#general accommodations
Text
Guide to Accessibility, Adiustments & Accommodations
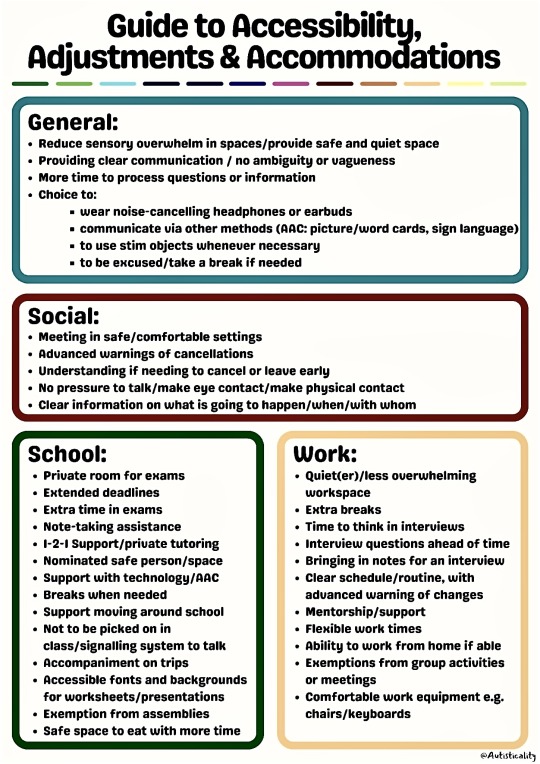
General:
Reduce sensory overwhelm in spaces/provide safe and quiet space
Providing clear communication / no ambiguity or vagueness
More time to process questions or information
Choice to:
wear noise-cancelling headphones or earbuds
communicate via other methods (AAC: picture/word cards, sign language) . to use stim objects whenever necessary
to be excused /take a break if needed
Social:
Meeting in safe/comfortable settings
Advanced warnings of cancellations
Understanding if needing to cancel or leave early
No pressure to talk/make eye contact/make physical contact
Clear information on what is going to happen/when/with whom
School:
Private room for exams
Extended deadlines
Extra time in exams
Note-taking assistance
I-2-I Support/private tutoring
Nominated safe person/space
Support with technology/AAC
Breaks when needed
Support moving around school
Not to be picked on in class/signalling system to talk
Accompaniment on trips
Accessible fonts and backgrounds for worksheets/presentations
Exemption from assemblies
Safe space to eat with more time
Work:
Quiet(er)/less overwhelming workspace
Extra breaks
Time to think in interviews
Interview questions ahead of time
Bringing in notes for an interview
Clear schedule/routine, with advanced warning of changes
Mentorship/support
Flexible work times
Ability to work from home if able
Exemptions from group activities or meetings
Comfortable work equipment e.g. chairs/keyboards
Autisticality
Slightly edited the picture to make it easier to see
#autism#actually autistic#neurodiversity#actually neurodivergent#accommodations#types of accommodations#work accommodations#school accommodations#social accommodations#general accommodations#feel free to reblog/share#source: Autisticality (Facebook)
310 notes
·
View notes
Text
Would kill to read animal POV fiction that has the animal POV’s interaction with humans be like, semi realistic to the level of caution most predators take with large prey and/or competitors (including humans).
Like instead of the usual - “the human is such a weak, pathetic creature... so slow, no claws, blunt teeth… completely helpless without its 'Fire Sticks'. how is it the master of the earth?” type crap it’s like, the bear protagonist or whatever approaches some dude who spreads their arms and yells and the bear is like “FUUUUUUUUCK THAT THING JUST GOT HUGE. IT'S LARGE AND MAKING NOISES. HOLY FUCK.”
#A lot of this realm of fiction tends to severely overestimate how physically weak humans are in the grand scheme of things..#A human body ft. no tools has a pretty average level competency at escaping predation. WITH tools it's significantly above average.#Like a lot of human physiology IS the way it is because of reliance on tool/fire use but interspecies competition/predation is really not#a literal battle won by physical strength + teeth + claws (at least until the actual process of killing)#Intimidation and shows of strength/threatening behavior can go a long way. Healthy predators (who aren't unnaturally#accommodated to humans) are generally going to be cautious and may avoid confrontations they absolutely COULD win because#the risk of injury is judged as too high#And most animals can't weigh risks in the most objective manner and won't understand that you aren't any 'bigger' just because you#wave your arms and yell. That is why puffing up/spreading out as a threat display is so ubiquitous in nature.#Massive tangent but this is why I fucking loved Prehistoric Planet so much like the commitment to having its dinosaurs behave like#actual animals is fantastic and tragically rare#Like having a scene where a T Rex gets bullied away from a carcass by two much smaller azhdarchids.. Yeah that is probably#how it would behave. It's not a mindless killing machine it's an animal so is going to avoid confrontations it deems too risky even if it#WOULD win in an all out brawl. thank you so fucking muych.
181 notes
·
View notes
Text
Doctors and nurses who are not willing to listen to their patients should be replaced
BY VICTORIA SMITH
The third time I went into labour, I was determined to avoid getting told off. With both of my previous births, I had somehow managed to get things wrong. My errors the first time: going to hospital too early, then, when I returned three hours later, “leaving it so late”. The second time: ignoring assurances that I didn’t need to come in yet, then giving birth in the car park — an event I later discovered was being used in antenatal classes as an example of women “not planning ahead”.
“My previous births have been fast,” I said, when I went into labour with my third, “so I’d like to come in now.” I was speaking to the woman at the midwife-led unit that is the only option where I live. (If you need a caesarean section, you have to be transferred to next town.) “Third babies are notoriously difficult,” was her response.
What an odd thing to say to a woman already in labour. The “notoriously” suggested it wasn’t based on any actual evidence, but rather a kind of folk wisdom. It felt as though I was being warned not to tempt fate, not to assume that this baby would just pop out. I saw myself being categorised as one of those arrogant women who presumes to know her own body, only to be taught a harsh yet much-deserved lesson. “Third babies are notoriously difficult” sounded not unlike “third-time mothers shouldn’t get above themselves”.
In fact, I have never been particularly cocky about childbirth. When I was pregnant with my first child, back in the days when the Right-wing press were still obsessed with famous women being “too posh to push”, I wondered if I might be able to get an elective caesarean myself. I did not particularly care about childbirth being a wonderful experience, or about “doing it well”. I didn’t care if the Daily Mail thought I was a joke.
