#that this so called symptom is this severe for me and no medical professional… addresses it
Text
thinking about how every doctor, psychiatrist, and therapist i’ve seen have all dismissed my anxiety as a symptom of my other diagnoses (ptsd, adhd, and bipolar) and if they can just get these diagnoses under control then my anxiety will cease to exist.
(tw for under the cut: anxiety ofc and suicidal ideation
i’ve been on anti psychotics, anti depressants, mood stabilizers, and stimulants and the anxiety has never gone or eased unless i take my emergency anti anxiety med…
like these other types of meds have helped! i won’t say they haven’t.
however comma
my anxiety has barely lessened all these years and has, in fact, gotten worse. i’m pretty convinced rn that if i could get that part under control of my mental health, i’d be doing so much better.
literally today i got so anxious about my future/financial problems/life that i got suicidal. and yes that’s definitely paired with depression (which also hasn’t been diagnosed because oh that’s just part of the bipolar!)
and yet i’m going to find a doctor who will yet again dismiss anxiety as a symptom that will go away when treating the underlying cause… i don’t think it’s a symptom, my dudes!
#personal post#mental health#suicidal ideation cw#anxiety cw#i am safe! just so everyone knows. i am okay but it’s just ridiculous#that this so called symptom is this severe for me and no medical professional… addresses it#even when i bring it up and discuss how it’s affecting me
7 notes
·
View notes
Note
i'm curious at what point you think smth ceases to be cognitive dissonance and becomes a system? i have severe trauma which resulted in a sort of split within me between my 'true' self and a 'defensive' self which is cold/unemotional/obsessive/productive. i have done some IFS work and found it very helpful and as a teenager i did identify this second self as a separate person who i converse with (and still do). i often have to recognize that i'm in that second self/state and forcibly drag myself out of it in order to be present emotionally or address certain things. at the same time, i don't experience time loss and i don't often converse with the self, it feels a lot more like a defense mechanism. i'm unsure if continuing my childhood habit of identifying and speaking to it as a separate person is more harmful or helpful, like if it is further disassociating me. i have had conversations with it and he has alluded to a third self which is deeply deeply violent towards me that he is trying to protect me from, but again i'm not sure how much of this is just IFS separation of parts as opposed to a true system. i'm mostly interested in where you think the line is between fractured selves with trauma as opposed to a system
so like, imo, the line between system and not-a-system is wherever you decide to draw it, and that's probably the most important takeaway here but also might not be the kind of answer you're looking for, lol. So the answers i will give include like. medical language, and my understanding of how clinicians differentiate this kind of stuff, which is a) something i spend a lot of time reading about but am not an expert on, b) not at all meant to define what i think a 'real system' is or isn't and c) something you can totally discard if it's not helpful to you personally.
fwiw, i'm pretty sure 'fractured selves with trauma' is exactly what plenty of MH professionals would describe as a system
i can't diagnose you with anything nor would i want to but your description of the 'defensive' self protecting you from another self (that you are not in contact with, but that the defensive self is) sounds To Me like there are dissociative barriers involved here that are stronger/more complicated than what's typically seen between parts in an IFS framework.
re: worrying about worsening dissociation, i don't think categorizing this other self as a separate person would cause further dissociation on its own. i think if you are welcoming, curious, accepting of and work to communicate with the other self you're describing you might even find dissociative symptoms Improving. on the flip side: if you identify this self as a separate person and then use that to reject and disavow it, that probably Will worsen dissociation!
^ i've talked about this in more detail in a post here
i do think there are probably some safeguards you could put in place if you're worried about worsening dissociation as you explore this. i'll put my thoughts on that under the cut bc this is getting long
it sounds like you are looking for an objective standard you can use to categorize what you're experiencing, and i don't think i can provide one for you, but i can tell you some stuff about how i draw the line for myself, personally. i'll put that under the cut as well:
so like. this gets kind of complicated to explain because i exist as a member of a larger system with very differentiated alters. however for ME as an alter specifically: my subsystem functions kind of similarly to what you describe. we don't experience time loss, we present as different versions of the same person that each exhibit different defense mechanisms in response to being triggered.
the reason we decided to call ourselves separate facets and differentiate from each other--even though we basically identify as the same person--is when i'm in one self-state, i feel like the emotions and behaviors of the other self-states don't belong to me. me (🐛) and another facet (🎶) share the same name and identity on the surface, but he tunes out stressors with fun distractions and blind optimism, and i don't. i wouldn't do that. when i remember times he was fronting i think 'that's not something i would do'. his behavior is outside my understanding of myself. so we call ourselves separate from each other.
basically for us it's a matter of "wow, i was feeling really triggered/stressed/unusual when i did that" vs. "i don't understand why i did that, i don't feel like i would do that, i can't imagine why i was thinking/feeling that way when that happened". it's not always clear-cut but you might find these things helpful to consider, idk.
FINALLY if you want to explore seeing this other self as a separate person/a member of a system but are worried about worsening dissociation--these are TOTALLY optional and it's completely up to you what you decide to do, but here are some (open-ended) questions you might want to ask yourself:
how do i feel about the aspects of my inner experience that i'm exploring? scared? guilty? hopeful? curious? many or none of those things?
am i usually able to identify when i'm dissociating? do i have coping methods i can use to ground myself?
do i feel safe? if i start feeling unsafe, are there ways i can return to feeling safe in my mind and body?
i hope literally any of this was helpful and/or made sense! i wish u the best as u explore this stuff and at the end of the day it's Completely up to you how you want to identify your experiences.
18 notes
·
View notes
Text
Here are some tips that I have discovered that are beneficial and healthy ways to cope with your mental illness in order to feel better. I understand it is very difficult to cope with, but here are some things that are helping me currently. (I am still learning healthy coping mechanisms myself, and I am in the process of beginning medication and therapy again, so by no means am I a saint or a know it all when it comes to this, and I realize everyone is different, and what may be right for me may not be right for someone else.)
*When you are having debilitating symptoms, or bothersome symptoms/behaviors that affect your day to day life, relationships with others, employment, etc. Here is what I believe that you should do.
1.) Actively seek out a therapist, psychiatrist, (or nurse practitioner) and seriously consider medication and therapy if you feel that your symptoms and behaviors are negatively affecting your daily life, relationships with others, your employment, and the relationship with yourself. The quicker you seek treatment, the quicker you will begin to learn how to cope with your symptoms and learn how to replace unhealthy destructive coping methods with healthy ones, as well as taking your medication as prescribed.
2.) Even though it is difficult to calm down, and relax, do your best to grab some paper and write down how you are feeling. It can give your brain a mind dump, and try not to be judgemental with your thoughts at first. You don't even have to look at them at first if you are too uncomfortable with your thoughts. If need be write them down, and then try to occupy your mind with something else, like a TV show. If this happens, please refer to your therapist, and he or she will help you address those thoughts in a safe, structured setting. The words or thoughts don't have to make sense, be upbeat, or sound pretty. Journaling is a way of getting out those thoughts, no matter how negative or scary they may sound.
3.) If your symptoms are so severe that you cannot be alone, and you are planning to hurt yourself, or others, or are thinking suicidal thoughts, or planning suicide, PLEASE call 911 immediately and get yourself checked in to a mental hospital. It sounds scary as fuck, but you need to protect yourself. I myself have been in a mental hospital for a week. That is the safest place you can be, until your doctor can get you stable enough to get back into society.
4.) Invest in some Dr. Teals bubble bath or soaking solution Epsom salt. I highly recommend the Calm Your Mind one. Or the Soothe and Sleep one with Lavender. It does help. ❤️
5.) If you have animals, hold them and pet them. It is scientifically proven that pets help reduce anxiety and stress. I know I love holding my kitty. ❤️
6.) Phone someone you can trust and feel safe with, but don't get on the phone with them and catastrophize your issues and make a habit of crying wolf everytime something negative effects you. Simply open up to them about how your day is going, and try to keep the conversation lighthearted, and try to remain as positive as you can, despite all the bullshit going on with you. Leave the complex issues, symptoms and behaviors you are experiencing to a licensed and trained professional. They went to school and are employed and licensed to give professional advice and show you how to implement healthy structure and habits in your life, not your family, your boyfriend, husband, or your friends. It may be tempting to let it all out to someone like an avalanche, but that is not a tactful or healthy way of dealing with your issues. If you let all of your issues, behaviors, anxiety, etc out on someone other than your therapist, and doctor, it will burden and overwhelm them with your issues and it will become an unintentional habit, to where all you talk about with them is your issues and insecurities, and that is not what friends or family is for. Friends and family are there to support your mental health and growth, not be a promoter of your vicious cycle of unhealthy and destructive behaviors be it intentional or unintentional. There is a difference between seeking support, and seeking rescuing. You don't need to be rescued by someone, and your friends, family, employer, etc are not in your life to be a toxic filter that you spew your issues to all the time, because it will inevitably push them away from you and you will lose that valued friendship or relationship with that person or people. You may feel like you are at your wits end and have a sense of impending doom all the time, but the best way to deal with those issues is with a TRAINED AND LICENSED professional that you can trust, and that is right for you. It may take multiple therapists and doctors you may have to go through before you find the right one, but don't give up, getting started on the healing journey is a process and it takes time, patience and effort.
7.) Talk to your therapist about learning how and when to address your issues with yourself or someone else.. And learn how to set some boundaries with yourself and others. Learn how to keep certain things private that you normally unintentionally allow yourself to share with everyone in your life. Not everyone needs to know your goddamn business, for a multitude of reasons. Not everyone is going to hear you out, and they might make assumptions of you based on your behavior and what you tell them. They may judge you, condemn your behavior, etc. and may not have your best interest at heart. They will become overwhelmed with your issues and they will begin to see it as a toxic behavior that you may or may not be intentionally rubbing off on them. There is a time and place and correct way of addressing your issues, so please make sure that you choose carefully about how and when you open up to someone about how your feeling. Again, I highly recommend divulging your issues solely to your therapist. That is what they are there for.
8.) Analyze your behavior and symptoms that you are exhibiting. Begin to take control, responsibility, and accountability of your issues with yourself. You are in the driver's seat of your life, no one else. Only you can make the change for the better or worse. Remember that your behaviors and actions not only affect you, but everyone around you. So remember that if you want to do better and improve your quality of life in a healthy way, you have to make the effort to implement change in order to heal and grow. Don't give up.
Thank you.
*****I am not a licensed professional. These are only tips and advice.
2 notes
·
View notes
Text
Best Lady Doctor For Piles Near Me | Yazh Healthcare

Welcome to Yazh Healthcare, where we prioritize your well-being. If you are looking for relief from the pain of piles (hemorrhoids), you have come to the right place. We understand how sensitive this issue is, particularly when seeking medical attention. That's why we've put together this guide to help you identify the best lady doctor for piles near you, assuring both comfort and quality care.
Understanding Piles:
Before beginning your search, you should understand what piles are and why obtaining medical attention is critical. Piles, also known as hemorrhoids, are enlarged blood vessels in the rectum and anus. They can cause discomfort, pain, itching, and even bleeding, making daily tasks difficult. While piles can be treated with lifestyle changes and over-the-counter medications, severe cases may necessitate expert intervention.
The Importance of Choosing the Right Doctor:
Selecting the right doctor for your piles treatment is vital for several reasons:
Comfort and Confidentiality: Many people find it embarrassing to discuss their piles, especially when it comes to symptoms and treatments. A female doctor can provide a comfortable and empathic setting in which to address your issues.
Expertise and Experience: Treating piles efficiently necessitates knowledge and experience. By selecting the best lady doctor for piles near you, you can be confident that you will be treated by a qualified specialist who is well-versed on the condition and treatment alternatives.
Personalized Care: Every person's experience with piles is unique, and treatment options should be customized accordingly. A caring female doctor will listen to your individual needs and create a personalized treatment plan that is ideal for you.
Yazh Healthcare: Your Partner in Piles Treatment:
At Yazh Healthcare, we recognize the difficulties involved with piles and the significance of choosing the proper specialist. Our staff is lead by competent and compassionate female physicians who specialize in piling therapy. We provide specialized care in a warm and confidential setting, assuring your well-being at all times.
Do not allow piles prevent you from living your life to the fullest. Relief is within reach when you consult with the top lady doctor for piles near you. Whether you choose Yazh Healthcare or another reputable provider, prioritize your health and get professional help to effectively treat your piles. Remember that you deserve effective and compassionate care, so don't hesitate to take the first step toward relief now.
Contact Us:
Website: https://yazhhealthcare.com/
Call Us: +91 7418879188
0 notes
Note
I have a story regarding to "The Twitching Generation" or at least similar to it.
I have a female cousin who's dearly close to my family and she self-diagnosed herself with narcolepsy because she's constantly falling asleep during the day mostly of the time but her mom already took her to see a doctor and made several tests even with a polysomnography multiple times and they found nothing wrong with her. Her blood is clean, there's no disease or disorder of any kind that they could find in her.
So, what's causing her to fall asleep during the day? Well, her mom admitted during a lunch that she's always sleeping very late after midnight like between 1 a.m. to 3 a.m. and wakes up very late almost at noon, plus she doesn't eat properly and eat junk food and is addicted to social media. Here's the worst part: my cousin denies everything and insists that she has a medical condition despite having medical evidence that contradicts her.
This is the most eye-opening and shocking thing I've encountered in first-hand. Her family and my family have tried everything to convinced her to change her lifestyle since what she's dealing with could've been addressed easily with a 9-hour sleep, healthy food and less usage on the internet but she refuses to do that.
It's really sad to see someone, especially a family member destroy themselves for an irrational belief.
This is a great example of the problems with self-diagnosis and self-identification, and the devastation it brings.
Self-diagnosis isn't great. Even a trained professional might need to get you into an MRI or take a biopsy or something to be able to accurately diagnose you, and yet you think you can just read WebMD and accurately diagnose yourself? No.
Interesting how you never see self-diagnosers diagnose themselves with pancreatic cancer, liver failure, multiple sclerosis or malignant narcissism. They always seem to be the quirky, yet transparent ones that attract attention and sympathy, justify their behavior - which is sort of like "I can't help it, I'm a Scorpio!" - or both.
It wouldn't necessarily be so bad on its own. You look up your symptoms and try to guess what you've got. You go to the specialist and you find out "oh, I don't have Dissociative Identity Disorder, I have Type 2 diabetes because I eat like every day is Halloween, boy do I feel silly."
When the self-diagnosed condition becomes a part of the individual's personal identity, it becomes threatening to suggest otherwise. To paraphrase Kimberlé Crenshaw, 'we all can recognize the distinction between the claims "I am Narcoleptic" and the claim "I am a person who happens to have Narcolepsy."' To question any of this is to be regarded as some kind of bigot or hater for not celebrating this identity.
It also seems pseudo-religious when you think about it. What would convince her that she didn't have narcolepsy? When I ask a similar question to the religious, the answer, stated proudly and confidently is "nothing. Nothing could convince me that my god is not real." If you got an answer like that from her, you can be certain she's not rational and her belief is just as faith-based.
Since social capital is now calculated on acquiring "marginalized identities" and perceived "victimhood," not on ideas and values, it's even worse to dare point out that they don't have a condition at all, and are remarkably ordinary. That would be the worst thing of all.
It would be interesting to ask her about an article that you read, that she's no doubt well aware of, about an injection you can get every two months which will eliminate narcolepsy entirely. And whether she will be getting it. I would put money on her "narcolepsy" being the "wrong kind" or some other excuse.
What's really gross is that there are people who actually have narcolepsy, DID, Tourette's and other conditions who would love nothing better than to wave a magic wand and just be merely ordinary, to fit within the statistical bellcurve called "normal."
And then you have people mapping their personality traits or flaws onto these serious conditions and adopting them as an aesthetic, trivializing them in the process.
