#gender transformation surgery
Text

Day 5!, when you can finally fill out your fav blouse without stuffing a bra! I'm so happy right now. They are the perfect size for me!
For those of you who have been asking. I got 470cc implants. No big but not small. I wanted a natural size proportionate to my body. I gave my surgeon a ton of leeway on that. He went 55cc more than I thought I wanted. I feel he picked a perfect size for me! I couldn't be happier 🥰🥰🥰
#trans surgery#transgender surgery#gender affirming surgery#transgender#trans#transisbeautiful#trans pride#transgirl#mtf hrt#mtf#girlslikeus#maletofemale#transformation#mtf hormones#trans mtf#actually mtf#mtf positivity#transwomen#transition#actually trans#mtf trans#trans feminine#trans girl#trans is beautiful#this is what trans looks like#trans is sexy#trans positivity#tgirls are better#tgirlsdoitbetter🌈#cute tgirl
623 notes
·
View notes
Text
Breakdown and Bulkhead being exes and there being so many emotions about that
Especially with me remembering the semicommon hc that Breakdown used to be an autobot, which considering how he's often a stunticon and the stunticons are in rid15 gives me the crack idea of
At the beginning of the war Breakdown left the stunticons to join the autobots because of his boyfriend at the time and him disagreeing with Motormaster, leading to MM saying he won't under any circumstances take BD back if shit with Bulk and the bots goes sideways
Shit with Bulkhead and the autobots goes sideways as Breakdown grows increasingly dissatisfied with his role in the autobots, leading to him breaking up with Bulkhead and him joining the Decepticons like he was "supposed to" in the beginning of this scrap
Well. Now he's an ex-autobot in the Decepticons and again the stunticons kept to their word as he burned that bridge, leaving him a tidge of a mess.
Enter Knockout, who's looking to take on an assistant with at least SOME medical experience. Breakdown fills this requirement because i say so and because i love nurse/medic!Breakdown. Breaky says yes because fr what the pits else is he supposed to do.
After a rough adjustment period, they grow close and the more familiar power couple KOBD we recognize and love ensues
In his wiki page tfwiki suggests that in aligned Breaky used to be a scout, actually, who was real super anxious before getting a frame upgrade in order to keep up his grudge with Bulkhead and this did wonders for his mental health from what i can see. This may be another reason why Breaky seeked Knockout out
THERE WE GO, TFP BREAKDOWN: AN EX-STUNTICON, EX-AUTOBOT, UNEXPECTED MEDIC, CURRENTLY KNOCKOUT'S PARTNER IN CRIME AND MOTHERFUCKER WITH A HAMMER
#maccadam#transformers#a bullshitted up mix of canon_ fanon_ and situations where you remember it's a continuity family rather than a single continuity#Breakdown deserves more love. ik he already gets a lot but like. more please.#breakbulk#kobd#tfp breakdown#tfp bulkhead#tfp knockout#knockout was glad to oversee his fiancé's gender affirming surgery (/hj) go well#unusual metaphors for dysphoria GO#how funny would it be if they actually do have the equivalent of courting rings but they keep them safe in their quarters#i saw the idea of courting rings being made out of a literal piece of their partner's plating and the symbolism is insaneeee#i love the idea of Cybertronian courting gifts and rituals that get practiced in a variety of ways or even not at all#some of this may be nonsense
58 notes
·
View notes
Text
I JUST SCHEDULED TOP SURGERY!!! Jan 3!! I’m so amped. Just needed to share. What a great way to start a new year. 😭😭

((If you want to help w my top surgery fund my venmo is @luckysparks and my cashapp is $misscobblebottoms, no pressures though & interacting helps too!))
#ftm#tboi#nonbinary#non binary#transgender#transmasc#transformers#top surgery#gender#gender affirming care#gender affirming healthcare#gender affirming surgery#fundraising#healthcare#celebration#happy news#bye bye#dolly parton#tatas#bodacious tatas#hospital#lgbtqia#lgbtq community#lgbt pride#lgbtq#lgbtqplus#lgbtqiia+#lgbtq positivity#queer pride#trans pride
31 notes
·
View notes
Text
Transformation - Agent Girlfriend
Here's a line art commission for Jet.
A hitman takes on a job with… special requirements. He goes under the knife to transform into a copy of his target's girlfriend.
Feel free to check out the full resolution version on my Patreon!
www.patreon.com/retrosqueeze
#tsf art#tsf#genderbend#gender bender#gender bent#genderbender#transformation#mtf#m2f#surgical transformation#surgical#plastic surgery#disguise#hitman#secret agent#disguised#undercover#transgender
20 notes
·
View notes
Text

People on here are always talking about Tzimisce fleshcrafters as Vampire Gender Affirming Surgeons but no one ever once mentioned to me that that’s explicitly a canon Thing Thin-Blood Alchemists Can Do??
#it is explicitly stated to create a permanent change even in vampire recipients#and that it has no efffect on the Nosferatu clan bane#rather incorporating a Nos’s Bane into the transformation regardless of their mental image of themselves#and calls out that it does not do non human elements in the transformation#it seems almost explicitly to me to be Potion Of Gender Confirmation Surgery#reading thru the Thin Blood Alchemy section has me like ‘shit maybe I want to try out playing a Thin Blood next’#vtm v5#vampire the masquerade
17 notes
·
View notes
Text
WAKE UP PEOPLE LOOK WHAT I’VE MADE



TRANS ICONS IF YA ASK ME 😩👌
(In this picture I used the Transmasc flag)
#tfp#transformers prime#tfp optimus prime#tfp ultra Magnus#tfp wheeljack#transmasc#icons#pfp#for some reason I feel like this fits them#the bots learn about LGBT+ Q and find out the meaning to which they fit the most with#their holoforms have top surgery scars#because I said so#I know transformers don’t specifically have gender#and they just choose whatever gender they want (I’m very jealous)#but I feel like this is what they would be#or Transgender#either way their valid ❤️❤️❤️#transgender#lgbtq
56 notes
·
View notes
Text
Vulvoplasty Research Notes
PLEASE NOTE THAT THE RESEARCH NOTES ARE COLLECTED FOR FUTURE OPPERATION AND UNDERSTANDING OF WHAT TO EXPECT BEFORE/DURING/AFTER VULVOPLASTY AT OHSU.
