#this is specifically why self diagnosis doesn’t work in practice
Text
I just need you all to understand “doing research” does not and will never end in “looking at articles online”. You’re not researching, you’re looking something up.
These two actions do not hold the same weight and you should not be acting as if they do.
#anti intellectualism#tik tok#science#research#I hate a do your own research ass bitch#you’re not advocating for that person to learn or whatever#you’re sending them down a conservative rabbit hole and doing it on purpose#this is specifically why self diagnosis doesn’t work in practice
12 notes
·
View notes
Text
Book Review 64 – Poverty, by America by Mathew Desmond

I read Desmond’s Evicted a while back and found it a really excellent bit of sociology/journalism about the specifics and mechanisms of housing inequality and how modern slumlords exploit the poor. So this has been vaguely on my list for a decent while. Sadly, I found it a bit of a disappointment – more listing of facts and statistics that I already basically knew to support a manifesto than anything new or enlightening to me. Not that it’s bad, but if it was 20 pages instead of 200 I’m not sure much of value would really have been lost. Many such cases, I suppose.
The book is about exactly what it says is, a polemic decrying and investigation into why the United State’s poverty rates, and why extremes of material want are so much more common there than in comparable (poorer, even) western democracies. Refreshingly, Desmond has a clear thesis he doesn’t beat around the bush before saying – self-interest, essentially. The affluent benefit from having an underclass to extract resources from, and from excluding its members from the amenities they share, so they do. The book spends most of its wordcount enumerating and describing what Desmond considers the main problems: direct exploitation (underpayment, predatory financiers, slums, etc), an underresourced and misdirected wellfare state (compare the cost of middle/upper-class targeted programs like the mortgage interest deduction or tax-exempt savings accounts to the cost of adequately ending hunger or providing healthcare) and segregation (both spatial/residential and in terms of access to public or semi-public services).
It’s pretty traditional for a book like this to spend 90% of its wordcount diagnosing problems and then end with some publisher-mandated optimism and a chapter of solutions with a fraction of the care put into them as in the diagnosis. Desmond, to his credit, avoids this – each chapter includes both the problems and he considers the most feasible solutions to them to be. He actually makes a point of it, arguing that having practical, winnable goals that will actually improve things when achieved (and then celebrating them when they are) is a key part of any political organizing with a chance of actually working. Now, what I think of those solutions varies quite wildly, but they’re there and exactly what you’d expect for his politics – and speaking as someone whose been renting my entire life I wholly endorse fucking all the tax benefits you get essentially for having the cash on hand to make a down payment. (Relatedly, the book has a great deal of scorn for comfortable, affluent people whose progressive politics amount to lots of critiquing and zero actual positive action.)
Desmond is clearly writing this from the point of view of a(n inspirational) public intellectual; that is, by writing this he’s trying to call an audience and movement based around it into being. He likes the label Poverty Abolitionist and the central project of the book is basically trying to make it happen as an umbrella term people identify with – especially the affluent well-heeled people who read books like this, and might be persuaded to start boycotting companies for underpaying their employees or union-busting, or campaigning against government subsidies that benefit them instead of the poor. I did appreciate the relative hopeful tone, given the usual coverage of American politics – or, well, is ‘Washington was at least this fucked when it passed the Civil Rights Act or the New Deal” optimistic? Whatever the right word is.
Now, I’m summarized all this in ~500 words, obviously actually making the argument needs more space than that. But it really did not need to be as long as it was – a huge fraction of the wordcount is spent either restating arguments or just throwing around numbers and statistics without really contextualization (anyone who spends so much time comparing expenses and budgets across the decade should be legally required to adjust for inflation imo). There’s a good, well-cited (excessively cited, if anything. The footnotoes are like a fifth of the book) persuasive essay in here, but there is so much fat to cut around it.
Anyway yes, disappointing reading experience, given I was hoping for more sociology and less polemic. But as far as American political polemic goes, it’s pretty decent.
23 notes
·
View notes
Text

My Brain Doesn’t Picture Things (Marco Giancotti, Nautilus, Oct 04 2023)
"My whole life, I’ve been aware—sometimes painfully so—of my own peculiarities, strengths, and weaknesses: A terrible memory, a good sense of direction, and what I felt was a lack of “visual creativity,” among others.
I always thought these were just random, disconnected traits, and didn’t think much about them. Who doesn’t have their quirks?
Then, some time in 2021 (not coincidentally, I forget exactly where or when) I read about aphantasia for the first time, and it hit me hard: When people say “picture this scene in your head,” they aren’t speaking metaphorically!
People can actually invoke shapes and colors in their minds.
The shock of this realization was followed by a piecing together of many of those little idiosyncrasies of mine into a single, coherent phenomenon that fit with the scientific description of the condition.
By the time my formal diagnosis came, I was already quite sure I was aphantasic. (…)
The biggest source of confusion with aphantasia comes from the assumption that “imagination” and “forming mental images” are one and the same thing.
This is, of course, incorrect.
I’m able to imagine anything, except it is all devoid of sensory representations.
The imagined objects exist in my mind as interconnected concepts, like bullet lists of facts about things. (…)
Past episodes of my life—when I can recall them at all—feel distant and non-sensory.
SDAM is a new discovery, still unknown to most practicing psychiatrists, so people like me have to rely on self-diagnosis for the time being.
But the symptoms described by the researchers match with what I’ve always taken for granted.
I would describe my recollections as summaries of key facts rather than first-person “mind movies.”
When asked, out of the blue, about an experience I’ve surely had—say, any childhood birthday party—my mind first responds by drawing a blank.
It feels as if my episodic memories were filed into a “mental cabinet” without an index.
Many memories are in there, somewhere, but retrieving them is a daunting task unless I’m provided with very specific prompts.
With some groping work of deduction (where did I live at the time? Who did I hang out with?) I can gather enough hints to bring out some locations and non-visual facts: I had a big party in our countryside garden when I was 11 or 12; there was cake; a lot of kids running around and … that’s about it. (…)
Suddenly, your performance in every other aspect of life comes under scrutiny, and blaming your congenital aphantasia for it is almost irresistible.
Is drawing without a reference so difficult because of my aphantasia? Could SDAM be why I’m so bad at keeping in touch with people? Would I be less socially awkward without it?
Very few of these supposed connections have been tested yet, let alone confirmed by solid scientific studies.
Yet almost every aphantasic I’ve talked to does this. But everyone seems to focus their self-doubt on whatever they don’t like about themselves, scapegoating different shortcomings."
20 notes
·
View notes
Text
The barriers to accessing treatment keep on pilling up...
“Affordable” therapy that isn’t really affordable. Therapists who offer low cost and/or sliding fee are limited to certain places and professionals, and the waiting times are immoral.
The “specialties” are focused on resolving “simpler” issues that impact quality of life. Even when you can find something more particular (such as trauma-informed, or queer-specific), it only goes skin-deep.
Maybe this is how I see things now, since I have years of treatment on my back. Personally, it feels like it’s not enough, it doesn’t reach the root of the issue and... I’m on a stalemate.
There’s 2 things that feel especially sour for me, considering my personal circumstances: the fact that professionals (and clinics themselves) are not willing to take upon patients that are suicidal, and the fact that all therapy is supposed to do is to get a person to achieve a degree of functioning and decrease suffering.
In the latter, I feel I’m 100% functional. I can take care of myself, I’m lucid and I’m able to do basically everything on my own (taking into account limitations due to physical and other psychological conditions). I’m already doing everything within my power to “decrease suffering” that is... all those things you see out there about exercising, diet, hobbies, going outside regularly, sleep hygiene, self-care, etc... they all, indeed, decrease suffering.
I’m still suffering though. At times, I feel like it’s worsening actually, the activities I engage with to “decrease suffering” end up having the opposite effect so... I feel like, slowly, some of those activities are augmenting suffering instead.
It makes sense considering treatments and “solutions” for all kinds of issues have “standards” and these standards, in practice, don’t really apply to everyone.
When I was in the process of getting a diagnosis for chronic pain, I was told I “should exercise more”. Yeah... I guess I didn’t think about that, huh? The funny thing is that I’ve been always a very active person, one of the reasons I started pursuing a diagnosis was because I was unable to exercise.
I guess it’s trickier in the realm of mental illnesses, because oftentimes, they’re “invisible” conditions. Of course, a doctor will see me suicidal and suffering and assume my sleep/diet is bad, I don’t exercise, don’t go outside and don’t have any hobbies. When you do tell them that, then the answer is “therapy”.
And you go to therapy, where the exact same assumptions will occur because that’s usually how it goes.
My impression so far is that I need to do everything “harder” and “stronger”, as if I were doing those activities lightly, and this is why they’re not working. The intensity or amount don’t really make a difference in my suffering, but it will surely leave me more and more exhausted. And it’s all such a horrible trigger for obsessive-compulsive behaviours: I obsess over sleeping well (so I put myself through a very strict schedule), I obsess over my diet (I have a million eating disorders), I obsess over exercising and my hobbies and going outside (so I force myself to do these things whether I want it or not), I obsess over self-care (so the inside of my head is a echo-chamber, from which I can’t escape), and so on...
Not surprisingly, my sleep is shit, my diet is shit, and everything else is also harming me in a way or another, but I (feel like I) need to keep on going because “this is also part of the treatment”.
The other piece, suicidality, from what I understand, is about professionals and spaces not wanting to take accountability or be held responsible for someone else’s life - many explicitly will exclude people who are “in active psychosis” or “suffering with homicidal or suicidal urges”, etc, so... the patients need to have some degree of functionality, and achieve some level of “normalcy” to be able to receive treatment.
Well, okay then, what are the options for me? I’m suicidal but I’m no in imminent danger of dying so I don’t want to access mental health crisis resources because they would not be helpful for me in my current state. At the same time, this is something that’s affecting both my quality of life and functioning as I’m unable to, among other things, seek and maintain stable employment or a support system. Trapped in poverty, unable to afford treatment as well, and so on... predictably, all things that increase suicidality.
I either have to lie to, maybe, receive treatment, mention suicide during therapy and have it become a shitshow because the therapist thinks I’m going to die ASAP, don’t listen to me and everything goes to shit. Or I do mention it beforehand and am barred from receiving care altogether until I’m “stable enough”. Regardless, I feel like I have to lie and water down my issues to be seen as “normal” and palatable and not have my autonomy taken away from me.
The last thing, and I guess the thing that stings the most, is the fact that anything that doesn’t “improve” with the most common styles of treatment, therapy, coping skills and self-care approaches, fall into “treatment resistant” territory.
To me, the answer and the reason why that happens is quite simple: it gets to a point that it’s not an individual fault anymore.
I have to believe in this. I’m doing already everything I can to get better, if I’m not getting better there must be another explanation that doesn’t have to do with me and my efforts. I have had my share of self-blaming and it didn’t help, it never does. At least blaming literally anything or anyone other than myself doesn’t corner me into despair. I can try and have some hope I’ll find a way out.
Maybe you think it’s hard to believe? Society is built upon ableism, culturally, socio-economically and more. Oh, I wonder why things like schizophrenia, eating disorders and depression are so hard to treat... I’m sure it has nothing to do with stigma, sanism and demonization of mental disorders, neurodivergent and fat people, it also has nothing to do with increasing rates of violence and discrimination, oppression, capitalism, the political climate, the environment that’s falling apart... I could keep going.
In my personal case: personality disorders are deemed difficult (if not straight up impossible) to treat, and people with personality disorders are to be avoided at all costs, left to remain marginalized or just thrown under the bus, as collateral damage or worse. Who the fuck cares about these “sickos”, right?
I care. I have to care.
As it stands, my mind is set on dying so I need to keep on going despite it all. It’s hard... experiencing rejection upon rejection, so many doors closing, so many opportunities gone to waste, so much time that has been lost and can’t be recovered. Trying the best I can, doing all these things that are supposed to help, smiling through it all, being positive through it all, trying to keep my head up and stay optimistic through it all.
My mind, I, don’t see another way out. It’s just a matter of time now.
I’m sure I would definitely improve with the right treatment, the right professional and the right amount of time - I know I would because I still feel like I’m so close to finding a satisfactory answer(s) - but when I’m faced with reality, the lack of a support system gets to me, and so do all these barriers to accessing treatment, and so does existing in a society that either/or don’t care about me, don’t see me and don’t want me here.
I don’t want to die, and I don’t want to live a miserable life either.
It is all really painful after all...
