#Psychodynamic Theory
Text
"Everybody acts out a myth, but very few people know what their myth is."

Carl Gustav Jung was a Swiss psychiatrist and psychoanalyst who founded analytical psychology.
Born: 26 July 1875, Kesswil, Switzerland
Died: 6 June 1961, Küsnacht, Switzerland
#Carl Jung#Analytical Psychology#Archetypes#Collective Unconscious#Individuation#Persona#Shadow Self#Dream Analysis#Self-discovery#Psychodynamic Theory#Psychological Types#Introversion and Extraversion#Anima and Animus#Synchronicity#Depth Psychology#Symbolism#Mythology#Alchemy#Psyche#Psychological Development#Self-realization#Inner World#Dream Symbols#Jungian Therapy#Inner Self#Ego#Transcendence#Unconscious Mind#Spiritual Growth#Symbolic Imagery
17 notes
·
View notes
Text
I just had the horrible thought that I need to fall in love because having devastating crushes on beautiful, competent, authoritative women that I desperately want to please is exhausting and I need it to stop
#this one is straight so there's no room for delusion which is good#but my burning need to be her most favorite is eating me from the inside#it IS making me better at my job though#.......i mean i think so but what the fuck do i know#on friday night amongst the grueling psychosexual chaos that ensued a very smart guy that I LOVE said to me#i have no doubts you're gonna be a great psychiatrist actually#i traded a month with him to have another month with her#he's a phenomenologist she's a psychodynamic....ist? rival theories#I don't like most of psychodynamic theory.......so far#but i love the way she works and i can see how well it fits with her manymanyMANY patients and goddamnit i love personality dosorders#so i made the choice to go with her yes and im very torn casue i LOVE that guy and i wish i could become his friend like my bff from my year#also.......kind of dumb of me since I'd only soend two days a week woth her and the other three with very scary ladies#but I've been in scarier situation i can manage#and god when she praises me (silently obv she's only been forward about my merit ONCE and i almost pissed myself like an overexcited dog)#the endorphin rush is........man#but yes i need to work on this.......idk how to define it. closest i can get to explaining it is professional sub space#with strong aspects of praise kink#pathetic is what it is really#but hey if it makes me study harder who fucking cares right#I'm gonna be the smartest most intuitive fucking bitch amongst my peers so if I can't have her (them) carnally then goddamnit#I'LL HAVE THEIR PRAISE AND RESPECT AND ADMIRATION AT LEAST#........I'll be normal again in a week or two i just need to get over these next couple of days of....idk. inflammation i guess#yeah it's just like an infected wound right now#angry red throbbing hot pain#i know the drill it'll be better in a couple of days you just need to not freak out and let it do its thing#it's nice to be mature-r about emotional impulsivity and the shame that comes after an episode of deregulation#it really doesn't have to be a big deal even while it still feels like it#it still hurts but it's like......hour three of a tattoo. it's a bitch but you know it's gonna be over eventually and wriggling won't work#the only thing left to do is enjoying it all while it's happening or trying to#I don't think I'm doing a great job but what're you gonna do right
2 notes
·
View notes
Text
a ver si no termino autodiagnosticandome con la personalidad als ob

#procrastination comics#karaii art#thus far my psychiatry residency has had 0 focus on psychology so i've been studying a little on my own time#somehow i ended up reading psychodynamic stuff#i avoided that like the plague when i was doing my psych undergrad but i figure i should at least give it a bit of a read#lest i sin in throwing out the baby with the bathwater etc etc#thus far the only thing that's really caught my interest is attachment theory and a bit of the concepts behind personality organization
11 notes
·
View notes
Text

Rules to Mind Reading! (Personality theory)
Keep in mind that these may go under amendments as this is a new theory.
Basic Dichotomies:
I(N)tuition: Broadening and Breaking Down sensations for new perception. Highly suppresses pure sensation.
(S)ensation: 5 senses. Highly suppresses intuition.
(T)hinking: Logic. Highly suppresses sentiments.
(F)eeling: Sentiments. Highly suppresses logic.
Attitudes
Introverted: Psyche-Based
E.g Ti, Fi, Ni, Si
Extroverted: Tangible-Based
E. g Te, Fe, Ne, Se
Information Elements
Ti - Philosophy and Theories, Relativity, ‘Unbiased’ Systematization, Fairness, Impersonality, Understanding of world
Fe - Connotation, Intonation, Emotional atmospheres, Expression, Sentiments, Selflessness, Colloquialisms, Census bias
Te - Efficiency, Relativity, Fairness, Objectivity, Practicality, Logical Adaptability, Tactics, Utilitarianism, Abiotic Environment and People, ‘Unbiased’ Systematization
Fi - Own emotional relationships to things/people/and concepts, Values, Morals, Absolutes, Personal Bias, Preferences, Obsessions, Individuality
Ni - Inner World, Thematic Imagination, Prediction, Guessing, Whole Picture, Mental Rotation, “3D Software installed”, Memory Icons
Se - Kinetics, Motion, Symmetry or lack there of, Environmental Awareness, Harmonization and Disruption, Grounded thinking, Realism, Memory Icons, Echoic memory,
Ne - Potential, Open-mindedness, Multiple Angles, Diversity, Lack of and presence of Congruence
Si - High Resolution Inner World, Internalization of Pleasant and Unpleasant Sensations, Remote memory
*REMEMBER* : IMs can interact and all information is used!
Valuation
Valued: Fixated and mostly focused on.
Unvalued: Distributed else where to the opposite attitude.
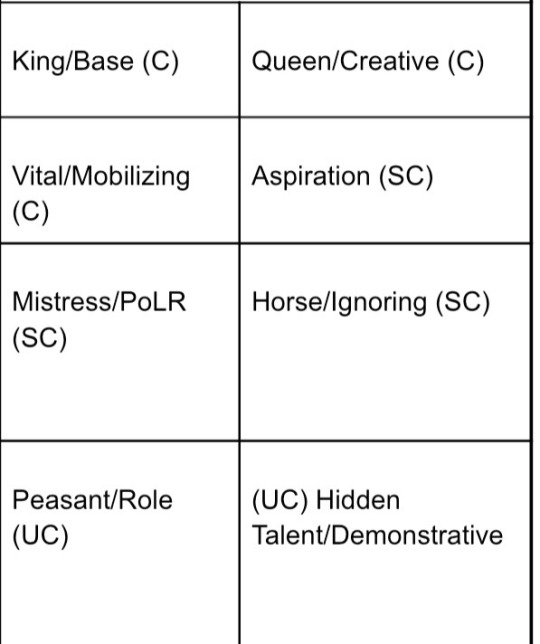
Functions
King: Main Fixation. Conscious.
