#and prescribe hrt as he recommends
Text

Gothmog clearly understands that Someone has Done Some Bullshit to me and I require Affection from her, but sadly does not understand that in doing so is preventing me from taking the necessary response
#doctor who's been refusing to follow national advice from the nhs and association of gps to work with my private endo#and prescribe hrt as he recommends#was supposed to call this afternoon#having previously accepted that she would have to write such prescriptions#but only after id already started them privately#well my phone had its volume up all day#and it did not ring#i did get a missed call though#immediately followed by a text telling me to ring the reception to rearrange if still needed#this appointment was booked a month ago#i immediately ring the reception#it is still only a minute since the missed call#(she must have hung up as soon as it connected)#then I spend 15 minutes in a queue#which depressingly is a lot better than it often is#only to be told shes gone home for the day and the next time it can be rearranged for is in another month#at this point its clear theyre just going to keep pissing me around#so i need to find a new gp#as well as get and pay for another private prescription that should be covered by the nhs#and submit a complaint because jfc
4 notes
·
View notes
Text
Gender, Dissociation and Clinical Stigma - The Third Person
Before I begin I just want to note that typically Media, Myself and I entries are aimed at depictions of dissociative disorders in popular fiction. Today's entry is a graphic novel memoir by a transgender woman with dissociative identity disorder. As it's both not in the public zeitgeist and good representation by virtue of being lived experience of someone who struggled within the mental healthcare system I want to recommend people buy the book (or check it out of their local library). I fully support the artist and want to prop up something good and beautiful.
With that said, let's begin...

CW: therapy abuse
With all the recent hysteria in the US and UK media over transgender healthcare it can be easy to forget the hurdles we all have to climb to receive care. Though Informed Consent is becoming more of a standard practice these days the DSM-5 Criteria for Gender Dysphoria indicates a 6 month requirement for observation before HRT can be prescribed. Many of us needed to jump the hoops of living 6-12 months "in the gender role that is congruent with their gender identity" before we were allowed to begin our gender journey in earnest.
Of course. This requires a clinician (or two for surgical options) to observe this, monitor it and sign off on it. But therapists are humans and are full of prejudice, bias and their own beliefs. They aren't guaranteed to think it is medically necessary or positive for a person seeking gender affirming care to receive it.
So where does DID fit into this picture?
A study, published in 2015, states clearly that 30% of transgender individuals met the criteria for a dissociative disorder.
Yet even still, The World Professional Association for Transgender Health (WPATH), the gold standard for transgender care included this warning in their Standards of Care up until September 2022.
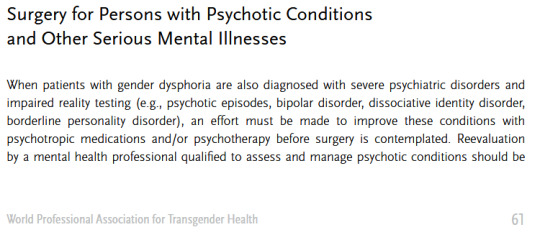
(source)
Fortunately that passage is no longer included in WPATH guidelines as of the 8th revision released in 2022. I shall say the above passage did grant a scare for us, though, as it was very much the practice when we were going for our surgery.
Standards of Care improve and medical understandings of both gender and dissociative care are becoming kinder towards clients.
Even still. There's always that fear. That months of therapy could be wasted on a clinician who was never going to sign off on HRT and was never going to believe our lived experience as a system.
We wouldn't have gotten nearly half as far as we have gotten without our therapist helping us identify our condition, manage our symptoms and develop cooperation and communication.
It's terrifying to think what life would be like if our symptoms not only went unmanaged, but we were made to feel fake and attention seeking by the very person we paid to take care of us...
-
With that intro in mind, The Third Person by Emma Grove is a memoir told in graphic novel format over 920 pages covering the period of life where she began therapy in hopes of receiving feminizing HRT not realizing she had an undiagnosed case of dissociative identity disorder.
When one opens the book they will see an Author's Note declaring that every word in the book is as accurate as Emma's memory will allow and any edits are to streamline the story, not to tailor anything to match the author's point of view and there is a dedication:
"For Katina - We finally did one together"
The story proper begins in media res Winter 2004, as Emma asks her therapist if he would like to hear about the book she was reading and the therapist responds asking why the client decided to speak with him "as Emma" today. Emma, confused, does not understand the question and is probed about her parts, about Ed and Katina and about her childhood. That last word being enough to cause Emma to freeze up, dissociate and...
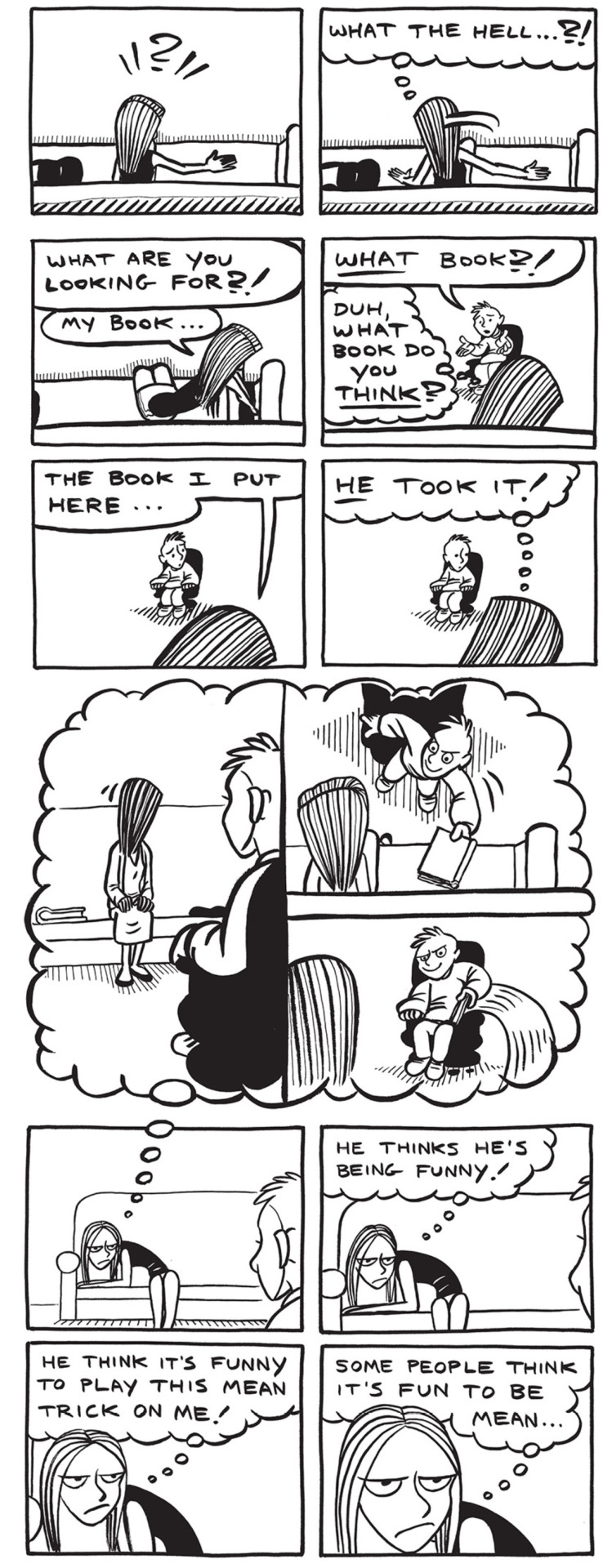
This simple intro gives us all the context a reader needs to understand the antagonistic dynamic between Toby, the therapist, and his patient(s). Both client and patient are unable to understand the other and harbor suspicions about the other's intentions.
Without the context we only know Emma had a book, she no longer has a book and she suspects her therapist of being a mean person who is playing tricks on her.
We will get context later.
The first chapter of the book provides an introduction to the author's late teens and early 20s where they explore their gender identity and have their first experiences with their masked dissociative disorder.
The book goes to lengths to show the stress of the author dividing themselves between having to present male in their public life and sneaking out to bars where they can wear make-up, wigs and outfits to present female.