9 notes
·
View notes
Text
Finding the Best Skin Doctor in Chandigarh
When it comes to taking care of your skin, finding a qualified and experienced skin doctor is essential. Chandigarh, known for its high-quality healthcare facilities, is home to some of the best dermatologists in India. Whether you're dealing with acne, pigmentation, hair loss, or other skin-related issues, having a reliable and skilled skin doctor in Chandigarh can make all the difference. In this blog, we'll guide you through everything you need to know about finding the right skin doctor in Chandigarh, with a special focus on Ageology, a leading dermatology clinic in the city.
Why You Need a Skin Doctor in Chandigarh
Skin problems are more than just a cosmetic concern; they can affect your self-esteem, comfort, and overall well-being. Chandigarh’s climate, lifestyle factors, and increasing pollution levels can contribute to various skin issues, making it crucial to seek professional help when needed. Here are a few reasons why consulting a skin doctor in Chandigarh is beneficial:
Expert Diagnosis: Skin conditions can often be complex, with symptoms that overlap. A qualified dermatologist can accurately diagnose the issue and recommend appropriate treatment.
Customized Treatment Plans: Every skin type is unique, and a one-size-fits-all approach doesn’t work when it comes to skincare. A skin doctor will provide personalized treatment plans tailored to your specific needs.
Advanced Technology and Treatments: Modern dermatology offers a wide range of advanced treatments, from laser therapies to chemical peels. A skilled dermatologist in Chandigarh will have access to the latest technology to treat your skin condition effectively.
Prevention and Maintenance: Regular visits to a skin doctor can help in preventing future skin issues. They can guide you on how to maintain healthy skin and avoid potential problems.
What to Look for in a Skin Doctor in Chandigarh
When searching for a skin doctor in Chandigarh, it's important to consider a few key factors to ensure you receive the best care possible:
Qualifications and Experience: Look for a dermatologist who is board-certified and has extensive experience in treating various skin conditions. Their credentials and years of practice can give you confidence in their ability to handle your concerns.
Specializations: Dermatology is a broad field, and some doctors may specialize in areas such as cosmetic dermatology, pediatric dermatology, or hair loss treatments. Depending on your needs, it’s beneficial to choose a doctor who specializes in your specific concern.
Patient Reviews and Testimonials: Patient feedback can provide valuable insights into a doctor’s approach, bedside manner, and the effectiveness of their treatments. Check online reviews or ask for testimonials from previous patients.
Clinic Environment and Technology: The clinic’s environment should be clean, comfortable, and equipped with the latest dermatological technology. This ensures that you receive safe and effective treatments.
Availability and Accessibility: Choose a skin doctor who is easily accessible and can accommodate your schedule. Consider factors such as clinic location, office hours, and ease of booking appointments.
Ageology: Your Trusted Skin Doctor in Chandigarh
If you’re looking for a reputable and experienced skin doctor in Chandigarh, Ageology stands out as one of the top choices. Ageology, located in the heart of Chandigarh, offers comprehensive dermatological services tailored to meet the diverse needs of its patients. Here’s why Ageology should be your go-to clinic for all skin-related concerns:
1. Expert Dermatologists
Ageology is home to a team of highly qualified and experienced dermatologists who are well-versed in treating a wide range of skin conditions. The clinic’s doctors are dedicated to staying updated with the latest advancements in dermatology, ensuring that patients receive cutting-edge treatments.
2. Comprehensive Skin Care Services
Whether you’re dealing with acne, aging skin, pigmentation issues, or hair loss, Ageology offers a broad spectrum of services to address your concerns. Some of the key services include:
Acne Treatment: Ageology provides effective solutions for all types of acne, including hormonal acne, cystic acne, and post-acne scars.
Anti-Aging Treatments: The clinic offers advanced anti-aging treatments, including Botox, fillers, and skin rejuvenation therapies to help you achieve a youthful appearance.
Laser Treatments: Ageology utilizes state-of-the-art laser technology for hair removal, skin tightening, and pigmentation correction.
Hair Loss Solutions: From PRP therapy to hair transplant procedures, Ageology offers customized treatments to combat hair loss and promote healthy hair growth.
3. Personalized Care
At Ageology, patient care is the top priority. The dermatologists take the time to understand your concerns, conduct thorough evaluations, and develop personalized treatment plans that cater to your unique skin type and condition.
4. State-of-the-Art Facilities
Ageology’s clinic is equipped with the latest dermatological technology, ensuring that you receive the highest standard of care. The clinic maintains a clean, hygienic environment where you can feel comfortable and confident during your treatments.
5. Positive Patient Experiences
Ageology has garnered a strong reputation in Chandigarh for delivering exceptional results and maintaining high levels of patient satisfaction. The clinic’s commitment to quality care is reflected in the positive reviews and testimonials from its patients.
Conclusion
Your skin deserves the best care, and finding a reliable skin doctor in Chandigarh is the first step toward achieving healthy, glowing skin. With its team of expert dermatologists, advanced treatments, and patient-centric approach, Ageology is an excellent choice for anyone seeking top-notch dermatological care in the city.
Whether you’re dealing with a specific skin condition or simply want to maintain your skin’s health, Ageology offers the expertise and services you need. Visit their website at Ageology to learn more about their offerings and to book an appointment with one of their experienced skin doctors. Taking the time to invest in your skin’s health today can lead to a brighter, more confident tomorrow.

0 notes
Text
of the person of my past
throughout our relationship and especially at its end, i was being diagnosed with mental disorders by the person i loved as if doing everything in their power to determine why i would leave the relationship, rather than instead taking into account everything i'd ever shared with them throughout our years together. so much was disbelieved, dismissed, and deleted in place of a reality more comfortably curated in their mind
they danced around bipolar, borderline personality disorder, and finally settled that it was covert narcissism at the end of it all, something so utterly far from who i am as a person you'd think it a bitter form of a cruel joke. i can’t lie that us coming out of a relationship as long as ours was, with all that we shared and enjoyed and experienced together, that them throwing out a misguided misdiagnosis like that one, damaged me in a way that felt irreparable at times, especially with the realization they truly are convinced of it themselves. that to them, it went beyond an extreme punishment clung to during the difficult pain of a sudden breakup, but became a truth they felt applied to the entirety of our relationship. i was physically sick over it, and still can be
always a strong believer in not feeling pressured or obligated to stay in a relationship you deep down feel isn't working, i constantly reminded them it was forever a free, nonjudgmental situation to leave at any point. i avidly support individual happiness more than all else, more than a people pleasing loyalty to any form of relationship
but with every genuinely concerned moment i expressed they didn't seem happy with me, with us, that they should leave to find something fit to their own idea of happiness, it was "no, i love and am happy with you" and "no, i know what i want and i want to stay" and it seems foolishly for us both, we stayed
the false diagnosis brought an ache that wrapped around what felt like my heart, the very core of me. yet i tried to see it from where they were coming from. a place of pain and perceived betrayal and abandonment. i imagined it came from a place of: "why, after so long, would this happen? why would they do this?"
it was quick that i was able to take the reasons they attributed to my given narcissism and wildly spiral in obsessive worry, guilt, and confused overthinking. i researched and asked questions of multiple different doctors over these following years (i wouldn’t trust just a single - even second - opinion only) if it was possible to be a narcissist without realizing, if my actions were really borne of those intentions. because the idea of it scared the hell out of me and had me constantly, sickly anxious that I didn’t know myself. i ended up learning a lot about a topic i never thought i’d have to. realized how simple it can be to assign false mental illness of this variety to almost anyone, especially in the relationship-breakup dynamic, if you’re looking for it. which according to numerous doctors and sources, is something that's become a pervasively common (and inaccurately harmful) practice
ironically, signs of narcissism i found easily in them, all from my research into their self-diagnosis of me (https://www.verywellmind.com/signs-of-a-vulnerable-narcissist-7369901). this article, for example, is almost eerily word-for-word what i remember of them, rather than personally applicable. i learned this could also tie into their tendency toward projection, which was a common theme throughout our time together. would i diagnose them with the narcissism this research, discussion boards, and medical journals almost convinced me they’d had all along, though? no; not only am i not a doctor, but it’s not how i like to operate. not even after years of knowing them, i wouldn’t feel confident or right in doing so. there‘s so much background context to every behavior that doesn’t necessarily need to be an assigned a specific illness, especially with so much unique and varied overlap
the person of my past had a rough upbringing with their parents and with their peers and likely continues to. all of what they have and may not have had and are going through, i realize they’re just a person whose ultimate want is to be loved, and i genuinely hope this for them in whatever form that may take. it was all i wished while I knew them, while i’d truly loved them, that they felt as happy as was possible, felt comforted and loved, and that they always had freedom in their own life; when I left, i still wished this for them, but knew it could no longer be with me. the compatibility for us both to experience those things with each other would never be there, and while it was shitty and sucked when the dream had been an everlasting love, there also had to be acceptance of this not being the case, as discovered over time, and inevitably having to choose what’s best for yourself, if not each other
finding out through numerous sources that claiming an “ex is a narcissist/covert narcissist” is a commonplace phenomenon despite the true rarity of this kind of disorder, that it's an even slippier slope that many in society who have experienced a breakup fall into, was an eye-opening moment. it's been found far more likely a breakup is caused by an intrinsic incompatibility of either understanding, communication, or both between two realistic, flawed people
long story long, with help from kind, thorough, and informative doctors as well as people who have known me since birth, i finally reached a point of peace i’m not in any true sense what was assigned to me by my ex. a dismal part of me almost wished i were, as it sounded easier in the way of not caring so obsessively about it. it was heartbreaking someone i’d loved could believe that of me, and why if they did, they repeatedly insisted on staying with me for so long. pretended they were the happiest they've ever been. i could only ask myself, were they suffering with me that whole time, and why did they decide to never tell me? why did they never listen to my repeated concerns, and instead dismiss them as wrong?
i admit while i ultimately got though this crisis, i did wield some extreme coping mechanisms that were likely to have triggered additional trauma at our relationship's end, and possibly been a part that led into their scrambling conclusions. since then i've managed to further deep-dive and work on these coping mechanisms (and have come a long way); however, at the time of the breakup years ago, i mentally shut down due to an immense fear of my ex’s extreme reactions i’d faced in the past; i was worried i'd allow myself to slip back into the relationship as i did in my previous attempts to leave if i didn’t detach myself from it in a more resolute way, a way where they couldn’t convince me to hang on or “try again.” i do regret this shut down, as i prefer to feel everything in its entirety and be more present in the moment, but like them, i had a pretty rough background that could feed this coping mechanism, and it existed long before we knew each other
this mechanism was like a switch was flipped, nothing but a distant, polite detachment that led me through our last, admittedly still-traumatizing moments. i regret it now, because it's clear it didn't help either of us in the way of closure and to the point i couldn’t share anything about the horrible fallout our relationship caused in this depth
but i hope by sharing all i have here and in other posts, others may relate and realize they are not alone. that no matter what another insistently deems for you, whether purposely or due to dark emotions of their own, it doesn't mean that it ever was or is you
i truly believe most of us don’t want and aren’t trying to be purposely cruel to one another, that most of us don’t have that rare, true lack of empathy that aims to cause pain. we’re all unique, complicated humans bumping into one another, simply trying our best to get through it
0 notes
Text
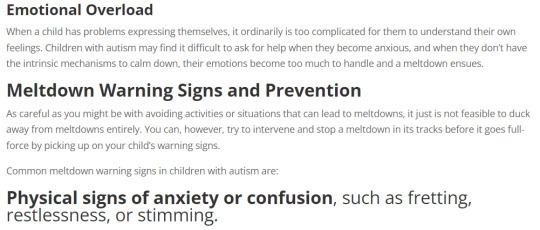
Gus Porter is autistic - Meltdowns and self-esteem.
So. Season 2 episode 18, Labyrinth Runners, huh. Tbh I’ve never seen Gus as autistic even tho I saw a short headcanon post here and there, but this new ep? Holy hell guys. This is as canon as it’s going to get, I cannot be convinced otherwise, and I’m pretty much convinced it’s intentional. This single-handedly made me love Gus much more, and I now hold him dear to my heart. If you wanna skip to the new ep stuff, go to the keep reading section.
First of all, let’s have a rundown of possible autism traits Gus has shown so far:
1- Like the others, he’s somewhat of a misfit and doesn’t have many friends.
2- Special interest in humans. Leads to rambling/infodumping and excitement, I’m specifically thinking of the whole “human” nickname scene but there are tons of examples of that.
3- His special interest in human culture is driven by a curiosity, the want to amass knowledge about it, and he likes to makes theories about it, like why humans get wires to their teeth. It’s kind of like a puzzle, but it’s also a whole rich world and culture to explore and, relatable. I couldn’t find a clip of it but iirc he explains what he likes about illusion magic at some point and it felt very in that same vein as well.