PLEASE NOTE THAT THIS INFORMATION CAN BE ANXIEY-INDUCING TO SOME.
-----------------------------------------------------------------------------------------------------------
WHAT IS VULVOPLASTY?
A vulvoplasty is a gender affirming genital reconstruction surgery that creates a neo-vulva from the existing genitalia. It fashions the external female genitalia but without a vaginal cavity. Depending on a few factors, this kind of surgery can have many different names, but in essence they are all the same:
Vulvoplasty
Vaginoplasty Without Cavity
Shallow / Minimal-Depth / Dimple / Limit-Depth Vaginoplasty
Cosmetic / Aesthetic Vaginoplasty
No-Depth / Zero Depth Vaginoplasty
Personally, I tend to call vulvoplasty - vaginoplasty, as my personal goal is to transition as much into a female without the addition of a uterus and ovaries (as the science hasn’t been developed to add these to the male body at this time). Calling it a vagina is logical in my mind as it affirms my gender as female. Also, most cis-females label their own reproductive organ as a ‘vagina’, including the clitoris and labia into the structure.
The outer characteristics of vulvoplasty are the same as those of vaginoplasty.
A clitoris and inner and outer labia are created, and the testicles and biological male sexual characteristics are removed and discarded.
The difference between a vulvoplasty and vaginoplasty is that a vulvoplasty provides a vaginal entrance that is up to 0 to 2 inches deep (depending on avaiable skin); whereas a vaginoplasty is usually 4-6 inches deep.
A benefit of vulvoplasty include:
1) Shorter Surgery Time (1.5 - 3 hours)
2) Shorter Inpatient Time (1 - 3 days)
3) Shorter Recovery Time (6-8 weeks)
4) No Need For Laser Hair Removal
5) No Dilation
6) Less Chance For Rectal Injury
Those seeking vulvoplasty should be aware that with no real depth, you will not be able to have penetrative sex.
-----------------------------------------------------------------------------------------------------------
HOW A VULVOPLASTY CREATES ‘TRUE’ FEMALE PARTS
This might be something that most people do not consider at first; but your new female parts will be actually true female parts (minus the uterus & ovaries). This is because all life on Earth in its earliest development begins as female.
This is why a vulvoplasty can be performed on a biological male; and why men have nipples on their chests and estrogen in their blood.
When a baby develops, the genitals are all the same; a urogenital slit bounded by periurethral folds and more laterally by labioscrotal swellings. It is only when the male chromosome activates, it causes the genitalia to develop differently. However, every masculine part to be traced to a feminine part. Dihydrotestosterone stimulates growth of the urogenital tubercle and induces fusion of the urethral folds and labial fold swelling during this critical period; it also induces differentiation of the prostate and inhibits growth of the vesicle vaginal septum, thereby preventing the development of the vagina
For example, the structure of the penis and clitoris are pretty much the same. It is an organ designed primarily to promote pleasure and reproduction. Both organs contain a nub or head that is packed with nerves.
The skin from the penis is used to form the area around the clitoris called the ‘hood’. Much of the shaft in a male is external, whereas a female contains the majority of her clitoris structure inside her body. Try to imagine anatomically that the inner labia are made of the penis’s ‘stretched’ skin, forming the foreskin at the end.
Scrotal skin contains a suture line down the center that once was the opening to the outer labia. The vaginal pouch is usually obliterated when the müllerian ducts are reabsorbed, although a vestigial blind vaginal pouch known as the prostatic utricle can sometimes be demonstrated. The prostate gland and the urethral glands of Cowper in the male are outgrowths of the urogenital sinus, in which male differentiation is mediated by dihydrotestosterone and requires the presence of androgen receptors
-----------------------------------------------------------------------------------------------------------
THE PREP / PRE-OP
Both vulvoplasty and vaginoplasty are major surgeries that are usually the last surgeries that MTF individuals have within 2-3 years on HRT.
Be aware of the following:
1) Persistent, well documented gender dysphoria diagnosis.
2) Capacity to make a fully informed decision and to consent for treatment.
3) 12 continuous months of hormone therapy
4) 12 continuous months of living in a gender role that is congruent with their gender identity.
5) Two letters from mental health therapist.
6) Nicotine Free for 10 weeks.
7) Documentation of recent A1C < 6.5% (diabetic patients only)
Pre-Surgery
At OHSU, it is scheduled to have a pre-surgery appointment one month before surgery. At this appointment, you will meet the Physician Assistant and be able to ask any questions before surgery.
You might be tested for nicotine and have blood work. A nicotine test will be performed on the day of surgery.
Stop taking estrogen 4 weeks before surgery. This is to reduce the risk of blood clots. Estrogen can be resumed a week after surgery.
Your surgical team might consist of the following people:
Primary Surgeon
Secondary Surgeon
A PA (physician assistant) Or RN
Medical assistants
Surgery scheduler
Resident physician’s
Physical therapists
Behavioral therapists
Social workers
Inpatient RN & CNA
-----------------------------------------------------------------------------------------------------------
SUPPLIES SUGGESTED
Roll fluff gauze: for surgical site absorption. Having 8-10 rolls be best.
Donut pillow or Hemorrihoid pillow for sitting: this will be important as it is almost a 4-hour drive. You can also use a u-shaped neck pillow or gel seat.
Maxi pads: to help with drainage. Larger is better as you don’t want it too tight.
Lots of toilet paper: You are likely to get messy.
