#I’ve already come to terms with accepting medical interventions
Text
should’ve just made a FAQ page for everyone’s questions about my baby/birth because it’s getting stressful answering the same questions and people throwing so many advice and unnecessary comments 🥲
#it’s all the same#and then I feel like I need to educate them on due dates#and then they throw the same jokes like ‘ha ha ur baby gonna be talking when he comes out’#meanwhile I am here mourning the fact I most likely won’t be able to experience spontaneous labor#it’s just something I don’t wanna deal w right now at this point in pregnancy#I’ve already come to terms with accepting medical interventions#and that most things in life don’t go according to our plan#including birth plans *shocking*#but just random people texting me asking me all these questions while im grappling with all these things#is such a huge stressor rn#wish mamas in their last couple weeks of pregnancy can just go into hibernation mode lmao
8 notes
·
View notes
Text
I have an appointment with a psychiatrist for next month. I’m a bit anxious, but mostly relieved. I’m already rehearsing my monologue.
“I need a diagnosis or a prescription or some kind of drastic lifestyle change.”
That’s what I’m going to tell him. I can’t predict what he’ll tell me though. My experiences with therapy have all been different.
The first time a saw a “counselour: was at university. One of my lecturers died suddenly in the middle of a semester and I didn’t know how to cope. I genuinely considered packing up and going home, but it was also the semester before my last and I’d have had to wait a whole year to write my finals.
I stuck it out and met with the school counselour a few times and we talked about my general guilt over having a good time and taking breaks. She told me to watch “Gifted” with Chris Evans and wrote letters to my other lecturers so I could have extra time to finish all my final assignments. I don’t remember much else.
My next time in therapy was with a psychotherapist and it was NOT a good time. That was when I first suspected that I might be experiencing PMDD symptoms and she was not having it. It was not something she would consider, that my hormones were involved at all.
It was not a safe place for me. I didn’t really want to tell her the truth about anything, because I felt like she would judge me.
I told her about the time my boyfriend’s friend posted an inappropriate message about me on my boyfriend’s birthday and how upset I was over it and her conclusion was that I care what other people think, I care about my image. When at that point, I was just hurt that my boyfriend hadn’t stood up for me. He should have known I’d be offended by something like that.
My mom used to come with me to my sessions and wait in the lobby and my therapist implied that meant I was too dependent on my parents. In all honesty, she wasn’t wrong. I am more dependent on my parents than the average twenty-something year old. And that was NOT the evidence of that. My family’s culture is that we’re there for each other. My mom or her sister (or even I, on one occasion) take their mom to the doctor or to run tests. As much as is possible, she doesn’t go alone. Unless nobody can manage, someone always goes with the others to the doctor if they’re open to it. I couldn’t understand how this was different.
Eventually I admitted that this therapist was not for me and I stopped seeing her.
A bit later, we came across a new one. She seemed nice. She had kids. Her office was in the same building as my workplace. It was a match made in heaven. Our first session, she sent me home with a comic to read! She was so understanding and she sent me to do some hormone testing to make sure my thyroid wasn’t part of the problem. Even though my hormones were normal, it was so validating to be heard, to feel like my voice mattered.
I stopped seeing her after one session where I felt embarrassed. We were talking about the menstrual cycle and she exclaimed at my ignorance of how it worked in terms of the fluctuations of hormones and their effects at the different phases.
“You should know this??!!”
And of course she’s right, but I no longer felt safe. I felt judged and a little ridiculous. So we had a conversation about me not needing any more sessions. Then the pandemic hit, the next month I think.
Since then, my mental health has been tossed between bad and worse. I can’t even remember a time when it was good.
I’ve always been anti-medication, mostly because my parents have been. And recently a friend advised against any kind of mood-altering drug. Her withdrawals were nightmarish. And where she lives, the mental health care system is so much better than where I live, so IDK if it’s a risk worth taking.
But I am also tired. I don’t want to have to accept that this is just the way it is, that this is how it will always be. I need some kind of intervention.
0 notes
Photo



“Are you going to have to work on Halloween?” Aster asks, picking everything bagel seeds off his bed with her long, manicured nails.
Bruno would rather not think about her question, instead letting out a groan that he attempts to sound anguished, but comes out more on the side of pathetic. He was aware his first year of medical residency was going to be hell on earth, but nothing could have prepared him for the bone deep exhaustion he was feeling. Despite his annoyance that his friends were cutting into his sparse sleeping time, Bruno felt a wave of relaxation from their presence.
Bruno shoves his face deeper into his pillow and mumbles out “I’ve got two 14 hour shifts this weekend, so I’m booked.”
Aster’s nails turn their attention to poking his cheek. “How about Friday? The restaurant is getting a deep fumigation this weekend, so both of us are off.”
The Laurent was the Irish-French-Russian fusion restaurant where Aster and Nico both worked. A pseudo fancy place that seemed to produce endless stories of rat infestations and staff circulations, yet still managed to get good enough reviews to get it featured in articles proclaiming it to be “probably” the best restaurant in Alphabet City.
He swats Aster’s hand away before she gets to the ticklish part of his ear. “I think I’m free that night, but I’ve gotta be home early so I can make my bedtime like a real adult.”
“We’re real adults too! We pay taxes!” Aster says, while accepting the pre-work blunt Nico had just rolled.
Nico laughs, losing his balance on the unstable seat of Bruno’s deflated bike he was perched on. He tries to gracefully fall but instead flops sideways next to Bruno on his bed. The smell of Nico’s sandalwood cologne and Aster’s blunt fills his senses.
“Since we’ve got this weekend off, maybe you’ll finally work on our bet.” Aster says, nudging Nico’s leg with her foot.
“What’s the bet this time?”
Aster and Nico’s love language seemed to be based entirely on betting the other will do things for prices neither can afford, both monetarily or emotionally. The betting currency often ended with them getting into days long fights and silent treatments. Despite the impracticality of it all, the two still continued to make bets, refusing to listen to their friend’s interventions.
“I have to ask out Willem by the end of the month, or she gets all my tips for the next two weeks.” Nico groans out, “I’m regretting saying yes to this one.”
“It’s not that bad! And if he does then I pay for his metro card for all of November!” Aster protests, “Boyfriend and free rides, that’s a good deal!”
“Neither of you can afford to do this, can you?” Bruno asks, getting a slight headache from their stupidity.
As if to distract from the conversation, Nico shifts his body to curl around Bruno, wrapping an arm around his huddled form above the blankets. His long, silky hair brushing the tip of Bruno’s nose.
For as long as Bruno knew him, Nico was never very good at staying casual with someone. Always torn between his hopeless romantic heart and the polyamorous nature of young adulthood. The cycle was always the same: meet someone exciting, agree to keep it casual, quickly develop feelings, risk it all, and then a two week heartbreak for someone he was only kind-of dating. Bruno was the only person to go through the whole cycle with Nico and end up actually staying friends.
He hoped for Nico’s sake this one wouldn’t turn out like the others.
“Do you know anyone who needs a job?” Nico muffles into the blanket.
“What kind of job?” He already dreaded the answer.
Aster sighs, “We need more busboys at the restaurant, we only have two right now and it’s making things a living hell there.”
“That, and the termites.” Nico adds.
Bruno wonders if he should even recommend that anyone get a job at The Laurent, but smiles and says, “I’ll inquire around.”
The two have already lost interest in his response, and have resumed their usual debates.
“Is busboy a gender neutral term?” Aster asks, with all sincerity.
#BRUNO POV!!!!!!!!!!#his favorite movie used to be twilight ironically and then he unironically started to love it#also this a very important conversation so remember it <3#ts4#ts4 story#foregone conclusion#circle the drain#bruno#aster#nico
42 notes
·
View notes
Note
Based on your experience and views, do you agree or disagree with the sentiments expressed on these two paragraphs? And why? twitter: /Kimberfan76/status/1501921784404324356/
Hello, Anon. First of all, I’m so sorry for responding to this almost a week after you sent it. I’ve had a difficult week and it turned out I had more to say here than I initially thought, so I needed to take regular breaks to ensure I was speaking from my brain and not my emotions. Thank you for your patience with me.
As I’m proofreading everything I wrote down here, I should probably clarify that I agree with both of these women. Objective agreement absent of a dissertation has never been my strong suit, so here it is ahead of time: I agree. You asked me to explain the “why” behind my position. So, here is my “why.”
I have reorganized the tweets here to help me organize my thoughts. You can see the tweets in order in the archived links I have provided.
FeministRoar
Reading through some of the responses from transactivists to the Cass Review and the main complaint seems to be it doesn't unquestionably accept every kid who has gender dysphoria as "trans" and recommend blockers/hormones ASAP in the name of "depathologisation".
I'll never understand how insisting immediate (and possibly lifelong) medical intervention can be framed as "depathologisation." Depathologisation would be acknowledging gender non conformity, confusion and dysphoria are normal but sometimes require mental health support.
Ah, nostalgia (derogatory). It's been a long while since I've heard this one. The depathologization argument is one that I am unfortunately all too familiar with. In fact, I used to argue it myself. FeministRoar already perfectly summarizes my own thoughts on this argument today.
Firstly, usage of the term “depathologization” itself does not even make sense, in my opinion. “Depathologization” is defined as “the process of coming to regard a formerly medical condition as a health or behaviour condition.” That... doesn’t make sense to me. A health condition is a medical condition and a behaviour condition, if not also a medical condition, to me, would insinuate something that is learned. Unless I am misinterpreting this, which I very well could be, I believe “de-medicalization” is a more appropriate term.
I also find it funny how trans rights organizations are the only other results to pop up when you search for the definition of “depathologization.”
Definitions aside, the actual point of this stance is to redefine transgender identity to be a natural variation of existence among humans, which sounds unproblematic enough until you interpret it beyond face value and realize it contradicts everything else that they stand for. If this is truly the end goal, there is no reason why “gender-affirming” care would be required for a transgender person’s mental health—because these services exist to treat something, and under this argument, transgender identity does not need to be “treated.” Why, then, does this care remain so important under this supposed “depathologization” model?
The typical response is “Well, gender dysphoria causes distress, which can cause mental illness, and that can lead to self-harm or suicide.” So, then, transgender identity is a medical condition, considering failure to treat it causes harm to the person, indistinguishable from any other psychological condition.
And then we cycle right back to the beginning.
If you pay close attention to those making these arguments, you may notice for yourself that they accidentally prove their counterpoints very often because they want two things that cannot rationally coexist. The crux of the position is “Include me but not in any way that may make me uncomfortable”—and that directly ties into, if not outright informs, the affirmation model.
A lot of anger about the discussion around the "affirmation" model too, because people have convinced themselves it's some well evidenced international standard, when obviously it's not.
The affirmation model is a product of the affective fallacy wherein “one's emotions, urges or "feelings" are [...] immune to challenge or criticism. [...] In this fallacy one argues, "I feel it, so it must be true. My feelings are valid, so you have no right to criticize what I say or do, or how I say or do it."”
Or, in this case, who you claim to be.
The other thing people are angry about (again) is inclusion of Lisa Littman's study and that should be a good wake up call that just because you and your mates go around yelling about something being "discredited" because you don't like it, it doesn't actually mean that it is.
Has Lisa Littman’s study truly been discredited due to genuine error in her methods, or has it only been “discredited” in the social sense because it makes transgender people feel bad? Personally, I have only ever seen evidence for the latter, and I find it funny (read: sad) because this response only further proves my point that the affirmation model is a product of the affective fallacy.
Another component of the depathologization argument, over-simplified, is that the current healthcare system does more harm to transgender people than it does good because it does not center them in their own treatment. This point is actually not a terrible one in and of itself because it does have some merit. For example, dysphoric people can and do have mental health conditions that may be chalked up to gender dysphoria or transgender identity when they may, indeed, be completely unrelated, rendering those conditions un- or mistreated. The dysphoric person’s own thoughts and opinions also may fail to be adequately accounted for in treatment under the assumption that they cannot, or do not, think for themselves.
Where this point becomes shaky is, it insinuates that the dysphoric person is taking the time to truly evaluate their supposed gender identity when this is just not true for the average person. I’d say it’s safe to speculate that most dysphoric people are not seeing a gender psychologist whose approach is not blind affirmation while they wait to be evaluated for medical transition. Many are not in therapy at all. Some of them can’t be.
So, when they have no one else to turn to, they are logically going to turn to the trans community, where they will generally only explore their identity superficially with other people who feel the exact same as they do and will rarely or never commit the taboo of looking at it more in-depth.
And you can see this in the animosity towards detransitioners. Plainly and simply, if transgender people truly spent as much time evaluating their identity as they want to claim, if transgender people truly knew who they were, detransitioners and the studies done on them would mean nothing—because when you know you are transgender, you don’t feel the urge to shut someone up just because they realized they were not.
I feel nothing when I hear or see transgender people because I remain secure in my “identity” as a detransitioner. They can’t say the same about me. Which one of us is more likely to be insecure about their gender?
Maugham's take seems to be: blockers stop sexed development and that's solely a personal choice, clinicians and whether it's the best route for an individual don't factor for him. So he thinks talking about the need for more evidence is a "central failure" of the review.
I have no idea who is being referenced here, but if this is an accurate summary of beliefs, this Maugham is essentially acknowledging that he does not care about any health problems that children may face as a result of puberty blockers because “that’s solely a personal choice.”
So, I don’t care what this guy’s “take” is. I am not going to attempt to counter someone who so blatantly admits that they do not care about children’s health and safety, least of all when the children in question are already vulnerable. I have no interest in giving that attention.
When someone reprimands a need or request for more evidence, consider what the stakes for them will be if that additional evidence proves something unaligned with their beliefs. They likely have an agenda.
Mainly I think it all boils down to activists wanting these young people to be seen as "trans kids" when clearly appropriate and effective health care requires seeing them as kids with gender dysphoria. I don't think that's a battle activists can win.
Kimberfan76
This is EXACTLY the problem. Activists want “trans” to be seen as a default start, so kids start as trans, they were always trans and so as trans kids they need this treatment. No, they aren’t. They are kids with dysphoria and dysphoria is not a one size fits all issue.