4- Speaks to himself pretty regularly. (Irl with asd it’s usually either to help sensory/emotional processing, but can also be because of a lack of awareness of social norms or even control)
5- Socially awkward gifted kid nerd trope. Self-explanatory.
6- Sometimes says rudely blunt things, seemingly not knowing it’s the wrong thing to say. Ex: Willow: “We weren’t going to leave you behind.” Gus: “I was.” Willow: “Gus!” -elbows him- (important to note it wasn’t in a sassy or bitter manner) / “Don’t worry, we’ll get you out, dead or alive!” -Willow looks at him and shakes her head. Gus sees that, his eyebrows rise and his expression shift- “Okay, alive!” / Even thought it’s magic, the “Better luck next time!” and “goodbye forever!” messages feels like an instance of this as well
7- That goes hand in hand with not being able to read a room. Ex: Willow, worried/horrified: “Luz is in a witch’s dual!” Gus, excited: “Yeah, and she can win it all! Yeah yeah!” -epic finger guns-
8- Generally a stickler for rules and knows a lot about cultural history of the Boiling Isles. He can remember specific rules and dates, etc.
9- Strong moral code, thinking of the illusion graveyard ep specifically. (that’s not a diss, rigid morality and unlikeliness for corruption really is extremely common in autism and a diagnosis trait)
10- A certain social obliviousness. With overcrowding Willow, getting betrayed by fellow illusion coven students, and I couldn’t find a clip of it but iirc most Human Club members weren’t as excited about human stuff as much as he thought
11- ”Gus chomp”? This boy just dissed every existing social norm ever
12- Self-esteem issues due to social problems and perfectionism, as well as feeling like his special interest/skill (illusions) is useless/dumb and wanting to change that about himself.
Here’s a good compilation to see many of those in clips: https://www.youtube.com/watch?v=ISSkcKdzN6s&ab_channel=Milasia
Ok. Um... I didn’t think that’d be so long. Well that used to not be enough evidence to sell me on the headcanon, so below the cut we get to the new ep! Beware spoilers!
The angst? Delicious. Relatable.
There’s obviously the obliviousness and naivety + hard time reading people of Gus thinking he’s friends with a classmate after they teamed up to work on 1 project together once and said classmate left all the work to him. Gus didn’t notice him/think much of him not working on the assignment at all and said “we’re practically best friends now!” before he learned the truth from accidentally eavesdropping. To think you’re best friend-level getting along with someone who was obviously using him, like let’s be honest the dude didn’t look like he’s a very good actor and the vibes are very much rather that Gus is very easy to fool, especially since Gus says he “did it again”. “Why does this keep happening?”.
This isn’t a “kid learns a lesson that some people will pretend to be his friend for their own gain” thing, this is a “it happens again and again but Gus can’t see the warning signs”. He’s confused. He doesn’t get it. This is a fundamental social thing that he cannot identify, that he does not learn from no matter how often it happens to him. “What’s wrong with me, why can’t I learn?”. I’m sobbing y’all. Undiagnosed autism right there. He knows something is wrong, but social cues just do not click, and he doesn’t have the tools or knowledge he needs to know why he can't read them. He can’t tell when someone likes him or not, leaving him to wallow or overanalyze social interactions or friendships sometimes, like when he was sad over overcrowding Willow.
And it’s not like he never got any trust issues either, after all he pushes away Willow at first, and wouldn’t believe Hunter’s comfort until he did the breathing exercise.
The confusion, the trauma, the anxiety, the sheer emotional turmoil of hurt and betrayal and the crushing of self-esteem for not being able to tell. “Everyone thinks I’m the smart one, so why do I keep acting so dumb?” “I can’t even trust myself [my perspective of what’s happening] anymore.”
Meltdowns share similarities with anxiety and panic attacks, because it comes from what I listed just above. This? Is a meltdown.


This isn’t just a panic attack. This is an outburst, a coping mechanism, even if it is characterized by intense emotions and stress and a loss of control.


Source: https://www.rdiconnect.com/what-is-an-autism-meltdown/ (don’t mind it being mainly written for autism moms)
It isn’t necessarily written the best way for the purpose of highlighting Gus’ situation, and meltdowns can also be from sensory overload and others, but Gus’ is obviously because of an emotional overload. Hunter coming in with the breathing exercise shows that he had to calm down for it to stop as well. This may be one of the most powerful visual representations of a meltdown I’ve ever seen. Meltdowns cause you to explode and often lash out, it’s not just internal or even crumbling down alone in a corner, it’s compared to temper tantrums and you can hurt others. Which is why the illusions are affecting others as well, not just him, despite them being caused by him because of his emotional state, and that he doesn’t want it to happen. It sucks for everyone involved and it’s very overwhelming.
As an autistic who only got diagnosed at 18, who learned that she had 0 friends when she thought she was bestie with all her classmates because everyone pretended, who when I look at memories of being tricked I can see obvious signs of dishonesty when it just didn’t register at the time, this resonates so, so much. Result: I got social anxiety, but overanalyzing everything and bending myself for other people didn’t help, I still got taken advantage of and thought of as annoying, though self-improvement and learning more about social stuff did help as I grew up. I was a gifted kid academically, but couldn’t tell who’s a bff and who literally could not wait to get away from me. Time and time again. And yeah, most of the time I learned through accidentally hearing something they didn’t want me to.
If you’ve watched She-ra and the Princesses of Power or you know a fair bit of pop culture, you can see huge similarities in Gus and Entrapta, who is confirmed to have been intentionally written as autistic. And that similarity is the confusion when it comes to social situations and betrayal.
It’s not that they’re not trying, or that they’re dumb, it’s that they genuinely can’t tell when someone likes them or not and such. In both cases, it causes deep self-esteem issues and trauma. It’s honestly heartbreakingly relatable to see their eyes widen in realization when the bubble gets popped and it becomes obvious and explicit that the friendship they thought they had was a lie. It’s even more heartbreakingly relatable when statements such as “I’m supposed to be smart, so why do I keep acting so dumb” and “I can’t even trust my vision of the events” and “I just wasn’t suited for friendship” be like... True, y’know? It’s not just an exaggeration of their feelings or 1 bad experience, it’s how we are, and we just have to cope with it, accept it and find a good entourage we can trust.
This is a good compilation of Entrapta angst if you’re interested, huge spoilers beware: https://www.youtube.com/watch?v=zrW54RZFTAQ&ab_channel=tlr748
Also on the note of several main characters showing numerous signs of autism or other neurodivergences: Neurodivergent people tend to gravitate to each other, which makes our main TOH cast of misfits all/most having some neurodivergence not surprising or “unrealistic”. A diagnosis shouldn’t make them any less loveable to you. Though, of course, we’re all entitled to our own opinions and visions of them & that’s valid. /gen
Thank you The Owl House, for keeping delivering with the great rep
Not me crying writing this, no u, nothing more to see here
#the owl house#gus porter#autistic headcanon#my posts#my content#asd#autism#analysis#character analysis#labyrinth runners#augustus porter#actually autistic#autistic#autistic pride#angst#meltdown#relatable#autistic gus porter
231 notes
·
View notes
Note
speaking of college boys, what do the college au aot babies study??
Okay, okay, I think I’ve talked about this in an ask before but I can’t find it 😭😭 but it’s okay, I love college aus, so I’ll talk about it again! Plus, now I’ve got more thoughts for more characters, so here we go
Levi — neuroscience and psychology of human behavior
He started out on track to do a bachelor of arts in psychology, but when they touched on the anatomy and biological parts of it during his first year lecture, he switched to a bachelor of science.
The focus is still psychology, but through a more clinical lens. Essentially, he gets the best of both worlds this way. He’s intuitive and analytical, so clinical and mental diagnosis is easy to dissect for him. He’s also canonically good at math, so the calculus and stats parts aren’t too bad, either.
This major also leaves him with a few options post-grad, which is a nice bonus for him. He’s likely going to medical school, but that’s not the only route open to him: law school, therapy, lab work, medicine and pharmacy, even teaching are all viable options without going to grad school.
Do not talk to him about Freud unless you wanna get punted off a building.
Be careful with him, because with a single glance he’s already got scarily accurate predictions about your parental and emotional attachment styles, your behavior in social settings, and the onset (or seemingly lack thereof) of your frontal lobe development.
He thinks he’s so smart making comments like, “I see those synaptic connections aren’t working so well for you today,” like mf come here let me lobotomize you and see how well your synaptic connects are working after that🙄
Eren — general health sciences
He’s interested in science and the discovery aspects of it, but picking a specific field of focus right now feels too final. He likes it this way, because his schedule and requirements are less restrictive, and he has more room to find out what really interests him.
He does best when he’s doing something he loves, so picking a major with a bunch of reqs that he couldn’t care less about would have sucked big time for him. It also would have affected his grades. There are still some classes he has to take that he’s not fond of (see: chemistry), but that’s to be expected. Science in general is cool to him and he hopes to make his own discovery some day, even if it’s microscopic.
He also plays a lot of sports, keeping his schedule flexible is important. The sports end up helping him excel academically, which is a nice bonus. Honestly, Eren uses his time at university to learn more about himself than anything, so having control and freedom to do what he likes the majority of the time was important to him.
He uses his elective credits to take philosophy or history courses of his interest, or maybe even a course that you’re in just to spend time with you. He also uses you as a live model for his homework bye, congrats on being patient number one to him.
Armin — astronomy and physics
He’s still interested in marine biology, but unless he attended a school near a coast, or with a specialized integrated program for that, it’s unlikely he’d major in it during undergrad.
Space and ocean exploration aren’t all that different. Both are vast, largely unexplored domains that reel-in Armin’s interest for discovery. So, while studying astronomy, he still gets to study evolution and make his own predictions about what could be out there because there’s so much to know.
Physics comes with the territory of learning about planetary science, and he’s mathematically inclined, so it works out for him. Learning about the different physical properties of other planets and space masses is honestly pretty sick to him. Because math isn’t a struggle, he actually considered aeronautical engineering, but he didn’t want to be a part of the college to military pipeline; that is, he didn’t want any potential design of his to be weaponized.
He still gets to study animal biology through his elective courses, and might even find a few focused on marine animals to satiate him. Plant and cell biology are also of interest to him, and are just further applications of his primary study anyway, so he’s got plenty of room to work with.
This boy is interning at NASA and still, with his whole chest out is like, “I don’t need to discover a new planet, you’re my whole world.” Armin, go check on the Mars rover or something please.
Mikasa — anthropology + minor in japanese language studies
Anthropology is virtually interdisciplinary in nature, and Mikasa is a pretty well rounded student, so she’s able to excel in a program like this. She gets to study history, science, cultural studies, and even a bit of art all at once.
She’s still debating between going to law school vs med school, so anthro this is a good in-betweener. She gets a taste of science through her anatomy and kin courses; and lots of practice with reading and dissecting texts through the historical and cultural lectures. So, when the time comes to decide, she’ll have some experience with both.
Don’t know whether it’s confirmed that she’s (part) Japanese or not, but either way I headcanon that she speaks/spoke some second language at home. She wanted to delve more into it, and courses were offered at the university so why not?
Cultural studies courses end up being her favorite. She likes learning about the history of people and their cultures, and it encourages her to learn more about her own family history and culture. It also propels her to apply for a study abroad opportunity, so she spends at least one semester doing an exchange program and absolutely loves it.
She would also encourage you to apply and go, too. You guys might not be in the same program, but if there’s an applicable program in the same country she’s going to, then she’d definitely want you to apply. Spending the semester away with you would be a dream come true.
Hange — bioengineering + minor in political philosophy and law
It’s almost self-sabotage to be in an engineering program and have a minor; the coursework for engineering alone is backbreaking, and bioengineering has the added weight of human intricacies, but of course Hange makes it possible.
They’re nothing short of a genius, so of course they have time to work a completely unrelated minor into their schedule. It doesn’t surprise anyone that they go on to complete an MD-PhD after undergrad. Insane.
Bioengineering is essentially the synthesis of chemical engineering and health sciences; Hange spends their time exploring biological sciences and applies the engineering aspects of their coursework to their understanding of (and interest in creating) medicine. Truly a one of a kind mind.
They also have an interest in philosophy and justice, so when they found out they only needed a measly nine or ten courses to minor in, they went for it, of course. In honesty, they don’t find the studies all that opposing: both law making and medicine making both have some kind of philosophy or method to them in their eyes.
Hange has... little to no free time pls. They don’t mind it, because they love their coursework, but this means you are essentially ducking into their labs or scrambling to find them in-between their classes during your time in undergrad. They appreciate every second spent with you tho, and will gladly rope you into long discussions about their work.