#ask#personal identity#identity labels#narcolepsy#identity politics#self diagnosis#self diagnosis is not valid#religion is a mental illness
42 notes
·
View notes
Text
Prelude (Ethan x f!MC)
Book: Open Heart, Book 1
Pairing: Dr. Ethan Ramsey x F!MC (Dr. Lilac Allende)
Word count: 1.5 K
Premise: Three moments leading up to their fateful meeting.
Author’s Note: In which I try to explain why MC didn’t know what Ethan, her medical hero, looked like. Also, my (late) fic for the book 1 replay. Thank you @aestheticartsx for pre-reading!

Three.
Harper frowns down at the file in her hand, her sharp gaze burning into the collated papers as though coercing them to solve their dilemma once and for all. From the end of the table, Cyrus lets out an inpatient sigh.
“It's very simple, Harper,” he drones. Ethan's fists clench reflexively at his sides, urging to remind Cyrus that Harper is the chief now and warrants more respect than his insufferable tone is offering. “The last spot should go to the candidate from Harvard. We are the best hospital on the east coast, after all. It only makes sense.”
Harper looks unconvinced and still, her pensive expression remains fixed in the file.
“An ivy league degree does not a good doctor make,” Naveen adds sagely into the ensuing silence. His smile is placid enough but Ethan knows the older doctor well enough to hear the warning edge in his voice. Evidently, even Naveen disapproves of Cyrus's lack of respect for their new chief.
Cyrus scoffs.
“And if you need further proof of that, Doctor Cyrus,” Ethan begins dryly, eyes boring into him. “Then look no further than your side of the conference table.”
A few attendings—at least the ones who have become increasingly tired of Cyrus's boastful proclamations about his alma mater—laugh quietly at the jab. Cyrus splutters, his face an unpleasant shade of red as he glares daggers at Ethan.
“This candidate,” Harper says at last, unaware or uncaring of what she had just interrupted. Her two lone words are enough to command the room's attention at once, but her hazel eyes are on Ethan. “You're convinced she's the best fit for Edenbrook?”
Ethan meets her eye and pauses.
It's the first time they look at each other directly since he ended their relationship two weeks prior. Despite the brief time apart and an unshakeable resolve to be professional, his stomach sinks heavy, like a stone.
Harper looks as graceful and dignified as ever, keeping every emotion in check. Yet, as she holds his gaze, Ethan can see a small flicker or sadness and his stomach twists with guilt.
“I'm positive, Chief Emery,” Ethan responds. “This candidate exhibits the type of potential we look for at Edenbrook.”
The use of her new title seems to snap Harper out of a reverie.
“She graduated top of her class and ranked in the top percent among our chosen cohort of interns,” Ethan continues. “I've also looked into her research and it's among the most promising I've seen. I recommend her without reservations.”
With a single nod and a sense of finality, Harper closes the file.
“Then it's settled. We have our last intern.”
“You're joking, Harper,” Cyrus blurts out, incensed. “We're giving a coveted spot to the candidate from UCLA?”
He says the name of the school with so much derision, Ethan feels his ears flare up.
“That Doctor Ayala?” Cyrus continues.
“Doctor Allende,” Ethan corrects, jaw clenched.
“Don't we have enough charity cases in the cohort already? This is token—”
But the vitriol is quickly interrupted by several things happening at once: Ethan darting forward, fists ready; a startled, collective gasp from the other attendings; Naveen, quietly intercepting Ethan and halting his steps with a steady hand, a feat that is impressive for a man much older and shorter; and Harper, also on her feet, directing a disgusted look at Cyrus she doesn’t bother to disguise behind professionalism.
“I would think very carefully about finishing that sentence if I were you, Doctor Cyrus,” she says, her voice low but with the impact of a clashing gavel. “And I ask that you address me as Chief Emery moving forward.”

Two.
“If you end up marrying someone with a Boston accent,” Laurel is saying with a devilish grin. “I will never be able to keep a straight face when they talk. Pahk the cah in Hahvahd Yahd.”
Her older sister peers at Lilac over the flaps of an open cardboard box, the glint in her eye growing wickeder still. “Imagine what they’d sound like in bed. You're so fucking gawgeous, dawctaw—”
Before her sister can escalate that impression into disturbing territory, Lilac silences her with a well-aimed pillow. It succeeds in hitting Laurel straight in the face but also in turning her laughter into a cackle.
“Are you going to help me pack or not?” Lilac says sternly, though the effect is entirely ruined by the smile that manages to break through.
Laurel raises her hands in defeat and returns to packing Lilac's books neatly. They work in companionable silence for a few minutes with nothing but their favorite music blaring from the speakers of Lilac's phone.
“Is this the book?” her sister asks suddenly, turning a worn textbook in her hands and studying it closely. “The one written by your medical crush?”
For some inexplicable reason, Lilac feels her face flare with heat. “He's not my crush.”
“You just worship the ground he walks on,” her sister returns, flipping through Diagnostic Principles. “Though, you're right. In order to have a crush you'd need to know what he looks like.”
Laurel reaches the back cover, frowning. “Why wouldn't he add an author picture?”
Lilac says nothing, biting the inside of her cheek. She can't blame her sister for being curious and a bit disappointed at the lack of visual representation. After all, Lilac had felt crestfallen when all she found in the author's information section was the green and blue Edenbrook logo.
“Maybe he's a private man and doesn't like his picture out in the world? Maybe he wants aspiring doctors to focus on his research and not his looks?”
“So he's either really hot or really ugly,” Laurel returns, unmoved by Lilac's impassioned speech. “Have you ever tried looking him up online?”
Lilac had been tempted many times, but she was fiercely adamant about keeping her medical hero a mystery outside of his work. It already felt invasive enough to track down his undergrad research and every other minor paper he'd ever written. When it came to Ethan Ramsey, Lilac had searched every corner of scholarly journals and databases, absorbing every piece of his work with an adoration that was already embarrassing enough.
Plus, she would never admit it out loud, but she was also afraid that knowing what the brilliant doctor looked like would somehow ruin him for her. Or at least, alter the image of him she had constructed in her head for so many years. It felt right to continue seeing Dr. Ramsey as the brilliant force that pushed her into her dream career and not as a definitive set of features.
“It doesn't matter what he looks like. He's the best and I'm going there to learn from him, not to judge his appearance.”
“I'm Googling him,” Laurel announces, already typing furiously into her phone. After a few seconds, her phone returns results and her eyebrows shoot up, staying suspended for longer than normal.
“What?” Lilac asks despite herself.
“Wow.”
“Wow what?”
“Just… wow.” Laurel stares down at the screen with such awestruck amazement that Lilac feels a powerful wave of curiosity. “He’s shirtless in some of these.”
“What?” Lilac yelps, feeling her face flare up at once.
“Yeah, apparently you’re not his only fan. Tons of people have taken his picture.” Her sister seems to blink out of a trance, turning the screen toward Lilac. “Here, see for your—”
But Lilac turns her gaze away almost out of reflex.
“No!”
The word comes out far more impassioned than Lilac intended. Still, she resolutely turns her head. “That feels...invasive, somehow?”
“Come on—”
“I'm serious, Lau. I don't want to see. I'm already nervous enough about this whole thing without having to worry about this wow-worthy revelation. And besides, taking someone’s shirtless picture without their consent and posting it online is already bad enough. It feels wrong supporting that.”
Laurel rolls her eyes.
“I'm going to see him in less than a week anyway. With clothes. In a professional setting. As I should. If I waited all these years, I can wait that long.”
A knowing, devious sort of smile pulls at her sister's face. She mumbles something over the music and Lilac can swear it sounds oddly like: “...worth the wait.”
One.
Ethan should have taken the broken and sputtering coffee machine in his apartment as an omen. His morning definitely declined from then on, starting with gridlock traffic and ending with an infuriatingly long line at his favorite coffee place.
The ultimate lack of coffee is probably his fault because Ethan had spent too much time deliberating whether or not he wanted to go with store bought coffee on what promised to be a grueling day. When he had finally made up his mind, however, the line was already out the door.
Irritated and caffeine deprived, he drives back to Edenbrook.
“You're earlier than we agreed,” Naveen says as soon as Ethan accepts his incoming call. “What was the point of rearranging the whole schedule if you were going to come in when you pleased anyway?”
“I'm not even through the gates yet. What are you spying on me?”
“No need. You forget how predictable you are.”
Naveen chuckles as he says this which eases some of Ethan's irritation. The older doctor had purposely scheduled him later in the day to give him some peace on the first day of the new intern cohort.
Naturally, Ethan arrived several hours early, as per his custom.
“Or maybe you know me too well by now.”
Naveen's benevolent laughter turns into a dry but lingering cough on the other end of the line. Instantly, Ethan's insides freeze over, his stomach sinking unpleasantly.
He opens his mouth to question his mentor about this persisting symptom, when sheer reflex prompts him to stomp on the breaks so suddenly, his body jerks forward then slams against his seat.
“Shit.”
Something—or rather someone— had crossed the parking lot road right in front of his car, standing mere inches away from his front bumper.
“Ethan?” Naveen asks through the speaker.
When Ethan recovers and regains movement of his arms and legs, he feels the spike of adrenaline give way to pure annoyance.
The offending pedestrian is a young brunette clad in blue scrubs, a medical intern by the looks of it. She stands there in the middle of the road, her mouth hanging open in a way that would have been comical to Ethan if he wasn't so irritated.
They stare at one another, though Ethan is convinced she can't see much through the tinted glass.
Then, right before his eyes, she seems to recover from the shock. Drawing herself to her full height, she glares at Ethan. At least, he thinks she's glaring through the dark lenses of her sunglasses.
Ethan almost scoffs.
She has the audacity to be angry when she was the one who made the rookie mistake of aimlessly crossing in front of him?
Who the hell does she think she is?
“Asshole,” she mutters, the word quite audible through his windows.
Before a stunned Ethan can respond, she turns on her heel and rushes toward the hospital, a curtain of dark hair dancing behind her.
“What was that?” Naveen asks, still on the call.
“I hate interns,” Ethan responds much to the older doctor's amusement.
Bonus:

Author’s Note: In other words, my MC was late to her orientation because of Ethan and that’s how she met him in the waiting room lol. Thank you so much for reading!
*Tagging Separately
#open heart#ethan ramsey#ethan x mc#Ethan ramsey x mc#ethan ramsey fanfiction#choices fanfiction#open heart fanfiction#Oph book club#playchoices#My writing
250 notes
·
View notes
Text
DAY 4791
Jalsa, Mumbai Apr 10/11, 2021 Sat/Sun 12:04 AM
Birthday - EF Lyudmila Zueva .. Sunday, April 11 .. wishes for your birthday and the desire to be safe nad be protected in your environ .. love from the Ef ..❤️
The desire to put details of time and years spent in the work I do .. in the films worked on .. in the details or stories pertaining to those times .. in any incidents occurred .. in .. whatever ..!!!
So there is refrain and restraint .. life is not about interviews .. to be given in the spent of another for the commerce of another ..
Firstly of course there is the most strongest of feels that the details or connects or conversations giving those events have nothing to do with the one that records it .. they are mine .. they should remain with me .. the idea of the ‘I’ is daunting somehow .. I did this , I went here , I felt this , I ..I I I .. so many I’s ..
The ‘I ‘ is me .. there is wonder then if it can be another’s .. do they really understand or accept or believe or feel the ‘I’ that I have .. and that dissuades me from accepting the request or at times the demand for the concept ..
And they come each hour virtually these days .. a symptom of age and ageing .. “ get him to talk before he leaves the World .. else we shall never know .. or shall never be able to exploit it .. for the public or the self ..”
Is perhaps the refrain in the minds of them that wish it ..
And my hesitancy needs to be understood and not be looked upon as arrogance and ego .. no .. many that I politely dissuade or come away from are graceful in accepting my response .. and I am thankful for that and indeed more ..
.. because there is at the end of it all an, unknown by others, a great disappointment for them .. for they shall get nothing that may be of any interest to any .. so ..
.. allow me to be in my self ..
.. egoistic .. narcissistic .. self centred .. self seeking .. vain .. !
I shall accept all , but shall not give in , I do hope .. and pray ..
Yes I shall not resist any other from exercising their own will and knowledge and interpretation belief and knowledge about me .. I am after all in the public domain , one where it shall be difficult to remain away , when all that we professionally do is to remain with them ..
.. remaining with them is profession .. remaining with me is my employment with me .. a reserve that shall need passwords to submit accede to .. you may guess the password, fluke it , guess it , track back in this so called secure preserve of the various internet traps of the advertised categories .. but it shall still be uninformed and unconfirmed .. and that shall be my submission in the courts of law .. better put, in the courts of the self , where the judge jury prosecution and defence shall all be played , hopefully amicably , with the writer of this four thousand seven hundred and ninety first missive ..
BUT .. the respect for the details that come in abundance from love and desire and affection must have respect .. and care and feel of the dedication devotion and the love that comes to me each hour from the Ef ..
.. and Moses Sapir , the keeper .. has this to say today ..
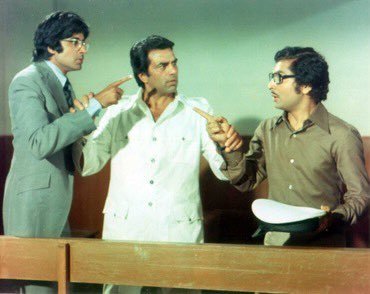
46 years of ‘Chupke Chupke’ , closing in today :
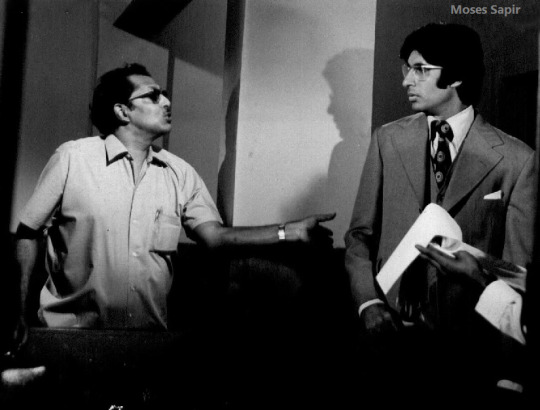
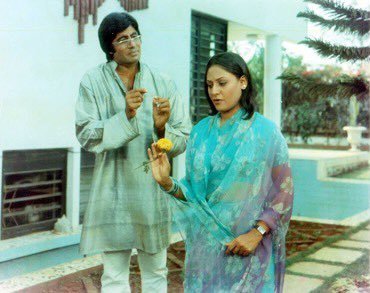
.. the great Hrishikesh Mukerjee .. and the most number of films that I did with him .. perhaps now Ramu - Ram Gopal Varma has overtaken him - and this from “chupke chupke’ .. this house that you see in the picture with Jaya is now Jalsa .. it was the home of Producer NC Sippy .. was bought by us then sold , bought again rebuilt and became Jalsa .. renamed after it was first called Mansa .. Mansa the Mother of this generational family of the Father .. the originator of this legacy of Bachchan .. not the Mother but perhaps the great great grandmother ..
tradition must be given respect dignity and honour ..
Mansa .. changed to be named Jalsa .. and the lawn behind Jalsa , a small lawn , acquired later, has been named Mansa ..
many important films were shot inside these premises .. Anand , Namak Haram, Chupke Chupke , Guddi , Satte pe Satta and several others ..
.. reflections .. that is all that shall be left behind ..
It is the beckoning of the bed now .. but the desire to go to it is hesitant addressal .. if there be such word .. for when you retire for the night - and it is important to specify that, for fear of the entity of ‘breaking news’, there is just the bed and the lethargic act of sleep .. which comes in the thoughts of memorised events , or at times when it does not , the counting upto whenever the counting disappears .. much like on the Operating Table just when they are about to make incision on your body the anaesthetic administered , the kind gentleman that has just given the passing out drug shall politely ask you if you know your counting or not .. say it he says ..