These women have successfully put into words something that I have always felt, yet could never properly express.
I was not always a transgender child. If I were to do juuust a little bit of reaching, I might be able to somewhat reasonably chalk up some of my experiences in older childhood to the beginning stages of dysphoria.
But I was not always a transgender child. I was “fixed” into being one.
I was a naïve child who thought I knew who I was with naïve parents who thought I knew best bringing me to naïve doctors who didn’t have the gall to tell me I was wrong.
I was taken to the higher-ups. My gender psychologist was known as The Best in the industry, capital T/B. I was set up to have what was essentially the best they could offer. This was back when no one cared about transgender people and it wasn’t taboo to say so because most of the people you met, both offline and on, had no idea gender was even a debate. Yet... well, I’ve been through it, and I struggle as a result to this day. It scares me to think where I would be now if unrelated life events hadn’t deterred me from continuing down that path.
If the automatic conclusion is “Trans people have always been trans,” then anything that suggests differently must be biased, discredited, inethical, outdated, unimportant, unreliable, or just plain wrong—but when the full picture clearly shows that transition harms, rather than helps, the only rational conclusion for me to come to is that it is not the answer and must remain unavailable to children.
That is my position. This is my “why.”
#i'm sorry if this response was underwhelming after such a long wait anon#this was so much better in my head but pretty much everything that is wrong with me mentally has been kicking my ass this week#so unfortunately i couldn't make it happen#but i tried really hard to give you a response that you deserved and i hope that effort shows.#i'm gonna take a weekend hiatus now because i need it lmao#submission#answered#gender critical#writing#text#my post
3 notes
·
View notes
Text
BNHA Common Misconceptions
I’ve been seeing wayyy too much bs on my dash lately. So I thought I’d share some of my thoughts on some Controversy™
***Spoilers For The Manga***
1. “What the HPSC did to Hawks wasn’t bad”
A government organization putting a young child through rigorous training so that he can be used as a tool is bad. I don’t know why I have to spell that out
Hawks had to abandon his real name at a very young age. That’s damaging for a kid’s sense of identity. His identity as a person no longer has any separation from his work as a hero. Being a hero is all he is now. I wouldn’t be surprised if (provided Hawks’s wings are gone for good) he has an identity crisis after this arc because he can’t be “Hawks” anymore.
Hawks is based on Lionel Messi, a soccer player recruited at a young age in return for paying for his medical procedures. I’ve seen people say that Hawks chose to be a hero. One, he was a child, young children shouldn’t be making decisions like that. Two, we know based on context clues that Keigo was more than likely living in poverty, possibly with alcoholic parents, and we literally are told that the HPSC payed for his family’s living expenses. Do you really think Keigo had much of a choice here?
I’ve seen people say “it’s just like what UA is doing”. First of all, UA is called out for being irresponsible and endangering their students IN UNIVERSE. Second, Keigo was a young child, the UA kids are 15+. There’s a huge difference.
2. “Mitsuki isn’t abusive”
Honestly when it comes to her smacking Katsuki, I could excuse it as a joke done in poor taste and not hold it over her as a character.
Hitting him WASNT just discipline tho. You should never, ever, under any circumstances hit your kid. Fuck that noise.
What I really have an issue with is what she SAYS to Katsuki. Her guilt tripping him isn’t a throwaway line either. He repeats the sentiment that he is responsible for Kamino during Deku v Kacchan 2. It’s one of the main reasons he fights Deku.
Horikoshi says that Katsuki has a good relationship with his mother. In that case, he did a horrible job at presenting that. What is written in the canon is what should be used as the basis for how we interpret her character.
3. “Shigaraki chose to kill his family/was born evil”
No...just...no. He was FIVE for crying out loud.
He wanted to be a hero, and took extra care to play with kids that had no friends. He definitely wasn’t born evil lmao.
His quirk manifested while he was having an emotional crisis. Decay is controlled by emotion so of course it went haywire.
He didn’t even know it was him doing it at first.
“But Shigaraki said he WANTED it to happen” Shigaraki is an unreliable narrator. What we actually SEE tells a very different story. He reaches out to Hana and his Mother for help. His grandparents are just caught in the shockwave. The ONLY person he killed on purpose was his father.
Now when it comes to his father, he had just beat him and locked him outside. He’s FIVE, and he has no healthy outlet for his anger and frustration. Hell, we see that in his “itchiness”, he only feels like this in the house, because his father makes him suppress his love for heroes and his dream to become one. He takes joy in killing his father because it’s the only release he’s ever experienced.
The fact that you guys forget that this is an abused child with no real control over his quirk that just got beaten and locked outside... Nope, no reading comprehension here.
4. “The League of Villains are justified/are a revolutionary group”
...Shigaraki has stated over and over again that he just wants to destroy everything. He doesn’t care about reform or improving anything. That one panel in Ch. 222, where he says he wants to destroy everything I think sums it up perfectly.

He wants to destroy EVERYTHING good or bad or neither or both. There’s a newborn baby, a field of flowers , Nine, various heroes, the UA kids, etc all varying in innocence.
The rest of the league have very different goals and reasons why they continue to support Shigaraki. Twice wants to protect the only people that accepted him. Spinner just wants to have purpose for his life. Toga wants to live the way she wishes with no consequences. Compress is also here.
The only “revolutionary” is Dabi. But his views are not universal throughout the league.
Even if they were trying to improve things. They have killed countless innocent people, they’ve tried to kill the UA kids too. That’s not ok. And it’s not erased by the fact that they’ve done good. (I do appreciate them for killing the MHA version of the KKK, truly epic of you)
5. “Hawks is abusive”
It’s not abuse to manipulate someone for info when you’re a double agent. It’s kinda shitty, and you could argue that it was unnecessary for Hawks to do so in context. But it’s not abuse.
Y’all need to stop using the word abuse/abusive tendencies to describe all immoral actions
I’ve also seen people say that Hawks has abusive tendencies (as in he’s abusive in all his relationships with other characters) and...do I really need to explain why that makes no sense at all?
6. “Twice deserved to die/it was necessary to kill him”
Feel like I need to remind people that we’ve only ever actually seen Twice kill one guy and that was one of the KKK guys.
Twice isn’t evil, even Hawks admits that he is a genuinely good person. Good people don’t deserve to die.
It wasn’t necessary, and here’s why: Hawks could’ve just knocked him out or even just severely injured him. (Or the HPSC could’ve just grown a brain cell and sent more people to back him up, making it easier to hold back his quirk and arrest him)
Hawks shouldn’t have killed Twice, he only killed him because he’s been raised as a child soldier and I wouldn’t be surprised if what he told Twice about taking out villains was a direct quote from the HPSC

Also, Hawks would’ve killed Twice with or without Dabi’s intervention
Something I do have to say though is that Hawks was right not to just let Twice go. It’s tragic because Twice WAS leaving to help his friends, but the other side of that tragedy it that his friends are terrorists. If he was allowed to leave a shit ton of people would have died (again that doesn’t mean he deserved to die either, don’t get it twisted)
The WHOLE POINT of Hawks v Twice is to make you question who the bad guy is. Both characters are morally gray and the only reason they even have to fight is because of the outside forces controlling their fates. It’s supposed to be tragic it’s supposed to be unclear who is in the right, so stop arguing about it.
7. “Bakugou is abusive/irredeemable” (I know it’s been talked to death but I still see it everywhere)
People are, in fact, allowed to grow past the person they were in middle school.
Most people get hung up on the “throw yourself off a building” line. Which is fair, but again, he was in middle school.
People also say “he hasn’t apologized yet”. Yeah? And? The story isn’t over yet. Horikoshi has already acknowledged that too. I don’t know what you want? People who like him know that his arc isn’t over yet.
I’ve seen a lot of people denying his character development. In the beginning of the series he was a bully and let his ego control him. I don’t think he’s bullied...anyone since Deku v Kacchan 2. He insults people but they obviously don’t take it seriously.
He’s also gone from preferring to fail a final exam to avoid working with Deku, to following him into battle against Shigaraki.
Also, when he actually likes and respects someone he doesn’t mistreat them. This is the same thing with Hawks where y’all NEED to stop misusing the word abuse. He was an abusive friend to Deku when they were kids, that’s it.
8. “Rei was abusive too!”
I’m BEGGING YOU to learn what the term “abuse” means istg
She had a psychotic break. She genuinely thought it was her abusive husband coming through the door, and she acted out of fear.
“Well that’s not an excuse” yes it fucking is. Not to mention that as soon as she realized what happened, she sobs hysterically because she hurt Shouto and tries to use her quirk to help him.
I genuinely don’t understand why people think this
9. “Dabi actually does care about the league”
Listen, I know it sounds harsh, but y’all need to get your heads out of your piles of headcanons.
We know next to nothing about how Dabi feels about just about anything. But we do see that he’s aloof and distant with the league, he doesn’t put in more than he needs to. The rest of the league think of each other as family. Dabi straight up says he doesn’t give a shit about them.
“What if he was just putting up a front for Hawks” Why? Why would he do that? When asked who he was he answered him. He tells him how he feels about hero society and Stain. Not to mention that he was getting ready to kill him. If he was hiding his true feelings about the league I doubt he would’ve so easily said that he didn’t care about them but rather how useful they were.
At this point it’s just wishful thinking. Based on everything we’ve seen in the series so far and everything we know about Dabi, I think it’s safe to say that he doesn’t care about them all that much. If he secretly does care about them, I’d say it’s likely that he doesn’t even know he does.
Idk why all of a sudden villain stans and hero stans are feuding over things that shouldn’t even be up for debate in the first place. Sorry if this came off as super aggressive, I’m just sick of seeing this stuff all over the place. If anyone has anything to add go ahead
#bnha#bnha spoilers#discourse#bakugou katsuki#Hawks#keigo takami#dabi#league of villains#mitsuki bakugou#shigaraki tomura
321 notes
·
View notes
Text
Show Me How Life Could Be
This is my extremely late gift for Jenny (@/froochette) for the @knbsecretsanta . I haven't written for this pairing or concept before and wanted to challenge myself with it. Well, the joke's on me that (once) again the fic went out of hand. This feels more platonic than romantic to me, but I'll let you guys be the judge.
Hope you like it anyway! ♥
P.S. Of course, I'd make it about basketball in one way or another, what are you talking about?
Genre: Humour
Pairing: (platonic) MidoMura
Rating: G
Word Count: 4,191
Summary: Midorima only wanted to do his job properly. Not get into a fight with their most loyal customer and have his life decisions questioned by everyone. Even if maybe, deep down, he was regretting some of them.
Humans show their true colors when faced with someone weaker than themselves.
Midorima Shintarou hadn’t considered himself weak in any regard. On the contrary, he had lived most of his life in moderate privilege: well-off parents, good grades, and boundless athletic ability. This didn’t stop him from always striving with his own two hands for the best humanly possible outcome though. Thus, above all, he fancied himself as a humble person. Acquaintances--friends, depending on who one asked--would often disagree with that statement. But Midorima wanted to believe he had never been as condescending as some of his customers.
The coffee shop he worked part-time was a small cozy place. Located next to the university’s library and lacking any big brand name attached to its identity, it exclusively attracted students who wanted a break from studying or to spend some time between classes. The relaxed pace and the versatile schedule were the biggest reasons Midorima had applied for the position--even if the pay wasn’t anything stellar. As an undergraduate medical student, he didn’t have a lot of free time but he couldn’t impose on his parents forever either. They were already paying for his tuition and half of his rent. It was only fair of him to handle the rest and his day-to-day expenses to the best of his abilities.
For the most part, work was uneventful. Except for the moments when Midorima had to wonder if it was indeed worth the trouble. From demanding customers to people skipping the line and making a fuss over nothing to his personal worst nightmare: customers that seemed to have lost their ability to read written instructions and signs. The redundancy of having to explain simple things annoyed him to no end, as well as the fact they were distracting him from his duties for these trivial issues. Instead of wallowing in despair, Midorima had settled for the next best thing: seething in rage silently. With no other outlet to alleviate this frustration, he’d often picture himself offering retribution to such customers. For example, jumping over the counter to land a solid dropkick to their chest, or throwing the tips jar to their head as they were about to leave. He could make that shot easily from behind the counter and none would be the wiser. The perks of being a former shooting guard known for his ridiculous three-pointers--distance was irrelevant.
Not all customers were irredeemable fools though. Some regulars could be considered at least tolerable, like one Murasakibara Atsushi. The only reason Midorima knew the guy’s name was because of Takao’s snooping. His old teammate/friend kept tabs for all the regulars, more so if they had been involved with high school basketball. Apparently, Murasakibara had been a formidable center in some powerhouse team. It baffled Midorima how such a player had escaped his attention during the championships he had participated in. It shouldn’t have been hard to recognize someone who loomed over the general public like some giant out of an old wive’s tale.
No one seemed to know what Murasakibara was majoring in, but it allowed him to visit the coffee shop every other day. After trying the entire dessert menu in the span of two weeks, he settled on a particular combo. It didn’t matter when he decided to appear, he’d always order the same thing. It saved Midorima a lot of time for which he was somewhat grateful; even if this person’s consumption of sugar worried him as a future medical professional, and cleaning the table after him could become quite a hassle.
Midorima valued rules and order. As painfully hard as it might be to accept, not everyone felt the same way. He was just a glorified waiter in a low-end establishment. He’d do his job, regardless if it was aggravating or not. Keeping his temper in check when faced with personal offenses included, but sometimes there was a limit for even the most patient individuals.
The first term’s midterms had just ended the previous day. Most students seized the opportunity to catch up with their friends over a cup of coffee and some sweets on the side. Suffice to say, the shop was relatively crowded for a regular Wednesday.
Midorima was on cash register duty. Passing all his classes should had left him in a good mood. His horoscope was a bit cloudy that morning though, placing Cancer in 5th place. Nothing too worrisome but he didn’t want to test his luck with handling beverages. So he pushed the responsibility to Takao--who, accustomed to his quirks, only mildly complained--and settled for taking the customer’s orders. Most of the shift went without any incident, but one thing was certain.