Queen: Main Conscious supporter of King.
Vital: Secondary conscious supporter of King.
Aspiration: Highly neglected. Subconscious.
Mistress: Alternative subconscious supporter of King.
Horse: Withdrawn from and only makes contact with, subconscious.
Peasant: Highly suppressed by King. Unconscious.
Hidden Talent (or H.T.): Head of Unconscious.
The "Main":
Your main Sociotype and generalization of personality.
The "Grip"
When you weigh too heavily on your aspiration and your type takes on the aspiration as the King, and the rest of the functions follows. A typically incompetent state.
The "Instinct"
The unconscious and functions' influence on you. Can change depending on what state you are in.
E. G. LIIs in the ESE Grip have an SEE instinct instead of the usual ILI one.
**4B Hidden Talent is influential practically all the time unless Instinctual Mistress is on, which would happen when Vital or Mistress is used.
3B Instinctual Horse is highly influential sometimes, when the King is out of the psyche.
3B Peasant is highly influential unless King or Horse is influential. Suppressed functions have a lot more influence than realized, has the most influence when Aspiration is used.
1B Instinctual Mistress is rarely all that influential unless Vital and Mistress are used.
2B Instinctual Aspiration has mid-influence unless Horse is on.
2B Instinctual Queen has mid-influence unless Mistress is on,
1B Instinctual Vital has low influence on the background instinct and strictly manifests consciously.
4B Instinctual King, both consciously works and influences all the time.
The "Shadow"
The circumstance where you embrace the opposite attitude. Also typically incompetent.
7 notes
·
View notes
Text
i just read such a stupid post about jedi adoption and attachment styles i need to go look at my masters thesis to calm down
#🤡🤡🤡 <- me and the psychodynamics gang showing up at star war to psychoanalyze the communally childrearing alien psychics#'anyone who knows anything about attachment theory–' name three findings on attachment styles in non-western contexts. quickly
5 notes
·
View notes
Text
psych major to make more money? no. psych major so i can use it for my stories ♡
1 note
·
View note
Text
What is Psychodynamic Therapy?

Psychodynamic therapy is founded on the principles of psychodynamic theories, which express the belief that we are driven by internal psychic energy and strongly influenced by our early childhood experiences. Experiences in our past have lasting effects on the conscious and unconscious parts of our minds. Psychodynamic therapy seeks to understand thought and behavioral patterns. This approach does not focus on problem behaviors, but instead explores the client in a more holistic way. The goal is for the client to gain a deeper insight about themselves as well as form a more positive sense of self.
The psychodynamic school of thought has several foundational theories and uses various techniques. Sigmund Freud is often considered the founding father of psychotherapy. Freud used free association, which is a technique where the client talks about whatever comes to mind in order to bring the unconscious forward. Another technique utilized in this therapy is dream analysis where the client is able to discuss their dreams to bring unconscious motives forward. Another important pilar to psychodynamic therapy is Alferd Adler. He focused on social interest and the roles of familial relationships. He used techniques like early recollections, the clients’ earliest memories. These first memories can offer insight on how the client feels about themselves and the world around them. The client can then work on creating more helpful and productive meanings of their early recollections.
In modern psychodynamic therapy, you can expect the therapist to encourage the client to talk freely about what is going on in their lives, and work towards the client recognizing and interpreting patterns. Psychodynamic therapists use various techniques to access patterns and deep underlying motives. The clinician and client have a trusting relationship that is encouraging and comforting. This process is collaborative and works on discussing thoughts, emotions, and behavioral patterns, in order to promote healthier thinking.
Several clinicians at LIFT, including Mary Dobson, utilize a psychodynamic approach in their work with clients. Psychodynamic is generally not short-term, solution focused work. Rather, it requires a commitment to an ongoing relationship of self inquiry between therapist and client. If you are interested in learning if you are a good candidate for psychodynamic therapy, you may contact us.
Contributed by Stasia Timan, Clinical Intern and Play Therapist, LIFT.
0 notes
Text
the way filatova/gulenko's socionics theories have phrenology in them to identify people's cognitive types + range of abilities and 'talents'. pseudoscience is so ass
#all fun and games until people try to make a scientific model out of cognitive functions like chill its not that deep#iceberg model and all havent u guys learned enough from freud's dumbfuck psychodynamic theory and linking it to evolution. who gaf abt eros#and thanatos this is so embarrassing#log21
0 notes
Text
Clinical Formulations of Narcissistic PD
Clinical formulations and case conceptualisations are introduced in this post.
These are all generalisations and theories of how NPD develops, not something that is supposed to be true for everyone with NPD.
Psychodynamic model
Freud suggests parents either overvaluing or neglecting (or both) a child can lead to NPD & especially inability to form healthy, lasting relationships and regulate self-esteem
"In other words, [NPD] is the outcome of insufficient gratification of the normal narcissistic needs of infancy and childhood."
Kohut theorises that narcissists' ability to form a cohesive sense of self and others was developmentally arrested in childhood, resulting in grandiosity & idealising others
"Narcissistic injury" = fragmentation of the self
Kernberg suggests grandiosity & exploitation result from maternal emotional abuse
Grandiosity is an "emotional escape valve"
Grandiosity & entitlement mask the "real self" that is "split off"
The real self unconsciously holds rage, fear, envy, deprivation
Defensive structure is same as BPD but difference is grandiosity
Biosocial model
NPD is primarily the result of environment, especially "parental indulgence and overvaluation, learned exploitive behavior, and only-child status"
Special treatment from caregivers leads children to believe that the "world revolves around them", and therefore they expect the same outside the home
When special treatment outside the home doesn't happen, they "experiment with demanding and exploitive tactics and subsequently develop considerable skill in manipulating others"
"At the same time they come to believe that most others are inferior, weak, and exploitable."
