that meds that act on activity in the brain (mental health meds/epilepsy meds) can help migraine. Makes logical sense, right?
The usual procedure for taking these medications for migraine (at least in the UK) is to titrate up to the correct dose, and then (assuming you tolerate it and don't get floored by adverse reactions or the side effects) remain on that dose for 3 months before concluding if the medication is successful or not.
If you're seeing some improvement but not a lot, they might keep you on it for longer, or increase the dose.
Otherwise, 3 months and no improvement means you move onto the next drug and/or treatment.
A lot of these drugs have some really heavy side effects. I've experienced worsened tremors, awful dizziness, change in sense of taste, changes in appetite, terrible brain fog.
For migraineurs it comes down to a balancing act.
How bad are the side effects vs how much is this med helping my migraines, and which of the two am I best able to handle.
Maybe you can manage dizziness or not being able to drink Coke anymore over the migraines.
Maybe the awful tremors and inability to think clearly is worse than bearing with the migraines.
This is usually something you discuss with your specialist.
Just saying again, some of these meds are a little hardcore. Don't try treating your own migraines on your own with these meds if you can get your hands on them somehow. Apart from the side effects, the dose if really important too.
In the UK, if you've failed at least three preventative treatments, and have been managed for medication overuse headaches, you can try botox.
BOTOX
The reason botox works for migraines isn't well known, but doctors think it blocks pain transmitters in your brain.
Botox, or botulinum toxin, is a nerve toxin that paralyses muscles.
It's used for cosmetics treatments, but also medically for hemifacial spasm, cervical dystonia, cerebral palsy, bladder pain, lower back pain, neuropathic pain and stroke.
When used for migraine, it's delivered in a series of 31 to 39 small injections, mostly around the forehead, but also on the temples and at the base of the skull.
If you've ever had acupuncture, the needles are a lot like that. I thought they'd hurt more than they did. They were just little stings, not even as bad as plucking an eyebrow hair. Of course, everyone's different with different pain thresholds (especially if you're oversensitised migraine pain leaves you with allodynia) but it's truly not that bad.
You get three sessions 12 weeks apart, just like taking the meds, and if you've had improvement you can continue. If you don't, its on to the next med or treatment.
It feels weird when it settles in. Your forehead tends to freeze, so you can raise your eyebrows and have no lines there. This might unsettle some people, but it does wear off over time.
Side effects include neck pain, muscular weakness and a drooping eyelid, but these improve as the botox wears off. I had a little neck pain, but nothing else. One of them in my forehead bled only a little, none of the rest did.
You can have an allergic reaction, but they will keep you in the treatment or waiting room for some time after your first treatment to check that.
Getting botox for migraine sounds worse than the experience is, but it is about 75% successful for reducing migraine.
Not for meeee
GREATER OCCIPITAL NERVE BLOCKS (GONB)
If your migraines have been resistant to drug treatments and botox, your specialist might decide to try GONB. This is usually a treatment for cluster headache or headaches that originate from pain in the neck, so it may not be applicable to your specific situation.
This treatment involves injecting an anesthetic and a steroid (not always both) into the back of your head/top of your neck around the greater occipital nerve (GON).
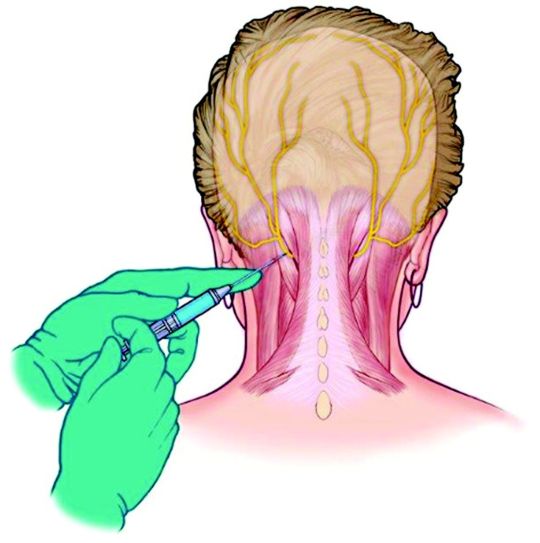
The GON runs from the top of the spine to the scalp, and feeds into an area of the brainstem called the trigeminal nucleus.