Oha Asa was never wrong about his fate.
Midorima didn’t notice the bell chime of the front door above the ruckus of voices. Neither the footsteps approaching heavily. It wasn’t until the lights overhead were partly obscured that he realized Murasakibara had arrived.
With a glance to ascertain the customer’s identity, Midorima began inputting his order. “Would it be the usual?” he asked.
“Actually,” Murasakibara said. “Muro-chin is going to order this time.”
Midorima’s fingers froze and looked once again, properly this time.
There was another student next to his regular customer. He was slightly shorter than Midorima; dark-haired with several locks of hair falling over his left eye. While he appeared like a polite individual, there was too much-concealed amusement in that eye for Midorima’s liking.
“My name is Himuro Tatsuya,” he said with a wave. “I’m sorry if I’m breaking your routine or something. Atsushi wasn’t really planning on coming today--”
“Because today is no good,” Murasakibara muttered under his breath.
“--I kinda dragged him along because I didn’t know where is this. You see, I’ve heard so many good things about this place, I had to see it for myself.”
Takao was wheezing in the back, the coffee machine’s whirling barely overshadowing his laughter.
Midorima ignored him. “What would you like to order then, sir?”
“Nothing extravagant. Just black coffee,” Himuro said. “I am curious about the desserts you have though. They look delicious, but it's hard to choose. Is there something you’d suggest I try?”
On most days, Midorima would stare blankly at such questions until someone came to rescue him from the embarrassment. Instead, this time, he had the fortune of having a dessert in mind. If only because he waited every week to keep a piece of it for himself.
“Today’s specialty is the red bean cheesecake,” he said. “It may sound peculiar but I assure you--”
“It’s stale,” Murasakibara interrupted him. He was examining the display, bored. “Let’s just leave. I told you there is nothing good today.”
“As I was saying.” Midorima adjusted his glasses, annoyance bubbling in his chest. “It tastes perfectly fine. It’s not too sweet so I’d recommend it if you are looking for something to enjoy along with your coffee.”
“This is worse than those in the convenience store,” he cut him off yet again.
“I assure you, sir, that all our desserts are freshly baked.”
“C’mon, Muro-chin. I can make something a lot better and you know it.”
“Why don’t you make it then?”
"Huh?" Slamming his hand on the counter, Murasakibara leaned over the register to level his gaze with Midorima. “Is that a challenge?”
Two things happened simultaneously: Midorima realized he had said that aloud and someone tried to separate them.
"I'm sure he didn't mean it," Takao said with a nervous chuckle.
His intervention only deepened Murasakibara’s glare.
Midorima remained unfazed in front of this attitude. He wasn’t one to get intimidated, even in the rare occurrence the other person was a head taller than him.
“I said what I said.” Keeping his tone even, he returned the glare with equal force. “Now, if you aren’t planning on ordering anything, I’d advise you to step aside. Other customers are waiting.”
On his side, Takao facepalmed with a groan, and he could certainly swear Himuro stifled a snicker.
They remained locked in their stare-off until Murasakibara pulled back. Turning on his heels, he stormed out without another word.
Himuro apologized for the trouble and followed him, leaving the rest of the customers to glance between them in awkward silence.
“Now what?” Takao asked.
For once, Midorima didn’t have the slightest idea.
Several days passed and Murasakibara was still absent.
Midorima went about his shifts, as usual, trying to ignore both Takao's whining and his internal monologue about the whole affair. Their manager had been furious. But no one was more disappointed than Midorima for losing his temper over something this mundane. Personal feelings aside, he should have kept his professionalism as he had always done.
Of course, he wasn’t planning on apologizing if they met each other again. While it had been inappropriate to get into a fight with a customer, Murasakibara had started it with his rude unprompted commentary. The shop had other regulars so one's disappearance wouldn’t have any impact on their earnings. It was going to be alright.
“Pretty boy alert at ten o’clock,” one of the girls announced. All three of them had gathered behind the desserts and snacks display, giggling among themselves.
Midorima seldom participated in such idle gossip. It seemed pointless and distracting. Maybe if his colleagues found something else to pass the time, they wouldn’t need to stay overtime that often.
Unlike him though, Takao seemed to enjoy the social aspect of it. So after taking a peek, he slid into Midorima’s personal space with a conspiratory air about him. “Shin-chan, you might wanna take this,” he whispered, pointing at the spot of interest.
It was one of the tables next to the shop’s glass facade. Himuro Tatsuya was sitting all alone there.
“Why don’t you go?” Midorima asked, shelving the washed cups from the sink.
“Don’t be silly,” Takao said with a laugh. “We, average guys, have our pride you know.”
That was the most absurd thing Midorima had heard in a while. Takao was by no means average-looking, considering the amount of attention he got from both men and women. But he kept this thought to himself.
“Ask someone else.”
“Don’t be like that. If you won’t do it for me, do it for Minami and the others.” He grabbed him by the shoulders. “Fighting over a guy is an ugly thing. They might break apart! Think of their friendship! Their friendship, Shin-chan!”
There was zero proof of something like that happening. Even for a reserved person like Midorima, it was plain as day those girls were joined at the hip. But whenever Takao resorted to dramatics, he could only oblige to make him stop bothering him.
He sighed. “Alright.”
Taking his notepad along, he approached the table in question. Hushed whispers followed him, making wonder with half a mind if this was some kind of ploy. His horoscope hadn’t heeded any important warnings for that day. He had been prepared with the appropriate lucky item regardless.
Himuro noticed him only when he reached him. “Hello again.”
“Hello,” Midorima replied politely, still a bit uncertain from his joyful greeting. “What can I bring you?”
“There must be a misunderstanding?” He pointed at the cup on his table “I’ve already ordered. Your colleague there brought it to me.”
From behind the counter, everyone gave Midorima a thumbs up. It dawned on him then and there. This had been a set up from the start. Forcing him to interact with Murasakibara’s friend in hopes of learning about his whereabouts.
He resisted the urge to snap his pencil in half. Even his good looks wouldn’t save Takao from his wrath when he returned to the register.
“It’s alright. I can order once more,” Himuro said, appeasingly. “I didn’t have the chance to try your famed sweets last time after all.”
Swallowing his anger, Midorima returned to his work mode. “Is there something, in particular, you’d like?”
“Some of your macarons perhaps.”
“Excellent choice. We’ve got a new batch just today. These are made from this university’s Culinary Arts Department.”
“I know. One of Atsushi’s upperclassmen is responsible for them.”
Midorima looked at him as if he had grown another head. “Pastry chef is his major?”
“I’m surprised you hadn’t figured it out already, given how often he visits this place.” Himuro’s visible eye twinkled with hidden amusement. “He eats too many sweets and snacks for his wallet to handle. This hasn’t changed since our high school days, to be honest. The only difference is that now he started making his own, so we don’t have something to bribe him with anymore,” he said with a sigh. “It’s an uphill battle to bring him to practice lately.”
“Both of you are still playing, I presume?”
“Yes, with the varsity team.” Resting his chin against his knuckles, Himuro assessed him. ”I see you’re very informed, Mr. Midorima Shintarou of Impossible Threes.”
“I’m simply acquainted with an extremely nosy person,” Midorima said. It didn’t take long for Takao to learn about the rest of Murasakibara’s teammates after meeting Himuro. “Where you aware of me from the beginning?”
“I had my suspicions since you’re quite the urban legend around here. FYI, your taped fingers gave you away,” he said with a wry smile. “As someone playing in the same position, I was surprised to learn that such a high-profile player as yourself wasn’t playing anymore.”
“Such is life. Different priorities call for different measures.”
“That is true, I suppose. Do you miss it?”
The sun reflecting on his glasses erased the current view from Midorima’s eyes. He was on the court. Everything was silent; no shoes squelching against the wooden boards; no desperate cries for victory. He was holding the rough leather ball, preparing to shoot. The motion effortless and practiced to the finest tuning possible. He always exhaled when the ball left his hands as if spelling a prayer. It went in with barely a sway of the net. It always did.
“My time is limited for the effort the sport requires,” he said.
“That’s too bad.” Himuro returned to his coffee. “I wonder if Atsushi would be more motivated if he had someone of your caliber to compete against.”
"It must be nice being so simple-minded."
"Simple-minded, huh?" He looked wistfully outside. "That's not a word I'd use to describe him."
Midorima stopped scribbling in his notepad. "Meaning?"
"Sure, to an outsider, Atsushi might appear as such. He seems to go with the flow of his surroundings because that's the easiest thing to do. It might be partly true. It's rare to see him get truly passionate about something that doesn't involve his specific interests." He stirred his coffee. "But you managed to light that fire in him, even if for a single moment. That must amount to something, don’t you think?"
This is preposterous, Midorima thought.
Not everyone had the freedom to just do whatever they wanted, whenever they wanted. Usually, another obligation or circumstance would force someone to go against their wishes and that's how their society worked. One couldn't bend the rules as they pleased. No one had such total control over their life. Midorima definitely didn't and it made him no different than the next person. That's another fact he had accepted without a second thought. There was no way a boring person like him could influence someone's life to any degree, more so a person he had barely held an entire conversation with.
Shaking his head, he focused on the task at hand. "Will that be all?"
"Yes." Himuro smiled. “That’d be all.
The Friday afternoon shift was the quietest of the week. Students preferred to visit the nearest bar or karaoke box rather than the café. It was only natural. No one wanted to follow the same routine, more so during the start of summer vacation. Midorima simply enjoyed the opportunity to avoid interacting with any customers for once.
A storm had been brewing over the horizon for most of that day. So, after a while, Midorima told Minami to return home; criminally unprepared that girl, she never carried an umbrella. Her assistance wouldn’t have been necessary anyway. The shop was empty, allowing him to do some deep cleaning of the place with everyone gone. Halfway through polishing the tables, the rain started to fall outside; a gentle pitter-pattering on the glass ceiling at first, before the heavens opened up and unleashed their fury to the ground. This downpour accompanied Midorima for the rest of his tasks--a white noise lulling him into some peaceful trance. Nothing else mattered; not his gossip-loving coworkers nagging him; not that Murasakibara hadn’t appeared for over a week.
He had finished mopping near the entrance when the double doors rattled. The sun wasn’t bound to set for a couple more hours. Yet, the scenery outside was as dark as if night had fallen. Midorima couldn’t figure out who was out there, knocking at the door with such urgency. Leaving the cleaning supplies aside, he unlocked the door.
Humidity hanged in the air, pressing against his face like a wet blanket. “Is there something I can help--”
Midorima noticed the jacket, draped over a light-colored package the person was holding in their hands. Allowing his gaze to travel upwards, he took in their bulky torso which was clad in a drenched t-shirt. Locks of hair were glued on their cheeks and forehead like jungle vines.
Despite all that, Murasakibara appeared only mildly annoyed and maybe a bit out of breath. “Took you long enough,” he drawled.
“What are you doing?” Midorima asked.
“I came as soon as it was ready.”
Annoyance spread hot in his chest. “In case you haven’t noticed, it’s raining right now!”
“That’s why I covered it with my jacket.” He had the nerve to sigh. “For someone wearing glasses, you sure are blind.”
“Excuse me?” Still processing what just happened, Midorima had lost his usual eloquence. “You...it’s been days...and the first thing that comes out of your mouth--”
“Do we have to talk about it here? It’s gonna melt if it stays outside any longer.”
You should have thought of it earlier! He cried in his mind, allowing the other inside in the process.
His sandals squelched against the tiles as Murasakibara beelined for the counter, paying no attention to the watery footprints he was living behind.
Conjuring all his remaining patience, Midorima took the dripping jacket from his hands. “I’ll get you a towel,” he said and disappeared into the backroom.
When he re-emerged, the other had made himself comfortable on a stool. Miffed by his nonchalant attitude, Midorima threw the towel on Murasakibara’s head and took a seat as well. The package was left on the counter between them. Similar to the ones their sweets tended to arrive in, the unassuming beige carton box was definitely from the Culinary Arts department.
Murasakibara peeked from under the towel. “Are you mad?”
“No.”
“You look mad.”
“I simply want to know what your issue is, coming here in such a manner.” He pointed at the box. “What is this thing too.”
“Open it.” Shrugging, he proceeded to dry his hair. “It’s for you, anyway.”
Midorima quirked an eyebrow, more baffled by this development. Since he didn’t receive any further clarification, he warily opened the box. It was a cheesecake; specifically, a red bean cheesecake like the one their dispute had been about. Perhaps it was the sentiment getting to him, but he was oddly touched.
“You made this?” He asked softly.
Murasakibara hummed in agreement.
“I can't possibly eat the whole thing alone.”
"You can share it or sell it. I don't really care as long as you have the first bite."
"We aren't allowed to put unregistered or unordered sweets for sale,” Midorima said absentmindedly. “Since you went through the trouble anyway, I suppose it’s only fair I give it a chance. I can leave the rest for the others to try. Do you want a piece too?" Seeing him hesitating, he stood up and put the machines to work. “I’ll make you something warm to drink. Summer colds are horrible to catch, especially this time of the year.”
“Yeah, sure.”
It didn’t take long for the hot chocolate to get ready. Meanwhile, Midorima found something else for Murasakibara to change into and leave his shirt to dry. As a future doctor, it’d be criminal to let someone get sick in his presence. He also dealt with the dessert, cutting two slices for them and putting the rest of it aside in the freezer. All the while, Murasakibara followed him with his gaze as he moved about like a busy bee. Midorima would prefer to renounce his lucky item of the day than admit he had missed the comfortable silence between them. In a world where everyone seemed eager to involve him in things, this moment was an oasis of tranquility.
“Alright,” he said placing the cup in front of Murasakibara.
“You won’t drink anything?”
Midorima returned to his seat. “I’m not one for sweets.”
“I thought you might have one of your canned red bean soups along with this.” He blew at his cup with an indifferent expression. But his eyes seemed to search for a reaction. “Why red and not green beans, by the way? Considering your hair.”
“I don’t mix those two.” Cutting his fork into the slice, he brought a decent-sized portion to his lips. “It’s unsightly.”