Extra pairs of loose or mesh underwear: With dressing and maxi pads, your regular underwear may be too tight. You also may have some drainage that might ruin your underwear.
Stool softeners: Opioid pain medication and inactivity will likely cause some constipation. Miralax is recommended.
Ice pack: To reduce swelling, inflammation and pain.
Peri bottle: For the first few weeks after surgery, you should shower twice daily with gentle soap and water. Use your hand rather than a washcloth to clean the surgical site. Some patients find a peri bottle, designed for postpartem mothers, to be a gentle way to clean the area after surgery, in addition to showering twice daily.
Items to keep you entertained: computer, books, games, ect.
Snacks: to help ease emotional pain and use as a treat.
Items that make you comfortable: like a blanket, pillow, aromatherapy, eye pillow, ect.
Sore throat remedies: tea, chocolate, medicated spray. The trachea tube can leave behind irritation.
-----------------------------------------------------------------------------------------------------------
THE SURGERY
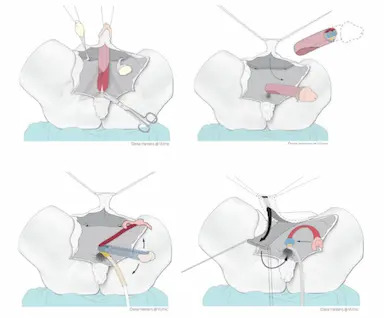
In vulvoplasty, the female genitals are created from the skin and underlying tissue of the penis. No vaginal cavity will be created. In most cases, the testicles are also removed in this operation. Be certain that you have thought about family planning before surgery.
Depending on the technique used, the operation will last anywhere from 2 to 5 hours. The operation will be performed by a plastic surgeon and/or urologist surgeon.
It starts with the insertion of a urinary catheter in the urethra.
The penile skin is removed from the shaft of the penis. The skin is shortened and sutured in order to make it look like a vagina (but without the vaginal cavity).
Then the testicles are removed, and the clitoris and inner labia are made from the glans and the foreskin. The urethra is exposed and shortened up to the new entrance.
The parts of the male genitals that will be incorporated into your new neo-vagina:
Clitoris is made out of the glans of the penis.
The outer labia are made from the scrotum.
The inner labia are made from the skin on the penis and/or urethra.
Urethra shortened and repositioned between the clitoris and vagina.
Introitus (opening of the vagina) is formed from the skin of the penis.
-----------------------------------------------------------------------------------------------------------
IMMEDIATE AFTER SURGERY & DAY 1
In accordance to OHSU Day 1 in Hospital:
After Surgery
Dr. Dy will speak with family after the surgery. Patient will be in post-anesthesia care unit for 2-3 hours for observation. It isn’t uncommon to feel nauseated (I tend to vomit after anesthesia), groggy, irritated, tearful, hungry and especially thirsty for a sore throat.
Patient will then be moved to Unit 4A (surgical unit). You will have a foley catheter in urethra, surgical packing, and drains with a collection bag. Your legs will have compression cuffs and an IV will be placed in the arm.
Medicine offered: nausea med, sore throat med, narcotic pain med, and stool softeners.
Diet: Begin with ice for sore throat. Water can be consumed in PACU. Snacks will be offered, like crackers or pudding, before the regular meal on day 2. Yogurt is advised.
Day 1
There is no strict bed rest, move as much as tolerated.
Rolling over in bed is comfortable if you do a ‘log-roll’. The bed should remain at 45 degrees or less.
Medicine Regiment: 650mg Tylenol every 6hrs. 15mg of Toradol IV every 8hrs. 5-15mg Oxycodone every 4hrs. Miralax.
No bathing, you can sponge bathe.
-----------------------------------------------------------------------------------------------------------
DAY 2
Medicine Regiment: 650mg Tylenol every 6hrs. 600mg Ibuprofen every 8hrs. 5-15mg Oxycodone every 4hrs. Miralax.
Encouraged to move around as much as possible. This will help with blood clots, maintaining your muscles, and digestion. Physical therapy suggests you do bed exercises every hour while awake.
Many patients will leave the hospital inpatient floor and go home on Day 2 with a catheter and external dressing in place. These dressings will be removed in the clinic on Day 3 or 4.
-----------------------------------------------------------------------------------------------------------
DAY 3
Medicine Regiment: 650mg Tylenol every 6hrs. 600mg Ibuprofen every 8hrs. 5-15mg Oxycodone every 4hrs. Miralax.
Today, the pressure dressing on the vulva is to be removed. Drains may be taken out today or tomorrow. Foley catheter removed. You need to try to pee without the catheter. 1-5 people find they cannot pee due to swelling, so a catheter will be placed back in. Your bladder will be scanned to see how much urine is left.
Take a shower today. User warm water, not hot! Clean ‘carefully’ all the folds and creases between your legs. Do not scrub! Do not use washcloth here!
Let the water flow over your vulva to wash away soap. Do not rub towel when drying...pat dry if possible.
Prepare for Discharge!
You and the caregivers should ask questions about anything not understood. Caregivers will pick up prescriptions before the patient leaves. Be certain to know the date of the next follow-up visit.
Transfer to the Rood Pavilion for extended stay.
-----------------------------------------------------------------------------------------------------------
RECOVERY AT ROOD
Not all hospitals offer off-campus housing, so your experience might differ. I live out of state, almost 200 miles away (4-hour commute) from OHSU; so, my care will be transferred there, giving me close access to the surgeon.
Medicine Regiment: 625mg Tylenol every 6hrs (end at first follow-up). 600mg Ibuprofen every 8hrs after taking Tylenol (end at first follow-up). 5mg Oxycodone every 6hrs PRN. 1 Lidocaine patch divided on inner tight and groin for 12hrs. Miralax. Resume your estrogen.
There is no diet restriction, however, drinking plenty of fluids is important with narcotics and flushing out the system. Miralax can be used for up to 1 month for constipation.