They take on their legal name, Ed, during their public life and when going out to clubs take the name Katina, from the first bar they visited presenting femme. The name Emma comes later when the system is working to transition into living as a woman in all aspects of their shared life.
The book patiently explores the stress of having to divide ones own self for their safety in spaces where they cannot present their truth without threat from an intolerant society. If 30% of transgender people suffer from dissociative disorders then a much higher number of them know the stress of having to compartmentalize themselves into different presentations for different audiences.
For us, we know that pain all too well. Our birth identity remains with us as a member of our own system. Less a ghost of our past and more a remnant of a mask we constructed to perform the version of self required for our safety.
The artwork does a good job of displaying switches and co-consciousness with subtle expression work, the hair style/wigs that each alter favors. For example we have the left displaying co-consciousness and a switch.


As the years go on, Katina finds ways to go out to the club and exist in her comfort and Ed labors hard to ensure that they can live for the times they get to "become" themselves.
Katina is established to be a fierce personality who will get aggressive when people push against her. She loves to dance and sing and party at the club. She is both a free spirit without inhibition and a fierce protector who will keep the system safe.
I recall feeling a deep fondness and connection towards Katina when we first read the book.
Once the narrative has firmly established the history that lead to the system seeking HRT we are brought into the meat of the book. A white void with a sofa and an armchair. The therapist's office where Katina, Emma and Ed speak with Toby.
Toby is a trans man that Katina believes to be an ally who will sign off on their HRT once the prerequisite 3 month waiting period is over. Unfortunately over the course of those months Toby becomes aware of Emma and Katina's switches and is convinced that it would be unethical for him to sign off on HRT when it is possible that there may be another 'guy part' in there who will 'wake up' one day and decide that he did not want to transition.
To his credit, once Toby suspects a dissociative disorder he does offer Emma a referral to a specialist. They do not take it as they just want to be signed off for HRT and have no interest in exploring their situation beyond transitioning. So they stick with Toby, convinced that another transgender individual will support them.
Toby, however, sticks to his guns and refuses to agree until they manage the DID.

In the opening, sampled above, Emma switches out at the mere mention of her childhood. Here we find that Katina will front any time Emma is made to think about her past and she refuses to allow Toby to force her to think about it or discuss it. She goes as far as to demand Toby promise not to push which, again, Toby refuses.
During this conflict both sides have exaggerated gestures of frustration, many exclamation points and underlined words. This is not a healthy dialogue at all. Toby is refusing to find middle ground or guide the therapy towards its intended destination. He denies all Katina's attempts to negotiate around the need to talk about her childhood (something she is convinced at this point has nothing to do with her stated goal of HRT) and continuously pushes that she needs to talk about it, without elaborating as to why.
Toby, untrained in dissociative disorders, is focused on getting her to open up about her childhood trauma. Katina, uninterested in exploring trauma, wants to be signed off for HRT. Neither side is willing to budge.
This isn't therapy. This is an argument.

Recently I wrote a Tumblr post about the "Hair Dryer Incident"
The Hair Dryer Incident is a story about a patient with OCD whose life was being massively disrupted by the fear that they had left their hair dryer plugged in at home and it would burn their house down. The clinician advised them to take the hair dryer to work with them every day so that they could see the hair dryer with them and not have to drive home to ensure it was safely unplugged.
There was debate in medical circles about whether this was "enabling" because it did nothing to treat the illness, only managed the life disrupting symptom of needing to drive home to check that the dryer was not plugged in.
For Toby in this scenario he believes that allowing Emma to transition would be "enabling" the sickness that he perceives, that being dissociative identity disorder. He has brought his own baggage into the office and only views Emma and Katina as parts of Ed. No amount of Emma and Katina self-advocating in his eyes will change his mind because they are not "real" in his view.
Of course, he is not fully sold on Emma's condition being real either. There is a sequence in which Emma is left alone in the room and she, having a fascination with books, checks out Toby's bookshelf. This causes Toby to become suspicious and decide that Emma has been reading the medical textbooks on dissociative disorders in order to fake an illness and trick him.
This is not a healthy therapeutic alliance and Toby is breaking all 3 key pillars of establishing a strong patient/client partnership.
Much of modern therapy techniques are based on the concept of Therapeutic Alliance. The history of which dates back to Sigmund Freud and the concept of transference but was refined and redefined by Carl Rogers in the modern Patient Centered Therapy (sometimes referred to as Rogerian Therapy).
With that in mind let's examine the 3 key elements of successful PCT(*) and how Toby failed.
Lead with a Patient Centered Approach
This means to check all baggage at the door. Cultural biases have no room inside the clinic (during the book Toby openly mocks Emma's faith in God) and that the patient's priorities are the ones that should be focused on. Both client and clinician should be on the same page of what treatment is being sought, what goals are and how they will be achieved. Toby and Emma (or Katina and Ed) never establish this agreement during their time together. Katina/Emma/Ed are firm in their desire to transition and Toby is firm on his refusal to allow this until the DID is addressed.
Set clear goals with a treatment plan.
A good treatment plan will have dates, targets and regular review and reward honesty for both/all parties involved in the alliance. Toby is telling Emma and Katina that they need to open up about their childhood but does not explain how this will benefit or what their goals are. Simply "it's good to talk about it" with no direction or assurances.
Regularly review satisfaction with the therapeutic process, relationship, and treatment plan.
This element states that it is important that the clinician be upfront with any potential misdiagnosis and discuss any skepticism in the process and lead from a position of patient satisfaction. I do not need to highlight how Toby failed to lead from a position of patient satisfaction here.
Clearly Toby has a personal concept of what the correct approach is and is holding Emma/Katina's gender affirming care hostage until they can satisfy his unspoken objectives. Correctly applied PCT should be a discussion of mutual agreement and achievable goals worked over a period of time. Toby is not applying these principals at all. His modality simply seems to be "talk about it."
I'll be an ethical writer who discloses their biases and say I despise PCT/Rogerian therapy. It is, however, the leading modality within western therapy and it is well researched. Not to mention it is the modality Toby appears to be utilizing in the book.
I firmly disagree with Freud on all things (except the concept of infant experiences have lifelong ramifications. A broken clock is right twice a day) and disagree with Rogers on the idea that the client has all of the answers and needs to get out of their own way.
An issue with this is that DID is a covert disorder and it will do everything it can to stay hidden. PCT does not offer an environment where patients will be able to navigate their condition as unless they are aware of their symptoms, how and when they manifest and are open to discussing those facts they will naturally steer away from circumstances that would lead to a diagnosis. Most people, including myself, have to exist in the mental healthcare system for 5-12 years before being correctly diagnosed with DID(*) and will experience a number of incorrect diagnoses before finding appropriate care. For us it was 9 years and 7 diagnoses.
So. Toby's directive is that the system needs to get to the root of the condition and neither Katina nor Emma are willing to open up about their childhood.
Katina continues sticking to her guns and refuses but Emma, desperate to start her medical transition, agrees to open up and the two form a shaky alliance where week by week the pair go back and forth between alliance and conflict.
In time Emma describes her childhood being raised by her grandfather who was physically abusive towards her. All too quickly Katina's fears are justified by Toby's combative approach to patient care.
One session Emma demands to know why she cannot work on her DID while she transitions and Toby states firmly that she is "not transsexual" which triggers Emma to dissociate into a black void that no one can reach her within.
She wanted to be seen and regarded as a woman and a trans man told her flat out that he cannot and does not see her as such.
Going back to the hair dryer incident as a reference for a moment. Ed is a member of the system and does show up for therapy on some days. At a point Katina, fed up with being denied treatment, makes a plan to quit their job and start a new life living as a woman 24/7. Ed creates a safety net to prevent this from ruining their collective life and continues to work in the meanwhile.
Ed's role in the system has been ground down to working and working alone. He spends his days keeping so busy that he cannot dwell, a panel having the thought bubble "I can't slow down! If I slow down I have to think!" which is depressingly relatable to how we were in the worst years of repressing our gender identity.