Whatever he might have wanted to add, drifted from his mind after taking that bite. It was leagues better than anything Midorima had eaten so far. Compared to this, his regular Wednesday slice might as well be from the lowest shelf of the bottom-ranked convenience store’s fridge.
“You liked it,” Murasakibara said.
It wasn’t a question, and for once Midorima didn’t feel like arguing.
“I accept my defeat,” he said with grave seriousness. “Why did you have to go through such lengths, though?”
“To prove you wrong.”
On second thought, pettiness was an acceptable reason. “I work here. There was no need to get personal.”
“Yeah, but you did.” Draping the towel around his neck, he tied his hair into a low ponytail again. “It was the first time Mido-chin reacted so strongly about anything.”
“I don’t believe we’ve been properly introduced to make nicknames for me.”
“I read your tag,” he said as if it was obvious.
“You’d be surprised how many people can’t do so. But that’s beside the point,” he said with a wave. “Emotions aren’t needed to do my job. In fact, this whole situation brought me a lot of trouble.”
“But you don’t look so dead inside anymore.”
Taken aback, Midorima was speechless.
“It’s true,” Murasakibara continued. “I know you don’t have to talk a lot and I didn’t mind. It made things easier for me too. I didn’t have to think about what to say back like with the others. But with nothing else to do, I watched you from my table. The only time I ever saw you enjoying yourself were in your breaks, sipping canned red bean soup in the corner, or whenever the others tried to pull you into their shenanigans.”
“I certainly don’t appreciate them making a fool of themselves in front of the customers.”
“You’re lying.” He leaned closer. “And when it’s not those moments, you’re like a beast. Pacing in the cage you made for yourself. Like you’re waiting for something. Why are you still tapping your finger if aren’t playing basket anymore?”
Clenching his fist, Midorima didn’t back down. “Let’s say you are right, and that’s purely hypothetical. What’s in for you?”
“Passionate but talentless players annoy me. But talented players choosing to give up annoys me even more.” Murasakibara sat down, his expression turning solemn. “They remind me of something I’d rather forget.”
This statement echoed personal and all too familiar. Midorima wasn’t someone that poked into other people’s business, not actively at least. Still, he could understand the sentiment. Sometimes, in the dead of night, he’d ponder over his current course in life and get mad at himself; for not pushing through harder; for leaving something he loved aside without much thought. Maybe this was finally the chance he’d been waiting to come.
“Say,” he said; his throat dry and his words timid, “if I challenged you into a match, would you accept?”
“You’re deaf as much as you’re blind.” The jab had not actual heat behind it though. “Yes, without a doubt.”
“With that settled, I hope you won’t hold back. Otherwise, I’ll obliterate you.” His ever-bored eyes widening, just a smudge, got Midorima a bit self-conscious. “Is something the matter?” he added.
“You surprised me,” Murasakibara said, rubbing his neck. “That’s the first time I’ve seen you smile, I think.”
“I simply enjoy a decent challenge.” He took another bite off his slice of the cheesecake. “Don't you?”
The other considered it for a moment. "Only when I know I'll win."
It roused another round of pointless bickering. But, truth be told, Midorima hadn’t felt more alive in while.
#knb#knbsecretsanta2020#midorima shintarou#murasakibara atsushi#takao kazunari#himuro tatsuya#knb fanfiction#knb fic#fanfiction#fanfic#coffee shop au#college au#coffee shop/college au#did I channel my feelings about work through Midorima?#yes definitely#those fantasies were the biggest reason I tried to write a coffee shop AU for the first time in my life#too hilarious of an opportunity to pass XDD#wolfswriting
4 notes
·
View notes
Text
I am overwhelmed.
I have lots of family on Facebook, so I generally don’t post stuff like this there. On my Twitter, I occasionally share short-form woes, but didn’t really want to put this there.
There is so much going on in the world. In addition, there’s so much going on in my life. So much feels like it’s piling on. And, before anyone might ask, YES, I’m seeking therapy. I’ve recently had to switch therapists and am still waiting on an appointment. But I AM seeking real help. I just need a place to shout into the void, and I’ve got some H E A V Y shit to share.
My mom has been in increasingly poor health. She has COPD, has had dozens of hospital trips in the past year, and has been on oxygen since September. That came out of nowhere. She hadn’t been hospitalized in something like 15 years for her COPD, and then WHAM, so much deterioration happened at once.
She receives palliative care, which is basically a step below hospice care, for those who don’t know. Palliative care is when you have a serious medical illness, and a nurse comes by a few times a week to check vitals, give you a basic examination, and is able to advocate for you more easily. If they suspect an infection, they can call your doctor for you and get antibiotics ordered without needing to go to the doctor’s office. It is designed to save you hospital trips, because your immune system is at risk of ANYTHING you come across.
My mom was told, last week, that she is in the end stage of her COPD. We were preparing for this, it was suspected, but it was different to be told that for sure by the doctor. Home hospice care was recommended for her, despite her already having palliative care. This is probably because palliative care still has more hoops to jump through to gain access to higher strength pain management medication, etc.
She also recently developed 4 compression fractures in her spine. T4, T5, T6, and T8. She has osteoporosis and RA. She has a brace for this so her spine can heal. She has a hunch now because of the fractures, and the hunch is permanent.
This hit me like a TON OF BRICKS. Anyone who knows me, knows my mom is my best friend on this entire planet. Yes, my dearly departed best friend Toni, and my Rachel Squared bestie are my best friends. But, I am SO incredibly close with my mom. I tell her everything, even the uncomfortable stuff that people often don’t share with their parents. Losing her would be unfathomable to me. And, yet, I have to start accepting that it may happen sooner, rather than later. Yes, she could live a very long time in the end stage. That doesn’t have to define her. Some people still live 10-20 years. But the vagueness of the situation is what eats at me. Could she live another 10 years? Of course. But would it be a surprise to any doctor if she passed in a few months? Not at all. And that’s what eats at me. I don’t want to live every day thinking that this is going to be the day I lose her, but my anxiety takes over and I do think that.
She just went back to the hospital the other day, for what we thought was a bowel obstruction. She hadn’t gone since she got home from the hospital last week. Nope. Not an obstruction. Good, right? Well...she had a HOLE in her INTESTINE. Part of her intestine is just paralyzed and not working, likely because of this perforation. So she had to have emergency surgery. It was successful, but recovery could take 6+ months, and she has an ostomy bag for at least a few months.
I’m glad she’s okay. I talked to her this morning. But, of all people these things happen to, it shouldn’t be her. My poor mom has been through hell and back. And, somehow, she’s still positive and SUCH a trooper. And it makes me sob. I love her so much and would bear all the pain for her if I could.
Besides my mom’s struggles, my son has a developmental delay, isn’t saying words, (but makes noises and single syllable sounds) and will be 2 this month. He’s being referred for autism screening. I love my son, he’s ADORABLE and is such a good kid. But the hard times with him are HARD, and it’s becoming harder and harder to manage on my own. (COVID still has things closed, and his Early Intervention visits are all teletherapy currently) He’s also got partial hearing loss, that we’re unsure is permanent or not. COVID has prevented him from seeing ENT until the end of July. All we have to go on right now is from the audiologist. He doesn’t hear until 35 decibels, and that’s a whisper for him. He has Sensory Integration Dysfunction, and seeks out sensory input he’s not getting. This results in him pushing over heavy furniture, which appears to be destructive behavior, but is him trying to participate in heavy play so his senses are stimulated. Reid is the light of my life, but it is exhausting. I will love him no less if he’s autistic, but I grew up with developmental delays myself, and it’s not a life I necessarily wanted for him. I don’t want things to always be harder for him. I want things to be easier for him than they were for me.
And, I’m filing bankruptcy due to massive medical bills from 2018. Basically, I worked at Cigna, and while I was pregnant, I had medical problems that didn’t affect Reid, but affected me, leaving me out of work. I had short-term disability from December through the middle of February. From February through May, I was supposed to have FMLA, and then from May-September was supposed to be maternity leave. I ended up leaving in September because I couldn’t afford to work and pay for childcare. Because I left, it caused a catalyst. FMLA retroactively denied, which caused my maternity leave to deny, because FMLA needs to be approved for maternity leave to approve. Because none of this approved, my health insurance from February-September essentially went retroactively unpaid. Because that happened, my insurance coverage terminated all the way back to February. Cigna recouped all the payments they made for ALL my health issues, and Reid’s birth, etc. So 6 months of insurance premiums AND every single doctor charge was on me. AND, to make matters worse, too much time had passed for Medicaid to pick up any of these bills. (You can only submit bills that are within 3 months.) So, I’ve been saddled with an insane amount of medical bills I just cannot pay.
I have multiple medical issues that require surgery. I require bladder surgery, and hip/pelvic surgery to correct dysplasia. My doctors won’t do it until I’m done having kids...all because I want one more in a few years. The pain and dysplasia with my hip/pelvis/low back prevent me from doing a lot of bending, walking, and lifting. This prevents me from doing much around the house. I feel miserable, like I’m useless and not enough of a person for my partner, because I’m not contributing as much as I feel like I should. If I clean the house, I can’t do anything else for the whole day. If I walk through a Sam’s Club, I’m done for a day or two. It’s a bad mental space to be in.
Sooooo, that’s my life right now. Then, add in touch deprivation because of the pandemic depriving me of the people I love. Add in my dread because of the state of the world. (#BlackLivesMatter, kiss my ass if you disagree) Aaaaand, I’m a million degrees of overwhelmed.
11 notes
·
View notes
Text
Atypical/Elliptical.
There was a tweet highlighted yesterday by one of the Neuro-Divergent accounts I follow, building pace on the back of a compare/contrast photo of an autistic female, and an autistic male. If you haven’t seen it, you can guess how it went, she’s all cute and ‘sailor suit’, he’s in a cluttered room, overweight, in food-stained clothing. Lazy stereotyping at best, offensive and dangerous in reality. The dangerous tweet I reported was one from a contentious incel, stating that females don’t have autism, further down the page of “Would you like to report any other tweets?”, we have that other old favourite “Autism isn’t real.” Yes, I’m shaking my head.
I’m not going to go into in-depth analysis of incel beliefs and values, I’ll just hover over the suggestion that this particular variant was whipping up his followers that ‘Women don’t have autism’, based on his interpretation that the female whose picture he was using was conventionally attractive, and neatly presented. If you tell someone the sun’s 93 million miles away, they accept it, but if they see a sign saying ‘wet paint’, they feel compelled to put their finger in it to check, then complain that they have paint on them. (I know, I don’t touch wet paint, I lick it, it keeps life interesting.) ‘Everybody knows’ that a common feature with autism is the special interest, that we will fixate obsessively on a certain topic, or subject, and woe betide any mere mortal who can’t escape before we get into full flow, what with us not always picking up on non-verbal cues, like snoring. It’s entirely possible that the ‘girl’ had a special interest of dressing and presenting herself in a certain way, even ‘normal’ people do that, hanging their entire identity on presenting a certain way, designer clothes, certain styles of dress, Angry Bird eyebrows. Step back, and absorb that, the girl wasn’t ‘properly’ autistic because she didn’t have food in her hair, wasn’t wearing a Star Trek uniform, looked ‘normal’. Specifically, she looked the kind of ‘normal’ that incels have experience of being rejected by, because they expect to have nice-things handed to them on a plate, and then blame everyone else when they’re denied. There’s a certain example of a petulant, pouty individual, who sulks when they don’t get their own way floating to mind.
Using the newfangled terms neuro-divergent, and neuro-typical, and pausing just for a second to point out that no, we’re not ‘all a bit autistic’ any more than we’re a ‘bit vegetarian’ or a ‘bit left-handed’, neuro-typical people are assumed to be the norm, anything else is deviant. I’ll hold my hands up to that, I don’t iron my laundry, or peel my vegetables, you can stop clutching your pearls, I’m not going to steal them, what would I want pearls for? People with neurodevelopmental disorders are atypical, outsiders, outliers, ‘other’, and it’s more than a little annoying that ‘everyone knows’ that, specifically autistic people, have a tendency to see themselves as different from others. (You started it, telling us we were wrong and weird for our plethora of sensory aversions, and routines, just because they don’t make sense to you.) We’re atypical, whether that’s because we’re genuinely distressed if our ‘usual’ brand of socks, or cereal, or soap is discontinued, or because we won’t cross the road if the light isn’t green, even if there’s nothing coming. Other examples are available.
I’ve spent vast chunks of my life being bounced between “Why are you doing it like that?” and “HOW do you do that?”, I don’t have any savant-skills, but I’m on an elliptical axis, I do some things differently. (The axis isn’t just elliptical, it’s occasionally highly irregular, I have multiple other medical issues, autistics are often blessed like that, to the untrained eye, it might appear I’m neurotic, or hypochondriac, or do my shopping on NHS direct. I’m an unfortunate combination of chromosomes and chronology.) You neuro-typical types bimble along happily enough on your spherical orbits. Yes, you have spikes, too, I know, but it seems that they’re the exception rather than the rule, your orbits appear far more regular than mine. I’m deviating from all-autistics, to ‘me’, there are common factors, but we’re not a one-size-fits-all contingent, I don’t get upset if different types of food touch on my plate, but I can’t use oven-gloves, and I’ll go all day without a drink of water rather than share a drinking vessel, we’re all different.
I’m sometimes envious of the spherical orbit, the regularity of being able to remember to prepare and eat three meals a day, not being afraid of bridges, being able to choose a direction and travel in it without sensory overload, it might as well be necromancy or Olympic level athleticism, it just isn’t ‘there’ for me. When my orbit is within ‘yours’, I’m highly efficient, that’s the “HOW do you do that?” phase. I just do. There isn’t really much of an alternative, but it’s not very healthy, I have all of your weird scripts and rules tumbling around my head, like that stage where you’re learning a new language, everything has to be double-processed, and checked, it’s clunky, not fluent. I’m 43, and I still don’t dream in your language, I can concentrate for periods, but remembering all of the verb endings tends to kick the tenses out of the window, we’re no longer congruent, and I don’t make sense to you.