Jean — biochemistry + minor in art sustainability
He was undeclared his first year, and took a little bit of everything: art, science, history, anthropology, english. Basically, anything that fit into his schedule. It was hard for him to pick one thing—he liked the science and lab applications of STEM courses, but not the math; and the obvious painting and creativity of art, but hated the pretentious air about art history.
What he wants to do is make a difference, which is how he ends up knowing that he wants to go to med school after, so he picks a science-heavy major, but uses his elective spaces to take art courses. When he mixes the two, he ends up on sustainability—and the complexities about it that are applicable to both science and art are what really reels him in.
Interdisciplinary studies end up being his forte. He can approach sustainability from a science perspective which impacts his art style and materials; and tuning into his creative side allows him to think about science not just from a purely clinical perspective, but from a human one, too—patients are people after all.
He believes that everything is connected somehow, even things as seemingly opposite as art and biochemistry. And he works towards finding the unique intersection where everything overlaps. His studies are pretty cool, and he’s very passionate about them, so ask him about it 😌
The art he makes is pretty sick, too, and often commentary about science; he’s proving they’re not so opposite. You also heavily influence his studies in both areas: caring about you so much inspires him to take the healthcare focus seriously, and your very nature is inspiration to his art.
Sasha — nursing
She’s friendly and good at working with people, so nursing was an easy choice for her. She accredits most of her motivation to being around her younger family members, and learns that she finds a simple kind of joy in helping to take care of others.
She struggles a bit her first year when it’s mostly all grades and standardized testing, but when she starts getting clinical experience and working in the hospital on campus, things round out for her.
Patient care is her strongest point. A lot of people often forget that knowing everything isn’t everything; if you don’t know how to calm or even just talk to your patient, you’re not that great of a healthcare professional.
Pretty certain that she wants to work with kids in the future, but she’s open to public health and even being a travel nurse if she finds opportunity there!
Of course, she’s pretty doting when it comes to you and all her friends. She might want to go into pediatrics, but the basics of nursing and health care extend to everyone, so you’re guaranteed to be well taken care of with Sasha around. You might even have to switch roles and take care of her sometimes, because her coursework can get pretty out of hand.
Connie — computer engineering with a focus on game design
He might not look it, but Connie has a brain under that shaved head of his. Computer engineering is cool to him because he basically learns about how simple things he uses every day (ie: phone, computer, microwave) works.
Systems and coding are actually the easy part for him, especially when they get into the application of it and aren’t just stuck looking at examples. That’s how he gets into game design.
The part about math and electricity and magnetic fields… well let’s just say he needed to make friends with someone who likes math and hardware his first year to get through it. But the struggle was worth it, because by his junior year he’s found a professor willing to mentor/supervise him as he works on his game and other projects, so life is good.
His school work is definitely hard, which is why the lives by the mantra of “work hard, party harder.” It’s only fair.
He makes you a little avatar so you can test out his games for him <33 best boyfriend things <33 He’d also… build a game about your relationship. Every level is a different date you guys went on, and he definitely includes something cheesy, like “There are unlimited lives because I love you forever babe <3”
Porco — kinesiology + maybe mechanical engineering
He’s pretty into athletics and working out, but didn’t wanna go down the sports psychology route; he wanted something that left him with a few more options, so he ended up in kinesiology.
He was surprisingly pretty good at biology in high school, so something stem-oriented works out in his favor, and it turns out he’s pretty damn good at anatomy, too. He’ll probably end up in physical therapy after graduation.
He’s also got a knack for cars, which is where the engineering comes in, but he doesn’t care so much for the math part of it (he doesn’t care for it at all actually, fuck that); he just wants the hands on experience of building/fixing things and working with his hands. So, if he can get a minor in it and not struggle through 4 years of math, then he’d do that. If not, he’d take a few workshop-like classes.
Because he wants to go into physical therapy, you are essentially his practice patient. Your back hurts? Not a problem, he’s basically a professional masseuse. Muscle aches? He’s got a remedy and understanding of why it’s happening. Don’t let him catch you hunting over your desk grinding away at your homework, because he will poke your neck and correct your posture (he’ll also massage your shoulders, but after the scolding).
Pieck — classics + minor in philosophy
Ancient studies interest her, but more than that, the language of ancient Greek and Roman culture fascinates her, so classics is the way to go.
Because her focus within Classics ends up being Greek and Latin language studies, she is essentially learning both languages at the same time. She gets farther with Latin that she does with Greek. For whatever reason, the former comes almost naturally to her, so her written and translated work is more complex in Latin.
However, she finds cultural studies relation to Greece more interesting than that of Rome, so it’s a give and take with both; better at languages for Roman studies, better at culture and history for Greek studies.
Her minor is a natural evolution from her primary coursework. Ancient Romans and Greeks set the foundation for a lot of modern day philosophy, so it comes up in her major classes, but she wanted to delve further into the philosophy, and not just look at it historically, so she takes more courses to fulfill the minor.
Can be found laying on a blanket in the quad on a hot day, with her books spread out all around her, highlighter in hand as she works through her reading. You’re always invited to sit with her, and more often than not, it ends up with Pieck’s head in your lap, a book in her hands, and your own schoolwork in yours as you both read in each other’s company.
Bertholdt — computer science and coding
He’s level headed, good at planning, and above all, patient, so he’s cut out for this. He doesn’t consider himself to be particularly creative, which is why he doesn’t pick a speciality with lots of design; but he’s good at streamlining and ideas to life.
The patience really comes in when his code doesn’t run. It’s frustrating to scroll for two hours just to find out that the issue is a missing semi-colon in line 273 that he overlooked, but Berty will sit there until he finds it.
He’s also good at fixing issues. That’s not limited to issues in the code itself; it can mean finding shorter ways to produce the same function or loop, or integrating new aspects into existing code.
Also, he’d just be so cute, coding away on his computer. Just imagine: Berty working on his homework in the library, he’s got his signature crewneck + collared shirt look going for him, his blue-light glasses, a cup of coffee nearly as tall as him sitting at the corner of his desk. Adorable.
He’d make little codes/programs for you, too, even if it’s silly. A simple code that helps you decide what to eat for dinner or where to go on a date, one that shuffles different reminders for you, hell he’ll even forgo the torture of design engineering just to build you a little robot that says “I love you” to you.
Reiner — english + minor in justice & political philosophy
Everyone expects Reiner, star quarterback of the university’s rugby team, to be a business student or communications student; but no, he’s an English major, and he loves it.
Just imagine a guy as huge as Reiner absolutely manhandling someone on the field, just to show up in his lectures with a tiny paperback of The Great Gatsby tucked between his fingers with his reading glasses on. It’s so precious.
He’s always running a bit late to class—either coming from the gym, or practice, or oversleeping from exhaustion—but he’s so sweet to his professors and genuinely interested in the literature that they don’t give him a hard time about it. They can tell that balancing school and sports is difficult, and they just appreciate that he takes his studies seriously.
Yeah he’s in a book club and he dog-ears his books. What about it. They’re doing poetry this month and Reiner actually likes Edgar Allen Poe. Who said jocks can’t be sentimental.
He also reads a lot outside of his classes, and has a soft spot for coming of age stories. He usually empathizes with the main character somehow. His ideal weekend plans after a week of grueling games and essays is taking a long, relaxing shower at your place, while you both share a bottle of wine, and maybe even get you to read a chapter or two of his current book out loud to him.
Annie — clinical psychology/neuroscience
Almost scarily analytical and methodic, so this major was calling her name. Localizing brain legions is… insanely intuitive to her it’s incredible. She’ll be an insanely impressive doctor someday, even if she doesn’t end up working with patients directly.
She doesn’t care too much for the more philosophical/reading heavy parts of psychology. Even experiments and research closer to the social end of the spectrum aren’t all that interesting to her; but the brain science behind it it.
Nobody should be good at cellular biology. Nobody should be able to ace cell bio and neuro and calc and work towards their thesis proposal in the same semester, but Annie proves it’s possible.
Ends up working in one of her professor’s labs by her junior year. She was offered three TA positions working with first year students, but she swiftly turned them down. Teaching isn’t her thing.
She doesn’t bring up her studies to you unprompted, but if you ask her about them she’ll explain it to you. Her notes are color coded and it’s super neat, and very cute; coloring them is somewhat relaxing for her. She usually saves the coloring part for when you guys study together; there’s extra comfort in doing it with you around.
#anonymous#anyways jean kirschtein date me challenge paint me like one of ur french molecules#aot x reader#snk x reader#levi x reader#eren x reader#levi fluff#levi smut#eren fluff#mikasa x reader#armin x reader#jean x reader#jean kirstein x reader#connie x reader#porco galliard x reader#pieck x reader#annie x reader#theres too many of them im tapping out#aot imagines#minicanons
534 notes
·
View notes
Text
Rambling About my Autism: Masking, Self-Exploration and Understanding Eachother
I don’t know if I speak for every single neurodivergent person out there but I don’t struggle with autism. I struggle with other people not having it or not even having a concept of what it is. I don’t expect total empathy but it would be nice if I got a centimeter of wiggle room when it came to social situations without coming across like I want cheat codes for life.

I use the pronoun “my” because everyone experiences autism differently and it’s such a complicated diagnosis that it’s entirely understandable why neurotypical people are very confused by it. It doesn’t help that autism isn’t really touched upon in education or that representation of neurodivergent people in the media is pretty poor. Often, whenever an uninitiated neurotypical person thinks of autism, they either think of edgy internet humour or Rain Man and they’re just as bad as each other in my estimation.
I was diagnosed in Primary School when I was about seven years old but at the time, I didn’t think much of it. I might’ve told some of my friends at school but I couldn’t tell them anything about what it meant or anything. I never understood why my parents took me to this place far out of town where this man in a suit was asking me bizarre questions and conundrums or why I had to leave the room for several minutes whilst the man just spoke to my parents.
I was one of those kids who was steadfastly attached to a counsellor because I had a short fuse in the nursery which carried on until I was about nine years of age. I don’t remember her ever having a conversation with me about my diagnosis. Maybe she wasn’t qualified to speak about it or something, I don’t know.
Anyway, I only really took notice of it when I was fourteen because I started to realize that I was missing pieces of puzzles all the time. Throughout school, I had a terrible fear of failure in the sense that I didn’t want to try and do anything without very specific instructions because I was scared of the consequence of doing it wrong. People would tell me jokes and I wouldn’t get them. I would miss social cues sometimes. I was overly self-conscious of things that “normal” people aren’t supposed to be self-conscious of like the size of my shoes.
Then, I was worried about telling anyone because of the stigma attached to it at the time. Being raised by the internet mostly, people made fun of autism all the time and not in a particularly fun way. Being autistic meant that you were stupid and sub-human. I feared facing direct harrassment in real life so I left it alone for a bit. Only my friends knew about it.
It wasn’t until I was about eighteen where I realized that it was something special about me; it was part of my character. I read more about it. I talked to people online who also had autism or they were concerned that they might have it and encouraged them to be diagnosed. I was exploring it and I realized that it was more interesting than I thought. I embraced it. One of the very few good things about the internet is that you are allowed to be who you are and find other people who are the same as you. I know this is because of social engineering and advertising etc but still.
To this day, I still live with it and it still does bother me from time to time but I feel like part of being human is self-exploration and learning to live with yourself. There are still times where I act irrationally because I’m socially paranoid which is an off-shoot of me being a constant thinker. There is still a fear of me doing or saying the wrong thing to upset people or that I’m misinterpreted. Not having many friends at school, I’m keen to get attached to people but I get quickly overwhelmed and anxious. I would still probably suffer a sensory overload in nightclubs which can lead to something like panic attacks All this is part of learning about yourself and it’s a disservice to not try and address it. Not to solve it, but to realize who you are and accept yourself.
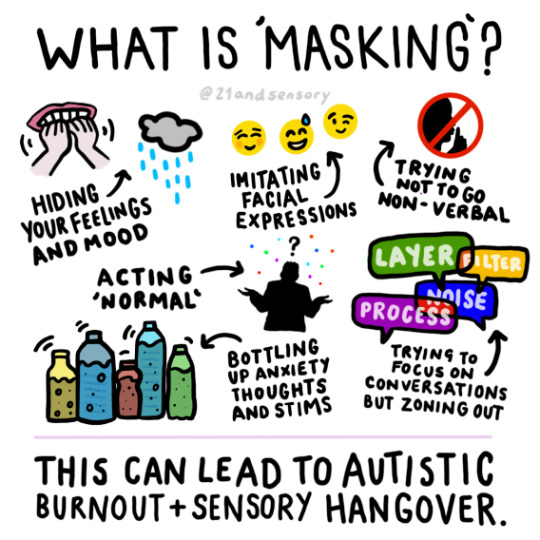
What some neurodivergent people are self-conscious of is the idea of masking. This essentially means that you hide autistic behaviours by doing an impression of a neurotypical individual which is a practice that is definitely unhealthy. I’ve been guilty of this throughout university when I’m rubbing shoulders with people I barely know because there is an element of safety in it. Ultimately though, you should be allowed to be yourself in real life and I do know that there are some people who see my overanalysis in conversation and wished that I would shut the fuck up. What I say to that is that there will be people like that anyway if you’re autistic or not and we should work together to normalize being who you are. “Normal” to me is who I am.