A nerve block reduces traffic in this nerve, so reduces the amplification of pain and other sensory information that might be overloading this area.
In simple terms, the nerve block stops the pain signals going into the nerves that make you feel the headache.
A lot of people have had success with this treatment, but I'm not one of them.
I don't want to scare anyone!
The reaction I had is (apparently) pretty rare.
After the neurologist injected the first lot of lidocaine into one side of my head, then the other, I almost immediately felt dizzy and sick.
He let me lay down for a moment, but I felt that I was going to puke, so I had to get up. What followed was tunnel vision, greying out, nearly full syncope (fainting) and then vomiting.
I was having a reaction to the lidocaine, which suddenly made my nausea and faintness when I had my lumbar punction (spinal tap) make sense.
I wasn't able to get to the stage where I had the steroid injection, and whatever there was of the anesthetic after my body tried to purge it made no change to my migraines.
I can't speak for the efficacy of the GONB because my body failed it, but if it's offered, I'd encourage you to try it. Apparently it has helped a lot of people.
CGRPs
After trying 3 meds, then botox, then the GONB and failing all of them, I was put on the next med to see if I'd respond to any of them.
You don't need to have exhausted every pill before trying injection treatments.
You can also mix and match treatments, especially a pill or a CGRP with botox.
With the knowledge that you spend a minimum of 3 months per med (and assuming you don't come off it immediately due to adverse reactions) you can only go through 4 meds in one year. It takes two years on this schedule to go through the meds I've worked through, not including the botox and GONB, and the extra time taken to titrate to the correct dose.
Finding a medication that works to prevent your migraines is a long and exhausting process.
Thankfully, recent research into migraine has come out with the biggest breakthrough in migraine management, I'm going to say ever, because we now have the first medication created directly for the prevention of migraines.
CGRP stands for Calcitonin Gene-Related Peptide
It's a chemical involved in transmitting pain signals through the nervous system – and it’s also associated with the triggering of migraine attacks (among others).
CGRP medications are actually ANTI-CGRP drugs, designed to stop the action of the chemical.
The ones currently available in the UK fall into two groups.
Aimovig (erenumab) that works by binding to the receptor.
Ajoy (fremanezumab), Emgality (galcanezumab) and Vyepti (eptinezumab) which bind to the protein.
Because of that, if you don't have success with Aimovig, try one of the others (and vice versa) as you might see some improvement.
These are adminstered by self-injection (although the first one will be done under nurse supervision) every month with something like an epipen that's injected into your thigh.
The injections hurt me and ached afterwards, but I had no other side effects than that.
I actually had one migraine day where my pain was a 3, which hadn't happened since I started having migraines, but unfortunately, NHS guidelines state that you need to have a reduction in pain days or a significiant reduction in pain in order to stay on them, so I was taken off.
We've just had Vyepti (eptinezumab-jjmr) approved for some people with migraine in the UK.
Vyepti is a CGRP administered via IV infusion over 30 minutes at a clinic, and it's still such a new drug that they're still collecting information on side effects, etc.
I've had my first dose (they're given every 3 months) and while I didn't see a reduction in pain days, I saw maybe a slight reduction in pain, but more than that, my brain fog and pain cloudiness really cleared up, at least for the first month and a half that the effect lasted.
I was actually present in my body for once, instead of half-checked out, even if I was still in pain.
I don't know what the review will bring, but I hope they let me stay on it.
In the US, they've also got a new group of drugs called -gepants (Ubrogepant, Atogepant and Rimegepant for now) which are being used preventatively, but also like triptans, acutely.
Like the injections, they also work on the CGRP receptors by blocking their effect.
I don't know very much about them, but they're also some of the first drugs made specifically for migraine, and there's a lot of excitement about them.
They're safer than triptans for people with heart issues to take, and they DON'T CAUSE REBOUND HEADACHES!
This is huge in the world of migraine treatment, as there are no other acute treatments that do this.