When I’m within your orbit, I take short-cuts, as verbose as I am here, I omit the unnecessary, because I don’t have the cognitive or physical energy for all of it. I’m a flat-pack item of furniture, I don’t need ‘all’ those screws and fixings to be functional, do I? I unintentionally infuriate and antagonise, because I don’t want to stop for a cup of tea, or chat about TV programmes, I want to complete the task set, before I run out of energy. (I know, but the externally imposed sanctions for non-completion generally have a ripple-out impact on others. My intense bursts of activity alienate other people, because they want to slow down, and chat, but that’s not the task in hand, and I know that my brain and body are temperamental, I *need* to finish within time, and properly, in case I’m less-functional the next day, I always stacked/banked work to make sure I was ahead of myself, to avoid letting other people down if I was ill.)
When our orbits converge, it’s phenomenal, on a ‘work’ level, a life-admin level, or, that holiest of Grail, an interpersonal level, those brief instances are stellar, apart from me freaking people out by my intensity sometimes, I’m an acquired taste. I’m really good at some things, a large proportion of which have yet to demonstrate a particularly useful potential, but there’s time yet. I’m steering very firmly away from the lazy stereotypes of ‘special talents’, I’m resilient and resourceful because I have to be, I often view things from an alternative perspective, and connect-the-dots that others don’t. I still can’t use oven-gloves.
When my orbit swings outside yours, it’s difficult, sometimes impossible for aims to be reconciled, That’s the kick in the teeth on a regular basis, last week, or last month, or yesterday, or earlier today, I might have been functional, or even brilliant, then, all at once, I’m not. “You were fine yesterday!”, yes, I know, I was there.
Chromosomal and chronological factors sometimes spin me out of orbit. I might have been able to walk to Tesco one day last week (Coincidentally, I wasn’t, but that’s not the point.), that doesn’t mean I can do it every day, it’s a cross-over complexity with my telephone directory of other ailments, as well as the autism. When I’m out of orbit, whether it’s sensory overload, burnout, or just my day-to-day ‘wrongness’, I process differently. A ‘normal’ action, like parking a car (I don’t know why I use driving analogies, I’ve never taken my test.) becomes a pantomime of a driving test, where the instructor speaks a foreign language, it’s an unfamiliar car, on unfamiliar roads, and the car’s on fire, and full of wasps, with an angry pig in the back seat. I don’t have muscle memory, or subconscious competence for a lot of functions people take for granted, not just oven gloves, sometimes events conspire to throw me out of spherical orbit, and everything becomes far more complicated than it needs to be. The elliptical orbit makes ‘just’ my ultimate four-letter word, and I know plenty of others. Some instances of being out-of-orbit are predictable, sensory overloads, other illnesses, compounded difficulties around other life-events, my toe having poked through my sock, and being strangled in my boot, it can feel like being an adult-sized toddler, and the temptation to throw down and scream on the supermarket floor because I’m tired is an unwelcome, but regular occurrence.
“Oh, we all get like that sometimes! Can’t you just...?” If I could have ‘just’, I would already have ‘just’, wouldn’t I? 43 years of having been chastised for being difficult, or ruining everyone else’s picnic feed very firmly into the ‘masking’ phenomenon. Charlatans and snake-oil sellers, and Gwyneth Paltrow, as well as even more insidious practitioners are always trying to promote some thing or another that will make us fitter, healthier, more productive, then, to continue the Radiohead theme, many medical types throw back “You do it to yourself.”.
Autism is a lifelong developmental disorder. I can’t consistently ‘try to be less like that’ any more than I can try to be less right-handed, or biologically female. (Yes, I *could* attempt to alter both of those, but to what end?) I’ve had a lot of medical interventions since the brain aneurysm ruptured, and 99% of them have tried to un-autistic me. That’s normal, because autism is abnormal. It’s also normal because autistic females broadly present differently to males. Broadly, I have observational experience from working in education, the ‘old’ perspective was that boys were more frequently autistic than girls, and, more-autistic. Slight tangent on the common misconception of the autistic spectrum, if I may? “We’re all a bit autistic, haha!”, no, no, we’re not, any more than we’re all a bit epileptic. The autistic spectrum isn’t a continuum-spectrum, from 0-100% autistic, while it is clear that some people are severely autistic, and others are not, it isn’t actually a point-scoring exercise, unless you’re UK benefits agencies.
Males and females are conditioned and socialised differently, after millennia of girls-do-this-boys-do-that, humanity is cautiously asking why. I’ll leave my wonky femininist soapbox under the desk, apart from the fact that females are ‘supposed to’ be quiet, and kind, and compliant, and all the gubbins that the incels say. I’m 43, I was raised pink-for-girls-blue-for-boys, there were a lot of things Girls Didn’t Do, it’s OK, I’ve done most of them now, don’t tell my Dad. Much like left-handed children in days gone by were forced to write with their right hand, there has been, and still is, to some extent, pressure on males and females to behave differently, as if keeping our reproductive paraphernalia in a more-or-difficult-to-kick location is an absolute-for-everything. I don’t think it is, but we’ve already established I’m atypical. Not all 40-something-year-old people, with, or without autism had the same childhood experiences I did. There’s no place for detail here, some of the embedded lessons weren’t kindly taught. That Pavlovian response system stuck, be quiet, be pleasant, be demure and train that flinch into a smile. (Various parties ought to apply for funding for having ‘tamed’ this particular shrew. I’m not tamed, I’m barely even domesticated, but I have a shed-load of coping mechanisms.)
Females shouldn’t feel the need to be less-than, to defer to males, but, in a disturbing number of arenas, that’s the norm. I spent the largest part of my life being afraid of men, because of what some men had done, and hating myself for holding a belief that was anathema to the absolute core of my being. (Chapter whatever, fundamentally knowing that males were not ‘better’ than females, but feeling obliged to concede, to avoid disturbing the peace.) The #MeToo disclosures and discourse picked that metaphorical scab, I’ll never go back to that half-life.
I’m atypical because, after decades of excruciating path-of-least-resistance masking, I’ve managed to mask proficiently to a point where I can ‘act normal’ for short stretches. I shouldn’t have to. I’m not suggesting I should be allowed to climb on top of the curtain poles, and throw things, but I don’t see why not-acting-feminine should be seen as disturbing or threatening. It hurts, not just the bras, and the stupid shoes, and the sitting-all-cramped-up, but the emotional and physical toll of carrying oneself ‘female’. When I had the full spectrum cognitive functioning assessment after the brain injuries had settled, the neuro-psych pointed out that a consideration was always ‘At what cost?’. The popular analogy for physical or cognitive energy is a ‘battery’ (A cell, doofus, a ‘battery’ is a number of cells together- behold, I’m reaching my cranky-pedantic cut-off stage.) In order to do anything at all, you need enough ‘charge’ to complete the task. Yes, given, BUT, with autistic masking, there isn’t just the ‘charge’ for the task, there’s the additional charge involved in keeping everything else running, without breaking down, or burning out, the energy overdraft. I’m virtually constantly in my ‘overdraft’, and it’s a bitch to pay back.
I’m elliptical because I frequently swing inside, or outside a typical orbit, I can be ‘miles ahead’ at some points, but ‘miles behind’, and struggling to keep up at others, it’s not a reliable pattern, I can’t predict all of it, and I am SICK of well-meaning “Oh, don’t be so hard on yourself!”. I’m rarely being ‘hard’, I’m usually being practical, if I do x and y on one day, I won’t be able to do z as well. (”Don’t call yourself disabled!” can be a blog for another day.)
This has been an attempt for me to shake myself out of a fog of not-writing. Autism is opaque and oblique, it can be brilliant at times, when things ‘click’, but it’s almost-always difficult to articulate in a way that’s palatable, let alone digestible, I know, it sticks in my own throat enough. The ‘experts’ trot out their theories, sometimes without consultation, and the organisations that set out to ‘cure’ us are pedaling the myth that autism is a disease. It’s not, it’s a divergence. Take this as ‘A Portrait of This Autist’, I can’t speak for anyone else, but I do think it’s important to speak.
1 note
·
View note
Video
youtube
(via "Medically Futile Care" As Ritual. I Fucking Knew It. And People Are Okay With This?)
I’ve been researching so-called “medically futile care” lately, or more accurately, it’s a rabbit hole I fell down while researching nursing and what nurses have to say about witnessing and participating in medically futile care, otherwise known as medicalized torture. My own mother is a nurse and I know that she, after being a nurse for some 30 years, started to become disillusioned by Western medicine and the horrific procedures and treatments imposed on intractably and/or terminally ill and actively dying patients. Of course, she didn’t start having a problem with it until after she had reaped the social and material rewards of being a disgusting handmaiden and middle class patriarchal enforcer for her entire adult life including subjecting her own children to medicalized torture: my own brother died from it and earlier this year she brutally criticised me for abandoning Western medicine after 2 years of conventional Crohn’s treatments that were not helping and only making me worse. With a Western medical nurse as a mother who needs a firing squad (or torturer) amirite?
https://youtu.be/ujANeiNYHU8
I have written here before about disillusioned Western medical doctors resisting their evil profession by leaving the field, including leaving via suicide. Apparently there is currently a movement headed by Western medical doctors themselves to challenge abusive practices in their field including but not limited to hazing and domination rituals in medical school and medical residency; overwork, sleep deprivation and other conditions related to employment in the Western medical field; and cruel standards of care including those implicating medically futile care where doctors feel “forced” to literally torture sick, injured and otherwise vulnerable patients lest they lose their jobs or be sued for medical malpractice. Doctors are actually feeling sorry for themselves because their jobs as patriarchal enforcers and medical torturers makes them feel bad, and while anyone who has ever worked before knows what it’s like to be coerced for money (and survival) those who literally, physically harm and torture other people in order to maintain their own standards of living will garner no sympathy from me.

The same goes for Western medical nurses who my research indicates suffer greatly from vicarious trauma and professional burnout from “having” to witness torturous medically futile care in their professions. Examples of such care include flogging corpses which have no reasonable chance of being revived; continuing invasive so-called “life support” for those who are dead to the world and will probably never regain consciousness or if they do will be horrifically and permanently impaired; refusing to let extremely premature or terminally malformed or diseased infants die naturally, and so on. Get a real fucking job, no matter how low it pays, is my response to all medical professionals who have a problem with physically harming and torturing people…yet continue to do it anyway because some man somewhere tells them they have to lest they lose their jobs if they want to continue to fund their own middle- to upper middle-class lifestyles. Seriously fuck you a million times you poor, poor self-proclaimed victims of workplace abuse who continue to physically torture vulnerable people for money. You absolute monsters.
As a chronically ill person suffering from an incurable and progressive disease that is notoriously unresponsive to conventional care, I recognized awhile ago that for me to engage with Western medicine when it has nothing to offer me in terms of pain and symptom relief or a net increase in my quality of life (net meaning overall, or a positive rather than negative score in benefit-minus-risk) would be nothing more or less than an engagement with a patriarchal ritual, and one that as a radical feminist would give me no comfort. Because I see no objective or subjective value in participating in patriarchal rituals I have declined to use the doctors’ office as a confessional, to confess my sins of being a disabled female under capitalism and patriarchy to a patriarchal authority figure who can do absolutely nothing for me except to witness my confession and absolve me of the emotional burden of being sick in the first place, and medically noncompliant in the second. That is literally what Western medicine is to me now — a patriarchal ritual — and I reject that on its face as a female who is deliberately denigrated and harmed (not healed) by patriarchy and patriarchal rituals by design.

Well come to find out this business about Western medicine and medically futile care in particular being a patriarchal ritual has been described by other people and wasn’t just something I and other radical feminists have made up in our heads: researchers actually admit it’s true in a medical journal article entitled “Rituals, death and the moral practice of medical futility.” Of course, they frame the use of ritual in this context as a positive thing. Here is the abstract of that article:
“Medical futility is often defined as providing inappropriate treatments that will not improve disease prognosis, alleviate physiological symptoms, or prolong survival. This understanding of medical futility is problematic because it rests on the final outcomes of procedures that are narrow and medically defined. In this article, Walker’s “expressive-collaborative” model of morality is used to examine how certain critical care interventions that are considered futile actually have broader social functions surrounding death and dying. By examining cardiopulmonary resuscitation and life-sustaining intensive care measures as moral practices, we show how so-called futile interventions offer ritualistic benefit to patients, families, and health care providers, helping to facilitate the process of dying. This work offers a new perspective on the ethical debate concerning medical futility and provides a means to explore how the social value of treatments may be as important in determining futility as medical scientific criteria.”
Oh by all means, let’s remove the expectation that medical care provide positive “final outcomes” for the one being subjected to it — the patient. Because to ignore fail to extol the broader social function of torturing sick and dying people in a medicalized authoritative setting would be problematic, you see. Do you see what they did there? They are talking about social engineering and the effects on society at large of flogging corpses, equating zombification/maintaining a state of undead with “life support”, and spitting in the eye of natural law by refusing to allow congenitally unviable infants to not-survive infancy and so on. And while the abstract does not list or detail the alleged benefits, the writers believe the social engineering effects are positive. Sure, if the reader is one who benefits from collective trauma and trauma-based mind control among other things. The rest of us, I suppose, are just expected to adopt the perspective of our oppressors.
These medical researchers aren’t even hiding the fact that most if not all medically futile including end-of-life care is ritualistic and does not benefit the patient. They assert that it is not intended to and should not be intended to benefit the patient because why waste an opportunity for social engineering and propping up medical (patriarchal) authority by “facilitating the process of dying” as if natural law needs their help? This is megalomaniacal.

The shit icing on the cake may even be that these researchers used a woman feminist’s ethical framework in order to justify using patriarchal authority as social engineering in cases of intractable illness and injury, including at the end of life. They rely on Margaret Urban Walker’s Moral Understandings: A Feminist Study in Ethics, published in 1998 which is described here:
The central concept of Walker’s work is the development of the expressive-collaborative model of ethical discourse. The expressive-collaborative model is a participatory model that engages people of all different kinds in a deliberative process that develops shared morality for a community. She develops this model as an alternative to the theoretical-juridical model [which model is a top-down authoritative model that assumes a universal moral code applies and does not accept input from the community it asserts moral authority over.]