NPD is self-perpetuating through sense of superiority, lack of self control, sense of entitlement, and dismissing of those who reject their world / self-view
Cognitive-Behavioural model
Key feature of NPD is self-aggrandisement
Core beliefs:
> Deserving of special treatment
> Not bound by social norms and rules
Conditional beliefs:
> Others should be punished for not recognising their specialness
> To maintain that special status others should be subservient to them
Instrumental belief:
> Always strive to demonstrate their superiority
> See themselves as special, superior, entitled to special favors and treatment, and vulnerable to loss of status
> View others as inferior but potential admirers
Main pattern of behaviour is "seeking prestige, power, position, and wealth as a way of reinforcing their image of superiority", using "manipulation and guile" if necessary
The primary schema is superior & special (/ entitlement & grandiosity)
> Superior schema "shaped by flattery, indulgence, and favoritism"
> Special schema shaped by "rejection, limitations, exclusion, or deficits"
> Common denominator is the belief that the individual is different in some way
Three subtypes:
> Self-centered impulsive type
> Ruthless impression-management type
> Acceptance-oriented impression-management type
> Each type is centred around an impulse control deficit developed in childhood
> "Specifically, these individuals learned to seek reinforcers without having to work for them. This resulted in their development as self-indulgent, egocentric, and impulsive individuals."
> Ruthless & Acceptance-oriented types focus on creating favourable impressions with others, but struggle with long-lasting healthy relationships because of their empathy deficits
Interpersonal model
People with NPD were raised in an environment of "selfless not contingent" love, leading to insensitivity to others' needs
The caregiver was over-adoring, but there was also a constant threat of a "fall from grace", with pressure to be the perfect child
The constant overbearing love means that any criticism or disappointment hits very hard
"In short, there is extreme vulnerability to criticism or being ignored, together with a strong wish for love, support, and admiration from others. Noncontingent love and presumptive control of others is expected and even demanded. If support is withdrawn, or lack of perfection is evident, the self-concept degrades into severe self-criticism."
Integrative model
People with NPD are hypersensitive
Seen as exceptional children, leading to pressure to perform
As children likely had highly developed speech and interpersonal skills
Life purpose: "I’m special and unique, and I am entitled to extraordinary rights and privileges whether I have earned them or not."
World-view: "Life is a banquet table to be sampled at will. People owe me admiration and privilege."
Goal: "Therefore, I’ll expect and demand this specialness."
Defense mechanisms: rationalisation and projective identification
Parental injunction: "Grow up and be wonderful—for me."
"The illusion of specialness, disdain for others’ views, and a sense of entitlement lead to an underdeveloped sense of social interest and responsibility. This, in turn, leads to increased self-absorption and confirmation of narcissistic beliefs."
- From Sperry, Handbook of Diagnosis and Treatment of DSM-5 Personality Disorders (2016)
#len sperry#handbook of diagnosis and treatment of dsm 5 personality disorders#personality disorder concepts#case conceptualisations#clinical formulations#pd info#npd#npd info#dogpost
161 notes
·
View notes
Text
TREATMENT BOOKS (a few suggestions, listed alphabetically)
Rebuilding Shattered Lives, Treating Complex PTSD and Dissociative Disorders, 2nd ed, (2011), by James Chu.
A valuable book for beginners and experienced clinicians, this text offers practical advice on therapeutic techniques and treatment, with information about early attachments and their effects, neurobiology, crisis management and psychopharmacology
Shelter from the Storm: Processing the Traumatic Memories of DID/DDNOS Patients with the Fractionated Abreaction Technique, (2013) by Richard Kluft. Integrates elements from psychoanalysis, psychodynamic psychotherapy, hypnosis, behavioral therapy, cognitive therapy, and EMDR to support a practical, empathic, and compassionate approach to treatment, taking care to avoid retraumatisation
The Haunted Self – Structural Dissociation and the Treatment of Chronic Traumatisation, (2006), by Onno van der Hart, Ellert Nijenhuis & Kathy Steele. This key text draws attention to the substantial problems suffered by chronically traumatised individuals. It presents the theory of structural dissociation of the personality, a phase-oriented approach to treatment, and hope that recovery is achievable
Trauma Model Therapy: A Treatment Approach for Trauma Dissociation and Complex Comorbidity, (2009) by Colin Ross. A practical, well-structured manual, presenting theory, assessment and treatment strategies, techniques and interventions for severe dissociative disorders
Treating Complex Trauma and Dissociation – a practical guide to navigating therapeutic challenges, (2017) by Lynette Danylchuk & Kevin Connors. This highly readable book combines clinical experience and insight. It presents clear and practical information to support understanding and offers guidance for navigating a phased approach to treatment, handling foundational issues and potential challenges’ 2nd Edition due out July 2023, includes the latest research and treatment developments
Treating Trauma-Related Dissociation: A Practical, Integrative Approach, (2017), by Kathy Steele, Suzette Boon & Onno van der Hart. Written by leading experts, this comprehensive text extends the content of the skills training manual, (listed in the ‘Self-Help’ section). It offers a practical, thorough, and insightful approach to treatment based on the structural dissociation model
Treatment of Dissociative Identity Disorder: Techniques and Strategies for Stabilisation, (2018), by Colin Ross. Practical, concise and informative, especially useful for practitioners new to working with DID
Working with Voices and Dissociative Parts – A Trauma-informed approach, (2nd edn, 2019) by Dolores Mosquera.
A comprehensive, elaborative, and inspirational workbook, that is truly integrative, structured and collaborative, and informative for both the novice and the senior practitioner
26 notes
·
View notes
Note
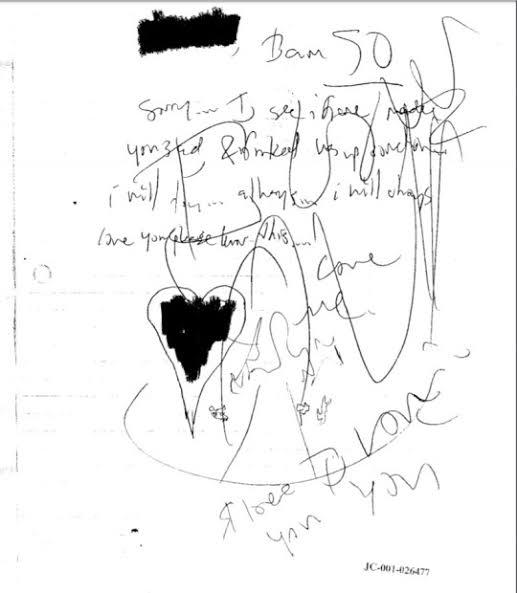
Hey so I saw your post about Dylan referring to himself as an entity and drawing spirals. Since youre a psycology student, i would love to hear your analysis of this. Also, if possible, could you do the same for Eric's writing? Thanks thats all
I was doing a lot of psychological analyzes of Jeffrey Dahmer and posting them here, but then I started attracting a lot of strange people, so I stopped...