Really, I’ve had it easy in comparison to other autistic folk. Some won’t find out for ages that they’re autistic because they don’t have anyone around them showing concern or, if you’re AFAB, you have to jump through all these hoops because of the inherently sexist industry. In 2021, the “woman are just hysterical” viewpoint is indeed, still a thing. I spare a thought for people who are getting diagnosed after their teens when I got diagnosed in about an hour. To those people, I encourage you to keep pressing forward with it and to not give up getting the help and support you need. It’ll be alright because it’s not as scary as Rain Man makes it out to be.

If there is anyone reading this who is concerned that they might be autistic or that they know someone who does. I say that you don’t need to be concerned. If you want to be diagnosed, push for the diagnosis but if you can’t or you don’t want to. That’s fine too. Do what I did. Reach out to other autistic people and talk to them. Join a Discord server and have a chat because there are more neurodivergent people out there than you might think and they are all looking to open the conversation as well.
Outside of that, I don’t know where this was going. Just try and understand each other.
#autism#autism awareness#neurodivergent#neurodivergencies#asd#autism spectrum disorder#autistic#mental health#wellness#mindfulness#ally#nd#aspergers#neurodivergent blog#mental health blog#masking#autism masking#autism in girls#autism in women#autism representation#representation#neurodivergent representation
123 notes
·
View notes
Text
Elderly Black man with autism and anxiety
@xcherry-popx asked:
I have a Black man in my story. Some main features of him include 1) being an older (60+?) man and 2) being rather nervous (and likely having anxiety). I've also considered him having autism, but I wanted to handle the anxious aspect first since it will be more prominent.
when creating him, I started out with the idea of an anxious older man and then decided on race. I'm still working on how his anxiety tends to manifest, but my current thoughts include some anger (not violence) and self-soothing in ways like running his hands through his hair. [autism + anxiety is ownvoices]
my main concerns are that:
A) having his anxiety manifest in anger could be seen as an Angry Black Man, even if he doesn’t hurt anyone (this is in a story where there are some incidents where someone is attacked by someone else, so its not as if his anger is being toned down for the audience)
B) his anxiety-autism could be seen as infantilizing him (its not immediately obvious, and he is seen as a father figure by many of the other characters. he will probably mostly grow stronger on his own rather than relying on the rest of the cast [if he does use their help, its more indirect, such as someone’s courage inspiring him or another nervous character working through their problems together])
I haven't heard a whole lot about 'weak’ (used very loosely here) Black man stereotypes, but i wanted to double-check since i know i dont have a whole lot of experience
Do you think he may come across as an 'infantilized Black man’ stereotype, or to a lesser extent, an 'Angry Black Man’ stereotype?
[ask trimmed due to length]
The possibility that he’s undiagnosed
Depending on the context of the story, it wouldn’t surprise me if his autism and anxiety went undiagnosed (mental health can be a taboo among some Black communities). So one of the questions is : does he know or not ?
Dealing with emotions / how he handles things
Also it’s hard to deal with really strong feelings, sometimes irrational when you don’t know why you react like that. Being undiagnosed could explain his anger. But judging by his age, he could have learned to live with it ? We don’t know his personality and his life so it’s hard to tell.
Also, I don’t see anything wrong with not being strong or just having weaknesses. It’s human. You just have to take your character’s past into consideration when writing about it, but the rule for the story is that he must evolve. It doesn't mean he should finish entirely strong, without any weaknesses. It’s all about change and being a better person (or not, it depends on your themes and the message you want to convey).
He hates being helped ? He learns to accept it and ask for help when needed. This is evolving. He could also find a relieving practice to sooth his anger, or that helps him control his emotions. This is evolving too. Or it could get worse, he could totally close up to the others because of the frustration of not being understood, of feeling weak for needing help. That’s life. He’s old and sometimes, people just stop trying. But again, I don’t know what your story is about so I can’t tell you if you should go towards a positive or negative character’s arc. Just remember : it’s all about his evolution.
Anyway, there’s only one thing that will probably prevent you from falling into stereotypes : make him as human as you can, with all his qualities and flaws.
- Mod Lydie
First of all, I second everything Lydie said, especially that first paragraph.
Undiagnosed (potentially) & coping
Being able to write part of this character from experience will be helpful, but you noticed correctly, being a Black man on top of that does have an impact. Like Lydie mentioned, he could easily have gone undiagnosed. There is a taboo in some Black communities, but keep in mind misdiagnoses and lack of professional support can happen as well. Though there are great psychologists out there, there are also those who will be influenced by racial prejudices, who simply won’t take people seriously, and Autism is still poorly understood outside of stereotypes a lot as well.
Going undiagnosed or even just a late diagnosis really impacts a lot of one’s experiences growing up and how you see yourself. It could be another deeply influential part of his identity that mixes things up again so do keep in mind if this is the case for him. Especially when he’s reached 60+, comorbid is very common aside from the anxiety (depression and C-PTSD come to mind). Not that you need to put those in there, especially because it really depends on his background and direct support group, but something to keep in mind as you further flesh your character out.
At such an advanced age one will probably have learned to mask a lot (though a turn to masking less can be seen in older people, especially men, as well). They might have grown used to being different, including feeling misunderstood, frustrated, could become withdrawn or a people pleaser as a coping mechanism, but all of this is all highly dependent on their character as well as their experiences.
Dealing with his anger & stereotypes
Thinking outside of the box of how anger can manifest could help as well. Sometimes people express their anger in less obvious ways, or the anger could be hidden under a secondary emotion. His anxiety and Autism will probably be affected by each other as well. Like sensory overload coming hand in hand with anxiety attacks of one leading to the other.
Your concern for having him turn into or interpreted as an angry Black man stereotype is something to look out for. Make sure you fully develop his character, show him to be multifaceted, and give him agency.
I personally don’t see how he’d be seen as infantilized as you described him in your concern B paragraph. It sounds to me like he’s doing to opposite, trying to be hyper self-reliant, but yeah, depending on how you let his anxiety and autism manifest, it could be an issue. It’s hard to really say a lot more than this without more specifics.
Characterization
To me, this character comes across as one who could have a lot of depth and complexity to him. He would be flawed, he would be interesting, could easily be made relatable as well. But as you guessed, it will take work, care and research to pull him off without falling into potential pitfalls. Having weaknesses and having your character grow is a good thing (and mentioning for anyone who needs to hear it: Autism and Anxiety are in itself not character flaws or weaknesses, but they can lead to someone manifesting them). This is not only due to the stereotypes, but also because there’s not that much rep out there and you will be battling against ingrained biases and stigma as well.
That said, this is the type of character I always look forward to reading.
- Alice
#Black#black men#autism#anxiety#mental illness#characterization#character design#angry Black man#asks
241 notes
·
View notes
Note
(Thank you)
1. Can you be a system with absolutely no idea what caused you to split? Or to not be aware of your trama at all?
I’ve only very recently come to terms with the fact that I have trauma and haven’t done any work on it yet. I don’t have an event I can point to and go “this traumatized me.”
2. What does it feel like to have an alter front?
3. Are systems usually aware they’re a system before they’re diagnosed?
4. Do alters always know what they look like beforehand? Previously I thought alters knew everything about themselves but one of the answers I got mentioned hosts sometimes helping to figure out names.
I'm curious what kind of answers you've gotten to these so far that made you seek us out, of all people, lol
1. Can you be a system with absolutely no idea what caused you to split? Or to not be aware of your trama at all?
Absolutely, both of these scenarios are not only possible, but completely normal. We're going to switch these around and talk about them in the opposite order, starting with, "not aware of trauma at all". The purpose of a system is to hide trauma. When you're young and going through traumatic situations, and you dissociate, what usually happens is one of two things. Either the child mentally goes away (dissociates, imagining being in a different situation, ignoring what's happening to them in the moment), or they imagine actually being someone else ("this isn't happening to me, it's happening to someone else, I'm (fuck it, uh) Zoro, and I, Zoro, can handle this"). Both of these scenarios lay the groundwork for the creation of a system, and both cases lead to the loss of memory of traumatic events when a child experiences that extreme level of dissociation over prolonged periods.
What this means is, there is no one event that creates a system. It's event, after event, after event, until the child can no longer form a cohesive sense of self. They've become too reliant on dissociation as a coping mechanism, these dissociated parts have taken on a life of their own, and a child's identity has become so fractured and they're so confused that they can't tell who or what they are, and the memories of why are scattered between these parts.
It's not as easy as pointing to an event and saying, "That was it. That was what happened, that's what did this to me-- to us."
This sort of plays in to the next point of, "why did a specific alter split." And this can apply to childhood, later, hell, today, ten years ago, fifteen years from now. It's not always as easy as pointing to a specific event for each alter, either. Some alters take months and years after an event to come forward and make themselves known. This can make pinning down their "origin" almost impossible. What made them could have happened a long time ago. Sometimes it's not a specific event, but a combination of several events, just like in childhood. Are your parents always fighting? Maybe, by the tenth time they're blowing up at each other and you're curled up in your room trying to ignore it, a part finally splits to help you handle that stress. It wasn't specifically the tenth fight-- it was the combination of ALL of the fights.
2. What does it feel like to have an alter front?
This depends. I'm old. I've experienced a lot of different feelings when someone else fronts. When I was kid, it sometimes felt like I was asleep. No memories of it, just blissful darkness, no real time loss, things would go dark for what felt like ten minutes, and then I'd be back, several hours later, barely even realizing I had missed an entire day. I also had pretty bad maladaptive daydreaming, and sometimes I would go into my daydreams while another alter took over. I just thought this was normal. I was just REALLY good at multi-tasking, you know?
When I got older, and I learned more about what was happening, sometimes it would feel like a battle to the death-- two of us fighting desperately for front. Sometimes it honestly felt like a punch to the head-- a knock out when I lost, unpleasant darkness, fear, anxiety, what was I going to come back to? Other times, when I won, I was left with a massive headache and exhausted. Sometimes I welcomed the break, and over time, it became easier. It became like watching things happen through a foggy window. Sometimes I wanted to do something, and I couldn't, and sometimes I felt helpless and lost. As communication got better, I could see more clearly, I could ask for things to happen, I could occasionally... steal a moment, use a hand, set something straight on the counter that was bothering me.
When an alter fronts, it can feel like a lot of things, depending on the situation, depending on communication levels. There's no "one way" or "right way".
3. Are systems usually aware they’re a system before they’re diagnosed?
I would say, in the age of the internet, it's more likely than not that someone is aware they're potentially a system, than it is for them to be completely unaware at the time of diagnosis. Before the internet, before you could just google symptoms, a lot of people weren't aware prior to diagnosis. Even these days, it's not unheard of for someone to only find out around the time of diagnosis, because you don't always realize you're losing time, or have amnesia. Your alters aren't always so completely different that the people around you notice and point it out. The entire point of this disorder is for it to be unnoticeable. It really just depends on the person, their exposure to information about the disorders, and how bad their dissociation is. Some know, some don't. Some go seeking therapy for help with other issues and eventually it just comes out over time that you have something else going on. Sometimes you suspect, and you go to therapy specifically for it. It's different for everyone.
4. Do alters always know what they look like beforehand? Previously I thought alters knew everything about themselves but one of the answers I got mentioned hosts sometimes helping to figure out names.
Not at all. It's actually really common for alters to be... essentially blank slates in the beginning. Let's look at the example above, of the child dissociating out of a bad situation. If they're going away into their daydreams, the body is essentially left unattended. Any alter that forms in that moment could considered to be "blank" at the start. In the other scenario, you know who Zoro is, what they look like, what they like and dislike, what their history is. It doesn't even need to be a character you know of, maybe you, like me, had MaDD, and you'd become one of your characters, your OCs. I had one.
She was strong and had superpowers and was beautiful and confident-- and that was one of my first alters. I imagined being her often enough that I could eventually take the other route, disappear into my mind while she handled it herself (this was totally normal multi-tasking, apparently). She knew who and what she was right off the bat. What she looked like, her history, her personality. In the first scenario, that alter may or may not come up with that information on their own. They may remain blank until communication is good, and then they might start to grow, maybe you do help them find a name, maybe they find it years later on their own. Again, there's no "one way". It depends on the circumstances.