If Ed is unhappy living as a closeted man who has to occupy himself 24/7 to stop from caving in on himself, if Emma and Katina are both completely stunted by their inability to transition; is it ethical to allow them to transition and to work on their condition while allowing them the freedom to live openly as their chosen gender and prevent a circumstance that is harming the entire system?
Toby seems to think it is enabling.
30% of the transgender individuals in the study above were observed to meet the criteria for a dissociative disorder. Living a life where one must mask has severe detrimental impacts on a person's psychology. This is true not just for transgender individuals but for those with autism (*) and other individuals on the LGBT spectrum (*) where the cognitive dissonance between who a person values themselves to be versus how they must present to the world causes the mind to dissociate further and allow contrary thinking to exist in individual pockets of a person's life as well as creates an alienation of the self. Healing under these circumstances requires accepting and embracing oneself, not creating a further divide.
After Toby "caught" Emma looking at the bookshelf he became convinced that she was faking her condition. That she had been plucking symptoms from a book and performing them for him. That she fit the criteria "too well"
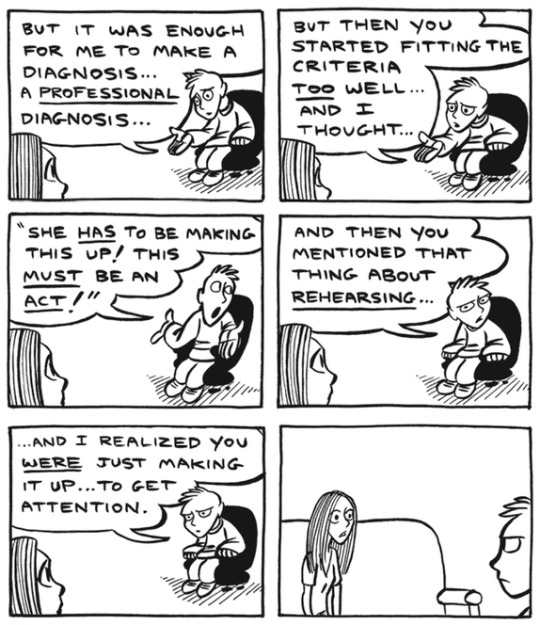
Emma rightfully demands to know why she would complicate her receiving HRT by doing something that prevents her being able to. The pair bicker and Toby cuts off the session abruptly.
in the heat of the moment, assuming that Emma was an attention seeker who does not deserve care, Toby declares "Your grandfather was right to hit you."
Even Emma later admits later that therapy should have ended with Toby right there and then. Hindsight is 20/20, as they say. Alas, a mixture of finances and sunk cost keep Emma returning to the chair week after week.
Being trans and having DID are terrifying. In order to receive care and treatment we must insist to a world that what is happening in our hearts and minds is true in spite of all that the world outside tells us is true. We need to not only reach that conclusion within our own lives but must express that truth loud enough that the people around us see it, regard it and accept it.
As so many things in this world are, it's so hard to earn and so easily burned.
"You're faking it for attention" is such an easy sentence to fling at someone and in a therapeutic setting all things should lead to curiosity. Even if a person were faking, it's not normal and healthy behavior for someone to do that. Toby is displaying a complete lack of curiosity and compassion. He is framing himself as the victim in a potential deception from someone who is paying what little money they can put together to receive his care.
I hate Toby.
As the story continues, Emma and her system begrudgingly continue, flitting back and forth between a healthy and unhealthy dynamic with their therapist that shares a lot of similarities to abuse honeymoons. It is worth noting that as the book is a memior it will inevitably be painted with the author's personal view of past events because, as discussed in the Umineko article on recontextualized memories, a human mind cannot avoid applying present understandings to past experiences when recalling memory. This is seen in the book when we see things that Emma cannot possibly have witnessed, such as Toby's facial expression after she leaves the office.

This is not to throw shade at how Emma depicts her former therapist, as he was quite horrid to all 3 of them and quite obviously did more harm than good during their time together. I just wish to note that skewed perspectives are an inevitability.
Even still. They do make some progress in talking about the situations. We come to learn of the system origins and how Katina was a friend to the young and lonely child they used to be and that their abusive childhood was centered around physical abuse from their grandfather.
While discussing this Emma notes that she could make Katina go away forever with a single phrase. A few short words that she can never ever say and mean or Katina would go away and never come back...
and I think that's where I'll stop with the synopsis. I (specifically me, Dawn) broke down in tears the first time I read the book and I have no will to put myself through that again at this exact moment and I wish for you all to have the catharsis of experiencing it for yourself.
I will say in way of positivity that the story is quick to make its conclusions in the final chapters by displaying therapy done right and the fact that even if parts can no longer be heard or even felt, they will always endure in moments where they can add a little color to the world.
They got to write this book together, after all.
For all the sadness this memoir elicits it speaks an honest and hard truth of the desperation, isolation and confusion that can be found in managing sentiments of identity and gender in a time when there was so little understanding and acceptance, particularly for transgender people.
We are lucky these days to have the internet as it is where we can create community and find our people and in finding our people have a better understanding of who we are and how we can live our truths. Visibility of transgender and plural populations has been increasing in part due to the fact we are able to feel unalone and forge community.
2004 did not have those luxuries and I am saddened that Emma Grove had to live through that stigma and lost so much time to unethical and prejudice care from a clinician.
I do hope that in the future we can continue accepting and encouraging one another and living lives where we are not forced to hide, mask or pretend.
-
For other Media, Myself and I articles, please check out the following:
#dawn posting#media myself and i#media essays#plurality#did#watch me post my trauma in public#this is my gender and I am proud of it
64 notes
·
View notes
Text
I have an actual appointment with a real trans clinic coming up. I'm excited and scared at the same time
I've had a lot happen to me in doctors' offices.
As a teen, I had doctors give me antipsychotics to make me "normal." I've had others since who recommended me electroshocks and this weird magnet helmet thing. Some of them laughed when I told them I had experienced things they should have reported to relevant authorities (and also my parents? they didn't care either, though).
My first HRT doctor talked like an expert but only had a little experience in the field. My dosages and blood tests were handled well, and he gave me injectables by default. He got very familiar with me and starting trying to get me to let him examine my body. Unfortunately, i trusted him. He did prescribe me benzos regularly out of "concern" though. Does that make me cheap? I've done worse for less, I guess. If nothing else, I was free of narrow WPATH guidelines for a few years.
A few doctors in-between just filled my prescriptions and never spoke to me. I figured they wanted to get me in and out of the office quickly and quietly. I often didn't get blood tests as a result. Sometimes, I had to get my meds from alternative sources.
I had a doctor responsible for my care treat me like wet shit for five appointments and then just ghost me without refills. He laughed in my face when I told him i wanted to talk about progesterone and threatened to "take away" my medication if I didn't comply with his decisions. He reduced my dosage to the point that my meds weren't working and I was forced to buy supplementary amounts online. He insisted it was in the WPATH guidelines, but he also didn't check my blood very often. He was a very pushy man and I hated his eyes.
I started running out of HRT. To make matters worse, a package I had ordered as a stopgap was seized by customs. My last option was the shitty hotline on my insurance card. They never work for me, but I tried.
The guy I connected to first was in Alabama. You can guess how it went. I hate it when breeders couch their disgust in sanitized terms. It's like if someone painted a portrait of a monster, but never painted the figure itself. The background and foreground are there, but the intended figure is just filled in with raw canvas. They didn't color and detail the monster, but it's still clear that it's there. Everything else frames it in place and offers clear context for it.
The second was in Stillwater, Minnesota, and he was just confusing. He told me that he couldn't refill my medications because they were potentially dangerous. The spiro supposedly carried a serious risk of blood clots and required blood tests. He said that if I really needed this medication, my doctor would have ordered blood tests. I tried to explain my situation, but he wouldn't listen.
The real ridiculous part was the estradiol. He said it caused cancer and was a known carcinogen.
I told him otherwise, which upset him. He brought up breast cancer, so I told him that went up because I have boobs now (by choice). He added that I was at risk of cervical cancer, as well. I tried to explain why that wasnt true, but he continued to insist he couldn't rule out the risk.
(I don't have a cervix 🙃)
I just hope this goes better.