But since a lot of people are asking for this, here we go 🙄
In Carl Jung's psychodynamic theory, spirals or mandalas are expressive artistic forms that can emerge during a psychotic episode when the patient's mind is trying to organize itself.
Here are many examples of art made by psychotic patients in a psychiatric hospital, they are from the book Images of the Unconscious by Nise da Silveira


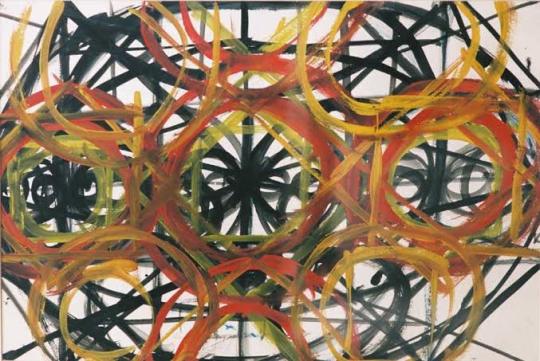
(it doesn't mean that everybody who does drawings like this are psychotic, obviously it has artistic styles and things like that, but these paintings were made by patients in hospitals. Nise was a brazilian doctor, and Jung was from Switzerland, they notice that without any contact, their patients were drawing the same spirals figures. You can also see that these drawings are somewhat organized because the patients were receiving treatment. You can see from the geometric shapes that there is a meaning, it is the mind trying to organize itself).
Not only did Dylan draw a lot of spirals, but you can also see that his drawings are extremely disorganized and don't make any sense at all.
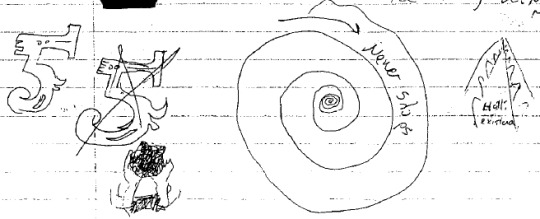
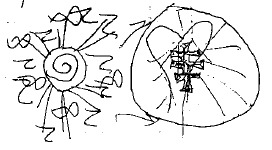
Furthermore, his writing is extremely confusing, it took me weeks to understand what he was talking about, (while I read Eric's diary in just one day and found it extremely boring)
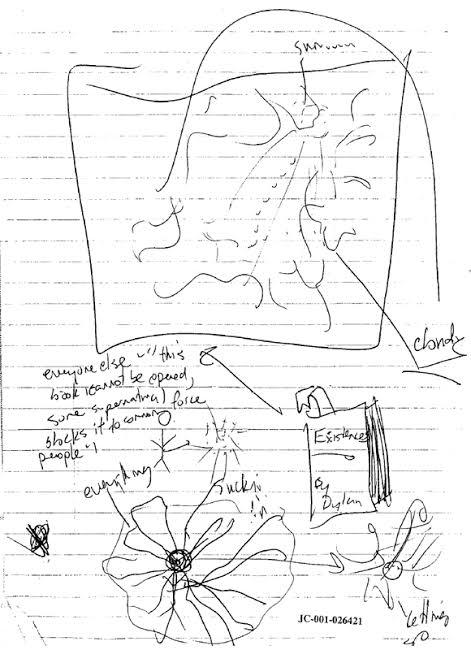
Here is an example, you can see that love (heart), the road, this fifth dimension, the donward spiral is all mixed up, extremly disorganized.
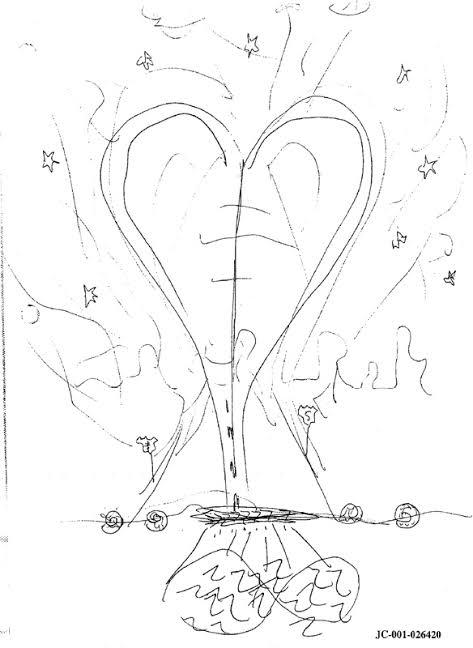
It's very different from Eric's drawings, which despite the violent themes, you understand what's happening
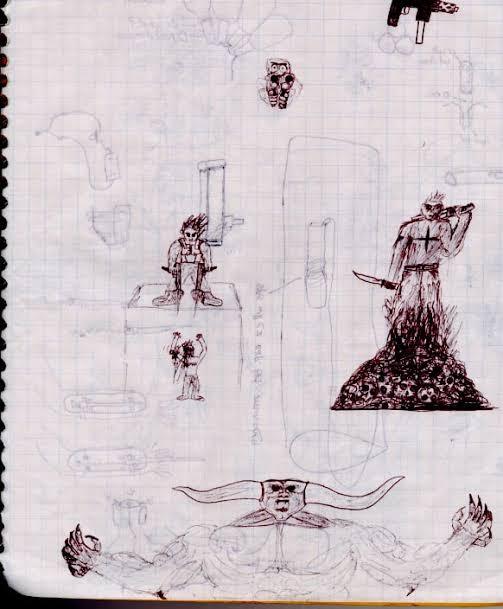
Dylan's writing often does not follow a chronological order, nor does he talk about real events of his life, he constantly refers to himself as if he were an entity that lives in another dimension (the number 5 in the drawings represents this fifth dimension), in other words, he was unable to establish a connection with reality. Unlike Eric who proclaimed himself a god to irritate people, as a form of rebellion, Dylan really believed in this, in his mind, he literally lived in another dimension. And these spiritual themes regarding the ego itself ("I am an entity") are indicative of psychosis as well.