.. and by the time you reach 8 or 9 .. its over .. gone into oblivion .. out for the count .. out for all the procedures to begin , with precision and surgical excellence .. the Gods of the medical fraternity .. God made them special .. when they open up the hitherto unseen insides of the human body , they and only they can realise the complexity of our making and why we resolve and be dependent on and pay obeisance to ‘the Maker’ .. He and only He can explain how He did it .. because its is beyond human know .. beyond by millenniums to the power of infinity ..
.. and they, the medical fraternity, study it and excel in it and execute the procedures and know and execute .. and still to this day , have not been able despite their dexterity , to give a believable answer to the trillions of questions that arise ..

.. so signing of ..

Amitabh Bachchan, the one eyed jack
141 notes
·
View notes
Text
Neuroessentialism and mental health
Hi!
Time for a little rant about neuroessentialism.
The aim of this post is to provide the opportunity to be conscious of the things that influence us when it comes the way we think about mental health and to challenge stigma around mental health.
First off, I’m not a doctor and the information here cannot serve as medical advice. Always consult your doctor before changing your medication or treatment approach.
Secondly, a lot of the information I present here is elaborated on and further discussed in an episode of the Psychiatry and psychotherapy podcast called “Free will in psychotherapy and psychiatry Part 3” and while I will link to as many things as I can, you can also find a lot of the source material on the website for the podcast. https://www.psychiatrypodcast.com/psychiatry-psychotherapy-podcast/2020/7/22/free-will-in-psychiatry-amp-psychotherapy-part-3
So, I see a lot of people talking about mental health on here through a neuroessentialist perspective in memes or text format and I don’t think they’re aware of it so. I’d like to talk a bit about it.
First, I’ll offer a definition of neuroessentialism:
" Neuroessentialism is the view that the definitive way to explain human psychological experience is by reference to the brain and its activity from chemical, biological and neuroscientific perspectives. For instance, if someone is experiencing depression a neuroessentialistic perspective would claim that he or she is experiencing depression because his or her brain is functioning in a certain way.” - Schultz, W. (2018)
I see people talk about, for example, depression in this way often: in memes when people say "I have a literal neurotransmitter deficiency, Karen." or " God forgot to add serotonin when he made me".
Now, why can this be problematic?
Before I get into the issues with this perspective, I will first acknowledge that one of the reasons this view has become so prominent lately is because it aims to reduce stigma around mental health issues.
In the podcast episode mentioned above they point out that “Efforts to reduce stigma should be praised, but they should also be critically analyzed to determine if they meet their goal.”
And that’s the thing neuroessentialism, while aiming to reduce stigma and shame it only does so short term and ends up contributing to stigmatizing attitudes about mental health.
I want to say that it's great to see people fight back when it comes to stigma around mental health. That's what I see people do in these memes. But the effects of neuroessentialist perspectives end up othering people; making them inherently “bad”, “defect” or “helpless”.
Here the deterministic aspect of neuroessentialism comes up - it tells us that there’s something wrong with our brain that we can’t change. It alienates people because it chips away at their and our belief in their ability to change. If you believe that someone's mental issues are rooted exclusively in brain biology, you're less likely to believe that they can control their behavior and so it is less worth the effort of getting them better. This brings about more stigma.
Another thing that’s important to talk about is how neuroessentialism is an extremely simplistic perspective on mental health. And that’s also one of the reasons it has become so big- because it offers a simple explanation to very complicated illnesses.
Here, I want to add a quote by Psychiatrist and psychotherapist Dr. David Puder:
“There are prominent theories out there that we know just aren’t true anymore and that get propagated because they are simplistic ways of explaining things; for example, depression is because you have low serotonin in your brain. That’s just not true. It’s a whole lot more complicated than that.
You could probably show 20 or 30 things that are going on in the brain during depression. Inflammation. Like initially I thought ‘oh depression is inflammation!’
Well, it turns out not all depression has inflammation. Maybe, only one third [of patients with depression] have inflammation markers in the brain.”
We have been looking to neuroscience for an explanation when it comes to mental health and been satisfied with the idea of a simple "chemical imbalance" but truth is that there are many more neurotransmitters which significantly affect our brains when we talk about depression – it’s so far from just serotonin.
Another example of how neuroessentialim can oversimplify mental health is with brain scans. So, in the podcast episode mentioned above, Dr. Puder talks about how he was really interested in emotions and especially studying anger and he was looking at all this research on the different areas in the brain involved in anger. After a while, he says, he began to understand that it’s really complex and you can’t just point at one area and say that’s the area that’s involved in the emotion anger. There are several areas involved in just that one emotion and different studies show different things.
The truth is that the manifestation of mental illness in the body is a very new area of research and we haven’t found physical manifestations for most mental illnesses and the important thing to note here is that despite this we still do have ways of treating all of them.
Alright, all this can seem quite removed from us so how does neuroessentialsim affect us?
In the episode the guest star, Mathew Hagele, further discusses the article which provided the definition on neuroessentialism above: “Shultz looked at studies investigating how patients viewed their own prognosis and later the same with professionals.
The study found that biochemical or genetic attribution scores were a significant predictor of longer expected symptoms duration and lower perceived odds of recovery.” (Lebowitz et al., 2013, p. 523).
Now, this means that the more a patient attributes symptoms of their psychopathology to genetic (inherited disorderes) or biochemical (serotonin deficiency for example) factors, the longer they expected to struggle with their disorder and the smaller the belief that they can recover.
If a person doesn’t believe they can be helped or get better they’re a lot less likely to try and a lot more likely to feel scared and hopeless.
The other side of this coin is the effect the neuroessentialist narrative has on clinicians which Matthew Haegel dives into in the next part of the quote:
“Another study shows that clinicians believe psychotherapy to be less effective when shown biological descriptions of mental health pathologies...
They took a couple different disorders that these clinicians were looking at and one group had a biological explanation and the other did not- had a different type of explanation. And [in] the results that were across disorders, the biological explanation yielded significantly less empathy than the psychosocial explanation. They also did some additional analysis and they found that biological explanations yielded less empathy than the psychosocial explanations among both MD’s and non-MD’s…..”( Lebowitz, M. S., & Ahn, W. K. (2014). )
So, in these studies we see that a neuroessentialist perspective lowers empathy for the patient in medical health professionals and people who weren’t medical health professionals.
Okay, so how does this perception of the patient’s illness affect the patient’s treatment?
I’ll start with a quote where Hagele elaborates further:
“…and finally, that clinicians perceive psychotherapy to be significantly less effective when symptoms were explained biologically than psychologically…[ Lebowitz, M. S., & Ahn, W. K. (2014). ]
basically, linking the idea that the diminished importance of psychotherapy among mental health professionals ascribing to the concept of neuroessentialism is doubly harmful when considering the multiple contexts in which psychotherapy matches or outperforms pharmaceutical interventions.”
What Hagele points out here is the way neuroessentialism can lead to a less effective and ethical treatment of mental illness. It makes us approach an issue in one manner only- fix the brain, fix the behavior. But sometimes what can treat he issue in the brain is, working on the behavior. This can be talked about in terms of meds vs. psychotherapy.
So, seeing mental health from a neuroessentialist perspective, completely excludes the effects of psychotherapy. A classic example is CBT (cognitive behavioral therapy) in which we have “Cognitive restructuring”: a psychotherapeutic process in which a person learns to recognize maladaptive or distressing thoughts and teaches their brain to consider other perspectives or different thought pattern. This is an example of “work on behaviour to better brain” rather than “working on brain will fix behavior”. According to strict neuroessentialism therapy shouldn’t work as well as it does but there is a really big body of science backing psychotherapeutic intervention and its efficacy compared to psychopharmacological intervention.
I feel I should address the discussion of Meds vs. therapy before I continue, (it is a whole topic worthy of a post on its own) but to be brief, they work best together and if you’re weighing one against the other psychotherapy has more long-term effects and barely any side effects compared to medication. There are other factor affecting what would be the most effective treatment approach that further nuances this discussion.
Now this is all a pretty big picture but how is this seen every day?
Well, its seen in the downplaying of the importance of therapy. Often, I see this as people normalize behavior where they kind of devalue the importance therapy or put off working on their issues in therapy with the excuse that it’s only for “crazy” people or not something worth the effort.
Therapy then increasingly is seen as this unimportant, extra thing rather than, in most cases, the most effective and safe treatment. And the less crucial therapy is considered, the less accessible it’s going to be – in the U.S. it can often be easier to get your insurance company to cover for a doctors visits where the treatment would be for your GP to prescribe you an antidepressant than an inpatient or outpatient treatment with a mental health professional.
Another point I wanna put out there is that that neuroessentialist narrative is incentivized by pharmaceutical companies. Dr. Puder talks about his own experience in the podcast episode and makes sure to stress that practitioners are humans too and will of course be biased towards something if that something writes them a check or pays some of their expenses. In the episode they discuss a way in which we have seen the neuroessentialist narrative progress:
“Second, there is evidence that the significant increase in direct-to consumer (DTC) advertising for antidepressants is related to rising prescription rates (Park & Grow, 2008). Such advertisements portray depression as a biological medical condition that can successfully be treated with medicine (Lacasse & Leo, 2005; Leo & Lacasse, 2008)” (613).
Now, medicine is an important tool in psychiatry and there is a lot of unnecessary stigma around medication for mental health conditions. I am under no circumstances arguing that medication is bad and therapy is the only right way to treat mental illness. That would be an extreme simplification and invalidation of human experiences. I also wanna acknowledge that being able to go to therapy in many places in the world is a matter of privilege. Therapy simply isn’t accessible for everyone and people can choose an “only medication approach” for many valid reasons. And if that’s the only treatment that was accessible to you I’m really proud of you for taking care of yourself and doing what you can.
If your doctor has prescribed you a medication please take it and know that the purpose is to help you and that you are worthy of help and good health care. The situation where I would suggest to be a tad critical is when people come in with disorders and issues that they have dealt with for years and most of their life and they are just prescribed an antidepressant and sent home. That simply isn’t effective and ethical care. In that case it is worth investigating getting access to a mental health practitioner as well as continuing with medicinal treatment.
I could talk about this for hours but the last thing I wanna get across is that this is a societal problem. I don’t suggest we turn away from pharmaceutical intervention which saves thousands of lives and helps people get better, rather that we work to make psychotherapy (which can be and is crucial for long term remission and recovery) more accessible for when it’s appropriate.
When your doctor tells you that this invisible illness is because of your biology most people feel validated and experience less shame. The fact that people feel like they need to have a tracible biological “anomaly” in their brains to be worthy of treatment and care speaks to an invalidation that many feel. But the issue here is that we're taught to invalidate invisible illness in society which in the end makes people delay critical treatment or blocks access to ethical and effective care.
We also have to acknowledge that with the technology we have now we are not able to know whether all mental illness manifests in the brain in a way we can see so hinging our worthiness of help and care on the definition is in the end harmful.
TL;DR
" Neuroessentialism is the view that the definitive way to explain human psychological experience is by reference to the brain and its activity from chemical, biological and neuroscientific perspectives. For instance, if someone is experiencing depression a neuroessentialistic perspective would claim that he or she is experiencing depression because his or her brain is functioning in a certain way.” - Schultz, W. (2018)
Neuroessentilism can validate a patient and bring relief of shame short term but ends up contributing to stigmatizing attitudes and thus doesn’t help reduce stigma overall.
The neuroessentialist narrative can downplay the efficacy and criticalness of psychotherapeutic intervention
Neuroessentialist perspectives foster lower empathy levels for patients in medical providers and non-providers alike.
Neuroessentialist perspectives of a patient significantly increases levels of prognostic pessimism which leads to worse treatment outcomes
Neuroessentialism arose because of a real invalidation people feel around their mental health and it is a societal issue we need to work on
We can combat neuroessentialism and stigma by working to make psychotherapy more accessible and talking about our experiences openly as well as giving each other kindness and empathy.
#i tried to make this a readable as possible but shoot me a message if i missed soemthing#neuroessentialism#rant post#mental health struggles#recovery data#psychiatry#medication#psychotherapy#therapy#psychology
13 notes
·
View notes
Text
Suggestions on how to improve fanfic writing:
I was talking with @angelfishofthelord recently (not that recent, time is a concept that escapes our collective grasp) and I jokingly suggested that I make this post. I am in the middle of an insomnia night, so. Here be us.

Characters use the same nicknames and phrases inside their head as speaking. This doesn’t necessarily mean they’re sharing the humor they’re speaking. I.g.: For SPN, I see a lot of people write Dean as a little careless in his POVs, because that’s just how he portrays himself, but Dean, I think, while having a dark sense of humor, isn’t actually very funny in his head. Same goes for MCU and Tony Stark. Funny characters does not always equal happy head space. :)
Nicknames--this used to bother me to no end, because nicknames were never something in my family, and people shortening down the names felt wrong. But you nickname what you love. If someone has given a nickname (and not in mockery) to a character, chances are, they call them that in their head. Like in MCU Clint calling Natasha "Nat", or SPN Dean and Sam calling Cas "Cas" however, with that said, unless the nickname is self chosen, most people will use their full name when narrating. Castiel, Natasha, etc.
Headcanons! This is going to sound a little backwards, but headcanons have always helped me sort between characters. I know that some fic authors are very against headcanons, but to me, you HAVE to make these characters and their world your own, at least a little. You need to understand how their brain functions, and headcanons are a wonderful, wonderful way to do that. So long as you can conceivably fit them into canon, I think you’re good. One of the ones I have about SPN Cas is that he doesn’t actually give off body heat, so he’s constantly room temperature. It’s a detail for people that’s not Cas’s POV to notice. So getting some headcanons like that will help differentiate between POVs because it’s different things for characters to acknowledge.
Mimic writing that you admire. (And ask yourself WHY you like it) I really, really love the way that TFW/avengers team is portrayed in some stories, in others, I’m like “meh.” Write to please yourself, first and foremost, on how to read these characters thoughts. Those who agree with you will flock to be your audience, and they’re who matter.
Language/word choice is really important for POV change. Again, people talk like how they think.
POV change? Treat the character whose POV it is like they are THE most important person in existence. Their reactions get a front seat. Their five senses are your concern. What they notice about a character may not be true, but it's what they notice. They are human, not omniscient, ergo, they'll get things wrong. Even if the story is written with a completely different character in mind, this character is still the most important. POV's time to think, talk, panic, angst, express, etc. That chapter was about how they felt. That’s why sometimes, even if I really do want them to talk or something, a character might think “please don’t say xyz” because THEY don’t want that, and how I feel as an author isn’t relevant here. Remembering that they’re human, and need time to process/react to things is huge.
Practice, practice, practice. It does get easier with time, and effort. I promise. All of you would laugh at my first few weeks of diving into fandoms. That stuff is garbage.
Conscious stream of thought is generally the best way to engage readers, and the most enjoyable. This is how we immerse ourselves into the story. We become a part of it because we follow their thinking. It is always ideal to start where you are the most comfortable, whether that's 3rd omniscient, 2nd person, etc, but, in my opinion, you don't get that true "click" with the characters until you've conscious stream of thought them.
Research. Lots of research. Don't know how long battieres could last in 2002? Look it up. Don't know how to do stitches? Google it. Try to avoid making things up.
Look guys. Everyone understands that you are most likely NOT a doctor or have any semblance of a medical degree. This is fiction. Research what you can, and move forward carefully or vague it out with the rest. The worst that can happen is someone correcting information you got wrong.
Please, please, please stay within the range of human limitation. (Or whatever creature/being you are writing for) You can't lose more than five pints of blood. You CAN die from pain. Infection spreads quickly. I'm sorry. I just. Have read so many fics from newbie writers who push their characters past extremes that is almost impossible. You want to hurt them that bad, break a bone or something. Just. Please try to be realistic. (Don't misunderstand here, I love me some well-done whump.)