Im going to ask about moving forward towards surgery.
3 notes
·
View notes
Note
I've been seeing the term diy hrt around, I've never heard of it before but I assume the name is self explanatory. Is it like where you make your own T or what? Is it cheaper than going through therapy and getting a diagnosis and prescription? Or is it something else entirely?If you have any resources on what it is exactly/how to safely start diy hrt could you answer with a short explanation or some links(preferebly within tumbler posts, I can't look anything up on this topic, otherwise I wouldn't have bothered you with this question).
Again sorry to bother you, hope you have a nice day.
Sincerely, a trans guy in serious need of HRT
Long answer, sorry…
DIY HRT is just a catch-all term for “not under supervision/guidance of a doctor”. The most well-known example of this is grey market estrogen bought online, but it can really look like anything. Using leftover patches of your friend, getting spare vials from a guy with a stockpile, buying HRT online… etc. Resources for trans guys who want to DIY are a bit harder to find because T has actual legal repercussions in most places.
In my case, I’m mostly taking the piss because a lot of people seem to think that if you take hormones without a doctor who has no fucking clue what they’re doing to shrug at you, you’ll fucking explode and die.
I’m a dual-citizen. In the States I have a prescription through Planned Parenthood, but where I actually live trans care is abysmal. We have a local group of transmascs who used to stock up abroad then distribute/sell T to the others who didn’t have a prescription. Nowadays though the T shortage in Europe isn’t as bad and our country isn’t as serious about restricting T, so I found a way to buy mine without a prescription.
Getting bloodwork privately and checking your own levels is pretty easy once you know what to ask for and know how to read your results. Big news: the labs don’t actually give a shit what the results say, they’re just going to give it to you. If a “woman” shows up and gets hormones tested and has male range T levels they’re not going to do jack shit about it because their job is just to test it and tell you. I’ve been doing my own bloodwork and adjusting my own dose based on my levels and how I feel for the last 2 years and I haven’t died horribly yet.
It’s not cheaper, unfortunately, because it’s all out of pocket. Insurance coverage would be really nice but I don’t want to risk having a transphobic doctor tell me what to do. (I wouldn’t listen)
The least blatantly illegal way I can think of DIYing is having a friend whose vials are prescribed single-use and sharing it. That way he’s not losing out, and you get to partake too. Where I live they sell ampoules, not vials, so you have to break them open to use them. Me and my best friend get together for shots sometimes to waste less by drawing up from the same ampoule, since we have to throw out whatever is left anyways. Nothing inherently dangerous about it as long as you’re all using sterile needles and syringes.
I have also seen cases where guys who suddenly switch to a different form of T (gel to injections or vice versa) and have some left over will give away their remainder to someone local.
If you’re in the States, I highly recommend trying Planned Parenthood or an informed consent clinic. I did my initial appointment over telehealth, signed some forms digitally, and had my prescription sent to the pharmacy of my choice the same day. It costed me like $170 without insurance. The prices vary regionally but you can try to ask for a price estimate if they offer gender services in your area.
If you lived in my city I would tell you to meet up with me in real and I’ll show you the pharmacy chain I go to and buy for you until you pass well enough to buy it yourself. Штета.
Dosing is easy. If you’re on cypionate or enthanate, those are weekly doses. You can start at 20-40mg a week and raise your dose little by little each week until you’re at a place you’re comfortable with or until you get the dose that works best for your body. It’s better to dose a little low than too high.
As for doing bloodwork? If private labs are easily accessible, ask for the following things: testosterone, estrogen (I do E2 estradiol), cholesterol, and hematocrit. Personally I get hormones, cholesterol, and a general blood test packet because it covers the rest. Make sure your hormones levels are in male range—look them up online if your results only show female ranges—and make sure your hematocrit and cholesterol aren’t getting too high either. Better to have slightly lower T levels and be healthy everywhere else than high T but also bad health elsewhere.
If money is an issue I get it. It’s not great for me either lol. I’ve had to delay my bloodwork for weeks because we get paid monthly and I didn’t have the $50 to spare for it, and I only just got a job that offers me any financial stability. Do what you can.
I’m sorry that I can’t give you resources on where exactly to acquire testosterone (and posting about them publicly risks getting them shut down, even if I did know) but I can advise you on how to care for yourself once you’ve gotten your hands on it.
6 notes
·
View notes
Note
Hi this is kind of invasive and you definitely don't gotta answer - I'm a trans guy ~2mo on T, and it's been great so far, already feel way better even with just my small changes. One thing I'm worried about is I've heard that once you're 10+ years on T, there are some unavoidable lower/reproductive system issues that can only be solved with surgery. Specifically painful cramping that requires a hysterectomy, and urinary urgency that requires bottom surgery with urethral lengthening. Was this your experience too? Can't really afford surgeries rn and if I can save for one, top surgery is way more urgent. I wouldn't mind getting hysto if I can afford it someday but I don't think I want bottom surgery; I do got bottom dysphoria but bottom growth is helping a ton. My doc did talk to me about atrophy and prescribing estrogen cream if I experience symptoms, but I heard that doesn't help with uterine issues at all, nor urinary urgency most of the time. I really don't wanna go off T ever if I can help it though lol, so I'm just wondering what other people's experiences were, if it was that big an issue, and how they dealt with it. Sorry for the wall of text and invasive question, thank you if you respond and hope you're having a good day either way
Hey glad things are going good for you dude! Since answers are medical and will involve certain medical terminology, I'll put that under the cut.
Honestly these are some tough questions to answer, because there hasn't been enough research conducted on trans men on T for 10+ years yet, at least not enough to be truly conclusive. I had an endocrinologist tell me that it was imperative that I get a total hysterectomy within 2 years because it was inevitable that I'd develop endometrial atrophy. Buck Angel (my opinions on him aside) often speaks of how he nearly died from atrophic complications. But I had another endocrinologist and ob/gyn tell me that there isn't really a lot of evidence that there's a particular timeline or even that it happens to everyone. When it does, it's typically gradual and very rarely severe enough to cause life-threatening problems. That doesn't mean it's to be taken lightly, but it also happens to some cis women who've had a total hysterectomy or are naturally producing less estrogen, especially later in life.
I had a hysterectomy just 3 weeks ago, after more than 10 years in HRT. The biopsy did reveal endometrial atrophy. I was not experiencing cramping or pain (actually, I had very severe pain and period issues before HRT, which went away entirely once I stared T) but sometimes penetration with toys caused some light bleeding. Estrogen cream can help with that, yes - but even post-hysterectomy, I'm producing natural lube down below so far. But with any medical intervention, there's risk involved.
For urinary urgency, yes lol, I do have to pee more often, but I also drink entirely too much coffee, so that may be a factor. I've never known any trans men who had surgery for urethral lengthening except as a part of bottom surgery (to reroute the urethra through their neophallus or bottom growth). Hysterectomies come with a risk of more urinary urgency and incontinence as well. There are pelvic floor exercises that are often recommended to prevent these problems, which I'll be doing once I'm a bit more healed up.
It's very good that you're prioritizing the surgery you most need, and not pursuing operations that you don't feel are vital for you. With costs, you may be able to get a hysterectomy covered by insurance, especially if you have any pre-existing issues like PCOS, endometriosis, or evidence of atrophy, so at least there may be financial options for you if you are one day in need of it - but there's no solid evidence that you will absolutely need to remove everything as a result of HRT, at least not that I know of yet.
14 notes
·
View notes
Note
What made you detransition or rather how did you realize you no longer identify as such? /gen
Well basically I went to a gender therapist per the recommendation of my regular therapist (who fully believed I was trans but she didn't feel comfortable prescribing HRT considering her lack of experience in the field). I had about 20 sessions with him and at one point after about 8 he said that based on the criteria for gender dysphoria he was prepared to write me a prescription for HRT but he wanted to know that I was comfortable with it. I realized I wasn't because giving up the possibility of having biological children hit me like a huge truck. I am aware that some trans men can get pregnant but it's not a sure thing for everyone and also the idea of being perceived as a pregnant man made me very uncomfortable (back then I would have said dysphoric, in reality I'm sure it was just the social stigma), more uncomfortable than the idea of being perceived as a pregnant woman. I am adopted and I have seen firsthand how hard it was for my mom to not have her own bio kids. She still feels sad about it even though I am enough for her. I had always planned on having kids and went through a phase when I was 15 or 16 where I was researching pregnancy in-depth. This should have been another sign I was cis lol.