-
You sent a second ask with some more questions, and I think this leads into the next one.
Is it normal for an alter to feel more comfortable in the body than the original host?
Like, you look in a mirror and you think “yeah this is [alter name]” Not really as a negative or positive feeling, just a neutral and true one. Being trans (or mistaking the presence of a different gender alter [the alter in question] for it?) might also effect this.
This can happen, yes! In the case of my OC/alter, of course she looked like me. She was everything I wanted to be when I was a child. She can look in the mirror and say, yup, definitely me. This is what I've always looked like, and I'm perfection.
I have another alter that just... isn't bothered by appearance. He looks in the mirror and it's like, "yup, I guess so, cool -finger guns-"
There's a lot of reasons some alters might be more comfortable in the body than others, and they're all totally normal.
-
And finally. The last question:
What is a tupla?
This is, surprisingly, a very loaded question.
First, right off the bat, the use of the term tulpa is cultural appropriation. I don't claim to be an expert, but to put it simply. The actual practice of tulpamancy is nothing, NOTHING, like what it's being used for in system circles. Here's a really, REALLY good post on how it's been twisted from the original practice and westernized.
The more accepted terms in system circles are willogenic, parogenic, and thoughtforms. These are "headmates" that are intentionally created. They're imaginary friends brought to life through meditation and practice. Some systems claim to be DID/OSDD and say they've intentionally created some alters, making them "mixed origin" (it's more likely that someone has convinced themselves that it was intentional and their choice in an attempt to feel a sense of control over their situation). Some endogenic systems claim to have intentionally created their entire system (which, because on the levels of dissociation needed to create alters, I don't believe is possible without a traumatic origin).
I hope this all helps, I hope it all made sense, if you have more questions, let me know!
23 notes
·
View notes
Note
Have you watched Kati Morton's new video about Maladaptive Daydreaming? What do you think about it?
[intro]
For years, I believed maladaptive daydreaming to be a form of dissociation, but it could also be added to the DSM as its own diagnosis, since it does have its own set of unique symptoms. Either way, at this time maladaptive daydreaming is not listed in the DSM as a diagnosable mental illness.
I was concerned because her last couple videos on the topic were very confusing to watch and seemed to conflate MD with the inner-worlds of DID. It looks like she has done some more research on it and is going to make a more informed video. This is great and I deeply appreciate that she’s taking the time to do a proper dive into this.
The closest diagnosis would be DPDR, or depersonalization derealization disorder. And this is the diagnosis given to those of us who struggle with dissociation. [explanation of DPDR]
Gonna need you to source that Katie, I’ve never heard an MD researcher say something like this. When they talk about MD they call it a behavioral addiction with OCD features which is related to dissociative absorption (different from derealization and depersonalization, these two dissociative experiences are not particularly significant in MD, though they can happen.)
These experiences are extremely common. It's estimated that half of all adults have had at least one episode of DPDR. 50% of people. That is a huge amount of people.
Cool but not sure it’s at all relevant to the video topic.
Also, it's important to mention that in 2016, four researchers put together the Maladaptive Daydreaming Scale, or MDS. This is a 14-item self-reported scale, meaning that you as the patient answers 14 questions based on your own maladaptive daydreaming experience.
It’s a 16 item scale now, it was changed very early on and has been 16 for years. This is a very small and forgivable knitpick, just fyi.
The MDS focuses on the content of our daydreams, how intense the urge to continue daydreaming is, and how much it impairs our ability to function in our lives, and the benefits and costs of our daydreaming. I am not personally familiar with this scale, nor have I used it in my practice, but I've linked the research article in the description if you wanna learn more about it.
A good description, and here’s that link again for anyone who wants to read about the finer details of this scale.
When it comes to maladaptive daydreaming, it isn't just feeling out of body or environment. We can create very intense and detailed daydreams with plots, characters, and very lifelike issues and storylines. Some people will get the plots for their daydreams from their real lives, while others can create a utopian place unlike their current experience.
Yep, decent overview of content, though content doesn’t matter that much. Also, use of “we”. Is Katie Morton an MDer or was this a creative choice? I don’t know, just a passing thought.
We can find ourselves staying in these daydreams for various amounts of time. And some of my patients have reported staying in them for hours. And many of you have let me know that you struggle to get out of them at all, spending days in this other life that we've created.
Yep, good overview, but more importantly she’s listening to her patients and the feedback of MDers in her audience.
...there are many causes for this, and the first I wanna address is trauma triggers. If we've experienced a trauma in our life, things that remind us of that time or situation can pull us into a flashback, cause us to dissociate, or in many cases push us into our maladaptive daydreams.
When our brain and the rest of our nervous system feels overwhelmed and unable to deal with what's going on in the moment, it can pull us out of our current situation through dissociation. I always talk about that, like our brain pulling the ripcord. And it can also utilize maladaptive daydreaming. It's a way to cope or get through an overwhelming situation when we don't have other skills to help calm our nervous system down. So we just rely on what we know, and that can be daydreaming or dissociating. It's almost like this coping skill protects us from having to feel traumatized again and so it takes us away, you know, drops us into a much safer and happier place.
Trauma is always talked about first when people do overviews of MD. She’s not wrong but just to add more information; about a quarter of MDers report trauma, the other 75(ish)% don’t. It’s a significant number but trauma is not the only pathway to MD. Sometimes people walk away from these videos feeling like “well, I don’t have any trauma, maybe I don’t really have MD”. That’s not a comment on what Katie has presented, she does go into other things below, just adding on.
Another cause or trigger can be high levels of stress or anxiety. We can slowly feel ourselves become more and more overwhelmed until our brain pulls us out of our reality and into a new one, aka our maladaptive daydreams. In short, we can want to stay in these daydreams to feel better and safer, but it can get in the way of us functioning in our life.
Yep
[audience anecdotes]
...Which is why even the term maladaptive daydreaming is used. Maladaptive means it's not providing adequate or appropriate adjustment to the environment or situation. So the daydreaming is only holding off the bad things. It's not actually making anything better or helping us process any of the upset. It's really just a temporary check-out, which can be helpful sometimes, but if it's happening all the time or making it hard for us to focus at work, school, or with our friends and family, we should find other, better ways to cope.
Exactly.
Which moves us into how we can better cope so that we don't get sucked into our daydreams for hours, days, or even weeks. And first up is mindfulness. Now, I know that term is overused now and super annoying but in order for us to know when we even need to use other coping skills, we have to know when the daydreaming urges are happening. So often we aren't aware of what we were feeling or thinking until it's too late and we're already pulled into our daydream. And at that point it's more difficult or even impossible for us to pull ourselves out. Therefore, we have to start being more aware of what we're going through.
[continues explanation]
Perfection.
And so next is figuring out ways to calm our system down. This can take the form of a distraction technique like going for a walk or organizing a part of our home, coloring, watching a show, playing a video game, you name it. These calming things could also be more process-based, things like journaling or talking to your therapist or a friend about it, or even using an impulse log.
[Continues with calming things]
Good examples, MD researchers specifically recommend keeping a log.
We're also going to have to find some coping skills that we can use when we're starting to feel overwhelmed and wanting to go back into the daydream. Maybe we hold an ice cube in our hands, clap our hands, count the number of things in the room that are blue, brown, black… whatever works for you, do it.
Good stuff.
And it's okay for something not to work. We just have to try it to know and then move on to something else.
Important point to make, happy to see this.
Once we have a few things that work, write them down in your phone or on a post-it note so that you can see it and be reminded when you need it. We will also need to come up with some ways to pull ourselves out of the daydream. And I know this is gonna be harder and we may even wanna call upon helpful and supportive people in our lives to assist us.
Good advise.
We could, because it's our daydream, right, we could put a big door in our daydream and we can choose to go through it and pull ourselves out, or have people in the daydream that remind us of our real life and tell us to go back.
A good suggestion. Q, on the Parallel Lives Podcast (I can’t remember which episode off the top of my head), did something like this by turning to his characters and saying “ok, take 5 guys, we’ll pick it up at xtime”, and many people have found that to be a clever and helpful method.
Now, I know this is really, really hard… which rolls into my final tip, which is to work with a therapist to heal from the trauma or to learn how to better cope with the anxiety or stress we're feeling. Working to heal or process through the reason our maladaptive daydreaming exists in the first place will ensure that we don't need it anymore.
Absolutely seek professional support if you can.
... if we heal the issue we're struggling to cope with, the urge to use those unhelpful coping skills will go away altogether.
[outro]
I think this last point will frighten a lot of MDers. It’s probably the brevity of the video that didn’t allow her to really expand on this, and I certainly don’t want to put words into her mouth that she may not have intended. Don’t be afraid of losing your MD. “Curing” Maladaptive Daydreaming does not mean “I’ll never see my world again.” You’ll always have the capacity to daydream like this, you were born this way, but it *doesn’t* have to be maladaptive. Like overeating, you will never not eat, you will fix your relationship with food.
Good video overall, brief but accurate and includes the standard helpful advise.
40 notes
·
View notes
Note
Book recs on autism/add/CPTSD?
Aside from the books I recced here ages ago, which are mostly PTSD and dissociative disorder focused, nope. There’s one book in there on autism, but it’s specifically for partner workshopping, and that’s it.
Part of the reason I don’t have any book recs on C-PTSD is that there is not a ton of great books out there on C-PTSD, and this is partly because it’s not officially recognised in most of the world’s major diagnostic manuals. People can’t decide exactly what it is, or whether it’s a combination of comorbidities. They can’t decide if they want to call it C-PTSD or DES-NOS or something else. Not only that, but a serious push was made to include DES-NOS and DTD (C-PTSD related acronyms) in the latest revision of the DSM, and all were pushed back/rejected for just being insufficiently presented as conditions. Imho, I don’t think the DSM was wrong to reject what was put forward as the disorder.
I followed research around C-PTSD closely (because my symptoms match the description of it closely) around 1994 and in the decade afterwards. A lot of the time it was described as PTSD made additionally complicated by a dissociative disorder or alternatively, a personality disorder like Borderline or Bipolar Personality Disorder. It was used to distinguish from say, one-off rape-triggered PTSD, and PTSD that might be triggered by hundreds of rapes over a prolonged period since childhood (understanding that obviously, these would create different types of severity in the post-trauma spectrum, and require different treatments and expectations of recovery), and as with all disorders, a lot of people began self-diagnosing with C-PTSD who may have been dealing with comorbidities (PTSD + BPD as an example) that felt or looked similar.
Anyway, as a result, the literature on it outside of Herman’s work (which is in my stack of books) is like... mmmm. Hit and miss. It’s mostly articles.
Over time, with more research, it’s become less popular as a diagnostic disorder over time and not more popular, partly because a lot of the symptoms can be accounted for by pre-existing other conditions (ditto the treatments recommended). That isn’t to say it doesn’t exist, or that people can’t feel like that’s where they belong in terms of a label - I used the label myself for like 9 years before I decided against it - but the research around it shows more holes than anything solid, and there’s still a lot missing in the understanding of what is trying to be attained in the description of C-PTSD in the first place. It kind of had a golden age from like 1995-2005, dropped off the face of the planet, and then got picked up again during the renaissance of Tumblr (and social media) self-diagnosis and post-trauma social media vlogs etc.
The gold standard for C-PTSD discussion was still what was put forth by Judith Herman in Trauma and Recovery in 1992. There’s a reason even the Wiki article doesn’t step out much past that; there’s not that much good scientific work that’s been done in the field since that’s consistent or proves the existence of the disorder in the first place. :/ Traumatology science is complicated, but...things are not looking good for C-PTSD and it’s related acronyms DES-NOS (Disorders of Extreme Stress Not Otherwise Specified) and DTD (Developmental Trauma Disorder, for the childhood equivalent of C-PTSD) joining the DSM any time soon. So I kind of...dropped off with that research myself.
I have a lot of feelings about the C-PTSD diagnosis because I’ve had therapists diagnose me with it. But for the most part, it doesn’t change your treatment protocol anymore than if you had severe PTSD from prolonged trauma complicated with other mental and physiological disorders. As a result, I’m satisfied with the books on PTSD that I already have. I don’t set out to write characters with ‘C-PTSD’ - I write characters with PTSD complicated with other issues a lot of the time; if that reads as C-PTSD, that’s fine, but that’s actually just what PTSD complicated with other issues looks like as well.