Again with the "you are not a professional thing." Those diagnosed with mental illnesses know that you may not be writing from true experience. This is okay. But please, please do not avoid using any words or phrases common with the illness as you try to "vaguely" write it. The more authentic you are, the less likely you will offend someone. Look. I would be so frustrated if someone tried to write about an ED and just... Avoided words like "starve" "binge" and "hungry" because they didn't want to trigger me. Like. Sweeties, I appreciate the thought, I do, but it's more frustrating that you can't even SAY it than actually putting it into your writing. So. Please just. If you're going to write about a mental illness, do so with the intent to WRITE it, not skirt around the bush.
With that, if you are not diagnosed with the mental illness your writing for (or suspect that you have some form of it) that's okay! Google symptoms to get a basic idea, and search for first hand accounts. People's experience is a lot different than the definition. For example, some of the most hilarious people I know are severally depressed, and Google will just tell you they are sad.
Write write and write. You are building a skill. You have to practice that skill frequently.
Do not be afraid to ask for feedback. Betas are wonderful. Asking for advice is wonderful. Being too shy and afraid of criticism for asking for help is perfectly okay. (Hello fellow traveler)
If your search history doesn't have you being watched by government organizations in the next few months, you aren't researching enough. ;)
Take your time. Quality over quantity. Do NOT conform to the update fairy that demands updates frequently. Look. I love my readers. I do. But you HAVE to take your time to finish things in order for them to be worth reading. If this is six hours or six years, that's that.
Do not give everything away. Stop answering questions. We keep reading because we have unanswered questions. Anticipation = good. Knowing everything at once: bad.
Do not put in funny for the sake of funny.
Insults should be insulting, not make people want to cringe and duck their heads.
Dialog should serve as people communicating... Like actual people.
Siblings (unless otherwise said so by canon) DO NOT address each other as "bro" and "sis"
Not a native English speaker? Cool. Natives would love to help you learn their language. :) English grammar sucks.
Analogies should make sense. They should flow smoothly into the writing. If they pop out, you've lost the attention of your writers.
please, please don't glorify rape, racism, homophobia, mental illness shaming/glorification, abuse, sexism, and other crappy things. Thanks. People came for a story, not to get their souls crushed.
35 notes
·
View notes
Text
Busting Dr Cynthia Buliks Injurious Revisionism of Anorexia and Eating Disorders.
By Michael Bench, MEP, WGSGC
1.Can you tell who has eating disorders?
Cynthia says “no”.
Actual Answer: Yes.
Starvation effects are observable and anorexia is cosmetic starvation. Those females with an early eating disorder (EDNOS) or using Anorexic behaviors should be addressed and reported to school staff or counseling for their safety; Crash Dieting is disordered eating even if not a diagnosis and is part of a larger social problem of aversions to patient and honest physical conditioning. Crash diets are the tools of lushes. The very lushes that publish female targeted media promoting cleanses and ‘quick fix tips’. Medical and health advice, if from a document, should only come from academic journals.
2.Are mothers to blame:
Cynthia says no.
Actual Answer: Often
Mothers who have seasonal weight control efforts and use crash diets to cheat their way to a 'beach body” are modeling disordered eating. Crash diets are disordered eating. Mothers involved with pageants have also been known to use other methods like infecting their daughters with tapeworms to reach a desired thinness.
3.Are families to blame?
Cynthia says no.
Actual Answer:Yes.Situationally.
Involvement with sport, social or classist activities that prioritize gender roles before sport itself is a complicity to eating disorders and body dysmorphia. A parent who willingly lets an industry or coach alter her child’s course of physical maturity is actively neglecting their child no matter what the presumed benefits. Families also normalize some seasonal classism, poor nutritional behavior, and poor communication that can be seen in children using anorexic trope behavior and insincere-suicidal attention getting. Mothers who believe their daughters should be paying attention to female targeted fashion media and other retail or pop culture are poorly guarding their children.
4.Is society to Blame? (Far too general. Go home Cynthia.)
Actual Answers: Media is to blame partly in that it protects its advertisers exploitation and revisionism of need/want psychology. Media also forwards health talking points for the unhealthy. The term “weight control” for example is an index case of tolerating a slothful deviant-leisure society who cheat their way to “good looks” simply for summer exhibition. Then they return indoors for winter with their indoor sloth and lazy nutritional rituals.
Coaching & Fashion: Females are not males. Training them as males or believing diet is a form of genetic engineering is magical thinking that can injure the athletes. Instead, minimum ages in sport should be raised so children in gymnastics ,for example, are not used as carnival acts. Lacking a period, a females maturity/fill out has not been “stalled”. She is amenorrheic whether with or without a visible menarche; an event itself that’s been postponed. Females cannot sustain low BMI male thinness to appear his heterosexual-binary-other. In fashion , the binary roles are actually the same , only at smaller emaciated sizes and not androgynous as reported.
Fashionistas who take their model's health for granted as an act of 'luxury artification” are long guilty of endangering her health/assault , among other violations like complicit child trafficking (Set aside whether the female volunteers the risk, the runway’s terms are decided by the foolish and nihilist cosmosexuals having very little competence about human physiology. Respecting ‘who we are” ,eh?) Females normalizing anorexic/disordered eating as a justification of their (model) career or fame are themselves a microphone for social blame.
5.Are Anorexia and Eating disorders a White race problem/Female problem.
Actual Answer: Yes.
The democratization of Western and American market views of ideal beauty and ideal sexuality has not changed the core source of toxic constructions of binary gender. The manipulation of the female body to conform to eras if disinformation and beauty trends, ie Gibson girl and the Heroin Chic waif, show that 'disordered eating' and its long term effects are practiced as luxury fads. Actual mental disorders escalated to Anorexia Nervosa or Bulimia Nervosa stem from European and South Asian religio-social pacts of personal virtue(Breatherism/Inedia). Ever since the first London and American reports of Inedia or fad fasting the practicioners lied about how little they ate. Anorexia, breatherism and inedia have always been appropriate religious rituals used by desperate zealots for attention.. The vulnerability to this sort of radicalization around fasting links to psychological vulnerability and distortions of their self (a specific form narcissistic personality disorder)
6. Consider the remainder of her list debunked.>>(will add the rest later)
>>Anorexia is NOT A CASH COW.
If researchers want to do genomics research, have at. Anorexia itself has provably been found occurring as fads. If the 'formal' uppity journal community don’t have the courage to admit mental illness can be market caused and that the external sphere of society can be toxic.. it is their own failure to confront it and demand regulation. Gibson Girl, Heroin Chic, and proana ‘lifestyle’, are fads whose females are too often seen as ‘victims’ of a male privilege error rather instead their own stubborn choices and long term effects there of : I reject the notion Anorexia should be tolerated as a go-to for researchers that simply need grant money and repudiate those that attempted to distract its identity. The democratization of Anorexia as ‘everyone’s disease’ leads me to be highly suspicious of Buliks motivations as a professional and what diet/pharm companies are handing her NCEEDUS checks.
“ Aye , I hear you was gonna go on a crash diet. You dont wanna be one of those wanna bes.. A real crash diet , ya cut your own brake cables , go for a drive on elevated roads and see how many cliffs you can climb back up from.”
What is Anorexia Nervosa:
Behaviors of Disordered Eating are not themselves the source of the problem. All persons using crash diet and anorexic symptom behaviors however should be considered ‘eating disordered”. Anorexic behaviors are actions of solving a problem the subject appears to suffer even if originally having a healthy proportioned body. Current research suggests that between 3-10 exposures to any message makes an audience more willing to oblige and 'know' its message. This also means a female convinced that eternal youth is where she must rest her physical body to be beautiful is not technically a mental disorder yet. In the struggle to keep her body looking prepubescent the damages of malnutrition and gray matter deterioration lead to distortions of thought. These distortions then create new symptoms, unoriginal symptoms that are signs of a narcissistic depression and helplessness.
Starting at that point for internal pathology....
If Anorexia is a mental illness aside from market learning then it must be recognized a problem of extreme dissatisfaction with the self that has escalated. Anorexia Nervosa , or the most extreme form of cosmetic starvation is then to be recognized : A narcissistic depression formed from the conflict or inability to adapt to adolescent body changes. Social messages denouncing the mature female body and independence may solidify these formerly inert cautions. Further, body changes of the teen are used by marketers to embarrass and humiliate the teen for imperfections; a classic 'witch hunt' scenario of threatening the girl with being burnt at the stake for not being a sexual object. The anorexic is faced with that environment daily; an environment where she has no choice to identify as an adolescent among peers and media , whether she’s ready to adapt or not. There is a clear ‘at adolescence trigger” that points to an adaptation difficulty in a soup of marketing that denounces the aged female as roast beef, spent, junk in the trunk and other negativity.
The Youngest females.. healthy or by pathology would have a difficult time concluding what is good about being female when the unhealthy deposition of fat at the waist and hips is normal for her maturity. That is mainly due to problems in the fitness community media leaving no appreciation for fitness itself. Magazine imagery is purely body sculpted or body building.. actual athletic conditioning with the time allotment it requires.
I am also referring to Anorexia as a form of Gender Dysphoia who's conflicted social and internal views of teen maturity can lead to traumatized states. This should not leave room for stable anorexics or unstable females to characterize the adoption of their injurious methods for 'an in-crowd” elitism.
Anorexia Nervosa and its less severe 'eating disorders.. should actually be called #BodyDysmorphicSIBDieting ( Self Injurious Behavior-Dieting)..It includes caloric restriction, multiple stimulant abuse, dissociative abuse and abuse of prescribed medicines, poor choices in recovery foods which adds to their narcissistic shaming. Pro Ana websites and groups must be understood part of the symptom of a sociopathic “narcissism supply”. Because Anorexia is so well known, applying its known traits can mimic actual anorexics but these body dissatisfied people are factitious disorder candidates. (they are still disordered and mentally unwell. Thereby groups calling themselves pro Ana that taunt new members as ‘wannabes’ are not doing their job as a support group; Support groups and other health resources pages welcome members and hope to spread positiivity. Instead pro ana sites often feature a core group functioning as an exclusive cliq who give merit to the identity of ANOREXICS as it surrounds her; the actual board member is of no consequence. The Pro Ana board is an active process of denial/bargaining by making their narcissist affliction sound positive and trendy.
In no way should statements of recovery or links on these proana sites be presumed to be safe. Anorexia Nervosa is technically an umbrella term for three or more groups necessitating 'shortcutting dieting techniques” to achieve a desireable body. One is truly a mental illness of its own, another is a sociopathic illness that has adopted anorexic traits for its factitious parading.. but is also as serious. Also be mindful that persons starting pro anorexic boards might also be sadists and psychopaths who find artificial arousal in providing a place for harm.
All persons utilizing starvation and self abuse for an undisciplined 'thinspired body” are all heading to the same fatal end; including fashion models. Anorexia in name, in diagnosis, or in method IS STILL ANOREXIA. A refusal of recovery and presumption that anorexia is a lifestyle in name , point to a group still in denial that their practices are injurious. Denial of self failure/deception is one narcissist flaw even if the personality disorder symptoms dont apply to the factitious supplicants
Third is a general category of body dissatisfied females who use encourage each other with SIB Diet techniques rather than actually go to a gym and perform both cardio AND resistance-exercise-for-STRENGTH.. which will infact lead to hypertrophy and better metabolism. This third group is often heckled by the others as fakers and wannarexics. In fact it is the other two groups proving the sociopathic tendencies of their guilt being made manifest on others. Since they cannot empathize, they neither should be empathized. Those yelling 'wannarexics” can be considered social trash and treated accordingly. A combined trait among all 'anorexics' is they mistake strength as an inside characteristic to excuse responsible self conditioning. .. or to justify their fears lifiting weights .. as a behavior is too masculinity defining. Her ego exploits her physical body and the body at times will take back such time to demand fueling.
It is then rightful the ego feels shame but not for eating .. rather for the fasting that causes binging in excess of regular fueling of activity. This singular matter has a strong motivation to be fatally thin and is their excuse to avoid most legitimate forms of balanced physical conditioning. The thinness is of no consequence. Those who intend to crash diet their way to a perfect body will eventually succumb to the cheapness of their diets. There is no diet that achieve what physical benefits come from physical conditioning. Research addressing diet as more important than exercise in weight control addresses a foolish society terrible at both.
MB.
2 notes
·
View notes
Text
DISCLAIMER: I have signed a waiver and become a contributor to an upcoming book by a fellow, healed Lyme patient. Some or all of this story may be published in the coming months. I have added and updated some of this information 9.12.2020, so hopefully I will not violate any copyright laws.
NOTE: Do not assume everything I write here or on my Facebook Lyme page will help. Everyone heals differently. Working with a knowledgeable, sincere doctor and finding the right combination of medication, herbs, personal lifestyle and diet changes will help. One size doesn’t fit all for Lyme disease treatments. Don’t be afraid to research and consult with your doctor. Get a notebook and write down EVERYTHING; diet, exercise, symptoms, dates, times, and ANY physical or emotional stress-causing events. Stress seems to be the biggest culprit of all diseases. Hypocrites stated, “All disease begins in the gut”. HE WAS RIGHT!!
NAME: Kathleen Meyer
I live in Northern VA. I am a retired, 60+ year old Grandmother. I am widowed, and I was living alone when Lyme hit. Symptoms began between September 12-14, 2012.
BACKSTORY: September 12, 2012. I felt something prick my lower back. When I reached around to check, the area was very hot to touch. This was in my car in Reston, Virginia, on a 90+ degree day. I had left the car windows open slightly during the work day.
The previous two weeks, I had been on vacation to the Pacific Northwest, to visit my Sister. While there, I visited a national park, which is highly populated by deer and other furry animals; large and small. There was hiking and a few photo ops while sitting on a rock wall. Deer roam around freely in the town where my Sister lives.
After going to my family doctor almost daily between 9/14-10/12 to complain of strange symptoms, I was finally tested for Lyme, West Nile virus and Rocky Mountain Spotted fever. My doctor was skeptical at first, but I kept insisting the symptoms weren’t normal for any flu I had ever had. When I mentioned living by woods and recently spending time in a national park, I was taken more seriously.
I was diagnosed with Lyme on October 12,2012, (clinically by relating symptoms) and blood work. Side note: Because I had Mono at age 18, I was also diagnosed with Mono “exposed”. I was instructed to go home, stay on bedrest and get clearance from an infectious disease doctor, before returning to work. I was on sick leave and coworker’s leave donations between 10/15-11/13/2012. I was also instructed NOT to work or look at work email while out sick; which I now understand completely. The philosophy seems to be, “Being out on sick leave means you’re too sick to be at work, so don’t try to do any work at home”. Never mind that after two weeks of bedrest, going stir crazy and wanting to do something, is very normal.
TREATMENTS: I was immediately placed on Doxycycline 200 mg, by the family doctor, for 20 days. That didn’t work. Then Doxycycline 200 mg for 10 days. When that didn’t work, there was 30 days additional. When I ran out, I waited between prescriptions about a week or two, to see if symptoms would come back. Symptoms kept coming back. I was on/off Doxycycline for a total of 60 days. My insurance company wouldn’t authorize more than 60 days, so I was given Cefuroxime 500 mg for 30 days.
NOTE: At the beginning of the Cefuroxime prescription I doubled the dose for the first 4 days, just to see what would happen. I realize that wasn’t a very smart thing to do, but I wanted to kill what was making me so sick. After the 4 days, I used the prescription correctly. At the end of the 30 days, no symptoms returned.
NOTE: I always eat yogurt in between any oral antibiotic dose. The reason is because all antibiotics kill all bacteria, including the beneficial bacteria we need in our gut, where the main part of the immune system is located. The other part of the immune system is our brain. The brain and gut communicate with each other UNLESS we have an illness like Lyme. The brain is affected and doesn't communicate correctly with the gut during Lyme, and probably during other autoimmune illnesses.