NON MEDICINAL
A large chunk of preventative non-medicinal treatments for migraine involve making lifestyle changes (I know)
The migraine brain is oversensitive and overreactive creature, and ANYTHING can push it into a tantrum. Weather changes, temperature changes, lights, sounds, smells, so many things that we can't control in our environment.
Our migraine brains love routine, and even though it's annoying and removes some chunk of flexibility in our lives, it annoyingly does help.
Sleep routines are helpful, as much as you can fit yourself into one. Setting sleep and wake alarms with x amount of hours in between (7 or 8?) and then sticking to them rigidly means that you'll be getting up when you're still sleepy and going to bed when you're not, but your body will eventually fall into a rhythm and you'll find yourself sleeping and waking at those times automatically.
Issues: daytime naps are no good for sleep routines, and sometimes you just HAVE to sleep when a migraine hits. What if you want to stay up on the weekend? It's difficult, but keeping to a schedule as much as possible is better than leaving it in the wind.
Eating regularly, small meals often is the best. I'm not going to spend a lot of time on this because diet is a huge and sensitive subject, and comorbidities can make this even more difficult, but as far as migraines on their own are concerned, they like the body to be kept as stable as possible, which means a level blood sugar level, etc, and avoiding hunger.
Exercise? I know, I'm not going there, apart from, gentle stretches for your neck, maybe your back, can help. Even if neck problems have nothing to do with your migraines, you're going to end up all crunched up and tense from being in constant pain. Look at stretches for post-operative, for the elderly, for anything you can do in bed. It doesn't have to be high impact or intense, just something you can do now and again to keep your muscles loose.
H~y~d~r~a~t~i~o~n. I'd say use a pretty bottle, but honestly, using whatever will make it easier for you to fill and keep drinking from is better than something that fits your aesthetic. You can always decorate a plastic bottle, or use a favourite glass.
Apart from all those irritating things that abled people always recommend (yoga anyone?) there are also non-drug but prescribed treatments.
One category is DEVICES
I've only tried the sTMS device, so I'll address that first.
sTMS stands for single pulse transcranial magnetic stimulation
You press the button to charge the thing. When it beeps you place the bean-shaped device at the back of your head so it cradles your skull, and then press both buttons at the same time.
There's a ka-chonk, and a sensation like someone's smacked you in the back of the head a little, which is actually the small magnetic pulse.
It works by generating mild electrical currents in the brain that are supposed to disrupt the brain activity linked to your migraines. You can use it acutely, but also daily (2 or 3 times a day, 1 or more than 1 pulse at a time) to prevent migraines.
The machine didn't do anything for me, and made my scalp feel a little sore, although that doesn't appear to be common.
You may also have heard of the Cefaly, a device otherwise called a 'external trigeminal nerve stimulator'
There's that trigeminal nerve again, running around the side of your face and your eye, playing up and causing pain.
You place an electrode on your forehead, and the Cefaly generates micro-impulses to stimulate the trigeminal nerve's nerve endings.
Be aware that the efficacy of the Cefaly device is debated, but it does help some people.
ACUPUNCTURE has been used to help migraine
I had many courses via my GP (the only good one I had) who was trained in acupuncture and went above and beyond to give me as many treatments as possible. I think I had 12. I felt something from them, but they didn't have any effect on my migraines.
Finally, not a drug per se, but VITAMIN SUPPLEMENTS
The best are a trio as follows:
Riboflavin 400mg once daily
Co-enzyme Q10 100mg three times a day
and Magnesium (there are two/three types and the doses are different)
Citrate 600mg OD
Tricylicate 250mg twice a day
or Phosphate 400mg once daily
There is also therapy that is prescribed for management of migraine, not so much prevention as just giving you tools to learn to live with being in pain.
I haven't gotten to that stage yet, and have mixed feelings about it.
Some people have said it's helped, some said it hasn't.
It -feels- a lot like being told 'we can't do anything to help you, you just have to deal with being in pain now'
I haven't tried it, I probably will end up doing so, and maybe I can write a little about it then. For now, I can see why it could be useful, but it does feel a little bit like being abandoned.
And that's all I've got for preventative treatments.