Of course, assuming Walker is actually a feminist, she is proposing an alternative to patriarchy and providing an entrance for women and feminists into ethical discussions surrounding social policy and practice that disproportionately negatively affect us.
But her work is not used here to challenge patriarchy, quite the opposite. These prick researchers appear to use Walker’s alternative feminist ethical framework to support the use of medicalized patriarchal torture as ritual and beneficial social engineering…why? Because men and Western medical doctors should be included in the creation of social policy and practice and to not include them would be unfair because they are part of the communities they serve? (Have we hit peak liberal feminism yet?) Because using the bodies of sick and dying people to literally send messages to other people is perfectly fine? You’ve got to be fucking kidding me, considering that men in general and Western medicine in particular, as a fundamental patriarchal institution, already wrote the whole show including the foreword, the afterword, and the credits — and have used women and women’s bodies as useful objects the whole time. The world is their stage, the rest of us only players, yet we mustn’t disallow men and patriarchal institutions their voice literal actual physical abuse because not only ethics, but because feminist ethics. Got it.
youtube
Did I mention that I was right about medically futile care being nothing but a patriarchal ritual that can only harm women because that’s what it’s intended to do? Yep. I absolutely did mention it and I will again. I have also discussed how sick women’s bodies are in fact used to send messages to other people, in the case of requiring women to accept harmful and misogynistic Western medical treatment in order to collect disability benefits, the message is comply or literally die. Of course, I also framed Western medical treatment of untreatable, incurable and progressive disease as medically futile care which for some people is probably controversial but hardly a stretch if you just think about it a little bit. Goddammit I hate being right all the time.
https://youtu.be/Auxn2VAdiKI
3 notes
·
View notes
Text
RHR: The Shift from Treatment to Prevention, with Vipul Vyas, Locke Ettinger, & Pat Charmel
In this episode, we discuss:
What the U.S. healthcare system focuses on
The cost of maintaining this system
How conventional medicine got to this point
How the healthcare landscape is changing
The shift from “sickcare” to true healthcare
How employers can help employees manage their health
The social factors that impact health
Show notes:
The Heritage Victor Valley Medical Group’s Heritage LifeFit program
Griffin Health hospital
Unconventional Medicine by Chris Kresser
youtube
[smart_track_player url="https://ift.tt/2KCklXi" title="RHR - The Shift from Treatment to Prevention, with Vipul Vyas, Pat Charmel, and Laura Conley" artist="Chris Kresser" ]
Chris Kresser: Vipul, Pat, and Laura, thank you so much for being with me today.
Vipul Vyas: It’s a pleasure.
Pat Charmel: Appreciate the opportunity.
Laura Conley: Thanks, Chris.
Chris Kresser: So, I’m really looking forward to this conversation. Most of the discussion that I’ve had around this topic has been with people who are working outside of the conventional medical system. And certainly those perspectives are valuable, and I think we all agree that we need to make significant changes to the current system. But what I’ve certainly come to realize over the past several years is that while Functional Medicine on its own can make an impact and people working in private practice and using that model can make a difference to really scale this and have the impact that we need to have on a population health scale, we need to change the system from the inside out. And that's why I'm so excited to have this conversation today.
So let’s start with the first question. Where has healthcare historically focused and what have the traditional economic drivers of healthcare been in the U.S.? Pat, if you could get us started, that would be great, and Vipul and Laura, if you want to jump in, feel free.
What the U.S. healthcare system focuses on
Pat Charmel: Well, thanks, Chris. Obviously, the U.S. healthcare system has been focused on, or at least the bulk of the resource allocation has been focused on, for the delivery of acute care. Let me just sort of talk about it more generally. Most of the focus is, when we talk about spending in healthcare, and the costs compared to, say, other industrialized countries, it’s been looking at the more expensive inputs. Things like hospitalization, for instance, or high-cost pharmaceutical treatment. And if you look at the U.S., our model has been focused essentially on taking care of sick people. And the incentives in the system pay higher for those more complex interventions.
Has conventional medicine finally seen the light? Find out how some progressive leaders in hospitals, primary care groups, and corporations are driving the shift from treatment to prevention.
So, whether it's high-cost diagnostics, or whether it's complex surgery, or it’s the treatment of acutely ill patients with higher complexity … And so our system has actually focused on that and built capabilities around that following those incentives. And we do that pretty well, although some would say it may not be as efficient as it should be and it's not as consistent as it should be because there’s still a lot of variation around how we take care of sick people. And because of that variation, there are some differences in terms of cost and quality in terms of outcomes between organizations. But generally speaking, we do that pretty well.
Chris Kresser: Right.
Pat Charmel: And again, I'm sure we'll talk about the fact whether that model is viable long term because most of the focus has been on raising questions about whether that’s sustainable or not.
Chris Kresser: Right. So our system’s been primarily, it sounds like, focused on acute care, acute interventions. If we look at disease on the spectrum where you have perfect health on the left and death on the right, it’s a system that really, it does a pretty good job at intervening at the far right end of that spectrum. People already have disease and they’re already at the point where they need that kind of acute care.
Pat Charmel: Right.
Chris Kresser: So let's actually talk about how sustainable that is and how the these economic drivers are changing. Where are we at here in 2018 with the system that we have?
The cost of maintaining this system
Pat Charmel: Well, let’s talk about how the system gets paid for in the U.S., and we can get into the specifics in terms of our ability to treat disease because that's where most of the innovation has been, whether it’s been in terms of devices or pharmaceuticals, and we can talk about the cost of those inputs here versus elsewhere. But the question of sustainability, the cost of providing that kind of care, has been growing faster than the capacity of the individuals that pay for it to actually pay for it. So who is that, right?
So we’re talking about government if it’s the care of the elderly, the Medicare program. And if it’s the care of the indigent, it’s states and the federal government, right? So, through the Medicaid program. And then the rest is essentially employer-provided healthcare through those who work for employers who provide health insurance coverage. And our system has been one of cross-subsidies. And it’s not something that gets talked about a lot, but generally speaking, when the government buys healthcare from providers, doctors, and hospitals, it essentially pays less than the actual cost of providing that care.
Now you may say that the cost is higher than it should be, but the cost is the cost and they pay less. So the employer-provided insurance is through commercial insurance companies, and generally speaking, they pay more than the cost. And it’s not insignificant. It’s 30, 40, 50 percent more than the actual cost of that care. So the cost of delivering that care by the provider, the commercial insurance pays much more than that because they’re subsidizing the cost based on the shortfall by government payers who pay less.
Chris Kresser: Right.
Pat Charmel: And that was kind of something that everybody knew about and everybody agreed to. But costs have continued to grow, and the gap between what government pays and the actual cost is growing, which means the subsidy for commercial payers is getting larger. So the only way that the commercial payer can sort of shoulder that burden is to push that cost onto employers. And employers have complained about it for the last 20 years but have accepted it. But in the last four or five years, they have said, “Look,” especially after the economic crisis in 2007, 2008, they really started to say, “We literally do not have the capacity to pay this. Our profits have shrunk. We can't afford this. We’re not competitive compared to foreigners who don’t have to shoulder this burden.”
So what did they do in response? They could’ve said to the health insurers, “We are just not going to pay this and you’ve got to figure out another way to buy care less expensive than what we’re buying now.” But no, they didn’t. In the short term, they pushed more of the cost onto their employee in the form of higher deductibles or higher share of premium, right? So, the average employer in the U.S. is asking its employees to pay 30 percent of the premium. In addition to that—and that premium for a family policy, by the way, could be as much as $20,000 and sometimes more—and then after you pay your 30 percent of $20,000, or $6,000 in payroll deduction, in an environment where wages are not growing, you're actually seeing an increase of what you're paying out of your weekly pay toward your share of the premium. That’s a problem. Then once you pay that, you get the privilege of having a $3,000 or $5,000, or even more, deductible, which means that your insurance coverage that you paid for through your payroll deduction doesn’t kick in until you’ve paid $5,000 out of pocket.
Chris Kresser: Yeah, and then depending on your plan, sometimes you still have a copay after that.
Pat Charmel: On top of that. So now the average employee that has employer-provided health insurance is paying $0.42 of every dollar out of their own pocket. So the question is, is that sustainable? That’s what’s really changed is that employers couldn’t afford it, so they pushed it onto the employee. The employee is saying literally, “I cannot afford this. I don’t want your health insurance.” And the penalty for not taking insurance is not that large. So now it’s backing up. So they’ve gone back to the employer and said, “I can’t afford this anymore. So you’re going to have to shoulder this burden, Mr. Employer.” And they’re saying, “We can’t afford it,” and they’re finally going back to the health insurers, who by the way, were part of this conspiracy because they never really wanted premiums to go down.
Chris Kresser: Sure.
Pat Charmel: Right? Why would they want it? If you get 15 percent of the premium for overhead and profit, why would you want the premium to go down? As long as somebody's willing to pay that premium, you want the premium to go up. That was kind of the dirty little secret. So the insurers, when they sat down with my hospital as an employer, and we have 1,600 employees and spend a lot of money on health insurance, they were always very sympathetic. They always had a sympathetic demeanor when we talked about the costs going up, and kind of … it’s interesting when you’re a provider and an employer of healthcare. But at the same time, you say, “Hey, it is what it is.” Now it’s at the point where those that are actually paying are saying, “We cannot afford it anymore.” And you have state governments, especially after Medicaid expansion, pushing back and saying, “We’ve got to change the incentive.” Employers who are now becoming somewhat enlightened and saying, “There’s got to be a way if we can no longer just push the cost onto our employees, we’ve got to figure out a way to actually make care less expensive.” In my view, that’s what’s sort of fueling kind of the innovation around a different approach.
Chris Kresser: Right.
Pat Charmel: And providers who were part of the conspiracy as well because they knew that the insurer was going to continue to raise the premium, and if they’re getting a fixed share of that premium themselves, they were sympathetic, but didn't change. Now we’re forced to change because the current model is not sustainable. And as much as we'd like to continue to get fee-for-service and take care of sick people, which covers the overhead, we’re realizing that we actually have to be partners with the employer and the insurer and the employee or the member or the consumer to basically work together to say, “Folks, we could wait for people to get sick and then try and do a whole bunch of stuff here, but nobody can afford to pay for that. So let’s get in on the front end now.” And now the problem with that is that disrupts your business model and it's pretty scary.
If you’re a provider with a lot of fixed costs, how do you shoulder that burden during the transition period? How do you reduce your operating costs so you can live with the low utilization that results from actually keeping people healthy?
How conventional medicine got to this point
Chris Kresser: So, let me see if I can summarize this briefly. So, historically, there’s been a misalignment of incentives where you have these various players—the providers, the payers and companies—who weren't necessarily aligned in terms of their best interests. And so that led to a lot of inefficiencies and excess costs, and it got us to this point where we have a system that's inherently unsustainable. And what's happening now, it sounds like, is there's a shift towards more aligned incentives and maybe even opportunities where providers and payers and employers can work together, or at least where their incentives are now aligned and there can be more efficiencies created there.
Pat Charmel: Yeah, Chris, I think you have it. I don't know that the incentives are quite aligned yet, but I think they have to be if we’re going to get through this. Because that’s really the only way that it’ll work. If we’re … each of the stakeholders is trying to maximize their position at somebody else's expense, we’ll basically come up with another unsustainable solution. I think it is that question, and then the question also is what is the role, the historical role, the traditional role of each of these individuals and if that needs to change. What’s the payer’s role?
Chris Kresser: Right.
Pat Charmel: The payer used to be, I’m a health maintenance organization. Inherent in that name was we actually manage care. And they really didn’t because there really wasn’t an incentive to do that. And by the way, even if there was, how effective are they at doing that truly? And what’s the relationship between a health plan and a consumer? And do you trust your health plan to manage your care?
How the healthcare landscape is changing
Chris Kresser: Most people would say no, for sure. I want to talk more about that. Vipul, you’ve been really instrumental in educating me about this landscape, which I appreciate. Let's talk a little bit more about incentives because, of course, in most industries, there is an incentive to perform better and more efficiently, and you’re rewarded for that. That hasn’t really always traditionally been the case in many areas of healthcare. So, what kind of changes are we seeing now in healthcare to move more towards this more of an incentive-based system of value-based care? I’ve talked about companies like Iora Health with my audience that are using capitated payments for diabetes prevention. So, can you give us a kind of overview of some of the broader changes that are happening here?
Vipul Vyas: I think Pat can obviously weigh in, in a much more deeper level as well. But I think what you’re seeing, Pat just shared it, is that as a risk has sort of cascaded from the insurance company—and I would actually argue to Pat’s point around the insurance company taking a 15 percent cut off the top, the insurance company really isn’t much of an insurance company. More they’re a transaction agent, similar to Visa. They own the network, they collect the premiums, they make the payments, they handle the claims. But in the end they’re not really assuming risk like they historically have. That’s been largely pushed to employers.
And many people may not realize, though I'm sure many do, that the employer typically, especially large employers, self-insure. Meaning they’re the ones taking the risk, and the insurance company is simply a transaction facilitator. And so to Pat’s previous point, there’s a significant interest on the part of the employer to reduce these costs. So in the end, it’s the employee, and then by extension, the employer, who’s probably the prime economic driver saying, “I can’t afford this anymore.” I’m sure the federal and state governments are, to Pat’s point, saying the same thing, saying, “I can’t afford this anymore.” Therefore there’s a competitive market emerging in terms of value-based care that says, “If someone comes along with a plan that says they’re going to be cheaper because their cost of production is lower,” and again, kind of referring back to Pat’s point about changing your cost structure, if you’re a provider or health system, if you can change your cost structure and create a competitive advantage by way of being able to price lower and going to an employer and saying, “Look, I can deliver the same set of services as my local large competitor at a lower price in partnership with an insurance plan. And then I can actively manage your employee population to be healthy as a sweetener to keep those costs down or at least keep the growth of those costs in check or at a manageable level,” then that becomes an economically attractive option for the employer.