I don’t have any book recs on ADHD or ADD, partly for selfish reasons - I don’t have it. I do have a lot of the symptoms, because there’s a lot of crossover between ADHD symptoms and severe PTSD symptoms and autism symptoms. (Fun fact, people with trauma who think they have ADHD or get diagnosed with ADHD first, often don’t realise that 70% of their symptoms can all be explained by PTSD. There are quite a few folks out there diagnosed with the latter, who might do better with treatment protocols for the former added in - many people don’t realise that mental illnesses trend in the mental health community. For like ten years it was bipolar and rapid cycling bipolar, for the last five years it’s been ADHD, some of those people have...you guessed it...PTSD, lol; when a disorder is trending, it gets diagnosed way more often whether the person has it or not - that’s why a differential diagnosis is so important).
I relate to almost every ADHD meme I see, because I have severe PTSD, lmao.
I’ve read a lot of articles on ADHD over the years because I have many friends who have it, but I don’t bookmark stuff like that so ¯\_(ツ)_/¯ I apologise! I mostly just pass them onto friends who have it and have appointed me their ‘research friend’ and that’s that.
And as for autism, I’ve never felt particularly compelled to read up on it, weirdly, outside of like the practical book that I’ve got in my collection (which I do, actually, recommend). Again, a lot of the symptoms between Asperger’s and severe PTSD actually are comorbid with each other, so again, a lot of the stuff covered in my PTSD research and therapy actually gave me adequate tools to deal with my autism.
But also just... most books on autism focus on boys with autism and focus on AMAB people and AMAB presentations and AMAB research and are less useful to me than like, articles and websites that specifically talk about AFAB autism presentation etc. The world of published autism books has a ways to go when it comes to not being like, sexist/misogynist in its presentation.
#asks and answers#inadvertent recs#judith herman's pretty baller honestly#but yeah you gotta be...careful with C-PTSD#it's considered super valid in social media circles#but like#diagnosticians and scientists are becoming more 'hmmmm' with it over time and not less#this might mean we actually get an even better acronym/disorder description#going into the future!#or it might just mean that we continue diagnosing PTSD across a spectrum#with potentially multiple comorbidities#as we've been doing for a long time now#that seems to be the preference at the moment#Anonymous
19 notes
·
View notes
Note
Ive seen a few blogs talking about Tony Stark with OCD and I was wondering what your thoughts on it were? I know it's not canon but would it be an okay headcanon?
Oh, goodness. This is a doozy.
First of all, I do want to give the obligatory "any headcanon is okay" when it comes to stuff like this, because some people do pick up comfort characters that aren't exactly like them and then use headcanons to push their characterization around until they become a more efficient catharsis vessel, and there's really nothing wrong with that in a space where characters are pushed around all the time anyway. Your headcanons are yours, and you interact with media how it best suits you. Just don't go talking like this is The Way The Character Absolutely Definitely Is, because not only is that misleading, but also it's kind of stepping on other people who need different headcanons for other reasons.
Now that that's out of the way.
You've come to the right place! I have actually been diagnosed with OCD and have been dealing with it now for a long, long while; funnily enough, the OCD is what led me to worry about the OCD, which is what led me to research the OCD in-depth for many, many years. Not to brag or anything. B) Like, literally not to brag, because it's a mental illness. Anyway, jokes aside.
I'm going to go by the DSM-5 and personal experience with the diagnostic process for now. I know some people have their gripes with the DSM, but it's what we're going with.
Before that, though, I do want to lay some things down here. Though it's not outlined by the DSM exactly, it's common among mental health professionals and people with OCD to categorize different symptoms based on causes of OCD. Because OCD is inherently ego-dystonic, your intrusive thoughts are going to attack whatever it is you care about most-- people with primarily contaminant symptoms might fear illness, people with primarily aggressive symptoms might fear hurting others, etc. There's no standard for what these categories are, really. Different places teach different things, and some people disregard them entirely. But it's good to know they're out there, some examples being contaminant and aggressive OCD as mentioned before, as well as pathologic doubt/completeness, religion, self-control, and superstition. There are more, less, or different categories depending on where you look, so we can just leave that there.
Now, onto the actual diagnostic criteria.
In order to be diagnosed with OCD, you need the presence of obsessions OR compulsions, OR both. So, you kind of don't need the whole set to have OCD, though it's argued that some people view "primarily obsessive" and "primarily compulsive" types of OCD as... plain old OCD. "Pure O OCD" especially has been criticized, as its based entirely on the concept of compulsions being in one's head as opposed to external, which then raises the question of whether or not we're defining mental illness by the sufferers or the observers. Regardless, this is what the current DSM says: obsessions, compulsions, or both.
They must be time-consuming (>1hr/day), cause clinically significant distress, or cause impairment in social, occupational, or other areas of functioning. So, could you be considered OCD if you're perfectly functional to the outside world but dysfunctional psychologically? Yes! Could you be considered OCD if you're mostly okay with the compulsions (often seen in people who believe their compulsions are rational responses to rational fears), but you can't function in day-to-day life? Yes! OCD is defined by how it affects you, and there are so, so many ways that it can do that.
The symptoms of OCD can't be caused by physiological effects of substance abuse or other medical conditions.
The disturbance cannot be better explained by the symptoms of another disorder (i.e. if excessive worries are better explained by an anxiety disorder, you're more likely to be diagnosed with something along the lines of GAD; if your difficulty discarding possessions is more in line with a hoarding disorders, you're more likely to be diagnosed with a hoarding disorder). One thing I would like to mention here is that this is often where the DSM breaks down when it comes to practice rather than theory. I'd like to specifically outline the example under this segment of the DSM that refers to "guilty ruminations, as in major depressive disorder". By these guidelines, would you be able to have both MDD and OCD if your OCD has mostly intrusive symptoms?
Well, yes, actually. There's a lot of discourse surrounding it, but here's the thing. Diagnosis is something meant to put you into a category so you can either seek treatment or get accommodations. For mental illnesses, physical illnesses... anything. This is it. I myself have both MDD and OCD, and part of why this is, is because there's an overlap between symptoms... but that's all it is. An overlap, borderlining comorbidity. And there are plenty of people who have similar diagnoses.
You'll see why I'm bringing this up in a second.
Let's go back to the diagnostic criteria and take it one-by-one.
Obsessions are defined by (1) and (2):
Recurrent and persistent thoughts, urges, or images that are experienced, at some time during the disturbance, as intrusive and unwanted, and that in most individuals cause marked anxiety or distress.
The individual attempts to ignore or suppress such thoughts, urges, or images, or to neutralize hem with some other thought or action (i.e., by performing a compulsion).
Does Tony experience obsessions? Well, he very well could.
There used to be a criterion in the now-outdated DSM-IV that outlined obsessions could NOT be "simply excessive worries about real-life problems." But in the DSM-5, this was dropped. So, an obsession, by current standards, most certainly can be defined as an excessive worry about real-life problems.
Whether or not Tony's worry is excessive is debatable. We're all aware of Clint's sentiment in New Avengers that basically boils the team's state of being down to "we're extraordinary people, so we have extraordinary problems." Tony's worries are extraordinary, but... are they excessive?
I could go either way on this argument. Due to Tony's massive influence and his feelings of responsibility, we can all see why these worries might be considered realistic and average. But it's those feelings of responsibility that would make a better argument for "excessiveness"; he has taken the stance quite a few times that he's been "the only one who could see what needed to be done", or something akin to that, at least. It's not just that he has serious problems and he's concerned about serious solutions. It's that he feels such a sense of responsibility and guilt that every single problem on the planet happens to be a problem he's obligated to consider by his own standards, and if he doesn't consider those problems, he's an awful garbage man. Again, by his own standards.
One could also easily argue that he could fall prey to both aggressive-type obsessions and pathologic doubt-type obsessions, given that he's terrified of hurting people or causing harm unknowingly and that he's never 100% sure of himself, always "almost certain", and often looking to others (like Happy in Civil War, for example) to vent and try to half-validate himself as someone who really is doing the right thing.
These very obviously cause him distress, and one could argue that his Atlas-like anxiety with regards to keeping the world afloat is a huge factor in his mental cycle of thinking he's not doing enough, which means he's not enough, which means he deserves to die, which means he actually should die if he's not doing anything right, which means he has to try really, really hard to do things right, but he'll never do everything he needs to do, so he's not doing enough, so he's not enough, so he deserves to die.
And the alcoholism could easily come into play here, being a default coping mechanism for almost anything he'd encountered, obsessive or otherwise.
Now for compulsions.
Compulsions are defined by (1) and (2):
Repetitive behaviors (e.g., hand washing, ordering, checking) or mental acts (e.g., praying, counting, repeating words silently) that the individual feels driven to perform in response to an obsession or according to rules that must be applied rigidly.
The behaviors or mental acts are aimed at preventing or reducing anxiety or distress, or preventing some dreaded event or situation; however, these behaviors or mental acts are not connected in a realistic way with what they are designed to neutralize or prevent, or are clearly excessive.
So, we're going back to the obsessions outlined earlier. One thing I neglected to mention there was what he's referred to as one of his biggest fears, and I neglected to mention it because of how it ties into potential compulsions.
He's mentioned that someone "taking over his brain" is possibly the worst thing that could happen to him, given that he is a man with incredible influence and incredible intelligence and if his mind falls into the wrong hands, it could have (and has had) disastrous consequences. We see a lot of Tony trying to protect his mind as a result, always having backups, always having alternatives, always having contingency plans. This could also be considered a response to an obsession with regards to “mental contamination”, which makes sense.
It's similar with the responsibility-induced anxiety; he made how many AIs, now? He quite literally can't let himself die. He needs to be up, awake, present, alive. He needs to continue doing The Right Thing. We see the same sorts of behaviors even when he's alive and kicking-- he's often in his lab into the late hours of the night. He canonically works multiple jobs at his company. He runs around holding babies around the world, for God's sake. He believes everything deserves to be cared for, loved, and he believes he has to be the one to love it, and so he does, taking up so much of his time and so much of his energy every single day in a desperate attempt to make sure he's done all he can.
This is a man whose every day life could be considered scheduled compulsions if you really wanted it to be, one after the other, in a never-ending cycle of behaviors that he canonically won't ever be satisfied with.
Tony certainly could have obsessions. He certainly could have compulsions. He certainly could have OCD.
It's worth it to mention that self-blame, even for the smallest little details, is extremely common in people with OCD, and... That's also a very Tony thing, isn't it?
All that to say...
Do I think he does?
Well, not... really. I mean, I don't very, very strongly believe that he doesn't. And a lot of neurodivergent people have created incredibly thorough explanations as to why a character not intended to be one way might still be that way-- not even as a headcanon, but quite literally, they just are that way. This is especially common among characters coded (intentionally or otherwise) to have things like autism and ADHD. Whether or not a character "has" something is difficult to decipher, but if you can outline all the symptoms and you can't come up with any other explanation for them, then, well... You've got a neurodivergent character on your hands.
But that's the thing. You certainly can explain Tony's feelings and decisions with a diagnosis of MDD and alcohol abuse. You can. Plenty of people don't really want to, especially with some more toxic beliefs in the mental health community that regard less stigmatized illnesses as somehow also less severe or less validating, and regards MDD as "just depression" in a way that more stigmatized illnesses aren't.
I don't feel terribly represented in Tony as someone with OCD-- I feel represented with almost every aspect of his struggles with mental health, but I rarely ever read through comics going, "there! There's my OCD thing!" Which isn't to say that it's never happened on a subconscious level, because... I mean, illness bleeds into every aspect of you. It's terribly difficult to find where one part of you ends and the other begins when there's so much overlap. But personally, Tony having OCD isn’t something that I really consider when I read or write (which is part of why I like having Ty Stone around so much-- I can pin a bunch of shit on him that I think Tony doesn’t have, and then I get to write everything I want while still keeping things true to the way I see them).
There are other sufferers of OCD who must certainly relate to Tony, and probably exclusively go "There's my OCD thing!" while reading his comics. I can see why.
So, again.
Do I think he has OCD? Eh. Not really my thing. But I think canon does what canon does, mental illnesses have plenty of overlap, and he meets the criteria enough that if you were to say he had both MDD and OCD, I wouldn't feel any reason to argue, especially if you’re saying it to better relate to him.