What I cared about was not having a child who would face the same difficulties as my brother, who was starved of oxygen at birth. This has had serious consequences for him, and for the rest of my family. Just how serious is hard to gauge. He was born traumatised; there has never been a before to compare the after with. What there has been instead is the hazy outline of an alternative life, one that runs parallel to the one he has now. It’s a life that began with the problem being identified sooner, with him being delivered quickly, perhaps by emergency caesarean. The difference between this and his actual life comes down to something small: mere moments, mere breaths.
I was born three years after my brother, in a larger hospital, where my mother was induced and monitored carefully. There is something very strange about being the sibling who had the safe birth. It feels as though I stole it. There is a constant sense of guilt, as if my life — my independence, my choices — constitutes a form of gloating. “This is what you could have had.” Everything I do feels like something owed to my brother (do it, because he can’t) but also something taken from him (you shouldn’t have done that, because he should have done it first).
Still, my family were fortunate, insofar as my brother didn’t die. Current reports on the Nottingham maternity scandal reference 1,700 cases, with an estimated 201 mothers and babies who might have survived had they received better care. What strikes me, reading them, is the enormous gulf between the cost of a disastrous birth and the trivial, opportunistic way in which childbirth is so often politicised — with mothers themselves viewed as morally, if not practically, to blame if anything goes wrong.
As a feminist who concerns herself with how the female body is demonised, my interest in debates about birthing choices is more than personal. I have read books railing against the over-medicalisation of childbirth, aligning it with a patriarchal need to appropriate female reproductive power. I have also read books protesting the fetishisation of “natural” birth, suggesting that it infantilises women, that it implies women deserve pain. To be honest, I find both arguments persuasive and dismaying. Both are right about the way in which misogyny and professional arrogance can shift the focus away from meeting the needs of women and babies. I feel a kind of rage that we are told to pick a side.
Representations of the labouring woman are so often negative: the naïve idealist, the “birthzilla“, the birth-plan obsessive, the woman who is “too posh to push”. This latter stereotype has gone hand-in-hand with a veneration of vaginal births, and stigmatisation of caesareans, that has had sometimes disastrous consequences. Midwives at the centre of the Furness General Hospital scandal were reported to have “pursued natural birth ‘at any cost’”, referring to one another as “the musketeers”; at least 11 babies and one mother died. But their approach was sanctioned by their employer: the 2006 NHS document “Pathways to Success: a self-improvement toolkit” explicitly suggested that “maternity units applying best practice to the management of pregnancy, labour and birth will achieve a [caesarean section] rate consistently below 20% and will have aspirations to reduce that rate to 15%”. Proposed benefits to this included “a sense of pride in units”.
Responses to maternity scandals now express horror that such an anti-intervention culture ever arose — responses in the same press that denigrated women such as Victoria Beckham and Kate Winslet for not giving birth vaginally. Instead, newspapers now stoke outrage over “natural” treatments during NHS births, such as burning herbs. Women have been shamed for having caesareans, but they have also been shamed for wanting births with minimum intervention — as though they are selfish and spoilt for seeking control over such an extreme situation.
In his memoir This Is Going To Hurt, former doctor Adam Kay writes disparagingly of women who arrive at the delivery suite with birth plans:
“‘Having a birth plan’ always strikes me as akin to having a ‘what I want the weather to be’ plan or a ‘winning the lottery’ plan. Two centuries of obstetricians have found no way of predicting the course of a labour, but a certain denomination of floaty-dressed mother seems to think she can manage it easily.”
Wanting to have some control over your experience of labour — which will hurt you and could kill you or your baby — is not akin to some messianic aspiration to control the weather. And in his mockery of the woman who wants whale song and aromatherapy oils, ironically, Kay deploys the same silencing techniques that might intimidate a woman out of seeking the very interventions he so prizes. What he and others do not seem to grasp is that their arrogance is a problem, regardless of which course of action they champion. It makes women feel they can’t speak, for fear of inviting hostility at their most vulnerable moments. It’s true that none of us knows our body well enough to know how we will give birth. But, looking back, I find it utterly insane, not least given my own family history, that one of my biggest worries during labour was “please don’t let anyone get cross with me”. Then again, I don’t think that fear is unrelated to the desire to remain safe.
Birth is not a joke. It is not a place for professional dick-swinging or political one-upmanship. I cannot describe — and, as I am not my mother, cannot fully understand — the shame of feeling that you “let down” your child before they drew their first breath, that they will forever suffer because of it. You watch an entire life unfolding and that feeling is there, every single day. This is the fear of the women in labour who are characterised as either idiots mesmerised by fantasy homebirths or cold-hearted posh ladies who can’t take the pain. If things go wrong, they are the ones who will bear the consequences, reflecting every day on what might have been, if they’d only done more.
When people discuss their siblings, my mind does wander to the one I don’t have, the one who was born safely. Perhaps he would have a job he loved, or one he hated, but in any case a job. Perhaps he would have a partner. Perhaps he would have children, and I would be their aunt. Perhaps we wouldn’t get on, wouldn’t even speak, but he’d have a life of his own. I know he thinks about this too. I wonder if the professionals who presided over his birth have thought about him since.