Anyway so I told my gender therapist I wanted to wait and have a couple kids with a likeminded bisexual cis man or trans woman and then transition. We then spent several sessions talking about other things entirely. In my mind I still identified as a closeted trans man for another year or so but I only told my boyfriend at the time who was bi so he didn't care and I un-came out to my parents - told them it was just a phase and they were relieved. :(
While I was dating that guy, I had a huge crush on a different cis guy who was straight. With this straight guy I would fantasize about having a straight relationship and straight sex, and eventually I did start dating him but didn't really feel the desire to come out to him as trans. I felt weird about having come out to my old bf and I wished that I could just pretend to be a cis woman again to everyone I knew. At some point it occurred to me that while the obvious explanation for this is that trans identity is stigmatized, many trans people do feel relieved when they come out regardless, especially to people that are as supportive as my boyfriend and friends were. It instead occured to me that I wanted to present as a cis woman because I WAS a cis woman but I was still kind of throwing ideas around in my head, not sure what was going on.
Then I happened to go on the subreddit for OCD and they had a bunch of subreddits for specific obsessions listed in the sidebar. I didn't know what /r/tocd stood for so I checked it out and it turns out there is a pretty common subtype of OCD based on the persistent idea that you're trans despite no evidence for this or pre-existing desire to transition (I think the sub is /r/transOCD now). I read through a bunch of posts on there and it basically explained everything I had gone through in the past few years. It was an OCD-based intrusive thought like my old ideas about having to do every problem in the math textbook or having to wear purple to open my crown chakra. Unfortunately this one was spurred on by a bit of social pressure like those posts that are like, "If you even are thinking about being trans, that means you're trans, cis people don't think about this shit" and egg memes on Reddit. Obviously there is also social pressure to NOT be trans but when you've filtered your social circle so stringently that it doesn't include any bigots and therefore anyone who would pressure you to not be trans, the pressure to accept it if you're thinking about it can be stronger in reality.
Like I'm sure that a lot of people who wonder if they're trans are the real deal, a much higher number than the general population, but people with OCD should stay far away from ideas like "If you think about X you are X." OCD makes you fixate on completely random things that have nothing to do with reality, they're not necessarily things you're afraid of, just because you fixate on being trans doesn't mean you're afraid of trans people or dislike them - it just means it's something that your brain has decided to latch onto because it's stuck in a horrible anxiety loop. Maybe I was afraid of being a man in women's spaces and the anxiety that unconsciously provoked in them, or of never coming across as feminine enough, or of my hypersexuality meaning that I was some sort of failed woman. There may very well be a rational root of the obsession but unfortunately TERFs and other people skeptical of trans people existing at all will take that and spin it to be an explanation for everyone who identifies as FTM. I'm sure a lot of trans men had similar feelings to me growing up in a lot of areas but the difference is that they have male brains and I simply don't, they're happier being men socially and physically as much as possible and I am happy with the opposite. So I hope no one takes my personal experience out of its personal context. If you have any more questions feel free to ask and sorry for the novel :)
4 notes
·
View notes
Text
Since its disability pride month, and this happened recently, I thought I'd share about a doctor getting it right.
I finally got to see an endometriosis specialist last week, after having endo for nearly 30 years, and having all sorts of treatments for it.
I sat down with this doctor, and he flipped through my file, looked at a piece of paper, and flipped it face down. He said, "That's the letter your doctor sent referring you to me, and the" and here he paused. I knew on that letter it recommended an operation I had already told several doctors I didn't want, because I had been sent a copy.
"What do you want?" He asked, softly, and waited for me to find my words.
"I've tried everything else, I want a hysterectomy." I honestly sounded a bit desperate, a bit hysterical. And I was. I was fully expecting and prepared to have to fight for this.
"I'm a surgeon, I'm always happy to do surgery" he said. If that was what i wanted, that's what he would do. Then he went through all the risks, the hormonal treatment I would need and my options, and his recommendations. Never once did I feel like he was trying to dissuade me or patronised. He filled out the surgical consent there and then and warned me that there is a BMI cut off for a hysterectomy, and that while I wasn't there, my BMI was up. So while he doesn't reccomend I loose a lot of weight, or any at all if I didn't want to, making sure I come under the cut off on the day would be a good idea, because it wouldn't be fair to me to lose the surgery slot because of it.
When it came to the HRT I needed, and would need to start straight away, he offered me 2 options, a pill or a patch, and said they would usually reccomend the pill, but went through the advantages and disadvantages of them both. Then again he asked me "what do you want?"
When I picked the patch, he said he would write to my GP to prescribe it and asked if there was anything else I needed from him or any other questions I had. No quibbles, no judgement. It was what I chose, so it was what he would get for me.
I had my husband in the room with me the entire time, and other than when I brought him into the conversation this doctor didn't talk to him at all.
Having spent years with doctors condescending to me, disuading me or outright refusing me this operation, and asking my husbands opinion on it, this was like sunshine after a storm. I came home and cried, in relief. Not only am I getting the operation I need, I have a surgeon doing it that I genuinely trust, who let's "what do you want?" guide his care.
This is what good care looks like. And this is a massive win for me.
#endometriosis#endo#tw medical#tw surgery#tw hysterectomy#discussions of surgical and medical consent#good medical care#good doctor
0 notes
Text
Cw negative, transphobia
I really have no idea how to handle all of this right now - I was getting HRT through a nurse practitioner and now that’s against state law, I thought maybe they’d fight it bc they’re an lgbt clinic but apparently not. Which is really disappointing. I liked that practice a lot
I made an appointment with a new doctor they recommended but it’s not until June
I can’t get a refill of my HRT so I guess I’m just going to have to deal with my hormones freaking the fuck out until then
And that’s assuming it won’t be illegal for that doctor to prescribe it to me by the time I actually get to that appointment
I feel like I can’t even feel anymore, everything is just numb. I don’t know how to exist with this. and I don’t know what to do. I can’t even articulate how afraid I feel and I know I’m not alone but I feel so alone, and I feel like there’s no hope at all
I just want to go to work at a job I tolerate, I want to play dnd with my friends, I want to cuddle with my cat, without feeling like I’m in grave and immediate danger, but apparently that’s something unfathomable to fucking desantis bc he decided trans people were an acceptable minority to exterminate so he can win presidential primary votes
There’s no hope at all. I’m stuck and there’s no way out. I can’t afford to leave my job and go to a new state, let alone out of the country. I have no way out
1 note
·
View note
Note
so i have a friend who is a trans man, who was told by his doctor that they dont recommend him start testosterone because of his risk of high blood pressure. this has made him very upset, and i feel sad for him especially because i know start T for me made me so much happier and comfortable in my own body. i just wanted to know if you or any of your followers have any advice or if any of you have experienced this, and if theres anything i can potentially recommend him ask his doctor about. or if going on low dose or maybe only going on for a limited amount of time for permanent changes, than going off are options. thank you in advance to anyone who replies
Low-dose and temporary T are definitely options he should ask about, but I'd also maybe recommend he consider getting a second opinion or like... a new doctor altogether, even, at least to handle his trans-related healthcare.
T can raise your risk of high blood pressure, but that risk is no higher than it would be for a cis man with the same tendencies. If T is important to him and his mental health, there should be no reason he can't take some steps to take care of his blood pressure & mitigate that risk, and go on T.
It's not always a red flag if a doctor is unwilling to prescribe T because of things like the increased risk of high blood pressure and heart disease that cis men on the whole experience, and trans men & others experience if they choose to go on T. But it's something I personally am wary of, just because I have personally had much more trans-inclusive doctors and nurses (the nurse for my HRT scrip appointment was a trans man on T himself, even) and I feel like their take on those things is typically more along the lines of, "it's a risk, but a normal/expected one, and if you still want to go ahead with it there are ways to mitigate that risk."