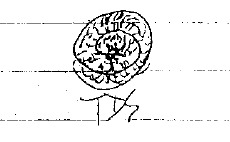
One interesting thing is that you can see that even the form of Dylan's writing is confusing. I'm not just talking about his bad handwriting, but he always wrote in the corner in a disorganized way, loose words without meaning. When he started his diary you can see that he was fine, but as time passed, his writing became more and more strange, he began to draw more and more these spiritual symbols, and his drawings became a great confusion.
I believe that his diary is a perfect example of a mind that deteriorated over time, but obviously this is just a supposition based on his diary. I also suppose that he wrote in moments of crisis, when he felt bad, sad, and needed to get these things out.
I know that a lot of people must interpret his diary in an artistic way, especially through his poems (and it still is!), but this is also an indication of a mind that was losing touch with reality
When he proclaimed himself the god of sadness, when he said that he had no friends, that he had no love, that no one would ever love him when he did have many friends who liked him, a functioning family that loved and accepted him, and still a promising future, since he was smart and was planning to go to college, all this god of sadness thing could be indicative of delusion too, he couldn't see how loved he actually was.
(there are cases of psychotic depression, it's very rare, but it does exist).
I know he was diagnosed with schizoaffective personality, which I agree with because often people with this diagnosis are also psychotic. But it really depends on how serious the case is, I have a friend who has this diagnosis and is also psychotic, but he has a good connection with reality and will graduate in psychology too.
Therefore, absolutely nothing about Dylan's supposed illness justifies what he did at Columbine. Eric himself was perfectly normal and also decided to do what he did.
#columbine#dylan klebold#eric harris#psychology#also i'm not a columbiner so please stay away#i just did because a lot of people wanted and so i can study too
87 notes
·
View notes
Text
Okay. Several of you requested my "the success of The Body Keeps the Score over Trauma and Recovery is symbolic of everything wrong with our world" rant. I am too tired and this topic is too intimately connected with my job for me to give you the full version, but here are the highlights.
(No reblogs on this one. Usual caveat that TBKTS has some valuable things in it and if it was illuminating or meaningful for you there's nothing wrong with that.)
TBKTS: positivistic ideas about science, leans heavily on the idea that the impact of trauma can be seen and verified through medical means; decontextualizing, politically neutral, edges towards trauma as free-floating concept not specific experience; lets the categories of victim, perpetrator, and bystander float away into fuzziness; buzzword-y, promoting quick fixes that don't require telling the trauma narrative. Written by a man who was exposed as bullying and otherwise mistreating his employees but has gone on after that to make untold amounts of money on the lecture circuit as a trauma theory celebrity.
T&R: unapologetically created out of the feminist movement and situates acts of violence within systems of oppression; insistently direct about the the inherently political act of believing survivors of trauma; deals with specific acts of violence and types of abuse as specific experiences leading to specific reactions; concerned with the particular psychodynamics of the victim-perpetrator-bystander triangle and impact of the bystander's inaction on the victim; honest about the fact that recovery is a hard, messy process with no shortcut that requires the trauma narrative to be told and witnessed and the survivor to be in contact with painful emotions. Written by a woman who started her career trying to get the prevalence of incestuous sexual abuse recognized within psychiatry, wrote an absolutely field-defining work and then had to retreat into partial retirement due to inadequately treated chronic illness and disability.
62 notes
·
View notes
Text
OHHHH THIS IS SO FUN thank you for the tag @aquadenks <3
rules: post the names of all the files in ur wip folder, regardless of how non-descriptive or ridiculous. let people send u an ask with the title that most intrigues them and then post a little snippet of it or tell them something about it! tag as many people as you have wips!
These are all hawks x reader except one LMAO so i'm just gonna put a brief hint next to them. I'M SO SORRY A LOT OF THIS IS SMUT I STILL HAVE HAWKSTOBER I WANT TO FINISH... I have a feeling this is gonna get people to scratch at me for not finishing these yet, but:
Your God Will Make You Speak in Tongues || Priest!Hawks × Zealot!Reader. This one will probably come out like.... never ever, it's my first slow burn and I want it to be like 50-100k words but I literally need to get better at writing long things first.
Like Father Like Son || a dive into Keigo's morality + history
Touch-Starved || This one is old so I'll have to do a major makeover but, title says it. This one is really cute!
Untitled || this is another substance use support drabble that I might not finish or post because I don't think I'm in the right headspace to be trigger-sensitive so it'd probably come out like, not super comforting?
Do You See Me? I Hope You Don't. || this one is uhhhh probably gonna be one of those fics I keep to me
Two more untitleds on the same topic I probably won't post
Untitled || this one is abt Hawks and his wings, no reader.
Asphyxia || this one is soooo fun like I am unsure if this will get me comments like "um. Weirdge." Or "oh my god kink unlocked" BUT I really like this one!
Nice To Me || being nicies to him, counterpart to Mean to Me (on my kinktober masterlist)
A Case For Psychodynamic Theory || DON'T ASK DON'T ASK DON'T ASK jk its not that bad
Clicker Training || aha
Pretty Boy || aha...
All In a Day's Work || shitty asshole boss! Hawks x employee!reader
Gluttony || panty stealer hawks turned munch. You know how it is.
Untitled || Hawks bullies u for your kinks...
Untitled || More bully!Hawks
Untitled || phone sex lmao
Untitled || he purposefully spoils reader until they literally can't get off without him. On purpose. LMAO.
Untitled || Hawks plays dress up with the reader aww
Untitled || Another sub!hawks, nothin special
Untitled || THE DABI CUCKING FIC MY BELOVED I will finish her eventually. Like this has been in my drafts since spring 2023.
Untitled || omegaverse drabble. Covers my face.
Untitled || foot fetish!Hawks lmao
Untitled || sub!hawks again
Untitled || this is the pred/prey fic
Untitled || puppy!hawks x dominatrix!reader
Untitled || the glove kink one
Untitled || a dark content one
Untitled || possessive!hawks x work partner!reader
Untitled || scummy best friend!Hawks x naive reader
Untitled || being SO mean to him (note to self this is day 25)
Untitled || keigo's first time hitting it raw fic
WOW this is a lot. I will finish them..... God willing.
I tag: actually just steal this and say I tagged you ^-^
20 notes
·
View notes
Note
do you have any good sources or tips on how to deal with apathy? im an artist and i realized i have no idea what getting inspired 'feels' like and im just kind of apathetic?
it might just be the tism, but its frustrating because i want to do things. (all my ideas dont feel like mine either so there's that)
Hi there,
Many neurodivergent people have something call Alexithymia, which is where you don’t know/explain what your feeling.