My third labour was not, by the way, “notoriously difficult”. My third son arrived into the world safe and well. No one can say why him or me, and not my brother. Mothers may long for control over birth, for which we are mocked; but we do not have it, for which we are blamed. Politics still takes precedence over our needs, and the needs of our babies.
#Traumatic births#Doctors not listening to women#There's no such thing as a birthzilla#Women aren't too posh to push#Doctors are so posh they schedule cesareans to accommodate their schedules not the mothers#Furness General Hospital Scandal#This is going to hurt#Keep Adam Kay away from women#Women wanting a say in their births are not acting like they want to control the weather#Nottingham maternity scandal#If the baby suffers during a traumatic birth it's the mother who will providing the care after they come home from the hospital
552 notes
·
View notes
Note
new gemini update was so good as always but I can't stop thinking:
big mama: there's nothing wrong with my sons
splinter: you fucked up two perfectly good kids is what you did. look at blue. he's got an eating disorder
wwhhhattttt? nooo, don't be silly. leo doesn't have an eating disorder.
leo and donnie have eating disorders--
#this is a Joke but also No It's Not#it's just different flavors lmao#but both of them have absolutely fucked relationships with food#my poor babies... :(... who did this to you...?#(it was me i did)#leo spends a lot of time worrying about whAT hes eating and how mUCH hes eating and if hes eating the rIGHT thing#largely due to his mom and also just being a celebrity/child celebrity in general#but also in part due to:#donnie has a lot of food sensitivities which have really never been accommodated for at all and as a result he just#has a very negative association with food and eating. he doesnt LIKE eating and he avoids it a majority of the time.#its stressful and unpleasant and he doesnt like it#which ofc only gave leo another reason to hyperfixate on food and calories and nutritional value etc etc etc#which leads to#ironically#leo (who def has an undiagnosed ed and restricts/denies himself food regularly): worrying abt making sure donnie eats enough#donnie will do the same thing back sometimes but not with the same obsessiveness that leo does#esp because the ideals surrounding eating and dieting set up around them really kind of just#lead them both to believe (at least to an extent) that leo is fine and eats a totally healthy and ok amount of food (esp in comparison to d#(no he doesnt)(and even when he does thats not the point)#tw eating disorders#cw eating disorders#eating disorders#tw disorders eating#cw disordered eating#disordered eating#gemini au asks#asks#anon
167 notes
·
View notes
Text
Hiii everyone, say, how do your Hawkes go go about sharing their estate? If they do it at all? Is everyone free to come and go or are they more private? Or do they only invite their LI to stay? I'm curious!! :)
#lay rambles#my ocs#oc: liam hawke#oc: lilian hawke#both my hawkes are very social w their friends but i love comparing their boundaries around it#theres variation in rules for specific ppl with both of them ofc but theres still general differences#with liam its all very open and everyone can p much come and go whenever#they dont get extra keys (theyll get lost and he doesnt want randos finding them lol) but they know where to find the spare key#and bodhan and sandal and orana know to let them in whenever#hes very lenient in this this regard but he does have rules abt what he does and doesnt want them to do#mostly its about not making too much of a mess lol bc liam prefers to clean himself#(he doesnt trust the crew with his household and also he has particular ways of doing things and Hates when theyre done differently)#so things like keep your dirty garb at the entrance dont cook by yourselves (this was banned after they did it one (1) time lol) etc#also no fucking allowed. do that somewhere else for the love of the maker he does NOT want to walk into that in his own house#(and it also comes back to liam not trusting them with cleaning but also Not wanting to clean that up lol)#also he is not fond of them going into his room uninvited. most of the house is chill but that is *his* space#he accommodates these rules by e.g. having spare slippers and a little washing basin in the entrance hall for dirty shoes/feet#always makes sure to have snacks in stock that he knows they like#food will have notes abt what to leave for leandra/orana/etc but otherwise food is prepared with his friends in mind#and in general he'll make sure to adjust the space/routine in little ways to accommodate them#(air out when fen isnt there cus he doesnt like drafts; keep curtains open cus anders prefers open spaces; etc)#lilian on the other hand doesnt like when her friends come into the estate without a heads up (cept for emergencies)#but once they have her 'ok' its basically mi casa es su casa#dont yknow. overdo it and get too rowdy but otherwise do whatever#however. she also expects everyone to clean up after themselves. she aint here to play maid and youre all adults#also liam has a general 'please try to not be too wild when leandra is here' and lilian doesnt#not cos she doesnt care but cos leandra is bothered by sth she can speak up herself#oh and lilian uses the basement space as temporary refuge for anyone who needs it (mostly escaped mages)#also side note: both offered gamlen to stay but he refused (out of pride/remorse)#...this got long and i ran out of tag space lmfao so this is it for now xD
83 notes
·
View notes
Note
How big were the land bridges your Magma created?
Uhhh. Pretty significantly big. I tried scribbling them in on a map of Hoenn. There was the big one, and then an island that had non-land bridges (so normal bridges) that connected Sootopolis to the mainland.