Y'know, like how informed consent works.
Maybe your friend is a super extreme case or something, but like... again, probably worth a second opinion at least!
160 notes
·
View notes
Note
Okay so update, my parents are finnaly letting me go off my meds (not that they were helping anyway) so weight gain should be easier. My meds caused a slight loss in appetite (very small) but especially caused big anxiety and frequent panic attacks. It was especially unusual because I was at the lowest dose (18mg Concerta) so I'll see to pause the meds, then talk to the guy who prescribed me them, he's very nice and comprehensive, so we'll see to change the treatment, and keep off it the time I go back to 40, then 43-45kg (reasonable objective cuz we skinny in family)
Good news thought, my physical health didn't take that big of a toll as I thought, did some rock climbing and managed to pass one that I always got stuck on :D, I'm also getting a appointment for HRT (Should be the last one) so I hope that'll help with the weight too, as well as some muscle gain! (also holy fuck finnaly this took so long and so much bullshit doctors manipulating and gaslighting my parents before I got them to get an appointment to an actual endocrinologist that the nice doctor recommended them, and yes, one of them manipulated that guy too, like how fucked up is that, they manipulate each other now??)
So yeah I'm less panicky, but still, situation is awful and I fucking hate doctors, hope fate doesn't fuck me up once again!
-♠️
FUCK doctors, but im happy to hear you're doing a little better!! Sounds like you're working really hard to figure things out and have a bit of a plan which is awesome
9 notes
·
View notes
Text
Interlude: Let’s Kill This Fucking Clown
Hello, I am here to join @girlfriendsofthegalaxy’s Tuesday Again extended universe! lmfao
Click below to see this week’s song recommendation, fanfic recommendation, what I’m currently reading, and a life update!
•• ━━━━━ ••●•• ━━━━━ ••
February by Dar Williams
I meant to start doing these posts earlier in the month and rec this song then, but alas, I have clinical depression. Incidentally, so does this song. I love that I’m still not really sure what I think the analogy in this song is despite having listened to it relatively consistently for over ten years.
•• ━━━━━ ••●•• ━━━━━ ••
Eddie Kaspbrak, Office Uncle Extraordinaire by kyaticlikestea
Okay, so I read this a while ago despite having at the time only seen IT Chapter 1. This week I returned to it after at last seeing IT Chapter 2. It’s a Fix-It AU from an outsider POV and is incredibly funny and sweet. The serotonin is a-firin’. It “saves” Eddie by giving him the deadly wound from the original movie instead of the impaling as seen in 2019, so he’s an amputee!
•• ━━━━━ ••●•• ━━━━━ ••
Next Girl to Die by Dea Poirier
I’m not very far along in this book yet so I don’t have a lot of thoughts and I’m reserving my judgement. So far it seems really predictable, but sort of in a genre-expected way. It’s been years since I read something in first person so that is taking a lot of getting used to. I haven’t really connected with the POV character yet, but I’m also only 12% through the book. We’ll see.
•• ━━━━━ ••●•• ━━━━━ ••
I repeat, I have clinical depression.
Not much to say here. I have just woken up from finally sleeping after thirty-five hours away for literally no reason. But on the other hand, I bought some groceries and I might make some money tomorrow. I have decided on my bullet journal theme for March (Paleo art). I have the first appointment with a new PCP on Friday morning, who will - if fate should allow ::praying hands:: - prescribe HRT for me. Cross your fingers, light a candle, make a wish, and/or pray for me.
Here is a picture of Luna sleeping on my freshly laundered towels.

9 notes
·
View notes
Text
ITS MY BLOG AND I GET TO INFODUMP ABOUT MY CHARACTERS >:D
Disability and gender experience
CW for ptsd, panic attacks, su*c*de [I will talk about at the end if you still want to read this and will add another warning] , gender dysphoria, mild transpobia and abelism both internal and external
Disability
Lyla has osteoarthritis that is due to Burns' pretty fucky genes. She found this out when one evening they literally couldn't get out of bed for anything due to intense pain in the knees. Waylon had to come and get them and when he got there Lyla was pretty much on the brink of tears. Lyla then got a diagnosis. At first she was frustrated because it changed everything about his daily life. He was prescribed pain medication that dulls the pain to a manageable degree and was recommended to use a cane to get around during mild flare ups. It initially upset her. He thought she was too young to be going through something like that and hated having to limit how much they work. They later realized that stigma was ableist and bullshit and eventually sucked it up and decided to just embrace his new way of life and let her Grandfather help him learn how to cope due to experience with chronic pain [which means its lifelong] . On some days they get around just fine with pain meds but on bad flare up days they have to use a cane or chair to get around. She eventually mastered working with the aids and can even pop a sick wheelie on his chair. The pain still gets to them and it really sucks but he does swallow his pride and allow themselves to rest and be supported by others.
Sometimes with her partner Ashley he'll get snuggled and taken care of by her. Lyla is pretty dang light like his grandfather and Ashley has no problem carrying him around. Lyla secretly loves being carried. He's pretty fucking privileged to have Mr.Burns allow her disability support. Lyla is very privileged. Sometimes they like to make his cane/chair look cool with spray paint and whatnot. Very cripplepunk. Lyla probably found a disabled community of people his age to help her feel less alone.
Abbey has undiagnosed innatentive type adhd and ptsd that she gets full on panic attacks from. Neurodiversity was something taboo and not talked about in her childhood and didn't even realize she was struggling more than she should be. As a child she struggled paying attention to long boring sermons/lectures and was shamed alot for it. She didn't understand how she occasionally made people uncomfortable with very weird and unconventional topics she talks about. Loud sudden stimuli and intense buzzing overwhelms her and can make her cry. She didn't do very well in school and barely graduated high school. She prefered watching her favorite movies and playing dolls with her sister over studying. She's extremely sensitive to fabric and only has certain types of blankets and clothes that she can stand. She absolutely hates the feeling of fabric draping against her legs too much so sometimes she either wears tight-ish pants and avoids skirts/dresses. She hates sitting and walking in dresses. She never wanted to wear them lol they feel bad to her. She refuses to sit up straight and will cross her legs. Abbey hyperfixates on animation, cinema, and dollhouses. She likes binging movies and making doll projects. She tends to bond with people through movies and model making. She struggled to make friends outside of her circle and just stayed friends with people she grew up with at her church. They all escaped that mormon hell. Abbey struggles with her emotions and usually gets overwhelmed too much which can often leave her drained and tired. She has an intense oral fixation and uses stim necklaces to chew on, before she would chew on her sleeves, pen caps, pens, her hair, her shirt, her sleeves, bottle caps, ect. She was a very curious kid and tried to eat playdough, dirt and grass lol. None of them where good. She is decent at working at the video store and feels happy with her job being related to her interests. Because hrt therapy is so expensive she doesn't feel she can afford any kind of therapy or medication and it's very overwhelming for her to have to prioritize one aspect of her health over another. But with financial support from close friends and her boyfriend Tim she gets by ok.
Gender
Lyla assumed that it was completely normal to have a fuzzy fluid gender due to believing gender is a lose concept for most people. He didn't realize most people have static genders that don't change at all. It wasn't something they never questioned. Later in Lyla's 20s they started to learn more on gender and realized she wasn't as cis as he thought they where. The term genderfluid fit his experiences perfectly. They never felt still in their gender. Even if they felt more towards one gender over another it wasn't a firm feeling. It felt fluid and lose. As a teen they dressed in goth fashion and was a self proclaimed tomboy. But they realized tomboys or most gnc women didn't dress up very feminine on somedays or even wear dresses. She loves wearing dresses and she loves wearing lose jeans and a lose men's tee.
Lyla's gender tends to shift weekly but it may present or change depending on who they're with or what media/environment they're exposed too. For example he might feel more feminine with certain friends and more masculine with strangers. Sometimes they feel more comfortable being agender or a nonbinary genders with certain people such as their partner. Sometimes they only use certain pronouns with certain people. He/she/they at work, she/he with parents, she/he/they/it with siblings, she/he with some friends, and she/he/moths/rots, rats, its with their partner. Lyla will either tell people upfront on pronouns for the week or use a pin.