And so creating those bundles and making that programmatic and scalable is sort of the key evolution that we’re going to see. When it comes to the general market and what the ACA did, it really fosters some innovations I think the market was going to kind of fall to anyway, just given the premiums rising and healthcare costs rising, and there’s just economic pressure to do something. Because the paying entities, the government, employers, employees just didn’t have any more money in their pocket to pick, has driven this sort of capitated payments. And capitated payments is where eventually the risk is taken by the entity that can probably manage it the best, and that’s the providers.
So instead of paying $1,000 to Aetna and them keeping it, it basically flows to the provider to, say, Aetna takes their 15 percent off the top, and there’s $850 that goes to the provider. And the provider’s then told for $850 a month keep this person healthy. If they spend more than $850 a month on average, then you lose. If they spend less, then that’s your margin. And that’s where things are headed. Pat can comment on that much more intelligently, but that’s the gist of I think some of the drivers that are emerging.
Chris Kresser: I think a lot of people who are listening to this might be surprised that that’s the way it hasn’t worked all along. Because that’s the way it works in most other fields. You have a certain performance target and if you meet it, you’re rewarded and if you don’t meet it, there’s some consequence. But that actually is not how it’s been going so far. Laura, I just wanted to touch base with you because I know the Heritage LifeFit Program that you’re working on is maybe a good example of this. I think some of my listeners are less familiar with the terminology we’ve been using. This might kind of help people to understand what this looks like in practice.
Laura Conley: Yeah, so I’m actually kind of on the ground level working with people, and Heritage started this way ahead of their time, just kind of as an experiment. And I think it grew beyond what they even imagined because it started out as fitness classes at the healthcare facility. And over time it grew into a community of, “Okay, so you’re not just going to see your doctor, you’re actually going to take some fitness classes as well.” And then it grew into a community of really deep bonds and friendships where these people were changing their lives together. And so we really saw that this could be so much bigger than just “how do we get these people healthy and reduce their cost?”, but how do we actually change their lives forever in multiple areas. Not just in maybe chronic diseases like heart disease or diabetes, but also in their wellness scores of anxiety, depression, just how they were feeling about themselves and their happiness.
So it really hit across all levels and it’s been fun to watch this evolution happen. But yeah, it’s kind of what we’ve been doing.
Chris Kresser: That’s a great example. Yeah, that’s an amazing shift that’s happening. And Pat, you’re CEO of a hospital and so I think some people might not expect that a CEO of a hospital would be someone who’s actually looking at how the practice of medicine itself has to change and how we have to shift away from acute care towards more preventative, integrated type of care. So tell us a little bit about how you came to that realization and what you're thinking of in terms of the future.
Pat Charmel: Yeah, so, we have a pretty long history, and again, as Laura said, she was a little ahead of our time. And I think Griffin, my organization, was as well. We actually made a decision in the early 1990s to start our own health plan. Not because we saw having a health plan as a wonderful business opportunity; we just kind of came to realize the perversity and the currency for a service system.
Now you have to understand, Griffin is a relatively small hospital. So in the fee-for-service environment, we don't have the leverage that, say, a large academic medical center has or a large system of possibles when it comes to negotiating with, say, commercial payers who if you have that leverage, you get paid more. We didn't have that, so we get paid less, significantly less, and many of your listeners don’t realize that the rate that a commercial insurance company contracts with a hospital for a specific service varies by hospital pretty dramatically. So in a single market, what most of it is is case rates, and the case rates are paid by diagnoses. So what a health plan or a commercial insurance company pays a hospital in a market for, say, a pneumonia admission may vary from, say, $7,000 per case for the lowest-paid hospital in the market by that insurer to $14,000. Twice as much.
Chris Kresser: Wow.
Pat Charmel: With essentially the care of the exact same condition. And often times the lower-cost hospital is the independent community hospital, less complex, but they produce a better patient experience and a better outcome.
So we were one of those:
Higher performing
Better patient experience
Better outcome
Fewer complications
Lower infection rates, and
Getting paid half of what the highest-cost hospital in the state was.
And because we lack that leverage, the margin on our business is razor thin. And we recognized also that there’s perversity in the system. We were paid to wait for people to get sick, the sicker the better. And then when they showed up being sent to us to (audio cuts out 23:48), I like to say whether they need it or not. But I don’t want to be righteous about this. If I was that large academic medical center CEO who had the leverage to get high rates, that I would have been so enlightened about the perversity of the system.
Chris Kresser: Right.
Pat Charmel: But I was, so our team decided to … the way to address this is to actually go upstream and control the premium dollar, own your own health plan, and then once you have that premium, decide how you want to spend it. And frankly, if you spend it on prevention and wellness and good primary care, as a health plan you could win, right? Because you’re collecting the money up front. So that’s what we did. Now what we didn’t realize is how difficult it is to run a health plan. And I won’t get into that. So it was a great idea poorly executed, and it didn't work financially for us. But it put us on a different path, and it was really because of our underlying philosophy about we really should be engaging patients and make them partners in their care. And this is what you’re hearing form Laura, she’s actually doing this.
Chris Kresser: Right.
Pat Charmel: And a partnership to keep them healthy or if they’ve already got an underlying chronic condition, how to manage that condition effectively to improve the quality of their life. So we began to do that and we built all kinds of infrastructure around it. We’re a teaching hospital. Most teaching hospitals who teach graduate medical students usually treat them in traditional internal medicine. And most of that training happens in an acute care setting, and a lot of it in an ICU. So their mindset is wait for people to get sick, the sicker the better, and then take really good care of them. And we did that.
But we decided in addition to internal medicine, which we changed the focus to community-oriented primary care training within internal medicine, we took it one step further and said, “Why don't we actually train graduate medical students in preventive medicine?” And we did that 15 years ago. We started a preventive medicine training program, and they were fairly rare, and still today they’re fairly rare because when … why would a physician who’s looking at the current incentives in the healthcare system want to be trained in preventive medicine? Nobody was rewarding that. In fact, you might be the medical director or the director of a local health department, or maybe you would get into occupational medicine and work in an employer health clinic. But for the most part, there were no jobs for these people.
Chris Kresser: Right.
Pat Charmel: So we did it anyway, and we developed a prevention research center that CBC funded, and we’ve developed lots of capabilities. Well, I like to say now that our preventive medicine residents are the rock stars of the healthcare industry. As our industry’s beginning to change with a focus on prevention and wellness, and there’s move to value, all of our residents have agents representing them.
Chris Kresser: Right, in the highest demand. Getting recruited.
Pat Charmel: Right, so the food chain is being reordered. The people who were at the top used to be the proceduralists, who were really good at taking care of sick people. And now it’s people who have this capability. So we’ve had to move here before the incentives were there, and partly because who we are, what we believed in philosophically, the disadvantage where because of our size … And so we are one of those organizations because we have these capabilities, we have the cost structure, we’re trying to move the market in that direction because it’s the right thing to do and it would advance us as well.
And I’m trying to bring a lot of other more traditional providers along with us. And they also know it’s the right thing to do, but they’re having a struggle with the economics. Because if you’re successful in the short term and you aren’t in one of these risk arrangements like Vipul described where you’re actually taking premium dollars up front, you’re acting more as much like an insurance company as a provider. And there’s an inherent financial risk in that. If you’re mostly a fee-for-service organization, you build this capability and keep people healthy, you’re actually cannibalizing your business.
Chris Kresser: Right, right. Yeah, you’d better have a new model for that.
Pat Charmel: And if you don’t have large reserves, how do you do that, and why would you do that? Most of these arrangements, and I have these conversations with colleagues all the time, the federal government is trying to create incentives through the Medicare program to push providers along this continuum more toward value-based care. And we’re doing some things here in Connecticut where we’re getting out to employers who are mostly self-insured, who didn't realize, by the way, that their health plan that’s administering their self-insured program pays between $7,000 and $14,000 for the exact same care. That was kind of a mystery to them. And now they’re saying, “Maybe I can change my plan design. Maybe I can look for those enlightened providers who will partner with me and my employees to keep them healthy.” But again, we’re in the early days of this.
The shift from “sick care” to true healthcare
Chris Kresser: Now that’s just a really big sea change that I want to highlight right here. In my book, I shared a statistic: it costs about $14,000 a year, from a few studies I found, to treat a patient with type 2 diabetes. So it becomes clear that even if you have to spend a little bit more up front in preventive care and intervening earlier on that spectrum when the patient has high normal blood sugar or even prediabetes, and you can reverse that so that they never develop type 2 diabetes, you can save an enormous amount of money over the lifetime of that patient. But what that requires is not waiting until the patient develops type 2 diabetes and ends up in your hospital or in the doctor's office. It’s actually going out and making contact and being proactive in engaging, creating new programs where these preventive efforts can become effective.
So anyone, Vipul, Laura, Pat, let’s talk a little bit about this shift. Because it seems to me that that’s, from a 30,000-foot view, one of the biggest shifts that is happening and needs to happen. Because historically in this country, I think we have had a, like you said in the start Pat, we have had a “sickcare” system where people just think of the doctor as a place to go only when they're sick, not as a place to go to get healthy or to prevent getting sick in the first place. So what’s happening now, and what do we need to continue to do to drive this forward?
Pat Charmel: Let me just give a little additional context, because I think it’ll enrich the conversation. So we do a lot of comparison between the U.S. and other industrialized countries, and it is true that we are spending a much larger percentage of our GDP. And on a per capita basis, spending twice as much as the average of other industrialized countries.
Chris Kresser: Yes.
Pat Charmel: But what we don't talk about is that the U.S. spends a whole lot less on social service support per capita than other industrialized countries who have better health outcomes. And so if you look at the combination between medical spending and social spending for us and the other industrialized countries, we look pretty good. Because we have this huge spending on medical and a little bit on social services. You combine them and we’re good, and we’re obviously better than the average. But if you look at social service spending as a percentage of total healthcare spending, that’s the combination of health and social service spending, we’re last of any industrialized country.
Chris Kresser: Wow.
Pat Charmel: And most of what you were just talking about, what can we do differently to manage somebody or prevent the progression of disease or help people develop healthy lifestyles so they don’t even get the precursors for something like diabetes, we’re going to have to spend much more money on social determinants.
Chris Kresser: Right.
Pat Charmel: Here’s the rub. Where does that money come from when, as a nation, we’re already spending too much money on traditional medical care? There has to be a resource reallocation. Now the people who are doing this wonderful work like Laura and local social service providers, when I say “resource reallocation” to them, they love it. When you say that to a bunch of hospitals and traditional medical providers, they’re thinking, “Oh, my gosh, you’re saying taking my resources and giving them to someone else.” That is a huge … that's one of the huge challenges. So are we willing to build that social service infrastructure? In my community, we’re beginning to invest in that, basically looking at who's got the capabilities. We’ve been doing this work in obscurity with under-resourced social service providers, who in partnership with medical providers can actually begin to make a difference. And that is something that we, from a policy standpoint, are going to have to really focus on. But a lot of people don't want to have that conversation.
Chris Kresser: I get it. I can see why. Vipul and Laura?
Vipul Vyas: I was just going to suggest to reinforce Pat’s point, when it’s New Year’s Eve or New Year’s Day, when people are doing their resolutions, very few people think about the healthcare system when it comes to, “I want to change. I want to transform. I want to improve my health.” It doesn’t really exist for the provider today and that’s what’s got to change in terms of engagements. So that people perceive the provider as engaged in their health. And that shift happens, I mean if you look at other industries, can you imagine, like, FedEx used to just be about shipping packages, but surely transformed beyond that to being a logistics provider. It’s more ingrained in your day-to-day life for a small business. Banks used to just be where you put your money. But now they try to take an active role in managing your whole financial life.
So these transformations have happened in other industries and can happen here. But it’s going to be an evolution. There’ll be a lot of experimentation. I think what you see happening with Laura’s program, and I’ll let her comment on it a bit more, is that the Victor Valley system is actually viewing their patents not as just patients, which as a word has a horrible connotation, but as a member, and members work for additional privileges beyond the traditional care. They also get access to these resources, all the services are free, the fitness passes are free, the engagement is free, the education is free in terms of how to be healthier, and how to transform yourself, and that comes along as a perk. And that is a first step conceptually, just like FedEx went from just shipping packages to giving people pick and pack, shipping software, and logistic software, so that they’re your logistics company. Or Amazon has gone from being just a place where you buy books to kind of where you get everything and anything for your household, the same way Victor Valley and what Laura’s doing sort of represent the start of that transformation as well.
Chris Kresser: Yeah, Laura, what did you see there of the transition from when it started when it was just a fitness program to where it is now? I mean, was there resistance along the way? How was that in your organization?
Laura Conley: Oh, yeah, definitely. So in the beginning, it was purely just fitness classes, and we grew with time. But one of the things that really built it was we told our members, bring somebody with you. Drag a friend in here with you. Literally, they sometimes had to drag. And the resistance in the beginning was really high, but then over time that touchpoint kept increasing, and okay, they would bring a friend, they’d bring a family member, and they would eventually start working out with us. And what happened that we all know is, you start to get results. And results actually build motivation.
So the more results they started seeing, the more motivated they became. And then other people within the community started noticing, and then the question became, “What are you doing? How did you change so much?” And the answer shocked people. Well, going to my healthcare facility. And in the beginning, the first two years, it was completely open to the community. So you didn’t even have to be a member of that healthcare facility. You could just be a member of the community and come take any fitness class for free. And then eventually we built it into, okay, now let’s have you switch over and become your primary care doctor as well. But really, it just took the community slowly building on itself of one person would bring in one friend, and maybe they’d bring in a friend.
And then the relationships grew and the camaraderie of doing these workouts together—I’m sure we all know, misery loves company—and you’re going through a hard workout, but you have these people next to you that are all pushing through together, and you build a relationship that’s really strong. And I think that that just organically grew on its own in addition to providing really good educational resources like free cooking classes and women’s seminars. And just the more we offered those and opened those up to the whole community, that’s what really brought everybody in and brought them together.