Try to keep your walking to 2,000 steps a day, for 4 weeks. Do not lift over 10 pounds for 4 weeks. Take stairs one at a time so you do not open sutures. Ice the mons (fatty tissue over public bone) for 20 minutes every 1-2 hours.
Be certain to rest and recover.
You will want to start using sanitary pads to collect blood from wounds.
Shower twice daily for 6 weeks after surgery. No pool or tub for 3 months! Stitches will dissolve on their own.
Appearance: Lots of swelling and bruising. To quote one trans individual, it will look gross, mutilated, or like a Frankenstein. The swelling can take many months to go down. In 6-12 months, you should start to see your vulva settling into form.
-----------------------------------------------------------------------------------------------------------
A CAREGIVER’S DUTY
A certain your caregiver knows their task and is comfortable with what is to be expected.
Surgery Day -- On site to talk to medical staff and to answer questions on the patient's behalf. Caregiver can stay in hospital in an extra bed.
Leaving Hospital -- Carry items, pick up medication, and drive.
At Home -- Help with putting you in comfortable position, give water, food, phone and supplies to patient. Observer and assist in showering and moving. This caregiver needs to be available 24 hours a day for about 14 days. This can be in person or on the phone.
The main goal is to have someone if there is an emergency, call doctors, and provide support and wound care.
Wound Care -- Help with cleaning, dressing, and observing surgical sites for 4 days.
-----------------------------------------------------------------------------------------------------------
FOLLOW-UPS
It might differ from different hospitals.
DAY 3-4 -- First Follow-Up: Remove dressing and catheter. Check surgical site and see how PT is doing with pain, urination, and BM.
4 WEEKS -- Second Follow-Up: 15-minute visit to check on health and answer questions.
3-6 MONTHS -- Third Follow-Up: 15-minute visit to check on health and answer questions. They will access the healing.
1 YEAR -- Fourth Follow-Up: 15-minute visit to check on health and answer questions. Last visit.
-----------------------------------------------------------------------------------------------------------
COMPLICATIONS DURING & AFTER SURGERY
This list is the most common complications seen in GRS patients; however, it does not mean that you will have these complications. It is just best to be aware during your recovery.
Vulvoplasty tends to have less complications as compared to vaginoplasty, but complications can happen depending on your current health.
These complications include:
Bleeding: Bleeding is to be expected after surgery. However, if it does not stop on its own in a few days, a second operation may be necessary to stem the bleeding.
Infection: Although the procedure is done in a clean and sterile way, there is always a chance of bacteria entering the wound. In the period after the operation, there is also a risk of infection. That is why it is so important to take good care of the wound at all times as infection can damage the structure.
Blood suffusion (haematoma): Some blood may accumulate in the surgical area, which may give the area a slightly blue or purple appearance, like a bruise. This will go away by itself after 2 to 4 weeks.
Fluid retention (oedema or seroma): Fluid may also accumulate in the surgical area. If this feels uncomfortable, the fluid can be removed by the physician in a follow-up.
Badly healing wound edges (wound dehiscence): After the operation, the wounds may not heal immediately, and may open up a little. Should this happen, it is recommended that you rinse the wound thoroughly with running water and, if necessary, contact your attending physician.
Hypergranulation: Hypergranulation is a very common problem. It is benign, but does involve a sizeable loss of fluids or blood. It may also have a certain odor and be painful, but it is easy to treat.
Loss of feeling/orgasm: As with any surgery, nerves may be damaged in the operation. Sometimes feeling will not be restored to what they once were. Orgasm can also change after the surgery.
Scarring: The growth in scarring tissue differs per person, skin type and surgical method. People and skin types all heal in their own way. Being overweight or a smoker means that wounds will heal less pretty than in healthy, non-smokers. Sometimes, a scar can be corrected (at least one year after the operation).
Urine spraying: One-third of people in published studies report this complication. Patients often find that it can take more than 6 months before the urine stream is more directed. If you still have bothersome urine spraying after 6 months, it can be often corrected with a second surgery.
Urinary urgency/frequency: This is a feeling of having to pee suddenly and often. This is common soon after surgery because of bladder irritation. This typically resolves on its own.
Urine leakage: This can happen without warning. This usually happens when pressure increases in the abdomen, such as with coughing, laughing or sneezing. This usually gets better on its own as you heal. Pelvic floor physical therapy can help.
-----------------------------------------------------------------------------------------------------------
END RESULTS
The final results will not be visible until after six months with the reduction of swelling. Most who have this operation tend to have an immediate negative experience after seeing their neo-vagina just after surgery.
Remember, this operation takes up to 6-12 months to complete the healing process.
The swelling and discoloration will slowly subside. The vagina will form naturally after the operation and will adapt to your body shape. For example, the color of the scrotum and the amount of fatty tissue will determine what the genitals will look like. The end result is different for everyone.
-----------------------------------------------------------------------------------------------------------
SCAR CARE
Massage is suggested to help loosen scar tissue. This can ease the discomfort and make them less visible over time. It is suggested you begin scar massage, advised by PT, 5-8 weeks after surgery. Daily exercise for 5-10 minutes.
Remember! A Massage Isn’t Meant To Hurt! Go gently to desensitized first.
-----------------------------------------------------------------------------------------------------------
CORRECTIONS
If you are not completely satisfied with the appearance or function of the genitals, you can discuss this with your plastic surgeon or urologist. They will be able to tell you whether an additional operation could lead to improvements.
Some surgeons report that nearly half of their patients will need a second surgery to fix complications or for aesthetics. Some surgeons also tell everyone that two surgeries are always necessary for a final result.
Corrections may, for example, be:
A reduction of the inner labia.
A correction of the clitoral hood.
A correction of the urethra.
In principle, corrections are not performed within 6 months of the first operation. It is advisable to wait at least one year as most issues are due to swelling.