MYSTERIOUS SYMPTOMS BEFORE TREATMENT: High blood pressure, cardiomegaly, chronic bronchitis, prolapsed mitre heart valve, GERD, Barretts esophagus, large hiatal hernia. Other symptoms; short term memory issues, difficulty with vision, floaters, reading, sensitive to bright light and sunshine. Difficulty walking, bumping into walls, problems with grip and dropping things. Insomnia, sometimes several nights in a row. Constant buzzing, tingling, pain throughout my entire body. Chest pain, head and neck pain, difficulty with bowels, difficulty swallowing and anxiety from feeling so ill for no known reason, except Lyme. I was able to swallow correctly again, after an endoscopy and scraping of webbed growth (non-cancerous).
WHAT THE WORLD NEEDS TO KNOW: ALL doctors, nurses including E.R. personnel need to be made aware of how many hundreds of symptoms Lyme can have. It is known to mimic at least 400 other illnesses and syndromes. Millions of people worldwide are being mis-diagnosed or given catch-all diagnosis out of frustration. Doctors have about 15 minutes per patient and don’t have time to research and address everyone’s symptoms. More research is needed and the patient’s symptoms need to be taken more seriously. The phrase “The customer is always right”, needs to apply to patients as well. Haphazard treatment of symptoms and covering up symptoms DOESN’T WORK FOR LYME!!
NOTE: Most medical schools are funded by big pharma. They do not provide enough education to upcoming doctors about Lyme and similar illnesses. They don’t stress enough on nutrition or healthy eating as a benefit to patients. I have asked my doctors and chiropractor about this, and they said the same thing.
Do NOT listen to any doctor who tells you your child has “Growing Pains”. Find a doctor who is knowledgeable about Lyme, preferably a young doctor with a growing family of his/her own. My family doctor diagnosed and treated me correctly, was THAT doctor, not a specialist, a general practitioner.
HOW HAS LYME CHANGED MY LIFE; GOOD AND BAD: Lyme caused me to be bedridden for over 3 weeks, afraid to drive for fear of getting lost, and feeling like I had early onset Alzheimer’s. I now feel that it was an eye-opening experience, which awakened me to how poorly I had been managing my diet and exercise on a daily basis. I also believe the 2012 influenza shot might have been flawed, because I never felt healthy after that, and it possibly weakened my immune system so Lyme and Mono could sneak in.
I went from quick and easy meals and very little exercise to self-improvement. I learned from the Lyme pages on Facebook from reading other people’s stories. It was almost like putting a really large jigsaw puzzle together, very slowly and not having all the pieces in front of me.
SOMETHING I DO NOW THAT I NEVER DID BEFORE LYME: I now pay closer attention to my physical and emotional health, what foods I eat and the amount of daily exercise I get. I also developed pre-diabetes type 2 during the Lyme period. I am now eating real food and watching my weight in order to keep the pre-diabetes under control, without medication.
NOTE: Doctor’s won’t tell you unless you press them, that medication for everything is NOT the best way to control anything, because you’re stuck on the medication for the rest of your life. Our bodies are capable of healing, with help by US.
THE MOST FRUSTRATING PART OF LYME DISEASE: I would have to say, lack of compassion for what patients are going through on the part of medical professionals, insurance companies, news media, and the general public. “Take these pills and you’ll feel better”. This doesn’t work with Lyme disease; trust me. However, I know many people who believe everything their doctor says and I hear, “My doctor says it’s__________. More research is needed and the actual CAUSE should be researched and treated instead of pills to cover up underlying symptoms.
MY BIGGEST SUPPORTER(S): I have a private Facebook page called “Where is Lyme Disease”, which has 249 members. I consider all of them to be my supporters; we support each other. I have been posting there since March, 2015, before any of us realized Lyme is EVERYWHERE!! I HAVE POSTED HOW I TREATED, HEALED AND WHAT I AM DOING NOW TO STAY HEALTHY. Those answers were not readily found using an internet search in 2012. Everything I post on the page is from what I went through. I am trying to help others with Lyme get through it and not give up.
I give all credit to healing to authors of books about Lyme struggles. There are too many to mention, but “Cure Unknown” by Pamela Weintraub was the best one. I read it several times, because the first time I tried to read, the words ran together and blurred because of Lyme. I am now able to read again, and have re-read several books I couldn’t comprehend before. If there’s a diagnosis of ADD or ADHD, suspect Lyme!!
BIGGEST DAILY STRUGGLE: Praying it never comes back and thanking God for every day which I am granted. Experimenting with different diet plans and keeping healthy. Getting away from white sugar, white flour and other overly processed, easy to fix foods and getting real food into my body is a daily challenge.
Continuing to learn about and helping others deal with Lyme. I have helped quite a few people NOT give up. I wish I could help everyone or was a millionaire so I could donate money for a cure.
3 notes
·
View notes
Text

As someone who works in medicine and someone who is a parent, the case of Justina Pelletier really interested me, and troubled me as well.
...
Justina Pelletier was brought to Boston Children’s Hospital at age 13, after testing and treatment at another hospital in Connecticut failed to resolve her health issues. Justina was born prematurely, and her parents reported she had experienced subsequent developmental delays and pervasive illnesses. At Boston Children’s, Justina presented with difficulty walking and talking, pain, and altered mental status. Doctors could find no medical explanation for her symptoms, even after extensive neurological testing. Eventually, they came to believe she may have suffered from somatoform disorder, in which psychological problems create, or exacerbate, physical problems.
There was also reason to believe Justina might be experiencing a form of medical abuse called factitious disorder by proxy (previously called Munchausen by proxy). Justina’s parents’ reported obsessiveness over her health, the multiple diagnoses they had sought, and the tangled network of doctors involved in her care all signaled possible “over-medicalization.” It was further documented that Justina seemed to be in better physical and psychological health when her parents were not present.
It was not just Boston Children’s providers who felt Justina’s parents may have contributed to their daughter’s poor health. Justina had previously received extended treatment at Tufts Medical Center, where doctors diagnosed her with mitochondrial disease but also observed both the psychosomatic severity of Justina’s symptoms and the possible barriers her parents may have created to her recovery. After Justina’s parents proved resistant to addressing the psychological aspects of her illness as well as the medical, the team at Tufts filed a report of medical child abuse with the Department of Children and Families in Connecticut.
As the providers at Boston Children’s struggled with how best to help Justina, they worked together with providers at Tufts to create a treatment plan for Justina, one that would address her mental health, help foster her independence, and minimize her parents’ involvement in her medical management. Justina began receiving intensive inpatient psychiatric treatment at Boston Children’s, but after a few days, her father demanded her release. Boston Children’s then initiated a report of medical child abuse with the Massachusetts Department of Children and Families. DCF took custody of Justina, authorizing her continued psychiatric institutionalization for nine months, with limited contact with her parents, before she was returned to the custody of her family.
In 2016, Justina’s parents sued Boston Children’s (and the doctors who treated her) for malpractice, alleging her treatment and limited contact with her parents caused PTSD in Justina and violated their family’s civil rights. Justina herself was adamant in her testimony that her hospitalization was a negative experience. After nearly four years of legal proceedings and a five-week-long trial featuring wildly varying accounts of Justina’s treatment and its effectiveness, a jury took six hours to rule in favor of the defendants, dismissing the Pelletier family’s suit. Now 21, Justina lives with her parents, who continue accompany her to hospitals in multiple states with complaints of undiagnosed illnesses. Her treatments, which include the removal of her colon, have been unsuccessful in alleviating her symptoms.
...
Again, as a mother, the idea of one or more hospitals and state agencies swooping in to override my concerns is troubling. But, as someone in the medical field, I’m troubled more by the fact that medical child abuse is not at all rare. In just the past six months I’ve encountered more than one child victimized by their parents’ factitious disorder by proxy, helpless as their parents doctor-shop for the specific tests, diagnoses and medications they want their child to receive. I’ve also interacted with dozens of children whose parents are guilty of (in my opinion) a different type of abuse, in which they willfully withhold appropriate and necessary medical treatment in favor of the latest designer diagnoses (or wastebasket diagnoses, as clinicians might say) and the corresponding “holistic treatments” that actually keep their kids sick. So, with that in mind, in these kinds of cases my bias tends to lean toward the medical professionals - especially when it comes to pediatric practitioners, who have no motivation beyond trying to make children well. Parents may (and typically do) love their kids, but that doesn’t qualify them to diagnose and treat these fragile humans entrusted to their care.
#justina pelletier#factitious disorder#factitious disorder by proxy#munchausen by proxy#munchausen syndrome#child abuse#medical abuse#child neglect#medical#tales from healthcare#personal#rant
4 notes
·
View notes
Text
[one-shot] say nothing more, baby
Pairing: implied Yamato/Taichi from Digimon Adventure
Rating: pg-13, tw: Character death, Hanahaki disease
fic inspiration from the song “like i need u” by keshi.
—
laying in bed waiting for your touch
Restless, tossing and turning
in the dead of the night, ears ringing
stay with me
nauseous, dizzy
eyes growing misty
i don’t want to be alone
filled with regret
wanting to reset
you don’t need me like i need you
yellow carnations bloomed,
these unwanted feelings consumed
wish we never met
left the boy torn, dragged through the mud
petals tainted by splotches of blood
pain, that’s an option
an inevitable infection
trauma inflicted on the destined
—
Yamato Ishida was stunned.
Lost in the confines of Tokyo U Hospital, the blonde felt lost in the eerie feeling the sterile white walls gave. Takeru was by his side when he received the call from Hikari. Speechless, with his lungs threatening to collapse after running into the unfamiliar building, especially upon hearing the news from his best friend’s little sister, whose voice was hoarse on the phone and reduced to mere whispers, as if she had just mustered up the strength to speak on the phone after sobbing relentlessly, informed them that his best friend was in the hospital.
His best friend, Taichi.
His partner-in-crime aside from Gabumon, his comrade, his best friend, his inspiration.
His exuberance, a demeanor akin to no other, shined brighter than a thousand suns. His smiles and laughter imprinted in his memory, alongside the desperately thrown fists and tears, reminded him of home.
For a disease that is allegedly produced in fictional Japanese literature, a disease that is observed to have been a direct result of unrequited love. The physical manifestation of the psychological pain, exacerbated further by heartache, was akin to somatoform disorders, but the disease had limited primary research findings on it as to the origin of the disease. Perhaps, this just served as a cruel reminder that God ceased to care.
Hanahaki disease, a disease ultimately caused from prolonged and extreme pain as a direct result of grieving a lost, unreturned love; painfully beautiful, it was equally fatal, with patients dying within mere days. Going from perfectly healthy, to frail and on the verge of death, all from an unreciprocated love. .
Hikari found out, after finding Taichi collapsed in his room in the late afternoon, with blood and petals left at the scene. Next to him, was the referral from the doctor’s.
Prognosis: severe case of alleged Hanahaki disease.
Duration: onset of disease, 2 weeks with the patient remaining mostly asymptomatic. Flareup occurred on March 4.
Symptoms: Coughing, blood in sputum, dizziness, nausea, fever, mood swings
Condition of patient: requires immediate treatment as soon as possible. Dr. Narukami M.D. at Odaiba General Family Clinic referral to Tokyo U Hospital. Immediate surgery recommended within 1 week, otherwise proven fatal, may result in asphyxiation due to uncontrolled growth of yellow carnations in lungs.
It was a cruel reminder, that fate was never on their side.
They were chosen as children to be the Digidestined, thrown into the Digi World; they were merely children whose clothes were far too big for them, children whose appetites exceeded their stomach capacity, children who were burdened and pressured as result of their parents’ problems and the weight of the world on their shoulders.
Feeble attempts to return to their world, turned into a mission to save both the Digi World and their world. Achieving the impossible, such as going through worlds via portals or a digital device to fight infected Digimon served as a reminder that in their world, the impossible could very easily be feasible. Taichi was resilient, he was a natural born leader. He was an athlete, his immune system stronger than no other, his appetite overwhelmingly large as a growing boy, his demeanor and boisterous laughter so full of life.
Yet, Yamato could not help feeling shocked.
Pale, with a weary smile that masked the pain, Taichi appeared sick, decrepit, and so, exhausted. Feeble attempts to muster up greetings, and reassurances to not worry, since he felt fine, and that he had accepted the outcome. The outcome that his love had not returned his feelings, the love whose identity remained unknown to Yamato. It was too late for preventative care, Taichi had refused to come in for early checkups, and the buds had sprouted into fully grown, beautiful carnations. Carnations that were equally deadly, unfortunate, and tragic.
A mixture of resentment, bitterness, mirth and frustration bubbled in his chest. Yamato was puzzled. Who could Taichi possibly be so in love with, that his love had left him incapacitated? Who would not return their feelings for the brunette boy? Shaking his head, Yamato recollected himself, but his thoughts were interrupted by a series of coughs.
If he did not know that Hanahaki disease was not contagious, he would have thought the persistent scratch and gnawing at his throat was a sign.
The image of Taichi laying in his hospital bed was burnt into his memory, as he quickly was escorted out of the room. One of Taichi’s coughing fits had erupted, so Hikari and Takeru quickly rushed out into the hallway to call the nurse. With blood staining the corners of his mouth, and full blown flowers blooming, Yamato could never forget the image imprinted into his memory of the boy who was reminiscent of courage, ambition, and hope. The stems and leaves filled his esophagus, the sprouts depleted his already limited air supply, and petals covered by blood and bile filled the bucket next to his bed; the damage had clearly taken a toll on the boy, and fast. The nurses escorted Yamato out, reuniting him with Takeru and Hikari, who were lucky to not witness the emptiness in Taichi’s eyes, almost as if he had expected this outcome, but did not let anybody know, due to his stubbornness. Taichi, whose voice was painfully hoarse, made feeble attempts to speak to Yamato, despite his earlier coughing fits. Yet, the following words he muttered left Yamato in an intense flurry of emotions,
“Yamato, please go.”
—
Patient ID: 4242564
DOB: 05/19/19XX
Patient Name: Yagami, Taichi
Diagnosis: Hanahaki Disease
Treatment: Immediate surgery to restore respiratory functioning. Requires removal of yellow carnation flowers from lungs, which are constricting air supply.
Expected recovery: If successful, 7-8 months with rest, close monitoring from family members in case of flare ups.
The paper that Hikari was holding, despite being a thin sheet with printed letters, felt like a quick dose of reality. Hikari called her parents, giving them updates, and the address of the surgery unit. Her parents, frantic and deeply afraid, just as they were when they heard that the kids were returning to the Digital World as mere children, had a semblance of hope amidst their worries. They wanted to put their trust and faith into the medical professionals at the highly-esteemed hospital.
They had giant digital dinosaurs and birds appear in Odaiba. How far-fetched was this disease occurring in their world, really?
Yamato felt torn. Usually, the two were able to communicate non-verbally; after all, Taichi wore his heart on his sleeve. Yet, this time, he simply could not understand. He did not even know that Taichi even loved someone, to the point where he had secretly gone to the doctor's and hid the fact that he needed immediate medical attention. He endured the pain to the point that Hikari had found him cold and lifeless on the floor with the petals scattered around him; the thought of the flowers taunted him, and reminded him of his friend, whose demeanor was untypical of the brunette. The unspoken communication between them bewildered Yamato, and scared him.
Knuckles growing white, his tight grip crumpled and threatened to rip the sheet of paper. Jaw clenched, tears threatening to spill, Yamato was so tense, and furious that the world was against them, and had decided to hurt his friend, his formerly abrasive and reckless friend whose compassion and courage had saved hundreds, if not thousands of people. His friend, whose stubborn nature, was easily just as self-sacrificing and selfless, had demanded his best friend to leave the room, so that he would not have to see him in that state.