I found an article from Healthline that says:
“Alexithymia is a broad term to describe problems with feeling emotions. In fact, this Greek term used in Freudian psychodynamic theories loosely translates to “no words for emotion.” While the condition is not well-known, it’s estimated that 1 in 10 people has it.”
“The symptoms of autism spectrum disorder are wide-ranging, but there are still some stereotypes associated with this condition. One major stereotype is a lack of empathy, something that has largely been debunked.
At the same time, some research indicates that up to half of people with autism also experience alexithymia. In other words, it’s alexithymia that causes the lack of empathy, and not autism itself.”
I hope this helps answer your question. Thank you for the inbox. I hope you have a wonderful day/night. ♥️
30 notes
·
View notes
Text
Ne Kings/Base: What Could, not What is (Model S)
Ne Kings see life as a book with no ending. It is an never ending stream of new and contradicting information, so much so that they can only really retain true principles temporarily. They are constantly changing their mind, and can seem unreliable, irresponsible, and untrustworthy.
They do not care about concrete reality to the point that they would vandalize it, simply just to see what it can do.
They may seem amoral, and haphazard, like a Ti King, but unlike them, they seem to lack principles altogether, and have a boost in the unpredictability factor.
They can get bored easily, and are on the constant search for novelty, leaving old friends and partners behind, especially if ILE.
They are the fastest to accept change, and can seem rather unfazed.
Fe Vital (ILE): Likes to focus more on the sentimental possibilities, how they can see one react or feel.
Te Vital (IEE): Likes to focus on the more logical and efficient possibilities, how they can catalyze production.
Questions?
3 notes
·
View notes
Text
From M[0] & S
We made this mainly to find out if we're suffering from C-PTSD instead of PTSD. We wrote for hours on end on this. Especially the fact checking was intense. We constantly cross-checked the information with "Coping with Trauma-Related Dissociation" by Suzette Boon, Kathy Steele, and Onno van der Hart (2011). In the end we even let chatGPT Scholar AI, a GPT that we're using to access recent scientific papers, books and patents, check it for potential errors and it didn't find any. We also included book and study citations that support the mentioned knowledge. We hope this in depth analysis of Complex PTSD will be helpful to those of you that suffer from it.
If you have want us to expand on parts of this analysis or if you want us to correct any information, please inform us about it through Ask a Question or through commenting. We want the information we provide to be absolutely correct and based on actual modern research and well peer reviewed research so that it'll be most helpful to everyone.
_______________________________________________
Trigger Warning: This article discusses trauma, abuse, PTSD, and related sensitive topics that may be triggering for some readers. Please proceed with caution and take breaks as needed.
Understanding Complex PTSD: Causes, Symptoms, and Modern Approaches to Healing
Complex PTSD (C-PTSD) is a psychological condition that develops after prolonged exposure to trauma, such as childhood abuse or domestic violence. It involves chronic emotional dysregulation, dissociation, relational difficulties, and disturbances in self-organization. This blog delves into the causes, symptoms, triggers, treatments, and advice for survivors, drawing from Coping with Trauma-Related Dissociation: Skills Training for Patients and Therapists by Suzette Boon, Kathy Steele, and Onno van der Hart (2011), alongside recent scientific literature.
Causes of C-PTSD
C-PTSD arises from sustained, repeated trauma. Unlike PTSD, which often stems from a singular traumatic event, C-PTSD results from long-term exposure to situations where escape is impossible.
Childhood Abuse: Repeated physical, emotional, or sexual abuse by caregivers fragments the child’s personality into dissociative parts. Emotional Parts (EPs) store trauma memories, while Apparently Normal Parts (ANPs) perform daily functions. The division of self into EPs and ANPs is central to Structural Dissociation Theory, which explains how traumatic memories are split off into EPs to protect the ANP from being overwhelmed. While this theory remains widely accepted, recent research critiques its emphasis on childhood trauma as the sole cause of dissociative parts, suggesting more complex, multifactorial causes of dissociation ([Suzette Boon, Kathy Steele, and Onno van der Hart, Coping with Trauma-Related Dissociation: Skills Training for Patients and Therapists, 2011, pp. 12-13]; Hans-Peter Kapfhammer, Psychodynamic Psychiatry, 2018).
Domestic Violence: Continuous exposure to domestic abuse leads to chronic activation of dissociative coping mechanisms, as survivors struggle to process ongoing trauma. These mechanisms can include emotional detachment, hypervigilance, and intrusive memories ([Valerie Valdez, Brenda Greenfield, and Margaret Ellis, Journal of Interpersonal Violence, 2019]; [Suzette Boon, Kathy Steele, and Onno van der Hart, Coping with Trauma-Related Dissociation: Skills Training for Patients and Therapists, 2011, pp. 14-15]).
Neglect: Prolonged neglect in childhood can lead to dissociative defenses, where the child emotionally detaches to survive, often resulting in severe attachment issues and emotional dysregulation in adulthood. Recent research highlights the importance of recognizing various forms of neglect and their long-term consequences (Vera Rüfenacht, Stefan Gerlich, and Richard Lally, Journal of Child Psychotherapy, 2023).
Detailed Symptoms of C-PTSD
The symptoms of C-PTSD can be broken down into several categories:
Emotional Dysregulation: Individuals with C-PTSD often experience overwhelming emotions that they find difficult to control. These emotions can include anger, sadness, or fear. Dissociative parts may take over in moments of stress, leading to impulsive behavior or detachment. This emotional overwhelm is often driven by EPs holding trauma-related affective states, while the ANP attempts to manage daily life. It is crucial to understand the roles of EPs and ANPs in emotional regulation and how this division influences daily functioning ([Ellert Nijenhuis, Onno van der Hart, and Kathy Steele, Journal of Traumatic Stress, 2005]; [Suzette Boon, Kathy Steele, and Onno van der Hart, Coping with Trauma-Related Dissociation: Skills Training for Patients and Therapists, 2011, pp. 101-102]).