The difficulty with cosmetic corrections is that getting them covered by insurance is difficult without a medical reason.
-----------------------------------------------------------------------------------------------------------
SEXUALITY
Your sex drive (libido) depends on the hormone testosterone. Most patients recovering from GRS report having a low sex drive for a while, as their testicles have been removed.
However, your sexual life depends not only on genital surgery, but also on many psychological and biological factors; so, do not be discouraged if you cannot reach climax at the time.
It can take upwards of 6-9 months for the nerves to heal after surgery. Nerves will not regrow for around 3-4 weeks after surgery. They will then begin to regrow at 1 millimeter a day or 1 inch a month. It seems that younger people will see the most regrowth. This packed regrowth might make sexuality more intense than before.
However, numbness is also a possibility.
It is natural to feel numb in some areas of the surgical site. With nerves regrowing, it will feel like pins and needles, tingling, and or a quick electric shock. Some find their clitoris desensitized, whereas others find it overly sensitive...it varies.
Becoming familiar with your genitals and learning to use them in a pleasurable way are significant challenges after genital surgery. It is important that you discover what gives you sexual pleasure and that you discuss this with your potential partner/partners
Some people have no desire for penetrative vaginal sex, in which case a vulvoplasty can be a good choice.
After vulvoplasty, you can still have orgasms through the stimulation of the clitoris — just like in the case of vaginoplasty. During a vulvoplasty, your surgeon will construct a clitoris from the glans and, if applicable, the foreskin of the penis.
-----------------------------------------------------------------------------------------------------------
RESUMING NORMALCY
Walking: 2000 steps (1 mile) a day for first 4 weeks | Afterwards, gradually increase. The more active you are, the more swelling there will be.
Showering: Twice daily for six weeks.
Bathing & Pools: No bathing or swimming for 3 months.
Lifting: Nothing over 10lbs for 4 weeks. | Afterwards, gradually increase.
Exertion: No workouts, running, or strenuous activities for 6 weeks. No biking for 3 months.
-----------------------------------------------------------------------------------------------------------
RESOURCES
https://genderaid.org/en/feminization/info/vulvoplasty
https://www.ncbi.nlm.nih.gov/books/NBK222286/
https://www.ohsu.edu/sites/default/files/2022-07/OHSU-vulvoplasty-booklet-2022.pdf
#gender transformation#gender#transgender#surgery#change#transformation#trans#tg#gender reassignment#gender reassignment surgery#MtF trans#male to female
17 notes
·
View notes
Text
🌟 Hey everyone, I hope you're doing well. I'm reaching out today to ask for your support. I'm an Afro-Mi’kmaw Two-Spirit system distributor on a journey towards self-discovery and self-acceptance, and I've come to a point where I'm ready to undergo top surgery. This is an important step for me to align my physical self with my true identity. 💪
💖 Finally, I've found the courage to live authentically, to embrace who I am. I've taken the step towards top surgery, a pivotal moment in my life. But here's where I need your support.
🩺 Unfortunately, I don't have the financial means to cover my care during the recovery period when I'll be unable to work. This surgery is not just about changing my body; it's about healing the scars of a closeted life.
💖 However, I can't do it alone, and that's where you come in. I've set up a fundraiser to help cover the costs of my top surgery. Any contribution, big or small, will make a huge difference in my life and my journey. If you can donate, please visit the link below.
💬 Additionally, your emotional support means the world to me. Kind words, encouragement, and sharing this post can go a long way in spreading the word and reaching more people who may be able to help. 🔄
✨ Thank you from the bottom of my heart for being a part of this journey with me. Together, we can make a difference and help me become the person I've always known I am. 🌈
Please donate through Wealthsimple: $shayco
Or via PayPal Can you help Help Shay “Yeet the Teet” on PayPal Fundraisers? Every little bit helps!
https://www.paypal.com/pools/c/8XQSNPvL8D
#TopSurgeryFundraiser #TransRights #SupportEachOther #TwoSpiritPride #CommunitySupport #wealthsimple #wealthsimpledonate #donate #topsurgery #twospirit #2SLGBTQIA+ #transmasc #bipoc #BlackandTrans #mutualaid #transcare #non-binary #Black #Queer
#transmasc#lgbt#gender euphoria#transgender#nonbinary#ftm#two spirit#Indigenous#afro indigenous#black#BIPOC#2SLGBTQQIA#top#top surgery#top surgeon#health#healthcare#mutual aid#trans#transformation#transformers#chest dysphoria#body dysphoria#life changing#donatetoday#donate if you can#paypal#donate
4 notes
·
View notes
Text
hm. maybe..... it's not that important?
#mind blowing thoughts at 10:40 watching youtube in bed stressed out of my mind#maybe. it just. doesn't really matter#i will apply to grad school and i will try but like. life will keep going whether or not it's perfect#i will find more schools and will apply to them#and if i apply to enough one of them will take me#so maybe it's not that important? maybe i don't need to feel this much panic over a resume and a ~1000 word essay#maybe my sexuality doesn't really matter#maybe literally no one cares#i can be whatever and it's chill. i could decide i am only attracted to transformers and i don't think anyone would give a fuck#maybe my gender is just 🤷🏼 and whoop dee do.#maybe i'll get top surgery just because i'm tired of living in discomfort#and maybe that doesn't mean anything besides. i don't want this pain anymore#it's just..... not that important#this isn't a big thing i don't think but it feels revolutionary#maybe i don't have to take on all this stress and worry because... maybe it's not important#life will keep going no matter what i pick or choose or do or feel or say#and that seems more important than anything else
3 notes
·
View notes
Text
The way I'm willing to forget Shockwave's consistent characterization of being a legit evil war criminal... to make him a dragon dad with autistic transmasc swag.
That's just too Lgbt for me to ignore. I'm sorry canon Themes and Motifs.

"Let's switch voiceboxes. For gender fuckery."