#cassks#suicide tw#sort of#ocd#is there a tag that means 'this talks about ocd but in a way that might trigger ocd'#because if there is. please tell me#i have thought many times that it would be cool to have a tag like this at some point#i'm very tired if there are any tags you want here just let me know
9 notes
·
View notes
Text
I canceled the appointment I had for August to see a psychologist that specializes in Autism Spectrum diagnoses for adults. It was going to cost more than $1,000. I guess at the time when I made the appointment, I thought we'd have that money. We just don't. It really sucks. It feels like there were possibly answers or progress within reach. But not anymore. I spoke with a few people who are on the spectrum or who have family that are diagnosed autistic. Everyone kind of concurred that unless it was for specific work accommodations, it might not actually be "worth it" to seek any diagnosis. At first I thought I didn't need any work accommodations. But the more I think about it, the more I realize just how desperately I do need small chunks of time of just silence and not interacting with people. Like, maybe just 15 minutes of quiet. Those are my best recharges during a work day, when I can find a quiet room to sit in for ten minutes and no one interrupts. It's almost impossible to ask of a NYC public school - a quiet place for people to go and recharge. But that is really what we need, students and adults alike.
I think I probably have a sensory processing disorder that leads to a whole host of other problems that look like other things - for example, the other night when I was cooking and I started to get too hot, and then hair was sticking to my neck, and crumbs were stuck to the bottom of my feet, and then construction was happening outside - I am not happy to admit this, but I quite literally threw a tantrum in the middle of my kitchen - clenching my fists as tightly as I could, gritting my teeth, trying not to physically react. I wanted to explode out of my skin. I wanted to punch a hole through a wall. I wanted to scream and cry. I screamed into a pillow. I didn't feel better until I showered and my skin didn't feel sticky. I think so many of these sensory issues lead to other problems - anxiety, perhaps at anticipating or enduring uncomfortable sensory experiences. Depression, realizing this is not the normal experience for everyone and it is very uncomfortable and practically invisible. Social anxiety, as I can't listen to what you're saying very well if there is music playing in the background, and I have to ask people far too often, "what was that?" A complete lack of executive functioning skills as I become distracted by every sound and smell and touch.
Maybe it isn't autism. Maybe it's crippling sensory overload.
Either way, I will just keep guessing and keep self-treating as well as I can. I'm lucky to have access to what I do - the Calm meditation app has meant the world to me this last year. It's $65/year. Not everyone can afford that. Stuff like that should be free. We lie and tell people the resources are out there and then they try to find them and they are not, they are not free and they are not easily accessible, and you better believe you're going to fill out a shitload of paperwork and jump through a thousand hoops before you can get even hope to get help. And I guess it stands true. What am I looking for in any sort of official diagnosis? Is it validation? Is there something so wrong with wanting to feel validated? To know that there is an explanation for why I have always struggled.
My psychiatrist, who is treating me for anxiety and depression since 2019, checks in with me about once a month before refilling my medications. I asked her about misophonia (literally - hatred of sound) - a condition that is also not often officially diagnosed. I was pretty surprised when she said she had never even heard the term. Misophonia is a strong reaction to specific sounds, such as pencil tapping or gum chewing. People with misophonia can become irritated, enraged or even panicked when they hear their trigger sounds. Hell if that doesn't sound like me.
I'm not entirely sure where to go from here. I'm finding a lot of success in just giving myself permission to avoid situations that I know are going to stress me out. If I am getting uncomfortable somewhere, I don't worry if people are going to be offended if I leave. I just leave. Obviously that's not going to fly at work. It's going to be an adjustment after working from home all last year. But I keep telling myself I have made it this far. I will figure out what works.
#mental health#sensory processing disorder#sensory overload#neurodiversity#neurodivergent#mental health awareness#misophonia
1 note
·
View note
Text
Common Sense Meets the Autism Spectrum:
| a Parental Aide for ALL |
Last month was Autism Awareness Month, and in honor of that I've whipped up a little Parental Aide to help all grown-ups understand neuro-divergence a tiny bit better. I meant to post it here during the last week of April, but I forgot because of the craziness with Finals... But since Autism and neurodivergence doesn’t just magically go away at the end of April, here’s a little skim of it now:
I've recently been chatting with a new consultation client / parent whose child has been recently diagnosed with Autism, and it got me thinking about the unfortunate nonsense surrounding the entire societal black hole of neuro-atypical / neuro-divergent presentations, especially in 'unusual' cases.
The first thing that needs to be said is IT'S A SPECTRUM, and it's honestly a comprehensive population spectrum, which means that EVERYONE IS ON IT.
Yes, say it with me: Everyone is on the Autism Spectrum.
From being perfectly, generically neuro-typical humans to rage-murder psychopaths to non-verbal, high-physical autistic kids to sociopathic con-artists. It's a SPECTRUM.
Accepting that is the first part of understanding it. And it's sometimes helpful to know in order for parents still in diagnosis shock to have something that reconnects them to their child. If you've recently received a diagnosis and you've dissociated at all, or know someone who is in that situation, knowing that the parents and the child involved are both still on the same spectrum, can help.
(It's a sense of cohesion and sameness that parents dream up for offspring, and can be problematic if over-done, which is why parents sometimes force their hobbies / goals onto children or react poorly to LGBTQ+ explorations / self-discoveries, both of which are fodder for plenty of other posts).
Once the spectrum is accepted, we can move on to understanding it better, and to diagnosing attributes of it that are affecting our lives. Knowing these attributes can help us navigate them, even in a capacity where the effect of them is not so severe that we call it a neurodivergence.
There's a stigma with mental illness, and autism is a trigger word regarding that, but it shouldn't be. We don't (as much, any more, at least) shame people who don't have clinical anxiety, but still exhibit crowd skittishness or phone distress or choice paralysis. And, honestly, mild autism frequently presents as anxiety, in our current popular understanding, as it's often limited to one or two aspects of life that provoke dramatic aversion responses where as actual, general anxiety is usually a more evenly distributed with lower-key hesitance / avoidance. Mild autism also presents as ADD / ADHD (and in my opinion the ADD / ADHD diagnosis tools are essentially boiling things down to 'not a psychopath but probably autistic, but not like the autism in in the popular imagination').
We accommodate the small symptoms of both autism and anxiety, adjust what we can and power through what we can't.
That adjustment is a lot easier when we know the triggers for the distress.
Now, the scaling systems I'm about to share are not professional, not part of the DSM, and not a tool of formal diagnosis. Consult a licensed professional before taking any big steps, but take a look at these scaling systems to help start a conversation (even if it's only with yourself). I might have another post on adjustment strategies, because these don't really address the links between presents-as-anxiety and autism, but for now, we're just gonna look at how to start asking questions and how to wrap your brain around the biggest bit of the autism concept.
Again, none of this is a diagnosis or a practical guide on how to cope, but it is helpful to be generally informed enough to start recognizing issues / asking questions about what else might be affected by a given place on a scale.
So, Autism is a spectrum, right?
Well, technically, it's multiple spectrums.
There are several sub-spectrums that layer over each other.
The crux of it, the most basic version specific to autism, is this:
Understands Emotion -- vs -- Does NOT Understand Emotion.
Now there are varied layers of that, such as 'displayed' emotion (like in facial expressions), or 'tonal' emotion (like voice tones), or even 'conceptual' emotion (as in the basic cause / nature of emotionality).
Plenty of kids understand Tonal Emotion (hearing and recognizing the difference between Mum is angry and Mum is happy), but not Conceptual (this is called being young, and usually gets grown out of as kids actually experience {and label} more emotions, the process starts at age 3 or 4, but honestly continues for most of life). Or kids may be able to hear tonal changes and interpret them accurately, but they don't read faces well (this is either a significant indicator of some sort of disconnect or, can indicate that the facial expressions they have seen shift do not shift in a way that is consistent with tonal changes {like if a parent is angry and tries to hide it with a smile}.). Some kids can track the changes in tone and expression but can connect them to a concept (such as 'fear' which doesn't develop as a concept to children until about age 5~7, even in horror-story situations, like children in warzones, only get a really nuanced concept fear a year or two earlier).
The second BIG scale to assess things on is intro- or outro-spective, and it's a 2-for1:
- misunderstand -- VS -- understands OWN emotions
-- vs --
- misunderstand -- VS -- understands OTHERS' emotions
AND misunderstands or understands the CAUSES of emotions in self / others, and why those causes and interpretations may be different for various individuals (which requires understanding the concept of there even being varied individuals, a process that ).
This is the line between "I like it, so others DO" vs "I like it, so others MIGHT", that is difficult for young children. Having a distinct sense of a separate self is actually a complicated psychology process, and it takes over a year for most infants to even recognize that they have a reflection. If understanding the self/others division stays extremely difficult passed age 7-ish, we maybe should look more closely. But at the same time, it's rarely before that 5~7 range when kids begin to understand that shopping for a birthday present for a friend involves thinking about what the friend would like, and not what the kid themselves like.
And there's still gonna be moments of grown-up fan-rage at why don't people ship my ship?, but all we might wanna do is limit time on Reddit or Tumblr when in anxiety mode.
The final BIG spectrum used in understanding these autism specific neuro-disconnects is one that revolves around concern for the disconnect:
Does not fully understand all aspects of Emotion and CARES that they don't.
-- vs --
Does not understand and does NOT CARE.
This disconnect leads to Performative Emotion, which means acting the part of emotional responses without a full understanding of all aspects of them. Sometimes this is good, as in exhibiting quiet displeasure even though I think this warrants screaming because, I don't wholly understand what I or others feel, but I do understand the appropriate / expected response. It can also be very bad, as in someone who understands the emotional response to pretend to have when a pet dies and is aware that doing so can cover that the pet was killed intentionally by said someone.
The last relevant spectrum isn't one that most people find critical, but I think it's important to delineate this one from the caring aspect. The previous note is specifically about caring in regards to the subjects understanding of emotion--and exclusively their understanding of emotion.
It is not a measure of concern for other respects of life, that spectrum is:
Sympathy -- vs -- Empathy
Now, defining terms is important here.
- Sympathy = care for how others feel
- Empathy = understanding / comprehension of how others feel
Someone who self-refers as an 'Empath' is actually expressing a high sympathy response, as in, I understand your pain so well, I feel it myself. What they mean to say, is that they understand the feeling and its causes well, and they care so much that they cause themselves to experience it.
This is also the line between Sociopaths and Psychopaths, as most people know it. The truth is a lot more nuanced, but basically, a Sociopath often lacks Sympathy, but has Empathy, where a Psychopath most often lacks both.
A Sociopath understands that they have a disconnect, cares that they do, and hides it by performing the emotive responses they are aware are appropriate (for the most part, occasionally making some exceptions due to exhaustion with the performance, or a lack of genuine care allowing for selective exploitation--making them great sales people / CEO's / business people / lawyers / writers / con-artists / Sherlockian private detectives etc).
A Psychopath either doesn't understand they have a disconnect, doesn't care that they do, or both. They rarely perform emotions and therefore often draw people in who feel trapped and in need of counter culture. They make great cult leaders, but not much else (occasionally business people, but some of them are cult leaders by a pseudonym). They truly CANNOT conform, and that can be seductive / freeing to others, but they also cannot conceive of anyone who decides to follow them ever changing their mind or not experiencing exactly the same emotions / emotive responses to stimuli as they do.
BOTH are considered extreme presentations of their respective trait.
People with both very high and very low sympathy get exhausted around others.
Because experience other's emotions or pretending to care about others' emotions is HARD. It's work and it's exhausting on both ends.
People with both very high and very low empathy get anxious in not being around others for prolonged periods.
High-Em usually worries over current states (ie, what if something happened to them or what if they hate me now), whereas Low-Em usually worries over reunions (did I forget something someone else would've remembered, birthday, holiday, or that I was gonna bring you something we discussed).
And, as always, Presentations vary. HUGELY.
But sometimes, being told you're looking at an abstract a picture of a dog, helps you spot the dog in the ink squiggles.
'Normal' isn't a fixed point, it's a range within every single subject presenting mild deviations that come together to form an average in a single person, and are then averaged again across populations.
Such data can always be understood better. And better understandings allow better accommodations to be made.
Therefore, a given person's place on any part of any one of these spectrums needs to be assessed and reassessed constantly.
Also, if you're interested in learning more / supporting Autism Advocacy, check out a few more resources, but for the love of god DO NOT give money to Autism Speaks. Take a looks at THIS and do some research of your own! ^_^
Again, this is just a vague baseline, and it doesn't address symptoms like Face Blindness (in ability to recognize people by faces) or stimming (self-stimulation or emotive overwhelm release) or even environmental sensitivity (extreme dislike / like of certain noises, colors, light levels / sources, tactile sensations). Even so, it might be informative enough to start getting a conversation started and it'll be helpful for me to refer back to this one while making other Spectrum related posts.
^_~
For more on what I’m getting up to (and for more timely updates), check me out on Patreon!
2 notes
·
View notes
Last Seen Blogs

botanicalcuties
I just want to be loved

duartegazzola
DuarteGazzola Corner

rockalily-blog
Rockalily

jessicasellsthings
Jessica Sells Things

drucifer666
more noise please...