Dissociation and Fragmented Identity: Structural Dissociation Theory explains how trauma fragments the personality into dissociative parts. EPs are fixated on trauma, while ANPs handle day-to-day tasks, avoiding trauma reminders. This disconnection can make survivors feel detached from their emotions and experiences, contributing to difficulties in both personal and professional spheres ([Suzette Boon, Kathy Steele, and Onno van der Hart, Coping with Trauma-Related Dissociation: Skills Training for Patients and Therapists, 2011, p. 140]; João Machado, Pedro Carvalho, and Ana Lima, Revista de Psicoterapia, 2022).
Relational Difficulties: C-PTSD survivors often experience significant difficulties in forming and maintaining trusting relationships. This is due to dissociative parts, particularly EPs, interfering with emotional vulnerability and intimacy. Survivors may experience emotional withdrawal or heightened mistrust, leading to relational isolation. These challenges in relational dynamics often worsen without intervention ([Suzette Boon, Kathy Steele, and Onno van der Hart, Coping with Trauma-Related Dissociation: Skills Training for Patients and Therapists, 2011, pp. 172-176]).
Negative Self-Perception: Feelings of guilt, shame, and worthlessness are common in individuals with C-PTSD. Survivors may internalize their trauma, believing they are responsible for the abuse they experienced. This negative self-perception is often held by EPs, which retain the emotional weight of the trauma. Survivors may struggle with feelings of inadequacy and self-blame, which can be exacerbated by dissociative processes ([Suzette Boon, Kathy Steele, and Onno van der Hart, Coping with Trauma-Related Dissociation: Skills Training for Patients and Therapists, 2011, p. 250]; [Hyland, Andrew, Scally, and Benner, Psychological Review, 2023]).
Somatic Symptoms: C-PTSD often manifests in physical symptoms, including cardiovascular, respiratory, neurological, gastrointestinal, and immune-mediated disorders. These somatic symptoms are thought to result from the body’s dysregulated stress-response system. Dissociative parts may cause a disconnect between the survivor’s mind and body, leading to difficulties in recognizing or addressing the physical manifestations of trauma ([M. Gupta, Journal of Psychosomatic Research, 2013]; [Suzette Boon, Kathy Steele, and Onno van der Hart, Coping with Trauma-Related Dissociation: Skills Training for Patients and Therapists, 2011, pp. 170-175]).
Loss of Meaning: C-PTSD survivors may experience a profound loss of meaning and purpose in life. Dissociative parts often hold conflicting beliefs about the self, the world, and others, complicating the survivor’s ability to find meaning or direction. This internal conflict often presents as existential crises, especially in relation to their sense of identity and purpose ([Suzette Boon, Kathy Steele, and Onno van der Hart, Coping with Trauma-Related Dissociation: Skills Training for Patients and Therapists, 2011, pp. 240-250]).
Discussion on Somatic Symptoms in C-PTSD
Somatic symptoms in Complex PTSD (C-PTSD) often manifest as physical discomfort, chronic pain, and other bodily issues that reflect the mind-body disconnection caused by prolonged trauma. These symptoms are particularly challenging for survivors because they are both psychological and deeply embedded in the body’s stress-response systems.
1. Connection Between Trauma and Somatic Symptoms
Survivors of C-PTSD frequently experience physical symptoms such as headaches, gastrointestinal disturbances, muscle tension, cardiovascular issues, and chronic pain. These issues are often exacerbated by the body’s chronic activation of the fight-or-flight response, even in non-threatening situations. Dissociative parts, such as Emotional Parts (EPs), store unprocessed trauma memories, which can manifest as physical ailments when triggered. Somatic symptoms arise because EPs and ANPs lack communication and coordination, leading to physical dysregulation ([M. Gupta, Journal of Psychosomatic Research, 2013]).
2. The Role of the Vagus Nerve and Autonomic Dysregulation
Recent research in the neurobiology of trauma highlights the role of the vagus nerve and autonomic dysregulation in C-PTSD. Dysregulation of the autonomic nervous system (ANS) contributes to chronic pain and stress-related illnesses. The polyvagal theory explains how the vagus nerve affects emotional and physical health, suggesting that trauma survivors may remain stuck in a state of hyperarousal or dissociation, leading to persistent somatic symptoms ([Stephen Porges, Journal of Psychophysiology, 2022]).
3. Psychosomatic Effects of Trauma
The physical impact of trauma can be seen in chronic conditions like fibromyalgia, irritable bowel syndrome (IBS), and migraines. In many cases, these conditions are exacerbated by dissociative episodes or emotional flashbacks. Survivors may not consciously connect their physical symptoms to past trauma, as dissociative parts often hold these experiences in isolation from daily functioning (João Machado, Pedro Carvalho, and Ana Lima, Revista de Psicoterapia, 2022).
4. Triggers in C-PTSD
Triggers are external stimuli that can provoke trauma memories or dissociative responses. Examples of common triggers include:
Sensory Triggers: Sights, sounds, or smells that resemble the original trauma can evoke flashbacks. For example, the smell of alcohol may trigger memories of an abusive parent. Sensory triggers are often directly linked to traumatic memories held by EPs, which react reflexively to external stimuli. Sensory triggers can activate dissociative parts, leading to intense emotional responses (Richard Bryant, Allison Bryant, and Naomi Andrews, Behavioral Research and Therapy, 2005).
Relational Triggers: Close relationships can activate feelings of vulnerability, causing emotional withdrawal or aggression when dissociative parts perceive the relationship as dangerous. EPs, which hold trauma-related fears, may react defensively to intimacy, resulting in relationship difficulties ([Suzette Boon, Kathy Steele, and Onno van der Hart, Coping with Trauma-Related Dissociation: Skills Training for Patients and Therapists, 2011, pp. 172-176]).
Body Sensations: Pain or discomfort in the body, particularly during medical procedures, can serve as a trigger for individuals with trauma histories involving medical trauma. The body itself can become a trigger when EPs associate certain sensations with past trauma, leading to dissociative reactions (Lev-Ari Sharon and Kipnis Angel, PeerJ, 2021).
Modern Treatment Approaches for C-PTSD
Advancements in trauma treatment between 2020 and 2024 have offered new, evidence-based approaches to managing C-PTSD, particularly regarding the integration of somatic therapies and neurobiological interventions. Below are seven modern treatment approaches that address both the psychological and somatic aspects of C-PTSD.