#Canon said he forced gender reassignment surgery on Arcee#As a transmisogynistic way of introducing gender on TFs when the writers were confronted on lack of female characters#I say HE transed his own gender and made gender affirming surgery on decepticons#tfp shockwave#transformers prime#Shockwave
16 notes
·
View notes
Text
I really love the 2015 run of transformers idw put out but I cannot get over the decision to make arcees backstory a terf talking point
#acrees trauma being forced gender reassignment surgery is so bad#like just make her from caminus#transformers#idw#arcee
0 notes
Text
A world without trans people has never existed and it never will.

Seriously just search (Trans History).
Here are some examples:
"Sumerian and Akkadian texts from 4,500 years ago document priests known as gala who may have been transgender. In Ancient Greece, Phrygia, and Rome, there were galli priests that some scholars believe to have been trans women.
Roman emperor Elagabalus (d. 222 AD) preferred to be called a lady (rather than a lord) and sought sex reassignment surgery, and in the modern day has been seen as a trans figure.
Hijras on the Indian subcontinent and kathoeys in Thailand have formed trans-feminine third gender social and spiritual communities since ancient times, with their presence documented for thousands of years in texts which also mention trans male figures. Today, at least half a million hijras live in India and another half million in Bangladesh, legally recognized as a third gender, and many trans people are accepted in Thailand.
In Arabia, khanith today (like earlier mukhannathun) fulfill a third gender role attested since the AD 600s.
In Africa, many societies have traditional roles for trans women and trans men, some of which survive in the modern era.
In the Americas prior to European colonization, as well as in some contemporary North American Indigenous cultures, there are social and ceremonial roles for third gender people, or those whose gender expression transforms, such as the Navajo nádleehi or the Zuni lhamana."
In conclusion. Being trans is not a fad and it isn't going anywhere just because some crazy religious nut jobs say we don't fit into their abusive hateful world views. We are here and always will be. So get used to it. 👋😘
#lgbtq#trans#transmasc#trans masc#transfem#transgender#trans woman#transgirl#lgbtqia#trans rights are human rights#trans rights
3K notes
·
View notes
Note
I'm imagining the very unfortunate 13 year old trans boy who has top surgery and then grows more later as puberty progresses.
(I know that 13 year olds don't get top surgery unless there's something VERY weird/wrong [for instance: cancer] going on with the kid's body.)
Minors absolutely can and do get, for instance, breast implants--but only if they're cis, and only with parental permission. The fucked up thing is that a lot of medical procedures that are considered perfectly safe and uncontroversial as long as you're cis (puberty blockers, HRT, various kinds of plastic surgery) get rhetorically transformed into a big scary cloud of evil for trans people, and even transphobes who are nominally opposed to, say, breast implants for sixteen year olds certainly aren't going to spend nearly as much time, if any at all, railing against that sort of thing in public. Because all of this is a post-hoc justification for an intense disgust they feel at gender nonconformity, not actually a principled defense of anybody's rights.
This is also why you can't rhetorically pin them down on any single point. They'll lie about GCS; and when you point out that's a lie, they'll go "well, what about puberty blockers?" And if you point out that puberty blockers are pretty safe, were invented to treat precocious puberty in cis kids, and their effects are entirely reversible, they'll leap to bathrooms or FUD about nebulous issues of "women's rights," and if you try to pin them down about that, they'll circle right back around to lying about GCS, hoping any onlookers have forgotten about or missed that part of the discussion.
I have very little sympathy for people who argue so transparently in bad faith and whose pyschosexual obsessions are so nakedly on display. Books like Irreversible Damage lay bear the extent to which transphobia is almost wholly about cis peoples' anxiety about their own gender and gender expression, in the same way that homophobia is often straight people twisting themselves into knots about their own sexuality. What these people really need is therapy, or an ayahuasca retreat, or to do some yoga about it, but that would require the uncomfortable process of cultivating self-knowledge, so plan B is "make sure I don't have to be confronted with evidence that the human experience is more diverse and complicated than I have been previously willing to believe."
3K notes
·
View notes
Text

I'm coming to love my graft.
It looks freaky. That's okay, I'm a freak.
It looks scary. That's okay, I'm scary (so I’m told).
It looks like it hurt. It did, and it was great.
It represents a long hard road out of hell. It's a sign of my dedication to authenticity. I'm proud of it.
Transphobes do their best to scare trans men away from life-saving medical care like phalloplasty with gruesome photos of fresh surgical sites. They want you to believe that it'll always look like that. But your flesh will heal, and so will your soul.
Here's the truth about transphobes: if gender affirmation surgeries were pristine, blood-free, scar-free, magical transformations, they would STILL try to scare you out of getting them.
Getting pins in a broken leg is gruesome, too. But isn't it worth it once the leg heals?
I love my scars. They're stories told in skin. Here's where I broke up a dog fight. This one's from a gun. Here's one from an Offspring concert. Here are the ones I got in exchange for a life without dysphoria. My scars celebrate my life and remind me of lessons I've learned.
So, too, with my graft. Every day I can look at it and remember that I made it. That I am made whole. That I am free.
I don't hide it when I go out in public. I am not ashamed. Let everyone who sees me know that I am a self-made man.