#rotomblr#pkmn irl#pkmn rp#ask#it feels really weird to look at a map and NOT see the Lilycove-Sootopolis land bridge#or the Lilycove-Mossdeep land bridge#like…there were communities set up there. Lilycove expanded of course to accommodate more people and pokemon#and the region just became much more accessible in general#hartelore
32 notes
·
View notes
Text

I mean yeah I agree for the most part but I guess I just can’t sequester my definition of “love” in the exclusive territory of emotion. That’s a big word, love. And it includes, for some of us who are awed and humbled by its bigness, love as law, as obligation…
#and then — shockingly! — it accommodates for community building. no wonder it’s one of the commandments :)#no comment re: empathy but I’ve got some bad news about cult ideology and even the most generous definition of ‘love’ —#— has got fuck all to do with its appeal or the human vulnerability to it
20 notes
·
View notes
Text

Doctor Beverly Crusher
@SpaceDocMom
When your society learns that maximizing disabled accommodations for everyone who needs them without means-testing everybody for everything actually results in everyone having an easier life, you'll all be better for it. emojis: black heart, blue heart, masked
3:59 PM · Mar 31, 2024
#star trek#doctor crusher#star trek the next generation#star trek memes#star trek tng#kindness#support#care#compassion#health care#healthcare#disability#accessibility#accommodation#spoons#spoonies
50 notes
·
View notes
Text
i think like. so much would be solved if we normalized the fact that some people do experience delusions and hallucinations. like yes, its something that those people need help with/need more accommodations for, but we could use being more understanding of people with psychotic symptoms in general.
like, i can tell you that at least one person raving about conspiracy theories is someone who experiences delusions, and if we understood that, we wouldn't have such a hard time getting them back to a more grounded perspective.
i am someone who experiences delusions and I do get incredibly triggered by all the unreality bullshit, the simulation theories, all that unreal bullshit, and it is actively negatively impacting people like me.
we could really use a better understanding of those with these symptoms, because acting like having hallucinations/delusions makes you a killer is a take that makes zero sense. Like, genuinely, you have no idea what you're talking about if that's where you immediately go. I can point out a bunch of shit discussing the darkness of humanity and that logic applies to anyone, regardless of mental illness. Delusions and hallucinations don't mean you'll act on anything, it just means that your brain is creating false images or thoughts, and that can get really fucking confusing.
We could use a little more empathy or compassion towards those with these symptoms, because obviously this shit isn't going away for us, just like other disabled people dealing with their disabilities. We are not idiots or monsters, our brain just gives us random false shit sometimes and it really fucking sucks. Be more understanding or I'll telepathically insert false shit into your brain one day, y'all should see the nightmare that some of us have to deal with.
#babey posts#actually delusional#delusions#hallucinations#schizo spectrum#actually psychotic#psychosis#paranoia#hypervigilance#honestly if i wasnt aware of my paranoia. id probably believe a lot of the conspiracy theories out there because of it#like that shit is so strong it makes me feel like everyone's out to get me#and i know they're not! my delusions are just delusions#but for some people. they struggle to tell about that sort of thing and i dont fucking blame them#and we should be more accommodating of people who experience symptoms like this in general#i can handle unreality to an extent. but there's some people who can't handle it at all.#be more respectful and understanding and dont trigger people for fun
190 notes
·
View notes
Text
Moooooooore bracelets