With a mirthful chuckle, Yamato wiped away at his tears, which threatened to spill at any given moment. His vision was blurry, and the noise coming from the bustling hospital was deafening. Bitterly, he thought to himself, denouncing the way that movies portrayed grief. His world of color did not come to a halt; traffic lights beamed, and the city of Tokyo was still lively as ever. His world of color, instead was muted, and it was difficult to concentrate on anything. He had dropped everything he was doing, when he received the call from Hikari. He couldn’t stop thinking about Taichi, and his bleary eyes, raw from the hours of crying in the waiting room, failed to shield him from his obstructive thoughts in facing this cruel reality. Hikari was sobbing, almost hysterical. Takeru comforted her, holding her closely, his tight embrace and face buried in her shoulders indicator enough that he was just as distraught. Taichi’s parents rushed into the emergency room, demanding to be at their eldest son’s side. Demanding answers, the duo were frustrated, as to why there were no other forms of treatment, or medication.
To this, the nurses shook their head, despite the couple’s insistence. Taichi was transferred to the intensive care unit of the Tokyo U hospital, and the nurses informed the Yagamis: Taichi, in an unconscious state, is physically unable to consent to the procedure. It was up to the Yagami family to decide whether they should proceed or not. The implications of the surgery was that Taichi would possibly never be the same afterwards, his lungs were salvageable, but his memories would be in fragments.
With such an intrusive procedure, it was difficult to tell how Taichi’s body would heal afterwards, or if he had a strong chance of surviving it. Yet at the same time, this was life-or-death. Hikari, after maintaining her composure, softly asked the questions everyone was thinking,
“Could we please see him? Will he be okay?”
This was all because of deceivingly harmless yellow carnations. His louder-than-life friend, who effortlessly ran from goal to goal and led his football team to victory, was the same person who passionately sprinted across the Digital World to save his friends; this same person looked unrecognizable, frail, and passive. All because of some flowers.
Yellow carnations, the flowers representative of rejection, bitterness, an unrequited love, are simultaneously considered the flower of friendship.
As if time went still, the low-light fluorescent fixtures of the hospital building and the vision of the Yagami family and his brother grew hazy. Yamato felt a sharp, sudden pain in his chest. Unable to hide the discomfort on his face, he excused himself as to not worry the others.
In the restroom, even with the dim lighting, the scene before him was unmistakable.
Orange petals accumulated in the sink, and he was left breathless.
After a quick google search, he realized the cluster of orange petals consisted of marigolds. Marigolds symbolized strong passion, being associated with a legendary brave and courageous lion.
At the same time, they represented cruelty, grief, and jealousy. How ironic.
Fate really was mocking him.
—
no time for nonsense
courage and friendship
a will weaning, weaker than his grip
can’t ask you nothing
grip on this fate
a fate he realized too late
drank, feeling nauseous
Scared and breathless
Oh, he could never guess
too many toxins
to the last beeps on the monitor, the angels sing
yet, what’s left is this scratchy, lingering sting
not even conscious
sheets blood-stained red
regret, from words left unsaid
say nothing more, baby
unvoiced emotions which undoubtedly dictate
the harsh decisions made at this rate
say nothing more
#j9 writes#digimon#taichi yagami#yamato ishida#tai kamiya#matt ishida#digimon adventure#oneshot#taito#yamachi#taiyama#hanahaki disease#they’re in high school so expect teen angst#tw: death#tw: character death#one-sided love
13 notes
·
View notes
Text
On the road again
Sorry this took so long to post. I’m having immense difficulty with screen time right now, so writing and editing are both very slow (especially with this 6k-word fic). It pretty much mirrors my recent time in hospital, so if you’re interested in what’s been going on with me lately, well, there you go.
Thank you to the amazing DD (@mohini-musing) for all the editing help.
Set in the Whoa Bessie ‘verse. TWs for needles and hospitals.
_____
It starts when James falls to his knees beside the breakfast table clutching his head. He’d gone to bed with a headache, but this is definitely an upgrade, and an impressive one at that. Steve whips around from where he’s burning the fried eggs and automatically reaches for the rescue seizure meds.
“Hang in there, Buck,” he intones.
“Mm,” James groans in response. “No, I’m--”
“Hold on, I’ve got your meds,” Steve says.
“No, I’m ok,” James repeats. “Just--”
“Bullshit.”
“Pain,” he grunts. “So much pain.”
“Where?” Steve asks. “Still your head?” He abandons the spatula and drops to a squat at James’s side.
“Yeah,” James croaks. “So bad.”
“This isn’t a seizure, is it?” Steve asks.
“No.” James makes to shake his head, but his eyes flood with tears. “I’m sorry,” he murmurs.
“What?” Steve uses his thumb to wipe the moisture away. “Don’t worry about it. Well, I’ll worry about it.”
“No, don’t,” James tells him with a hitch in his voice. “It just… really hurts.”
“Like, Excedrin hurts?” Steve asks. “Or Imitrex?”
“Um,” James gulps. “Neither.”
“What do you mean?” Steve’s eyes go wide. “Like, worse?”
James nods and bites his lip.
“Jesus.” Steve grits his teeth. “What do you want me to do?”
“I don’t know.”
“You want to lie down, maybe?”
Steve meant on the couch, but James gets clunkily down on his side on the kitchen floor.
“That can’t be comfortable,” Steve comments.
“‘S not, really,” James replies. He pulls his legs in toward his chest and cradles his arm around his head.
“What do you want me to do?” Steve asks again.
“I-- Just--” James stutters.
“Um. Here.” Steve stands and runs a dish cloth under the faucet. He pauses to turn off the slightly smoking burner before returning to James’s side and laying the towel across his forehead. “Better?” he asks, a bit stupidly. He knows it can’t possibly make a dent in a headache this bad, but it doesn’t stop him from trying.
“Ugh.” James grinds his teeth and lets out a strangled moan. “It’s just… the worst headache…” He gulps and nearly gags, but his stomach is empty and nothing comes up.
“Ok, um--” Steve gently pulls James into a sitting position, hanging his head between his knees. “It’s gonna be alright.”
“Mmph.” James gives a nauseous grunt.
“Is it like a stabbing pain? Or constricting?” Steve asks, well aware that he has no power to diagnose.
“I-- I don’t--” James does gag this time. A thin stream of bile dribbles down his chin and onto the floor.
“Ok.” Steve uses the towel to wipe him up. Then he throws caution to the wind. “Do you think you’re having an aneurysm?”
“Fuck,” James spits. “I don’t know.” He wipes his mouth on the back of his hand and gingerly maneuvers himself out of his own mess. “How am I supposed to know?”
“Good point,” Steve says with a sigh. “If you’re hurting that bad, though, we should go to the hospital.”
“Fucking go to bed,” James sputters.
“I just,” Steve nervously chews one thumbnail. “I just can’t let you do that.”
James starts to roll his eyes, then clutches his head in agony.
“See, I don’t want you to lie down and not wake up,” Steve says quickly.
“Yeah, I--” James gulps convulsively, sweat forming on his brow. “Ok. Fine.”
Steve leaves him on the kitchen floor for two minutes while he throws on jeans and digs up phones and wallets for both of them.
“Alright,” Steve says, “Come on.” It takes most of his strength and all of his grace to get James off the floor without winding up on his own ass. There’s a stain of stomach acid on James’s thigh they both pretend not to see as Steve supports him out to the car.
James leans his head back against the headrest immediately and closes his eyes.
“Not far,” Steve tells him. “Not far at all.” The closest ER is just around the other side of the VA hospital where they both spend most of their days. Steve has little idea who’s on during the dreaded weekend shifts; in fact, he barely knows the hospital aside from his own department and the staff in the cafeteria. He trusts the hospital, though. It’s highly rated for the area. At least he thinks it is. Though Steve may just be making that up to make himself feel better.
The drive only takes a few minutes. Steve parks in the staff lot, which is closer, hoping to all deities that nobody cares that it’s the wrong day for him to be using his permit. He runs around the front of the car and opens James’s door, then throws the man’s arm over his shoulder and helps him toward the entrance to the Emergency Room.
They dodge an ambulance pulling up to the bay and slide through the double doors.
“You need to be seen?” asks the gum chewing receptionist as soon as she lays eyes on them.
“Yeah,” Steve says, gently clapping James on his stump.
The girl directs him to a seat and asks his name and address, which Steve happily provides while James goes back to clutching his head.
“And symptoms?” The girl inquires.
Steve looks at James. “Severe headache.”
“How would you rate your pain on a scale of one to ten?”
“Um.” James swallows and lifts his chin. “Nine?”
Steve assumes it’s only his past experience with hospitals and surgeries that keeps James from saying ten.
The receptionists nods, unimpressed, and sends them into the waiting room.
They make it through vitals and registration without incident, though James’s blood pressure is high and his heart rate is through the roof. He starts to gag again when the tech puts the thermometer under his tongue, but a well-timed swallow keeps everything in place.
“How’re you holding up?” Steve asks when they’re relegated back to the waiting room.
“Hmph,” is James’s curt reply.
The folks in charge of triage seem to know their stuff, and it’s only a few minutes before James is called back again. He eschews the proffered gown and lies gratefully on the paper-covered cot.
“Aw, Buck,” Steve murmurs as James closes his eyes.
“Ow,” James groans.
“Should I be quiet?”
“No. Just, ow.”
Steve reaches for the light switch beside the door and flips it to the off position. “Is that better?” he asks before sitting on a spindly chair in the corner of the room.
James makes a dull sound of assent.
They get an entire minute of peace before an EMT comes bursting in, toting a huge gear bag and flipping the light back on.
“What’ve we got here?” the man says loudly, tucking his long golden hair behind his ear.
Steve cringes, and he hears James’s teeth clench from across the room.
“Um,” Steve says slowly, blinking as if in morse code. “Really bad headache. Really bad.”
“Headache, eh?” the EMT repeats. “First line of defense is always hydration.” He pulls the duffle off his shoulder and removes a clear bag of fluids, then begins opening packages of tubing and needles.
Steve recognizes all the makings for an IV, and it seems James does too. He groans and deflates, dropping his chin to his chest and pulling his arm in close.
“Geez,” Steve breathes, standing up to hold James’s hand. He realizes a moment too late that he’s being the opposite of helpful, James having only half the average number of easily accessible veins. “Look at me,” he says instead, going in to cup James’s chin. “Look at me, Buck.”
James obliges the best he can. He trains his eyes on Steve, and they slide out of focus before coming to rest somewhere in the region of Steve’s eyebrows. “Ok,” James whispers.
He blinks dazedly when the EMT rolls up the sleeve of his shirt. Steve’s glad James is wearing one of the tailored ones that only has the one sleeve, lest he give the whole of the staff the shock of their lives.
“Be gentle,” Steve says, probably unnecessarily. “He’s in pain.”
“Of course, man,” the EMT replies, though not quietly. He pushes James’s sleeve above the elbow and begins to feel for veins. “This will be tight,” he warns before pulling the tourniquet around his bicep.
James gives a strangled hum in response. Steve watches as his coarse arm hairs catch under the thick rubber band.
“Gentle,” Steve mutters again, but the EMT is already prodding at the veins in the crook of James’s elbow.
James practically growls at him, grinding his teeth and clenching his fist.
“That’s it, my man,” he has the audacity to say. Then, “Shit, no.” The EMT digs one-handedly in his bag and pulls out a thick pad of gauze and a length of coban.
Steve isn’t sure he wants to see the results of the shoddy handiwork, but he gets a glimpse of the already spreading bruise before James’s arm is bandaged up.
“What the hell?” It’s all Steve can do to keep from telling him off further.
“Don’t worry,” says the EMT. “There are plenty more veins. Like… Here” He rotates Jame’s arm and points to one midway between elbow and wrist. “Or...Here.” He points to the back of his hand.
“Right.” Steve fights the urge to roll his eyes. “Can we just,” he starts, going for his kindest tone. “A nurse, maybe? Or a doctor?” Even if this EMT wasn’t doing such a lackluster job, he’d still want James in the hands of the most highly trained medical trained professionals around.
“I got him,” the EMT says, tapping another vein. “This is a good one.”
“OK,” Steve sighs. He looks back to James and touches his stump shoulder, which he realizes is shaking. “It’s ok, Buck. It’ll be ok.”
“Mm.” James barely nods.
“Little poke…” the EMT murmurs.
It probably is just a little poke, but James’s entire body convulses in a flinch he does his best to control.
“It’s ok,” Steve repeats again. “Look at me, Buck, just look at me. You’ll be ok.”
“Yup,” James replies with a groan, his eyes and lips wet.
“You alright? You feel sick?” Steve knows the questions are stupid, but he wants to know the answers nonetheless.
“I’m fine,” James breathes in a choked whisper. “Don’t--” He stops to swallow. “Don’t worry about it.”
“Aw, c’mere.” Steve opens his arms, and James immediately leans in, placing his head against Steve’s chest. Steve feels his shallow breathing and resists the urge to give him a comforting cuff on the shoulder.
“Ok, that’s that,” the EMT says authoritatively, tearing off a piece of tape and smoothing it over the plastic catheter in the back of James’s hand. He loops the clear tubing and adds another strip for good measure. “Nurse and NP should be in momentarily. If you need anything in the meantime, I’ve been Aaron.”
“Lights back off, maybe?” Steve suggests. He looks to James. “It helps, right?”
“Hm,” James says into the front of Steve’s shirt.
“Sure thing.” Aaron catches the light switch and steps out.
There are a few minutes of blissful silence, during which Steve mulls over the EMT’s words. He definitely referred to a nurse practitioner, not a doctor. That removes any hope that he had of seeing doctor Hill, the wonderfully gentle MD who’d treated James the last couple of times he’d wound up in the ER.
“Hang in there, Bucky,” he says, two seconds before the door bounces off the wall with a crack loud enough to raise the dead.
James burrows further into Steve’s chest, and Steve wraps his arms around him. The light flips on again as a tall shadow enters the small exam room.
“Fuck,” James mutters around a queasy gulp.
“I’m Brock,” says the shadow. “Your NP this morning. What brings you in?” He sounds more like a hotel clerk with a bad attitude than a medical professional.
“Rumlow, wait!” A nurse comes skidding into the room, his sneakers squeaking on the polished tile floor. “This one’s a status migraine.” The young man pushes his blonde hair out of his eyes and gives Steve an apologetic look. “Hi. I’m Pietro.” He looks back to the NP and mouths, “Be gentle.”
“Ok, ok.” Brock lifts his hands innocently. “So, your head hurts?”
James nods into Steve, so Steve gives the verbal “yes” for him.
“Alright.” Brock sits loudly on a rolling stool as Pietro stations himself behind the computer. “I’m going to ask you some questions,” he says in a bored voice. “What’s your name?”
“James… Buchanan… Barnes.” The pain is evident in James’s voice.
“Date of birth?” Brock presses.
“March tenth--” James swallows hard and falters on the year.
“Eh, close enough,” Steve decides.
Pietro seems to agree, giving a quick nod and an affirmative keyboard clack.
“Ok.” Brock regains control of the conversation. “Where are you this morning, James?”
“Um.” James adjusts his position and furrows his brow. “Here?”
Steve sighs. ‘Oh no,’ he thinks. The staff seem convinced this is just a bad migraine, but should James really be so confused. Should he really be hurting so much?
“Here,” Brock repeats.
Pietro types a note.
“Ok,” Brock says. “And why are you here?”
“Uh.” James takes a breath. “2019?”
Steve shakes his head. There’s only one excuse for this one. “He doesn’t have his hearing aids--” he starts.
Brock holds up his hand. “You’re sure this is a headache?” he asks, raising an eyebrow. “You’re sure he’s not having a mental breakdown?”
“What?” Steve nearly loses his grip on James. Even Pietro seems to stop typing in surprise.
“This, you know,” Brock gestures with his pen. “Episode.” He puts a spin on the word that makes his opinion clear.
“No,” Steve says immediately. “And trust me, I would know.”