Most of the time clothes don't dictate their gender that week but there are some key differences. Lyla will not wear dresses on more masculine days and may draw on facial hair with a mascara brush. On more feminine days they dress more like a nature witch and loves floral stuff. They are more likely to have fun with makeup on those days.
Lyla doesn't want to undergo any kind of surgery or hormone therapy. Lyla may bind a bit with a sports bra but doesn't really feel uncomfortable with his chest and mostly doesn't mind having visibile tits on masc days.
Abbey always felt different from her birth sex and felt very frustrated learning she wouldn't just naturally grow into the chest and genitals she wants growing up. It was an extremely taboo and forbidden subject but despite that something inside her soul knew she was a girl. Her parents pushed very strict gender roles on her growing up and causes her to struggle with her femininity as an infertile woman who could not stand dresses. It made her feel a bit lost but she later felt better knowing other women cis and trans who don't conform to gender roles.
Abbey gets intense physical dysphoria from her crotch and for a long time she had to just deal with it until surgery was an option. Some days she could tolerate it but some days [especially when she got on estrogen and felt very hormonal] it was unbearable and a wet dream or boner would trigger a depressive episode that consists of cacooning a cover, watching her favorite movies and long naps. It was a toll on her mental health that was already pretty bad. But emotional support, understanding and patience from her friends and boyfriend helped her carry on though it. She eventually does get bottom surgery and it's a HUGE weight off her chest.
Abbey usually dresses in sweatshirts, graphic tees and cute jeans. Whatever's comfortable on the skin. She wore tank tops more when her tits grew in. And they grew in pretty dang fast and big and ah it hurt. She's a c cup which she loves but God they where tender for awhile. Double puberty isn't fun. Her transition was a bit rough and long being low middle class but she pulled through.
TW for su*cide. Leave the post now if this triggers you.
Abbey is a suicide attempt survivor. She suffers ptsd from her own husband taking his life leaving her a widow. She felt trapped and tired in her unbalanced emotions and uncertainty of ever feeling okay or getting the medical attention she needed and attempted to OD. Fortunately she was with Timothy who immediately called an ambulance. She was very tired and at first a bit disappointed she was still alive but also a bit relieved. She then had to cope with feeling suicidal.
2 notes
·
View notes
Note
So, I want to take T but the problem is it increases blood pressure. I have a history of hypertension in my family. Three who have had strokes from it, one actually died from that stroke (albeit elderly with other issues). I'm really worried but my doctor doesn't seem to understand. He just wants to prescribe to me and check my T levels with no regard to blood pressure. Apparently he "doesn't do" blood pressure and if I have a problem with that see another doctor.
it’s good to have a primary care doctor anyway, especially if you have a family history of health problems (regardless of whether or not you choose to go on T). The best science we have is that we offer HRT because it’s a lifesaving med- and while we caution about the possible side effects, we don’t baseline withhold it on the basis of other health conditions (or potential conditions) overall- we treat you the same way we would treat other folks with high blood pressure: with the typical exercise, diet and possibly medication regimen, depending on how high it is. (the same goes toward trans women who are high risk for blood clots by the way, or trans men at risk for diabetes). You can do things now to help reduce your risk for high blood pressure. These are the American heart association diet and lifestyle recommendations that help reduce blood pressure (and heart disease risk) and are the best science we have about this. If you do end up with high blood pressure, it’s also the first thing your doctor will recommend you to do, (if you’re not already doing it) unless it’s unsafely high- then you’ll go right on meds. It’s not too uncommon to have providers that are specialized in one type of thing (like hormones) and not too interested in managing other chronic health conditions like high blood pressure.
mod mayhem
21 notes
·
View notes
Photo

Inktober 2019 - day 16
Self portrait, because it was an important day.
Had my first appointment with the gender doctor!!
It wouldn’t have happened (or certainly not so quickly) without your contributions and support. Thank you so much. You guys are a blessing and I never expected so much help!
It means now I can finally do my *first transition update*
My hair was a bit more presentable than pictured above when I got to the touristy heart of London and sat in the (surprisingly posh, my mind of a poor art graduate was blown) waiting room to have my first consultation. If you wanna know which doctor did I go to or know more, please drop me a message; I just somehow don’t feel comfortable operating with names of respected medical professionals so openly on my fanart blog.
I don’t think I need to describe how nervous I was - today had a potential to either be the best day of my life (in unlikely circumstances of getting hormones prescribed there and then) or at least a step towards a better life, finally.
It was both slightly difficult and very relieving, that meeting. Mostly her trying to get to know me, asking loads of general questions rather than doing a dry box ticking exercise that I expected in that situation. Taking her time.
I was surprised when she mentioned she had concerns about me reaching out to her for testosterone and not making the top surgery my first step, seeing that I identified as non-binary (the exact opposite of how the public gender clinic approaches the situation!) - and that she had not had good outcomes who took that route. I think it got clarified when I mentioned that a desire to have a surgery first was the original reason why I contacted the GIC (Gender Identity Clinic - the public one) two years ago, and while waiting to be seen by them (as I ranted before, it currently takes 2 years to get to a first assessment) I realised that there were other things that affect how I feel about myself on a daily basis- such as my voice, the fact that I do not pass if I wear anything remotely feminine etc - I basically decided that I did in fact need hormones, and it would be a long route to even get a smell of it through the strained National Health Services.
It is worth mentioning that she is respectful of the non-binary identity and attempt not to make it more difficult (the GIC do, apparently?), however - how I understood it at least - she tried to exercise pushing me into binary for the sake of finding out whether hormones are what I really want, because of course taking it wouldn’t really leave me ‘in between’ and whether we want it or not, people do immediately categorise us as male or female. Her take was that being on testosterone, after certain point at least, would push me the other side, so she wanted to find out whether I would for instance be comfortable if people suddenly started calling me ‘he’. I of course exclaimed something along the lines of ‘hell yes??? i would be comfortable, please may I be a he???’, but I understand the concern. It wasn’t in a ‘you briefly mentioned you could describe your gender as enby, I will now deny you HRT’ way, not at all. It felt more profound and caring.
One thing that made me very nervous is the fact that she wanted me to change my name by deed poll. Now, I would have done it long time ago had I known it was legal for me to do! But I am not a British citizen yet, so changing my name and all British documents would result in a conflict with my Polish passport. Which I wish I could change, but as there’s no other way to have your sex reassigned in Poland but by taking your own parents to court (which in my case also requires a lawyer to represent my deceased father whom I never met) over mistakenly assigning you the wrong sex at birth or however else should I formulate this bullshit of a law - I can’t do it just right now. Yes, you don’t just go there and tell them you’re trans - you sue your own parents, despite being a grown up - and technically parents could make it difficult fot you. I don’t think I’m strong enough or have enough money to fly back and forth to a hostile country that treated me so badly just to follow this process. But if I do change my name in the UK now, this will have to be done asap. And the doctor, who said she’s advised that to multiple foreigners living here - says it will actually be required by the GIC as an important milestone in living in a desired gender role (screw that, I’ve been living in one for years, I just wanna be legal and use my passport, and Brexit is coming!!!)
Meanwhile, after 22 months of a wait about which I rambled multiple times, the GIC suddenly texted (!) me on Friday asking me to contact them asap cuz they might have a short notice appointment for me. I was at work til late, so I called them on Monday morning, just to discovered that the slot had been snatched. I was not particularly surprised by it. But then I got another call in the afternoon informing me that they had one more appointment available, but it was going to be this Thursday. That is, in a few hours from the moment I am writing it. I am shocked that I will finally be seen - surely no chance for hormones/surgery recommendation right now, and the next appointment won’t be in a year knowing how things work, but at least something!
So that’s it - congratulations if you’ve gotten to the end of it! I hope things progress soon; I am nervous AF but at least the ball is rolling now.