They will make a fine addition to my collection
#actually autistic#autistic crafts#autism win#autistic artist#autistic adult#communication#communication aids#aac#subtle stim toys#subtle#accommodation#autism acceptence month#star wars clone wars#star wars#general kenobi#hello there#general grievous#star wars memes#bluey#bluey cartoon#bluey and bingo#dance mode#dance mode bluey#bluey episodes#dinosaur#stims and fidgets
29 notes
·
View notes
Text
the thing about people setting boundaries with us is that it means I don't have to worry as much about whether they secretly think I'm really annoying or whatever, because if they've set boundaries and told me when stuff I do bothers them in the past, then I know they're willing to tell me if I'm doing something they don't like, and can assume that if they haven't said anything, I'm probably fine
#personal#thoughts#🍬 post#it's nice because it's like ''oh god what if I'm actually being really annoying? oh wait... they would have told me. okay cool''#also people communicating stuff very directly is great just in general#we have friends now who will just say things directly so we don't have to read between the lines#and it's so much better and we have a much easier time communicating#especially because we feel more comfortable saying ''I think I misunderstood this. can you clarify?''#and being open about where we have difficulty when it comes to understanding what people are saying#at the same time it is absolutely wild having people be patient with us and willing to clarify things and accommodate for us#we're very much not used to it and it still catches us off-guard but in a good way
15 notes
·
View notes
Text
a persona inspired ttrpg would fuck so hard
#i feel like it’s generally not too complicated to make an rpg into another kind of rpg#p4 style would be especially fun if you let that person control the shadows in their dungeon#i think the setting/mechanics/theming of personas and shadows and half dungeon crawler half social sim is just fun as hell#and i like ttrpgs. though i’ve unfortunately not had much experience playing them#to accommodate a group playing i’d probably make the slink system work more like fe supports#man someday i’d love to sit down and hash it out#rambles
22 notes
·
View notes
Text
I finished my Dr appointment and am planning on not going back to class lmaoooo
Submitted my group assignment too, so I'm soooo over that headache and heartache!!