“But he’s sick, he’s panicky, you bring him to the ER--”
“Yeah, because I don’t know what’s wrong with him,” Steve interrupts. “Because I want to make sure he’s not having a fucking anyeurism! But I’m a psychologist, and trust me, I know a mental breakdown when I see one.”
“Alright,” Brock huffs as he stands up. “Fine.” He takes a step toward the door. “Order MRI for this one, then have Dr. Pierce read the results. I’m recommending admission; I just haven’t yet decided which ward.” He leaves the room, and the door clicks shut behind him.
It takes all of Steve’s strength not to give the NP a good cursing out. Instead he refocuses on James, burying his nose in the waves of his hair.
“I’m so sorry about him,” says Pietro, moving out from behind the computer. “He’s not normally quite that rough around the edges…” He trails off with a shrug.
“Couldn’t imagine working with him on the daily,” Steve says honestly.
“Well, you get used to it.” Pietro shrugs. “As soon as he finishes with his MRI, we’ll set him up with some painkillers. A good migraine cocktail, some magnesium, maybe, or some steroids--”
He’s cut off when a transport technician arrives with a wheelchair. The man’s nametag reads “Hogan.” “Barnes for MRI?” he asks.
“Yup,” Pietro says. He looks to Steve. “Want me to help you transfer him?”
“That would be great, actually,” Steve replies. He grips James’s hand, careful not to disturb the IV line, and shifts him toward the edge of the cot. Pietro loops an arm around James’s waist and supports half his weight as Steve steers him upright.
They make an ungainly three-point turn and settle James in the wheelchair. He immediately lists sideways toward Steve.
“Ok, Buck,” Steve murmurs. He cards his free hand through James’s hair and presses a quick kiss to his temple.
“He’s real lucky to have you,” Pietro comments, hanging James’s IV bag on a pole above his head. “If you don’t mind me saying.”
“Oh, of course not,” Steve says quickly, feeling himself go pink.
He begins to walk into the hall beside James’s wheelchair, but he’s stopped when the transport tech’s arm hits him in the chest.
“You can’t come back that far,” Pietro explains apologetically. “Sorry.”
“Oh.” Steve tries to keep his voice measured. “Ok, sure.” He steps back toward the exam room and leans against the doorway.
“I’m really sorry,” Pietro repeats. “It’s just, policy and all--”
“It’s fine.” Steve crosses his arms, hoping he doesn’t come across as confrontational. “I’m just really worried about him. It all, like, came on so fast, and…” Moisture prickles unexpectedly at the corners of his eyes.
“Hey, I get it, man.” Pietro claps him on the shoulder. “Working ER, we kinda see it all the time. Not to trivialize it or anything, but, like, really bad, scary things happen every day, and most of them turn out to be ok.”
Steve gives a long, hard exhale. “Thanks.”
“Anytime, bud. You work here, right?” Pietro points to the access badge sticking halfway out of Steve’s pocket.
“Yeah. Counseling,” Steve replies, quickly wiping his eyes with his thumb.
“Well, if I ever pull a normal shift, I’ll give you a secret handshake in the cafeteria.” Pietro grins.
“Sure thing.”
“MRI takes, like, ten minures. Maybe fifteen, tops. Just wait here. Holler if you need anything, and Happy’ll bring your boy back once he’s out of the giant magnet.”
“Happy?” Steve asks.
“Hogan, I mean,” PIetro corrects himself. “We have all kinds of call signs around here.”
“Oh. Well, thank you,” Steve says. “You’ve been great. Especially after what’s-his-name.”
“Rumlow?” Pietro laughs. “It’s spelled just like it sounds. And my last name’s Maximoff, by the way.”
“Ok…”
“Patient survey’s on the website.” Pietro winks.
Steve laughs. “Will do.” He gives him a wave as the nurse takes his leave.
Steve reenters the small exam room and takes a seat on the rolling stool, then changes his mind and goes back to the chair in the corner instead. He crosses his legs, then uncrosses them and drums his fingers on his knee. It finally occurs to him to pull his phone from his pocket to pass the time, but Steve immediately feels guilty and puts it back. He checks his watch and sees that 12 minutes have passed. A thrill of panic rolls down his spine when he realizes James could be back literally any second, and a diagnosis could come any second after that.
A clatter sounds in the hallway, and Steve leaps from his seat. He reaches for James, who is leaning forward slightly in the wheelchair, his eyes downcast. Steve notices that his pajama top has been changed for a hospital gown, and his medical alert necklace is tangled in the IV line around his wrist.
“Hey, Buck,” Steve whispers, trying not to overwhelm him. “How’re you feeling?”
“Mm.” James slowly lifts his head as the technician, Happy, pushes the wheelchair back into the exam room. “Not so good.”
“I’m sorry,” Steve says. He gently untangles the necklace from James’s wrist and re-fastens it around his neck. “D’you want to lie down, or--?”
“Better stay put, if you ask me,” Happy says. “Doc will be in with results in just a minute and then he’ll be moved to a room upstairs.”
“So they are admitting him?” Steve asks. “Is that based on the scan, or just what that NP recommended?”
“Hey, I just drive the chair,” Happy replies, raising his hands palms up. “But he’s pretty sick, and a little bird told me room 211 is going to have a new occupant pretty soon.”
“Second floor?” Steve confirms. “Not psych ward, then. And not ICU, either.”
“No, it’s not,” says a new voice. A doctor with a white coat and ashy greying hair steps into the room as Happy vanishes down the hall. “I’m Dr. Alexander Pierce.” He waves a handful of printouts. “Here with actual results and orders, not prognostications and psychological philanderings.” He wiggles his fingers to emulate silliness.
Steve feels too caught to be offended. “My apologies, sir,” he says. Then he nods toward the printed papers. “What are the, uh, findings?”
“Nothing!” Dr. Pierce announces. He slaps one paper down on the cot and lines up another next to it.
James flinches at the sound. Steve squeezes his shoulder.
“Pain isn’t due to anything structural. Migraine activity behaves much like seizure activity, and I understand he does have a history of those.”
“Yes.” Steve nods.
“So I’d like to admit him and try a course of IV meds while keeping him under observation. The past traumatic brain injury makes things a little more complicated, and I want to be a bit more cautious, but it’s a headache disorder we’re treating, not a tumor or an aneurysm.” Dr. Pierce offers a wan smile.
Steve lets out a breath he didn’t realize he was holding. “Ok,” he says, looking at James. “Ok?”
“Yes,” James whispers, barely moving his lips. “I just-- anything--”
“Anything to feel better?” Steve fills in the gaps.
James nods minimally, then gulps. “Sorry,” he hisses.
“Don’t worry.” Steve rubs the back of James's neck.
Dr. Pierce is less impressed. He yanks an emesis bag from a fixture on the wall and holds it out. James shakily takes it, but lets the green plastic crinkle in his lap.
“Transport will take you up to the second floor,” Dr. Pierce says. “I’ve already put orders in for some medications.”
“Wow,” Steve comments. “That’s fast.”
“Saturday morning is a good time to visit us at the hospital, if there is such a thing,” Dr. Pierce smiles. He nods to Happy and says “Take ‘em on up.”
Room 211 is arranged the same as the exam room downstairs, though with a bed in the center instead of a cot. There’s a computer in one corner, a chair in another, and a small rolling table pressed up against the wall.
James is decidedly green around the gills again by the time he’s offloaded into the bed. “Steve?” he asks in a choked whisper, barely containing a gag.
“Here.” Steve opens the emesis bag and holds it open for James. A long string of saliva drips into it, but nothing else seems to want to come.
“It’s alright, Buck.” Steve gives him a gentle pat on the back.
“Feeling pretty crummy, there?” asks a kind female voice. A woman in pink scrubs enters the room, closely followed by a nervous-looking young man holding a clipboard. “I’m May,” she says. “I’m your nurse today. And this is Peter, my student.”
“Hi.” Steve waves with his free hand. “I’m Steve. He’s James.”
They attach a pulse oximeter to James’s finger and heart monitor leads to his chest, then Peter begins to scribble down a note as May clacks away on the computer. “Looks like we have orders for intravenous cocktail of painkillers, anti inflammatories, and a mild sedative to start with. That plus oxygen therapy can sometimes break a migraine.”
The words themselves hardly make an impact on Steve. May begins to list off drug names to Peter, and the kid leaves the room to fetch them.
“How’re you holding up?” May asks.
“Huh?” Steve snaps out of his daze. “He’s--”
“No, I mean how are you feeling?”
“Oh.” Steve scratches the back of his head. “I’m ok. Worried. Relieved, but still worried. I haven’t seen him this bad off since he had the first seizure…” The corners of his eyes begin to prickle again, and he quickly brings his hand around to cover his mouth.
“Hey, it’s gonna be ok.” May gives his arm a motherly squeeze. “Pain is hard to watch, but easy to manage once you give it some time.”
“Hm.” Steve slowly nods. “Good point.”
“Now, what can I get you? Maybe some soup?” the nurse suggests. “You should both eat something.”
“Oh, I’m fine.” Steve gestures to himself. “And--” He gestures to the the emesis bag in his hand.
“You shouldn’t worry on an empty stomach. And he needs something to properly throw up.” May grins. “I’m joking, of course.”
“Oh.” Steve finds himself fighting a laugh.
“Go ahead,” says May. “That was meant to be funny”
Peter returns with several syringes and an oxygen cannula. He sets up the O2 first, gently inserting the prongs of the cannula into James’s nose. James shifts to allow the tubing to be tightened beneath his chin, then he curls like a cat with his stump arm buried in Steve’s lap. Steve knows the oxygen is far from magic, but it seems James’s labored breathing immediately eases a bit.
“Now for meds,” May says. She tells Peter the order in which the drugs should be injected into the IV line. “Dilute them with a little saline so they don’t burn on the way in.”
“Do they burn?” Steve asks in concern.
“Nuh.” James shrugs. “At this point,” he pants. “Don’ really care.”
“Aw, Buck,” Steve says, gently petting James’s hair.
“That’s it for now,” May says. “I’ll bring you guys some food in a few minutes.”
True to her word, she does return with two bowls of soup on a tray. “Now, I didn’t cook it, so take it up with Nutrition if it’s the wrong flavor or something. I think it’s supposed to be corn chowder.”
“Thank you,” Steve says, maneuvering the rolling table over to the bed. “So much.”
“Don’t mention it. Just looking out for you.” May takes her leave.
Steve carefully peels the top off one of the bowls. Steam rises from it, giving off a bland savory smell. “You first?” he asks James.
“Nope,” James protests. “This one’s all you.”
Steve shrugs and dips in a spoon. He brings it to his lips and sips slowly. “Huh,” he murmurs, then takes another spoonful.
“How is it?” James asks. “Or do I even want to know?”
“It kind of tastes like...water,” Steve decides. “Or, like...like nothing.”
“Gross.” James gives a shallow cough.
“What, you don’t want to try it?”
“Not unless you want it back all over the front of your shirt.”
“Fair enough,” Steve laughs.
A man in an apron and hairnet comes to get the bowls after a while. James settles into the mattress on his side, his head on the pillow and his fingers threaded through one of Steve’s belt loops. Steve lies carefully beside him, taking up as little space as possible as he watches fluid slowly drip into the IV line on the back of Jamse’s hand.
“How’re you feeling?” he asks softly.
“Honestly?” James flicks his eyes upward to get a good look at Steve’s face, then winces. “Kinda the same.”
“Hm.” Steve presses his lips together. He’d hoped for the best, though he knows treating migraines is part science and part magical mystery, like throwing knives at a spinning roulette wheel. He reaches over James’s back and finds the remote with the nurse’s call button. He presses it and waits a moment before May and Peter appear.
“Tell them what you just told me,” Steve says, giving James a prompting nod.
James sighs. “Still don’t feel good,” he mutters.
“Oh, sweetie,” May simpers. “I’ll talk with the hospitalist and see what else we can give you. Dr. Danvers is on today, and she should be in for rounds in not too long. Your neurologist will be along later as well.”
James nods, then winces again and swallows painfully.
“You didn’t eat, did you, babe?” May puts her hands on her hips and shakes her head.
“Can I get you a basin or something?” Peter asks, seeming eager to be helpful.
James says “no” at the same time that Steve says “yes.”
“You don’t have to use it.” Peter gives a nervous smile. “In fact, we hope you don’t.”
“Go grab one,” says May. “I’ll grab Dr. Danvers.”
No sooner has Peter deposited the unwanted basin on the table than a tall woman with short caramel colored hair arrives.
“Dr. Carol Danvers,” she introduces herself. “I hear first line of defense hasn’t worked out so well.”
Steve shakes his head. “No, we’re still not feeling great.” He gives James a meaningful look.
“My head is fucking exploding,” he murmurs.
“I understand.” Dr. Danvers perches on the edge of the recliner in the corner of the room. “Unfortunately there isn’t a reliable cure-all for a severe headache like this. I have a couple more tricks to throw at it, and hopefully neuro will have a few more.”
“Ok,” Steve says. “What kind of odds are we talking here, doc? I just, you know, I just hate seeing him like this.”
“Honestly,” Dr. Danvers starts, “I couldn’t begin to tell you.” She presses her lips together. “The cocktail of painkillers and vitamins I want to try has a pretty good reputation of success against a status migraine, but it isn’t foolproof. Nothing really is.”
“Yeah,” Steve sighs. “So I’m learning. Thanks for being honest with us.”
“Sure thing. How do you feel about it, James?”
James swallows hard. “I’ll try anything,” he croaks.
Dr. Danvers offers a sad smile. “We’ll get you better. If not this round, then the next.”
She stands and leaves the room.
Barely a moment later, May and Peter are back with fresh bags of IV fluids.
“Some more saline,” May explains. “Then painkillers”. She slowly injects the line.
James closes his eyes.
Peter holds up the next syringe. “Now for magnesium. Um, this one can burn a little.”
“Whatever,” James mutters.
“Ok.” Peter smiles and shrugs, then begins to inject the clear fluid.
Within five seconds, James is gritting his teeth. His face goes a shade of fire engine red, and beads of sweat gather at his temples.
“Buck?” Steve asks, snaking his arm around his shoulders. James’s skin burns through the hospital gown as if he’s spiked an instantaneous fever. “Is this normal?” Steve demands.
“Yes, unfortunately,” Peter answers. “It only lasts a few minutes.”
“Jesus,” Steve says under his breath. He isn’t sure whether to pull James close or to refrain from touching him at all.
“Mm,” James groans, swiping at the perspiration running down his cheek.
“I got it, Buck,” Steve says. He stills James’s hand and uses his own shirttail to catch the drip.
“Next is a steroid,” says May, continuing to fuss with the IV. “Hopefully this will break the headache, but it can have a couple side effects. Can make you feel a little puffy, a little hungry. Nothing dangerous, but it can be pretty annoying once you get to feeling better.”
“Then we’ll deal with it then,” James says quietly. Steve imagines he can’t care less about side effects at the moment. He can’t either.
“That’s a good attitude you’ve got,” May comments. “Alrighty, that should knock you flat for a good couple hours. We’ll evaluate how you’re doing when you wake up, and hopefully neuro will be making rounds by then.”
“Ok.” Steve looks from James’s face to to May’s. “I guess that sounds good.”
“Call me if you need anything, Sweetie.” She grins at him, then she and Peter take their leave.
Steve lets out his breath again. James is still warm to the touch, but his expression is much more serene. His hair is damp with sweat and sticking to his face. Steve combs his fingers through it and murmurs sweet nothings until he feels sleepy himself. He curls around James as much as he can on the narrow bed, shuts his eyes, and drifts into a light sleep.
He wakes when James starts dry heaving again. Steve scrambles to grab the basin off the table and shove it under James’s chin, but it’s completely unnecessary.
“It’s alright.” he slips his hand behind James’s back and gives it a light tap. “Just get it up, if you’ve got it.”
“Nah,” James says, spitting out a string of mucous and wiping his mouth on his shoulder. “‘M hungry, though.”