#transgender#trans joy#trans positivity#phalloplasty#bottom surgery#ftm#trans men#trans matters#gpoy#surgical scars#self love#meatspace#lgbtqia#lgbt#queerdom#originally posted on twitter
2K notes
·
View notes
Text
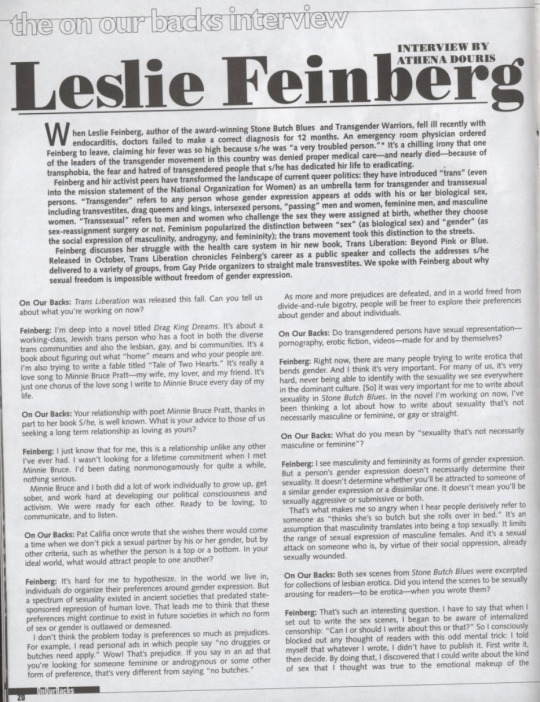
An interview with Leslie Feinberg appearing in the Oct/Nov 1998 issue of On Our Backs.
Please click on image to read or find the transcript below:
Feinberg and hir activist peers have transformed the landscape of current queer politics: they have introduced "trans" (even into the mission statement of the National Organization for Women) as an umbrella term for transgender and transsexual persons. "Transgender" refers to any person whose gender expression appears at odds with his or ber biological sex, including transvestites, drag queens and kings, intersexed persons, "passing" men and women, feminine men, and masculine women. "Transsexual" refers to men and women who challenge the sex they were assigned at birth, whether they choose sex-reassignment surgery or not. Feminism popularized the distinction between "sex" (as biological sex) and "gender" (as the social expression of masculinity, androgyny, and femininity); the trans movement took this distinction to the streets.
Feinberg and hir activist peers have transformed the landscape of current queer politics: they have introduced "trans" (even into the mission statement of the National Organization for Women) as an umbrella term for transgender and transsexual persons. "Transgender" refers to any person whose gender expression appears at odds with his or ber biological sex, including transvestites, drag queens and kings, intersexed persons, "passing" men and women, feminine men, and masculine women. "Transsexual" refers to men and women who challenge the sex they were assigned at birth, whether they choose sex-reassignment surgery or not. Feminism popularized the distinction between "sex" (as biological sex) and "gender" (as the social expression of masculinity, androgyny, and femininity); the trans movement took this distinction to the streets.
Feinberg discusses her struggle with the health care system in hir new book, Trans Liberation: Beyond Pink or Blue. Released in October, Trans Liberation chronicles Feinberg's career as a public speaker and collects the addresses s/he delivered to a variety of groups, from Gay Pride organizers to straight male transvestites. We spoke with Feinberg about why sexual freedom is impossible without freedom of gender expression.
On Our Backs: Trans Liberation was released this fall. Can you tell us about what you're working on now?
Feinberg: I'm deep into a novel titled Drag King Dreams. It's about a working-class, Jewish trans person who has a foot in both the diverse trans communities and also the lesbian, gay, and bi communities. It's a book about figuring out what "home" means and who your people are. I'm also trying to write a fable titled "Tale of Two Hearts." it's really a love song to Minnie Bruce Pratt-my wife, my lover, and my friend. It's just one chorus of the love song I write to Minnie Bruce every day of my life.
On Our Backs: Your relationship with poet Minnie Bruce Pratt, thanks in part to her book S/he, is well known. What is your advice to those of us seeking a long term relationship as loving as yours?
Feinberg: I just know that for me, this is a relationship unlike any other I've ever had. I wasn't looking for a lifetime commitment when I met Minnie Bruce. I°d been dating nonmonogamously for quite a while, nothing serious. Minnie Bruce and I both did a lot of work individually to grow up, get sober and work hard at developing our political consciousness and activism. We were ready for each other. Ready to be loving, to communicate, and to listen.
On Our Backs: Pat Califia once wrote that she wishes there would come a time when we don't pick a sexual partner by his or her gender, but by other criteria, such as whether the person is a top or a bottom. In your ideal world, what would attract people to one another?
Feinberg: It's hard for me to hypothesize. In the world we live in, individuals do organize their preferences around gender expression. But a spectrum of sexuality existed in ancient societies that predated state. sponsored repression of human love. That leads me to think that these preferences might continue to exist in future societies in which no form of sex or gender is outlawed or demeaned. I don't think the problem today is preferences so much as prejudices. For example, I read personal ads in which people say "no druggies or butches need apply." Wow! That's preiudice. If you say in an ad that you're looking for someone feminine or androgynous or some other form of preference. that's very different from saving "no butches." As more and more prejudices are defeated, and in a world freed from divide-and-rule bigotry, people will be freer to explore their preferences about gender and about individuals.
On Our Backs: Do transgendered persons have sexual representation-pornography, erotic fiction, videos made for and by themselves?
Feinberg: Right now, there are many people trying to write erotica that bends gender. And I think it's very important. For many of us, it's very hard, never being able to identify with the sexuality we see everywhere in the dominant culture. [So] it was very important for me to write about sexuality in Stone Butch Blues. In the novel I'm working on now, I've been thinking a lot about how to write about sexuality that's not necessarily masculine or feminine, or gay or straight.
On Our Backs: What do you mean by "sexuality that's not necessarily masculine or feminine"?