#nimo's sheeko sheeko time#today is my brothers hangout day yaaaaaay!#also yesterday I LOST IT LMAOOOO#so heartbroken depressed and a wreck#so glad this stuff generally lasts only a day for me 😇#its actually kind of funny how that works but yaaaaaaay#sometimes I think I am so dramatic#hooyo is supporting my leave today djejje#what else? I have an appointment with my dr on the 9th for my accommodations#lowkey think he tryna get out of it bc they sent me my documents of it today?#which cool but I need him to sign these documents bc I listed out more accommodations!!!#if youre wondering: more time on assignments/can take as many sick days as needed/one on one mentor meetings and#I forgot the last one!!!#but yeah uwu thats whats up
10 notes
·
View notes
Text

lizzie get two wolves 👍
#strato.txt#oil painting#wip#im worried ive unbalanced the composition w the second one on the right tho... its so much closer to the edge#ugh whatever. aunt lizzie is the focus here#i wish i knew what she actually looked like this is just cobbled together from general features of my family#solid build... dark curly hair... bigass ears. she could be one of my cousins. she could be me#ok rq im gonna lay out the story in the tags for anyone who hasnt seen the previous lizzie art#my great-something aunt lizzie was disabled and couldnt walk very well and she died young#she wanted to see the second floor of the farm house real bad but no one ever carried her up there and she died before seeing it#they buried her in a long white dress somewhere down at the creek. we dont know where her graves lost unfortunately#the night she was buried something wearing a white dress walked into the house and up the stairs and disappeared#and sometimes you can hear her down around the creek screaming#somewhere along the line wolves got mixed into the imagery for me#my uncle told me a story about another 'white thing' that was wolfish and would jump on cars#so i just assumed lizzie was a werewolf my whole life#anyways. i think her staying after she died was a manifestation of her desire for autonomy. maybe#maybe if shed had modern accommodations she wouldnt have felt the need to stick around. or maybe she would have idk#either way i think death afforded her control over her own desires in a way she hadnt experienced before#and i think thats why she still hangs around the creek#i hope she would like this. maybe ill take it down there and leave it out for a night when its finished so she can see
19 notes
·
View notes
Text
.
#vent post alert vent post alert!#you can skip ahead this is 100% me being dramatic but ohhh my god#why the fuck do people feel the need to comment on every single tiny thing that i do that literally doesn’t affect anybody#except for making my life that little bit easier??#a list of Very Rude things that i apparently do that don't sit well with people:#working with my overhead lights off when i'm alone in the office (one day a month)#greeting people with a general good morning and not going into every single room to announce my presence when i get into work#working with headphones on#(not bc it's against workplace policies just bc i don't make myself constantly available for chats with my coworkers)#worthy to note i'm not even the only one who does any of these things apparently it's just a problem when i do it go figure#rn it was keeping the pantry door closed bc the noise the electronics in the room make is particularly grating#(pantry door needs to be open at all times for ???? reasons)#i could go on#as you can tell these are all Very Serious and Bothersome Offenses#like i'm sorry very unobtrusively accommodating my autistic brain is such a bother for you#please how can i make YOUR experience even more comfortable at the expense of mine#fuck this shit honestly
12 notes
·
View notes
Text
I just came across this post which explains that disabled people are welcome in the community regardless of the source of their disability. Specifically, people who “did it to themselves” via complications from addiciton, injuries from high-risk behavior, or any number of other reasons (although someone in the notes correctly points out that addiction is already a disability on its own.) Its not currently reblogable but I really wanted the sentiment to reach as many people as possible
So just to be clear, people who “did it to themselves” still deserve accommodation and acceptance and community. In fact I would even go so far as to say nobody ever really “did it to themselves” because no healthy person with options would ever willingly or knowingly disable themselves, and also because factors leading up to pretty much any disability can actually be traced back for generations.
#disability advocacy#disability education#disability community#disabled community#physical disability#neurological disability#invisible disability#chronic illness#chronic pain#chronic fatigue#physical trauma#disability representation#disability rights#disability accommodations#disability resources#disability accessibility#generational trauma#genetics#addiction#addiction recovery#intersectionality#healthcare reform#healthcare access#intersectional social justice#addiction is a disability#addiciton is a chronic illness#substance abuse#chronic injury#mental health education#disability rant
28 notes
·
View notes
Last Seen Blogs

a-kichi
Heartbeat Photos

visaupdates
Untitled

falconshade
somebody stop me I love all Lego media now

memmitts
emmett

jade-and-shade
Ask Jade & Shade