1. Eye Movement Desensitization and Reprocessing (EMDR)
EMDR remains a leading treatment for C-PTSD, particularly in integrating fragmented trauma memories held by dissociative parts (EPs and ANPs). EMDR uses bilateral stimulation, often through eye movements, to help patients reprocess trauma, allowing dissociative parts to reintegrate into a cohesive sense of self. Studies have shown that EMDR is effective not only in managing emotional symptoms but also in reducing somatic symptoms like chronic pain and tension (Ad de Jongh, Erik ten Broeke, and David Hornsveld, Journal of EMDR Practice and Research, 2019).
2. Somatic Experiencing (SE)
Somatic Experiencing (SE) focuses on helping trauma survivors release stored trauma energy from their bodies. This body-centered approach addresses autonomic dysregulation, a key factor in chronic somatic symptoms. SE emphasizes slow, mindful awareness of bodily sensations, helping survivors re-establish a sense of safety in their bodies. This can be particularly helpful for managing symptoms like gastrointestinal distress or muscle tension ([Peter Levine, Somatic Psychotherapy, 2020]).
3. Trauma-Informed Yoga
Trauma-informed yoga offers a somatic therapy that integrates mindfulness, breath work, and physical movement. This form of yoga is designed to help survivors reconnect with their bodies in a safe and controlled manner, improving both emotional regulation and somatic awareness. It has been shown to significantly reduce symptoms of hyperarousal and help with the integration of dissociative parts ([David Emerson, Journal of Eating Disorders, 2021]).
4. Polyvagal Theory-Based Therapy
Therapies based on the polyvagal theory focus on regulating the autonomic nervous system, particularly the vagus nerve, which plays a central role in trauma recovery. These therapies aim to move the survivor out of a state of chronic hyperarousal or dissociation (freeze state) by promoting safety and social connection. Polyvagal-informed therapies help survivors regain the ability to engage with the world safely, reducing both emotional and somatic symptoms ([Stephen Porges, Journal of Psychophysiology, 2022]).
5. Internal Family Systems (IFS)
Internal Family Systems (IFS) therapy is highly effective for treating C-PTSD by addressing the dissociative parts (EPs and ANPs). IFS helps individuals recognize and dialogue with their fragmented parts, allowing for trauma integration. IFS can reduce both emotional dysregulation and the physical manifestation of trauma stored in the body, such as chronic pain or unexplained somatic symptoms ([Richard Schwartz and Martha Sweezy, Internal Family Systems Therapy, 2021]).
6. Neurofeedback
Neurofeedback is a cutting-edge technique used to retrain the brain's neural pathways, helping survivors of C-PTSD regain emotional and physiological balance. It can be particularly useful for addressing the dysregulated stress response that contributes to chronic somatic symptoms. By providing real-time feedback on brain activity, neurofeedback helps the brain learn to self-regulate, reducing both emotional and somatic symptoms (Peter Schoenberg and Duncan David, Current Opinion in Psychology, 2022).
7. Cognitive Processing Therapy (CPT)
Cognitive Processing Therapy (CPT) is a form of cognitive-behavioral therapy that focuses on changing trauma-related thought patterns and beliefs. CPT has shown to be effective in reducing C-PTSD symptoms by addressing distorted cognitions, such as guilt, shame, and fear. It can also help reduce somatic symptoms as the cognitive integration of trauma lessens the body’s stress response (Kathleen Chard, Patricia Resick, and Candice Monson, Current Psychiatry Reports, 2021).
Advice for C-PTSD Survivors
Here are 10 key tips from Coping with Trauma-Related Dissociation: Skills Training for Patients and Therapists (2011) by Suzette Boon, Kathy Steele, and Onno van der Hart:
Grounding Techniques: Use grounding exercises to stay present during moments of dissociation. This can involve focusing on physical sensations, such as touching a textured object. Grounding helps anchor the Apparently Normal Part (ANP) to the present moment ([Boon, Steele, and van der Hart, 2011, p. 199]).
Establish Safety: Create a safe physical and emotional environment to reduce the likelihood of triggers. Safety is a prerequisite for working with Emotional Parts (EPs) and building internal cooperation ([Boon, Steele, and van der Hart, 2011, p. 180]).
Mindful Breathing: Practice mindful breathing to regulate emotional responses and remain calm during stressful situations ([Boon, Steele, and van der Hart, 2011, p. 130]).
Building Support Networks: Engage with safe and supportive individuals to develop trust and emotional resilience ([Boon, Steele, and van der Hart, 2011, p. 164]).
Self-Compassion: Approach dissociative parts with understanding and compassion, acknowledging that they served a protective role during trauma ([Boon, Steele, and van der Hart, 2011, p. 240]).
Track Emotional States: Keep an emotion journal to track patterns and recognize emotional triggers, which can help in managing dissociation ([Boon, Steele, and van der Hart, 2011, p. 250]).
Pacing in Trauma Work: Take trauma processing slowly, ensuring safety and stability before addressing deeper trauma-related memories ([Boon, Steele, and van der Hart, 2011, p. 230]).
Set Boundaries: Establish healthy boundaries in relationships to protect against re-traumatization ([Boon, Steele, and van der Hart, 2011, p. 172]).
Focus on Strengths: Identify and focus on personal strengths to counterbalance feelings of helplessness ([Boon, Steele, and van der Hart, 2011, p. 112]).
Take Breaks: Healing is a long process; it’s important to take breaks and allow yourself time to recover between therapy sessions ([Boon, Steele, and van der Hart, 2011, p. 248]).
Conclusion
C-PTSD presents both psychological and somatic challenges that require a holistic approach to treatment. Modern therapies, such as Eye Movement Desensitization and Reprocessing (EMDR), Somatic Experiencing, and neurofeedback, address not only the emotional dysregulation but also the chronic physical symptoms resulting from long-term trauma. With continued advances in trauma research, treatment approaches are increasingly capable of providing comprehensive care to survivors, integrating body and mind toward lasting healing.
#cptsd recovery#trauma recovery#traumagenic#trauma#childhood trauma#abuse survivor#trauma survivor#complex ptsd#dissociation#somatic symptoms#recovery#mental health#mentalhealth#recovery inspiration#mental health support#mental wellness#healing journey#trauma response#post traumatic growth#mental health journey#traumagenic system#dissociative system#traumagenic did#did system#cptsd awareness
3 notes
·
View notes
Last Seen Blogs

johngsadv-blog
Untitled

vroomvroomcooking
Vroom Vroom

skmanikpuri
Untitled

sherapropertyagent
SHERA Property Agent

moregreenory
moregreenory