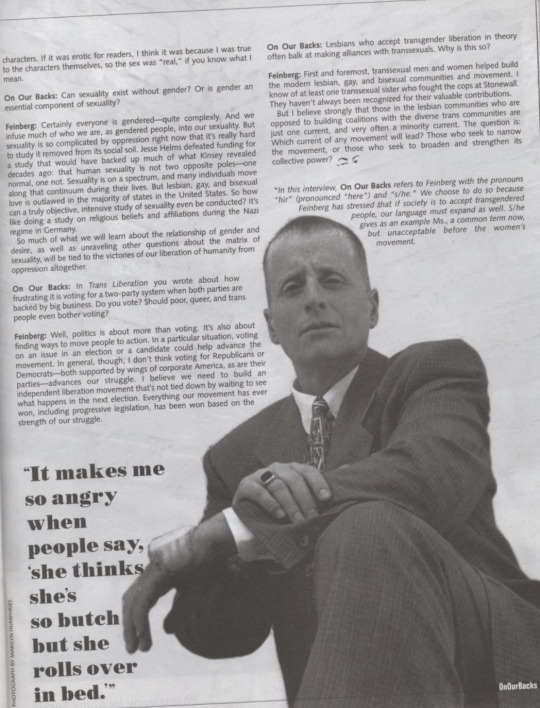
Feinberg: I see masculinity and femininity as forms of gender expression. But a person's gender expression doesn't necessarily determine their sexuality. It doesn't determine whether you'll be attracted to someone of a similar gender expression or a dissimilar one. It doesn't mean you'll be sexually aggressive or submissive or both. That's what makes me so angry when I hear people derisively refer to someone as "thinks she's so butch but she rolls over in bed." It's an assumption that masculinity translates into being a top sexually. It limits the range of sexual expression of masculine females. And it's a sexual attack on someone who is, by virtue of their social oppression, already sexually wounded.
On Our Backs: Both sex scenes from Stone Butch Blues were excerpted for collections of lesbian erotica. Did you intend the scenes to be sexually arousing for readers - to be erotica - when you wrote them?
Feinberg: That's such an interesting question. I have to say that when I set out to write the sex scenes, I began to be aware of internalized censorship: "Can I or should I write about this or that?" So I consciously blocked out any thought of readers with this odd mental trick: I told myself that whatever I wrote, I didn't have to publish it. First write it, then decide. By doing that, I discovered that I could write about the kind of sex that i thought was true to the emotional makeup of the characters. If it was erotic for readers, I think it was because I was true to the characters themselves, so the sex was "real," if you know what I mean.
On Our Backs: Can sexuality exist without gender? Or is gender an essential component of sexuality?
Feinberg: Certainly everyone is gendered - quite complexly. And we infuse much of who we are, as gendered people, into our sexuality. But sexuality is so complicated by oppression right now that it's really hard to study it removed from its social soil. Jesse Helms defeated funding for a study that would have backed up much of what Kinsey revealed decades ago: that human sexuality is not two opposite poles- one normal, one not. Sexuality is on a spectrum, and many individuals move along that continuum during their lives. But lesbian, gay, and bisexual love is outlawed in the majority of states in the United States. So how can a truly objective, intensive study of sexuality even be conducted? It's like doing a study on religious beliefs and affiliations during the Nazi regime in Germany. So much of what we will learn about the relationship of gender and desire, as well as unraveling other questions about the matrix of sexuality, will be tied to the victories of our liberation of humanity from oppression altogether.
On Our Backs: In Trans Liberation you wrote about how frustrating it is voting for a two-party system when both parties are backed by big business. Do you vote? Should poor, queer, and trans people even bother voting?
Feinberg: Well, politics is about more than voting. It's also about finding ways to move people to action. In a particular situation, voting on an issue in an election or a candidate could help advance the movement. In general, though, I don't think voting for Republicans or Democrats - both supported by wings of corporate America, as are their parties - advances our struggle. I believe we need to build an independent liberation movement that's not tied down by waiting to see what happens in the next election. Everything our movement has ever won, including progressive legislation, has been won based on the strength of our struggle.
On Our Backs: Lesbians who accept transgender liberation in theory often balk at making alliances with transsexuals. Why is this so?
Feinberg: First and foremost, transsexual men and women helped build the modern lesbian, gay, and bisexual communities and movement. I know of at least one transsexual sister who fought the cops at Stonewall. They haven't always been recognized for their valuable contributions. But I believe strongly that those in the lesbian communities who are opposed to building coalitions with the diverse trans communities are just one current, and very often a minority current. The question is: Which current of any movement will lead? Those who seek to narrow the movement, or those who seek to broaden and strengthen its collective power?
*In this interview, On Our Backs refers to Feinberg with the pronouns "hir" (pronounced "here") and "s/he." We choose to do so because Feinberg has stressed that if society is to accept transgendered people, our language must expand as well. S/he gives as an example Ms., a common term now, but unacceptable before the women's movement.
Source.
2K notes
·
View notes
Text
ill be honest about this perspective bc I don't rly see this all too often when people speak about transition;
top surgery was not really 'affirming' to me. i was not transformed into my 'true self'. it is more like I was carrying a heavy backpack, and now I am not.
I never really liked the butterfly metaphor for transness, for me personally. I get the utility of it, but for me, like a butterfly, the thing that comes out of the chrysalis isn't the 'true self' of a caterpillar. the caterpillar is a caterpillar. that's it's true self. eventually it has a different shape and we call it a different thing but it's not somehow a 'false self.' it was, and now it is.
do I like the shape of my chest more now? yeah. do I like that I lost 8 pounds of tissue that has hunched me and pained me for more than a decade? fuck yeah.
I appreciate it a lot. but I don't know if I would call it a 'gender affirmation' surgery because I don't particularly see my body after it and go 'now it's more in line with my gender, my gender has been affirmed.'
instead of being a butterfly transformed from a caterpillar, it's more the kind of transformation that accompanies taking your shoes off when you get home, I guess. it's comfortable.
if you asked me after I take off my shoes 'arent you so happy your gender is affirmed?' it would be as accurate of a question, too.
#to be fair if my gender in quesiton is autismgender then yeah i feel affirmed when i can discard the shackles of society (and shoes)#ok to comment on reply to etc
270 notes
·
View notes
Last Seen Blogs

jiayi202
jiaqing

shinobilegend
legendary.

beattheneetpg-blog
Untitled

mausoleefleuri
Le Mausolée Fleuri

ivorivet
Ivorivet