Steve laughs and presses the call button. He expects Peter and May to return again, but instead it’s a young black woman with long braids who comes toting the cup of pudding. She hands over the dish and spoon, then sits cross-legged on the end of the bed.
“Hi, Dr…” Steve squints at her name tag.
“Call me Shuri,” the woman says. “I don’t use my last name. No one can pronounce it. And I don’t use ‘doctor,’ either, but I’m your neurologist today.”
“Good to meet you,” Steve says.
James raises his spoon in salute.
“So,” Sure says, getting right down to business, “You’ve had two migraine cocktails. How are you feeling?”
“Still like hell,” James mumbles, his mouth full of pudding.
He looks like hell, too, Steve thinks, with circles under his eyes and a gaunt, greyish tinge to his skin.
“The brain is a mysterious thing,” Shuri explains. “You have a TBI, so I know you understand some of this already. Injury happens, then recovery. But with the brain, it isn’t like healing a broken bone. And when the injury isn’t even an impact, it’s spontaneous electrical activity…” She shakes her head. “It’s like fighting invisible enemies.”
James sighs and hands Steve his empty bowl. “You make it sound like a sci-fi movie or something,” he jokes.
Steve is glad to see him in a good mood, but he doesn’t like the way lines of pain appear around James’s eyes. Shuri seems to notice too.
“Here, why don’t you lie down,” she suggests, getting to her feet. “I’d like to try you on a new combination of medications. Some will be added to your regular daily regimen of anticonvulsants, and those will be a permanent fixture. Some others will be administered intravenously over a 72 hour period while you're here at the hospital. They take nearly the whole period to begin working, but I’ve seen good success.” Shuri smiles. “Does that sound ok to you?”
“So…” James’s brow wrinkles as he does the math. “That’s three days in here?”
“Yes,” Shuri says. “Fortunately. Or unfortunately, however you choose to look at it. It can feel like a long time, but it’s fairly quick in the world of intractable migraines. We’ll be sure to send you home with plenty of preventables. Injectable Imitrex, that kind of thing. To keep you ahead of the curve.”
“Ok,” James says, his voice going flat. The look in his eyes is hopeful, yet exhausted.
Steve nods and looks to Shuri again. “Alright,” she says. “I know this is complicated, but I like to keep my patients well-informed. You’ll continue to get your regular meds morning, midday, and night, with the addition of another anticonvulsant, plus oral painkillers as needed. Then you’ll get an antiemetic and an analgesic in your IV every six hours for the next three days. We’ll continue your oxygen therapy as well.” Shuri points to the cannula under James’s nose. “And we’ll keep the option for a mild opioid open should you need something that works a little stronger and faster. She looks between Steve and James. “Is that clear as mud?”
“Clear enough,” Steve says, pleased with the way she’s broken it all down for them.
“Yes,” agrees James, nodding slightly and wincing.
“Don’t strain yourself,” Shuri says. “I’ll put in the orders and see about setting up that first dose.” She nods to them and leaves the room.
Once they’re on their own again, James turns to Steve, cautiously rolling onto his side. “So. Three days in this place.”
“Yup,” says Steve. “Want me to run by home and get your toothbrush? Maybe some pajamas for you?”
“That would be great, actually,” says James, a little blearily. “But what do you mean, run by? Wouldn’t it be easier to come back and see me after work on Monday?”
“Buck.” Steve shakes his head emphatically. “If you think I’m leaving you here by yourself, you’re nuts. You know what, Sam has a spare key. He can pack up some essentials and bring them over.”
James blinks a few times. “Really?”
“Of course.” Steve kisses his cheek. “To the end of the line, remember? Always to the end of the line.”
#captain america#mcu#marvel#steve rogers#bucky barnes#stucky#whoa bessie#au#alternate universe#sickfic#emeto#illumivomi#hurt comfort#hospitals#needles#status migraine#seizures#headaches
47 notes
·
View notes
Text
If you hate your job so much, just quit.
Psychiatric Emergency Services at Victoria’s Royal Jubilee Hospital is a department that is run like no other medical department in the world. The treatments used in first-line mental health crisis were not designed to address the neurological functions associated with mental distress outside of psychosis. Additionally, the hostile environment created by staff serves no purpose in the treatment of mental distress.
I’ve been there countless times. I have witnessed the procedures and noticed alarming patterns in procedures were applied not to chemically subdue patients experiencing a wide range of psychiatric ailments.
When you first walk in, you are asked to hand over your bag and cell phone by a nurse. You are then directed to sit down in one of the chairs in the waiting room. Assessment usually begins with a nurse who asks you a service of questions in order to relay that information to the psychiatrist. You are then asked to go back and wait to see the next doctor, usually a medical doctor. Following that, you will be given the opportunity to speak to a psychiatrist. The psychiatrist will recommend medication or hospitalization based on what they observe.
Patients who suffer from psychiatric problems like psychosis are often unmanageable, hostile and may be physically violent. Anti-psychotics are the first line medications used to treat drug-induced or schizophrenic episodes of psychosis by correcting the irregular dopamine functions associated with the ailment.
These seem like standard, reasonable procedures, but what makes PES unique is the unexplainable logic used to validate the administration of psychiatric drugs and execute deplorable personal treatment of patients by support staff. Unlike people suffering from physical pain, people who suffer from mental illness are vilified for questioning procedures that include detaining people isolation if they were forced to go to the hospital by family members, friends or law enforcement after showing signs that their mental health was a threat to their welfare, or the welfare of those around them.
Distressed people who do not want to go to the hospital usually become aggressive and demand to let out. In my case, a friend overreacted to something I said online and provoked a team of law enforcement and an ambulance to raid my home, handcuff me and deliver me to psychiatric emergency services. After hours of trying to get out, worrying about the welfare of my pets after the dramatic scene the RCMP and ambulance had created, I became hostile. I used the phone in the waiting area to call 911 and try and get out. Having previous experience with psychiatry, I knew I would likely be forced to take the magic bullet of psychiatric medicine: Seroquel.
I’ve taken Seroquel before, naively after my psychiatrist recommended it for insomnia. After taking it, I passed out cold and woke up with a terrible feeling of depression, dread, anxiety and depression. I immediately made the connection between the drug and these symptoms but did not realize that all anti-psychotics by their very mode of action are directly responsible for chemically inducing these kinds of mental disturbances.
Anyways, I asked for a piece of paper and wrote down a lengthy satire targeting the over prescription of Seroquel. I was then guided to a private observation room where several doctors and a psychiatrists who did not ask questions about my well-being but addressed the very behaviour I was displaying as a result of being detailed against my will, and the audacity I had in ridiculing the well-known practice of prescribing Seroquel for psychiatric disorders where no evidence existed to support the administration of the drug. She called me a psychopath and then used the opportunity to impress the room by listing the qualifications she had acquired various certificates and degrees. No explanation of why anti-psychotics were being administered for psychiatric ailments outside of psychosis was provided and the illogical argument that a variety of vague academic achievements somehow qualified the psychiatrist’s relentless devotion to this magical drug.
The very logic behind administering these drugs for a rainbow unrelated mental conditions is an unexplainable practice that is incomparable to any other medical practice in the world. The assumption that one drug can treat the extraordinarily complex functions associated with multiple mental illnesses seems so obviously faulty. In no other medical practice can a drug be used without any scientific proof to treat illnesses by chemically inducing the blockade of the very neurostransmitter responsible for creating positive emotional responses. The very neurotransmitter that upon release is scientifically proven to be the reason why people feel happy is chemically supressed by anti-psychotics and by removing the ability to experience the ‘happy’ emotion, these drugs treat depression. Depression is unhappiness. So by eliminating the ability to be happy, people who experience chronic unhappiness will benefit from a drug that by its very mode of action chemically castrates the brains ability to make happiness. What in the actual fuck is going on? Imagine a doctor prescribing smoking to cure lung cancer. That’s the same thing as treating depressive mood disorders by administering medication that restrains the ability to make happiness. Happiness is the opposite of depression, no? Am I missing something?
After that productive discussion, the psychiatrist used her power ‘punish’ me by committing me to the isolation room where I violently banged on the door for hours until guards came in to restrain and inject me with anti-psychotics.
I woke up on the cement floor to see that one of the nurses had thrown a plate of food into the isolation room. Most of the food had fallen off the plate and were on the cement, but by all accounts the nurse fulfilled the requirement of providing a psychiatric detainee with food. I did not eat the food. Additionally, the anti-psychotic administered created an overwhelming sense of depression, anxiety and dread. Extreme mental distressed, faced with the realization that my freedoms and psychiatric well being were at the mercy of psychiatric decisioning was incredibly traumatic. I was then escorted to another unit in the hospital and put in another isolation room. I passed out again and woke up startled, not knowing where I was.
I got up and knocked on the window and was met by a nurse who let me out. The ward was a small, windowless set of rooms and a common area for eating. The medication I took both suppressed my cognitive functions, and chemically induced a state of dysphoria and dread.
Several days past, and I was not considered well enough to join the adjacent ward where more freedoms were awarded to patients. The continued administration of anti-psychotics caused insomnia and ruminating thoughts throughout several nights and after about seven sleepless nights, my cognitive abilities were so limited that I failed to recognize where I was when the doctor asked me. By some miracle, I was able to string together the words required to ask the doctor to review the records the nurse had kept about my sleep. She had lied on her report and indicated that my sleep was excellent.
I still have vague memories of countless nights where I pled for help at the window that surrounded the nurse’s station. If she even ever paid attention to me, she would do so by opening the window and yelling the word, “no.”
There are no words I can use to try and describe the dysphoria that anti-psychotics produce. There is nothing that I can compare to the anguish of chemically induced states of mental distress that they cause by their very mode of neurological action in blockading dopamine, the chemical responsible for mental well-being. There is no way out and no relief.
Patients in the psychiatric ward at RJH are treated with palpable disrespect. The chemical restraints forced upon patients do not treat symptoms of mental illness outside psychosis. They subdue patients in order to make them manageable and ensure the safety of medical staff if they display warranted frustration with being locked away against their will. Nothing more.
After weeks of forced medication, the psychiatrist started to put me back on the medications I was used to taking before being admitted to the hospital. My mental health quickly improved after anti-psychotics were removed from the schedule. Eventually I was released, only to relapse into psychosis again after months of isolating and self-medicating the trauma induced anxiety brought on by my incarceration in the psych ward.
I’ll never forget how I helplessly pled for relief of the anxiety produced by anti-psychotics. The prolonged insomnia had profound impacts on my cognitive functioning were so frightening. After seven days of sleeplessness, the doctor finally administered a drug to put me to sleep. There are no words I have to express the utter lack of confidence in psychiatry that I have after being submitted to the abuses of medical professionals responsible for psychiatric patient care. This was only the first, and not even the worst.
I can’t help but continuously think about the unrelenting desire support staff at the psych ward have to execute punitive actions on patients there, may they be the denial of medications they need to alleviate the unbearable stresses of forced incarceration or the overwhelmingly disdainful way in which they treat patients. I can only compare it to the way overworked parents abruptly address the frivolous demands of a fussy toddler. Only replace toddlers with adults and frivolous demands with helpless pleas for their lives.
The logic in which drugs that produce unhappiness are used to create happiness in psychiatry is also prevalent in the way in which patients are subjected to treatment that would cause emotional distress in facilities believed to treat them.
These kinds of absurd realities in healthcare are far too unreal for people to believe.
I can’t help but wonder why nurses who work there do work there. If you hate your job so much, do the world a favour and quit.
2 notes
·
View notes
Note
"Why the hell is there glitter everywhere?", Ethan x MC. Thanks 😘
Rating: General
Summary: A ficlet about Jenna, Ethan, and some glitter. It’s just fluff with a touch of mutual pining, taking place sometime after Book 1. MC name is Jenna Clark.
Word Count: 686
A/N: Thanks for the prompt! I hope you like it!
Jenna rapped smartly on the door to Ethan’s office, a bulkystack of papers in her hand. It had been a busy day, and her newest case was givingher a headache. She heard Ethan’s answering call of permission and opened the door,stepping inside and closing it after her. He was sitting at his desk, perusinga medical journal, and he looked up as she entered, taking off his glasses andslipping them into his shirt pocket.
“Ethan, I could really use your help with this patient Ihave. His symptoms are so bizarre—” She paused as she glanced at hisdesk, and the carpet surrounding it. “Hang on. Why the hell is there glitter everywhere?”
To her surprise, a slow flush crept over his cheeks. “Er…”He stared at her, like a deer caught in headlights.
She observed the small flecks that dotted the area. “It’s gold,too. What have you been doing?”
He sighed and opened a desk drawer, pulling out a simplewhite envelope. “I was going to give this to you later, but I suppose you mightas well have it now.”
Curiosity burning, Jenna took the envelope from him and openedit carefully. Inside was a white greeting card with the words, “Happy Birthday”stenciled on it in gold glitter. Even as she held it, a few flecks fell fromthe card onto her hands.
Ethan rubbed the back of his neck sheepishly. “You’re sohappy all the time… it just seemed like something you’d like. I didn’t expectit to shed quite as much as it did.”
Several thoughts bounced around her mind, begging to be addressed,like the fact that Ethan associated a cheerful personality with an affinity forglitter. Or that she couldn’t remember ever telling him when her birthday was. She’dbarely remembered that it was her birthday today herself; she’d never thoughtit particularly important, and she disliked having a fuss made over it. “Howdid you know it was today? I didn’t even say anything to my roommates.”
He shrugged. “You mentioned it once, about a month ago.”
And he’d remembered? Now it was her turn to blush, and she openedthe card to cover her embarrassment. He’d written a short message in blue ink.
Rookie,
You’re a damned good doctor, and an even better friend.Happy birthday.
Ethan
She glanced up to see him gazing at her, nervously waitingfor her reaction. “Ethan, this is so sweet.”
A relieved look passed over his face, but he quickly maskedit with a cough. “Well. Good. Sorry about the glitter, though. That was probablya mistake.”
She laughed, and tried futilely to brush a few of the gold flecksoff her palms. “It is the herpes of the craft world.” He cracked a smile, andas they looked at each other, she felt that thin line of professionalism they constantlydanced around blur.
He cleared his throat. “Well, anyway, what did you want toask me?” Jenna felt a small tinge of disappointment, but she tucked it away.What did she expect to happen? He’d made it clear on their first day back atthe hospital that things had to go back to normal between them. Suppressing asigh, she dragged the second chair in the room around to his side of the desk andbegan consulting with him about her patient.
A few minutes passed as they discussed symptoms andtheories, and eventually, the answer stood out to her. In a flurry of excitement,Jenna rose from the desk, ready to make for the door. Then she paused, and turnedback to face him. “Thanks for your help, Ethan,” She smiled. “And thanks forthe card.” There was a beat of silence, and then impulsively, she leaned downand dropped a kiss on his cheek, fleeting and soft.
Surprised by her own daring, Jenna quicklystepped towards the door. As she closed it behind her, she caught a glimpse ofEthan, still sitting in his chair with a bemused expression on his face, and afleck of gold glitter gleaming on his cheek.
Tag List: @dr-brianna-casey-valentine@paulfwesley @silverlitskies @togetherwearerapture
Let me know if you’d like to be added!
#this prompt was cute#and it went somewhere different than id originally thought it would#ethan x mc#open heart mc#ethan ramsey#ethan ramsey x mc#open heart#choices#oh#choices oh#open heart fic#ethan ramsey x mc fic#choices fic#playchoices#playchoices fic#open heart fanfiction#ethan ramsey fanfiction#ethan x mc fic#ethan ramsey x mc fanfiction#choices fanfiction#playchoices fanfiction#my fic
105 notes
·
View notes
Last Seen Blogs

millerntorfan
Millerntorfan

musicistheair-blog
Music Is The Air

abcd1234
无标题

rommipullo
a dusty black coat and a red right hand.

kikinibill
nap