I don't know when I'll be able to start writing about my diagnosis journey, but that should be the next part.
please excuse any typos!
i hope this is still helpful for some people.
#migraine isn't a headache#migraine#disability pride month#migraine awareness#chronic pain#spoonies#headache#preventative meds#migraine medication#migraine treatment
10 notes
·
View notes
Text
we feel like we have covid and we tested negative so hopefully that does actually mean we don't have it instead of it being a false negative but either way holy shit we feel ill
#personal#thoughts#🍬 post#vent post#I would like to stop constantly getting ill and having symptom flares and getting increasingly severe migraines and whatever the fuck else#every time one set of symptoms calms down something else seems to get worse for one reason or another#we found a medication that helps our IBS symptoms and some stuff that helps relieve the pain from our migraines#but then there are new migraine symptoms we can't figure out how to deal with#and the air pressure keeps causing pain from old injuries to flare up so bad we have to lay down for most of the day#we got treatment for something that'd been fucking us up for months and the treatment then fucked up our digestive system for months
3 notes
·
View notes
Text
Damned if you do, damned if you don't, in a society that refuses to understand
If you have a chronic illness, some weeks can be overwhelming & you need to vent off your frustrations, take a load off. But with that comes vitriol from a society that demands we bear down & crack on with it, ignorant to the fact that we can't.
A society that currently promotes being kind, stamping out bullies & reaching out for the sake of your mental health, suddenly shuns and forces you to be quiet. The chronically ill are stigmatised for highlighting their struggles because "others have it worse."
Whilst minimising our battle, they cannot relate to what being chronically ill means.
They can accept that you can leave the light on all day but if there's no money in the electric meter, it will turn off. But they can't comprehend that chronic fatigue is anything more than "tired," - a night's sleep will fix
They fail to understand that chronic pain is more than a bruise or an ache. We tell them. Oh how many chronically ill patients have told them! But they do not listen. They do not hear our words. I am screaming into a void right now. So many of us are. I hear you.
We are shamed for being house or bed-bound. Criticised for not helping ourselves. Ostracised when our symptoms get worse. Yet when we find energy, strength & the mental exertion to reach out, we're knocked right back down. When we do something that will relieve our symptoms, they claim it's "all about you."
Simply, what the f*** do you want from us?
Chronically ill people see treatments for so many other illnesses that are successful & give back life or prolong life to the person. We see medical success everyday, we bear witness to what seems impossible chances. We are asking for that too.
Many of us are waiting for treatment, longing for treatment, begging for treatment. We're labelled as mentally ill instead, because if you can't get out of bed, it must be your mind's fault, right?.. No.
Many of us are shells of our former selves, just existing, waiting, longing, hoping, self-soothing, without treatment. We are still people. There will never be another like you. We matter. Hear our voices.
Uniconic
#chronic fatigue#chronic illness#chronic migraine#chronic pain#chronically ill#fibromyalgia#mental health#fibro#myalgic encephalomyelitis#covid#long covid#covid19#health treatment#chronic life#chronically tired#chronically sick#M.E#POTS#life#society#social issues#chronicallyfabulous#out of spoons#disability#disabledandcute#disabled community#disabled life#disappointed#disabilties
24 notes
·
View notes
Text
I'm starting to think I just went from regular migraines to cluster migraines
#i don't know what to do anymore#it feels like everything is a cause#the weather#the light#not having coffee#not having breakfast#my sinus#my constantly blowing my nose at all fucking hours of the day#loud noises#too much sun#wearing sunglasses when its darker#not enough sleep#too much sleep#neck pain#back pain#speaking too loud#dead ass these all feel like they cause me migraines#i haven't been to the neurologist in years bc I sincerely didn't need it#i did treatment before and i got better#but it just got worse out of nowhere#and I am fucking sick of doctors#i genuinely dont have time for more appointments
4 notes
·
View notes
Last Seen Blogs

teamzenith
Teeeeeam Zenith!

night-giraffes
i wanted somewhere to post fic & reblog trek gifs

senqwr
sei

raikcwyc314
Led Tageslicht Hinweise

supremewriter
Untitled