I still do accept any donations from kind ppl who wish to buy me a virtual coffee - there’s a secret drawing of Aziraphale in the updates section that should be revealed upon making a contribution! Again, thanks to all of you who made things possible so I had something to write this long post about!!
and as always thanks to my dearest @mimimarilynart who is always here for me and somehow hasn’t died from listening to my rants yet. Thank you for being so supportive all the time <3
#transition update#inktober 2019#inktober#self portrait#personal#rl#my illustrations#doodles#transgender#transitioning in the uk#art#digital colouring#non fandom#toastedbuckwheat
77 notes
·
View notes
Note
when you start hormone therapy how do they base how much T to give you?
It all depends on your genetics and pre HRT hormone levels! You already have testosterone in your system, every single person alive does, and what hormone therapy does is safely and slowly bring those levels up to the appropriate & "standard" male levels so that your body can react and cycle through its injection properly.
Every starting dose should be very low. Mine was a .5ML of a brand I can't remember the name of rn but I'll edit this post when I find an old bottle, but other starting doses can even be a .25ML or .75 or even a full 1ML (which is honestly too high, but if your doctor prescribes it, they prescribe it)
When I started my doctor did absolutely not explain the injection process to me properly so I was injecting .5ML into my thigh every TWO weeks (when it should have been every week) and so the first 2 months of my transition I had absolutely no changes besides very little ****** growth and I was mad. When I had my 2 month check in he said I was supposed to be doing .5ML in my BUTT every 2 weeks or .5 every week in my thigh because my levels were basically going like this:

Instead of this:

You need to start on a low dose so your body becomes acclimated to it. If your initial dose is a FULL ml of testosterone, that's more than likely a problem (unless you already have naturally very high testosterone levels) because your body will convert it back into estrogen. This is a hormone you are injecting into your body and your genetic makeup will be shocked. Please do not be dissuaded if your doctor gives you an incredibly low dose, or what appears to be a low dose to you. It is only for your own health. Just make sure you clarify with your doctor on METHOD of injection or you might run into the same issue I did, with very unstable hormone levels.
The difference between injection in the butt/hips/stomach and injection in the thigh/arm (do not recommend arm) is that butt (etc) is something called SUBQ - subcutaneous injection, and the thigh is IM - intramuscular injection. Subq is when the testosterone makes a pocket inside of your fat, and distributes it very slowly inside a time frame of around 2 weeks (hence why when I was doing .5 in my thigh, my levels immediately went back down to the pre t normal because there was essentially AN ENTIRE WEEK I had no control over my hormones and they just reconverted to estrogen; had I been doing the injections every 2 weeks in my butt, I would have been better off because of the fat it would have been stabilized in). IM injections is when the testosterone exercises through your muscles, so your body works through it MUCH faster, hence why most IM shots are weekly.
A low dose is the normal, you will eventually work your way up to a high or "level" one ❤️
I currently am at .5ML weekly subq injections in my stomach fat because it's the only way I am comfortable doing my shots anymore, but I used to do a full 1ML IM in my thigh before I built up too much scar tissue. The new brand of testosterone I'm taking is twice the strength of the old brand I took so I push my shots to about every 10 days instead of 7 at my own discretion.
5 notes
·
View notes
Text
I'm sure lots of people have talked about this already, but I think it's really shady the way only parts of transition healthcare are ever covered by so many insurance providers. I'm talking both public and private here.
I want to be very clear about the fact that I'm arguing we add any additional roadblocks or gatekeeping to transition care. All I want to argue for here is that more options be available.
In Ontario, I was able to access HRT through an informed consent process, which means I proved to my doctor that I understood the limitations, side effects, and risks associated with estrodial and cyproterone, the meds I take.
I was lucky, this wasn't my GP's first time with this, so he knew what to do, I didn't have to educate him on the basics of it. He has his limitations, and eventually I want to see an endocrinologist about progesterone, and long term management of my hormones, especially post bottom surgery.
In lots of places, it's way harder to access even HRT. In the UK for example, my understanding is that you need to see a specialist, and GPs are generally unwilling to prescribe HRT even in the interim before seeing a specialist.
As far as I know, the UK is the only publicly funded health care system that covers gamete preservation for trans people, though it's not a part of the system I hear much about. Obviously the UK system has lots of issues, but on paper it sounds like it should be the best one to be trans in.
OHIP (Ontario's system) won't cover HRT for lots (most?) people, because OHIP doesn't really cover medication for anyone from 26-64(?). It does allow your doctor to prescribe you hormones, which was a big win. It also allows bottom and top surgery to be covered, but each has to be approved individually, according to the page listing the requirements.
The fact that top surgery to remove breast tissue has to be approved, but breast reduction is covered automatically, and all you have to say is that it prevents you from living the life you want (essentially, there's a specific wording, but any good surgeon will coach you during a consult, as my friend learned).
I don't want this to read as me thinking we should add gatekeeping to breast reduction, I just want to call out the double standard here.
Meanwhile, all of the trans affirming surgeries require 2 seperate assessments, by 2 health care providers, stating you have a diagnosis of persistent gender dysphoria. They also have that classic requirement: "have completed 12 continuous months of hormone therapy (unless hormones are not recommended) you have lived 12 continuous months in the gender role you identify with (for genital surgery only)."
These are a big improvement, for Ontario at least, over what they used to be. We used to be required to see a psychologist, which meant a 6+ month wait list just to get an initial assessment, followed by probably several appointments, hen being sent back to your GP before finally getting a referral to a (the, at the time) surgeon.
Under current requirements, I could probably see my doctor, and then a nurse practitioner with his office and get my surgery approval submitted in less than a month. Of course, that doesn't mean I'd be seeing a surgeon all that quickly, especially right now.
I'm supposed to talk to my doctor on Tuesday about getting this process started, so that's exciting, if a little terrifying, it feels like the biggest step in my transition so far.
I'm kind of rambling here, the thing I really wanted to talk about was what isn't covered.
There's no support for gamete saving, which kind of amounts to a form of mass coerced sterilisation, since many of us can't afford to save our gametes on our own, especially before we even start transition, and we know the hormones will probably make us infertile as long as we're on them. I know for me, I don't think I could tolerate the 3+ months off hormones required to produce viable gametes again.
I probably could have waited a couple more to start if I'd been trying to save gametes then, but there was no way I could afford it on my own, and I'd be wanting to start them for months at that point, and only waited until I came out to my family. I'm personally not that upset about never having children from my own gametes, it doesn't bother me that much, it's not being able to carry them that hurts more. But my personal feelings about this don't mean that I shouldn't have had the option??
The other thing that isn't covered, which really bothers me, is facial surgery. I know that masculising face surgery is in a very different place than feminising face surgery, but I'm going to speak from the perspective of a trans gal that wants FFS, I can't speak to wanting FMS, trans masc folks who know more than me feel free to comment, or link to other people talking about it. I don't think it's exactly my place to talk about it, and I really just don't know very much anyways.
Bottom surgery being covered is so incredibly important to so many of us, but the idea that bottom surgery should be covered, but face surgery shouldn't is wild to me? Ultimately, they're both somewhat cosmetic, but you know what else is? Brushing your teeth. Bad tooth health will eventually ruin your life, and so will dysphoria, so why can't we cover a surgery that would deal with a major source of dysphoria?
FFS procedures are not especially new or experimental, lots of cis women have some of these procedures as well. From a safety-via-passing perspective, FFS is probably more important than bottom surgery for at least some trans women.
I don't mean to say that we should all have it, or that anyone's priorities are wrong, personally even if both were free, I would still get bottom surgery first. I also don't want to imply that passing should be a goal, requirement, or something everyone, or even anyone should strive for. But, it's sometimes useful to frame things for the cis people that still get to make these decisions about our bodies, to be able to understand why it matters to us when it does.
In an ideal world, trans kids won't be forced to go through the wrong puberty, and hopefully some of these surgeries will be less and less necessary, but I don't think we'll be there for a while, and even if we get there, there will probably always be adults who realise their transness long after puberty.
#text#mine#paislee talks about trans stuff#trans affirming healthcare#trans surgery#facial feminisation surgery#bottom surgery#top surgery
1 note
·
View note
Last Seen Blogs

parkore
EXTRA SUGAR EXTRA SALT


stonedavengers
Mary Jane

thc-chaoz-tric
CHAOS!!!

mirkomedri
TUDO BEM?TUDO BOM!