How employers can help employees manage their health
Chris Kresser: That’s interesting. I can’t help thinking that the solution, we need a multi-prong solution here, and I’m a small employer myself, about 35 employees across a couple different companies. And what I’ve noticed, I’ve been thinking about this just in my own small scale for a long time, we’ve taken a lot of steps to create a culture of health within the company, and ways that we support employee health and wellness, everything from offering health coaching and mindfulness to having an environment where we do challenges, start to do challenges where people are getting together and accomplishing their health goals and cheering each other on and using that social support. And I know, the whole corporate wellness conversation is another big one, and there’s a problem with adoption, but I think that for a lot of people, they spend most of their time at work. Their employer is their payer, especially if they work at a big self-insured company. So it seems to me that that’s got to be, employers, especially large employers, getting smart about this is going to be one of the big drivers of change, or should be, at least.
Vipul Vyas: And I think, Chris, to that, Pat can comment on this further, but I think it is a three-part solution in terms of the payer, the employer, and the provider all have to be rowing in the same direction to create transformative change in society. Because if you think about modern life, it's really geared to incenting you to be quite unhealthy. In terms of stay up late and binge-watch TV, binge-eat food, be socially isolated by just focusing on your phone all day long, all the construct of modern life is really pushing against you. So we need all those other entities to be rowing in unison and aligned to push back against those forces. And it’s going to be a challenge. I mean it can be an amalgamation of lots of small things, where the provider works with the employer to figure out how to make a healthier environment in terms of stand-up desks. Little things that just sort of in aggregate, add up and cumulatively make an impact.
Chris Kresser: Yeah.
Vipul Vyas: I think that’s probably the path that’s most realistic. And to your point, work is where people spend most of their day, so that’s where things likely have to start.
Chris Kresser: So I know all three of you have been engaged in some interesting examples of this. Pat, I’d love for you to share a little bit about new partnerships between healthcare systems, employers, and payers that you’ve been experimenting with. I think you and Vipul and maybe Laura have been working on something together.
Pat Charmel: Yes, yes. And just to comment on sort of employee wellness programs in the workplace, they were, they are sort of enjoying a bit of a resurgence because I think that comes with the understanding. It’s a little bit more comprehensive this time and connected. So before you had employers who were aligned who understand what you understand, but were doing what they did sort of in isolation. It really wasn’t a partnership with the provider community or the payer. So if you had something at work, for instance, that employee’s primary care physician really wasn’t aware of what was happening at work, wasn’t necessarily encouraging participation. Certainly the payer wasn’t aware. Most of the approaches now that are real successful are where all of those are working together.
So I know that we’re working with area employers on everything from an occupational health program. So everything from pre-employment physicals to actually treating injuries where they occur, but:
Looking at biomechanics in the workplace
Looking at physical activity in the workplace
Looking at the food that served in the cafeterias in the workplace
Looking at exercise throughout the day
And we actually have programs where we can help employers incorporate physical activity throughout the day into the workplace. We’re also helping them identify who their employees are that have underlying chronic problems that need to be managed more effectively. And as you say, most people, their waking hours are spent at work. The effectiveness of the interventions are tied to what's happening at work as well as at home. So that wasn't happening before. You were doing what you were doing and it was successful. The level of engagement varied by employer. But we all need to be working together to do that.
So, for instance, Vipul has been helping us build the information infrastructure to be able to … everybody who's doing this work together knows what's been done throughout the system and knows everything that we need to know about that individual to keep them on that path, to either more effective disease management, or to help them move to healthier practices, a healthier lifestyle. So the integration of this workplace wellness into the overall approach of health management, or disease management, if you want to call it that, is critical. And it starts, it starts early on. We are actually bringing a large employer into our sphere as we speak and we’re starting to do so to baseline engagement with the employer and the employees. Everything from biometric screening to workplace assessment to developing a platform for education and coaching. Again, it’s a much broader approach, where all of the pieces are connected and we can monitor progress. And then the employer can build in the right incentives to motivate the kind of behaviors that are going to bring about success.
Chris Kresser: So in that case, Pat, is the employer also the payer? Is it a self-insured company? Or is there also an insurance company involved?
Pat Charmel: There is an insurance company involved. It happens to be one that we are partnering with with in sort of an accountable care relationship. But this is a self-insured employer with that payer as the administrator of their health insurance program.
Chris Kresser: So that's an interesting example of how this, all of the various players are realigning in a way that I would imagine serves everybody's interests. I mean, what, is everybody happy in that arrangement? Is the payer, I don’t know as much about this, but I wonder if a payer is happy to be … “relegated” might not be the right word … but to the role of just serving as the administrator rather than taking or playing a bigger role.
Pat Charmel: Well, I think Vipul said earlier, and I’ll let him address it again, the payer doesn't necessarily mind being the administrator of the self-insured program role, because they’re not taking financial risk taking, they’re not taking insurance risk. As long as they're getting enough margin on playing that role of administrator. But they see what I just described as the ability to develop a comprehensive program as they’re differentiated. Now they were moving toward sort of a health-promotion, keep-people-healthy model. There are folks who could process claims a lot cheaper. If you were just serving that administrative function, you're going to get marginalized or commoditized.
So what they're saying is the way we differentiate ourselves or add value is to be that integrator. Not that we’re going to provide the care delivery piece of it ourselves or the health promotion. They tried that before. And the problem with that is, consumers don't want to engage with their health plan. They don't trust and they don't have a relationship with their health plan. But the enlightened payers are now partnering with providers and say, “Look, we’re going to admit that we’re not really good at that. But we’re going to find the people who are really good at that, and we’re going to build the infrastructure and the glue to sort of make that really effective.” So there are a couple of payers that have really stepped up to look for providers like us in true partnerships.
And we’re still finding our way, but … and then also stepping forward together with the employer and their employees in ways that have never been done before, where you have both the employer and the provider, excuse me, the insurer and the provider talking to the employer and their employees. And so they're trying to get their engagement and build their trust, and provide them with the information that they need to make intelligent decisions, which also has never taken place before. As a self-insured employer who used to pay a lot of administrative fees through the health plans to administer our program, who told us they were managing our patients with serious underlying disease, the fact of the matter is we never got actionable information, and frankly we didn't get, we never got the information that we need. So even though we knew that we might've had, out of 1,200 employees at the time, 300 that had serious chronic problems, what we heard from the health plan is, “Well, we have disease management programs,” but when you really push them and say how many of our employees and their spouses are actually engaged in those programs, and we would find that it was maybe less than 10.
Chris Kresser: Right.
Pat Charmel: Now we’re saying to the provider and more so the physicians, especially primary care physicians who have a relationship with those employees or those consumers, we need to build capabilities around them because they're the ones that are going to bring about that engagement. And if we have things happening in the workplace and we have the right incentives so employees actually participate, they’re actually engaged, we’re going to get the kind of results that we’re looking for.
The social factors that impact health
Chris Kresser: This is so fascinating. I wish we could keep going. We only have a couple minutes left here. You touched on the social determinants of health earlier, Pat. And I just wondered if you could say a few more words about that because so often, at least within the functional integrative medicine discussion and for now, since it's not really integrated into our conventional health system, it's really limited to people who are middle class, upper middle class and above. It's quite expensive and yet if we, as we said in the beginning of the show, if we want to have an impact on the population health scale and really bring everyone along in this movement, we need to be thinking about things in a different way in terms of just the shocking number of people in this country that don’t even have access to fresh food. And just even the basic things that are required for health. So can we talk just about this for a couple minutes as we close?
Pat Charmel: Yeah. So we’re in a suburban community that most people look at the community and say this is a middle-class community, a working-class community. But when we did a study recently, we found that about 40 percent of the households in our community don't generate enough income as a household to meet essentially the basic needs of that household. So when you look at poverty, those numbers may be 5, between 5 and 10 percent. But when you’re looking at almost 40 percent can’t meet the basic needs of the household, so what suffers? So food, the quality of their housing, their ability to pay for traditional medical care now that we know that folks are paying $0.42 out of every dollar. They may not have adequate transportation, and it sort of goes on and on.
So what we recognize, if we really are serious about keeping populations healthy, we have to address the needs that come as a result of the fact that 40 percent don't have the resources. So we’re looking at housing insecurity, we’re looking at folks that have … the quality of their housing too. It’s not folks that, we’re not looking just at, obviously, at the homeless, so we have a huge problem with pediatric asthma in this community. And we truly believe that it’s tied to the quality of housing. So we have problems with homes that aren’t air conditioned, we have lots of homes that have mold problems, and folks can’t afford to do mold remediation. They could be in rental properties where we have landlords who are not addressing those problems. So they have code violations that are not being addressed by local governments.
So do we have to intervene there? How are we dealing with the issue of people who can't afford food, or nutritious food? We’re dealing with that as well. We’re addressing issues of transportation. We’re trying to get at the underlying causes of that, which are the inadequate household income and looking at things like job training. And how can we get people to sort of progress and build the skills they need to increase household income? Now you’re talking about a traditional healthcare provider looking at all of those issues.
Chris Kresser: Yes.
Pat Charmel: As I said before, that’s going to reach … we’re actually beginning to screen individuals in our community for those needs. And there are traditional providers of those kinds of services. Meal assistance, transportation, fuel assistance, housing assistance, they exist. But they’re under-resourced. So we’re out in the community now screening, and now we’re referring to them and building a system to track individuals who are referred to make sure that they follow through. But what are we doing? We’re burdening these agencies who don’t have adequate resources. And they said, “It’s great that you’re doing this, but we have to now build additional capacity to meet the needs of the individuals that you’re sending us because they weren’t finding us before.”
Chris Kresser: Right, right.
Pat Charmel: So we’re actually now beginning to actually say, “Hey, what is it going to take for those organizations to create the capacity to meet the needs that we’re screening for and referring?” And it’s a little daunting because the economics of our business model don't necessarily support that yet. But that’s the reality. And in many parts of the country, there are providers who do not want to go here. They know intellectually that it has to be done if we’re really serious about managing the health of populations, but do they want to take on the social support burden that comes along with it?
Chris Kresser: The full scope and complexity, and everything that … yeah. I mean, what occurs to me as you were talking is in holistic medicine or integrative medicine, we recognize that you can’t just treat one part of the body without treating, addressing the rest of the body. Everything's connected. Well, it’s exactly the same with this healthcare situation. As you’ve pointed out, we can’t just address how care is being delivered, and providers and payers, we actually have to think about the social determinants of health and really pay attention to those. Because if we leave that part out, no matter what changes are made elsewhere, they aren’t going to be effective because if someone can’t afford to buy the healthy food or they’re living in a house with terrible indoor air quality, then we’re going to be starting from 10 steps behind.
So it’s really illuminating and it’s just a, to me, an invitation or a reminder that we really have to be approaching this and thinking about it systemically. And I just want to say kudos to you, Pat, for providing an example of how this can be done. I think it's incredible what you’ve accomplished at Griffin and the way you’ve been thinking about this for several decades now. And I'm really grateful for your time and willingness to come on and share your vision with us. And Vipul and Laura, thank you so much as well for being here and for all the work you've done in this area. I'm excited. I mean it is a little daunting and overwhelming on the one hand, and on the other hand, it’s exciting to know that these changes are taking place and that everyone has a role to play. There are a lot of different ways that people can contribute to this effort.
Pat Charmel: Absolutely.
Laura Conley: Absolutely.
Chris Kresser: Okay, everybody, thanks for listening. Hope you got a lot out of this show. Remember to keep sending in your questions to ChrisKresser.com/podcastquestions, and we’ll see you next time.
Vipul Vyas: Thank you, Chris.
Chris Kresser: Okay, thanks everybody.
Vipul Vyas: Bye-bye.
Chris Kresser: Bye.
Laura Conley: Thanks, bye.
The post RHR: The Shift from Treatment to Prevention, with Vipul Vyas, Locke Ettinger, & Pat Charmel appeared first on Chris Kresser.
Source: http://chriskresser.com
August 07, 2018 at 10:22PM
2 notes
·
View notes
Text
MY BIRTH STORY
Trigger warning/s: Birth trauma and postnatal mood disorders
Less than a quarter of healthy, low risk, first time parents will have a normal birth in an Australian hospital. With the recent release of Birth Time: the documentary in Australia and New Zealand, I felt that revisiting my birth story was timely.
It’s a clichéd adage but it’s true: for me, the birth plan went well and truly out the window. In fact, it was never let into the building.
EST. READING TIME: 5 minutes
In my early twenties, I used to avoid making eye contact with the family planning section at the chemist. These days I have an emergency stash of tests in my bedside drawer. I’m not even late - my period tracker says it’s due today - but I have a nagging feeling that won’t go away.
I pee on the stick, and there’s only one line. Oh well. I shrug, insouciant, throw out the test and go about my day.
Until four in the afternoon, when I sit bolt upright on the couch and realise that I, generally a rule follower, hadn’t waited for that result. In fact, the box tells you to wait five minutes. So much for sitting on the couch with an egg timer.
I dig through the bin and in my shaking hands is a positive pregnancy test (note: those trying to conceive affectionately refer to this as a BFP). I test again, and again. I can’t wait, I race in my car to Victoria Park where my boyfriend of two years is working, with three BFPs sitting in the cup holder.
And so begins the uncontrollable for the Type A control freak.
In a pandemic, there are already things I can’t control. I’m redeployed to a different unit at my work and can no longer take potential COVID patients.
I’m anxious, exhausted and most of all - experiencing morning sickness that will turn into hyperemesis. Then, I have to take extended time off work.
As I do with most things, I jump straight into the deep end of pregnancy world and obsessively research. I avoid the foods you’re meant to avoid, and I buy all of the pre-baby accoutrements. Birthing ball, new yoga mat (and maternity yoga pants to boot), and the books. Oh my god, the books.
I do the hypnobirthing classes and listen to birthing stories while hiking with my dogs.
Being pregnant is simultaneously my new persona and hobby. I honestly still wouldn’t change a thing now, in spite of what I know, because even through vomiting for 7, nearly 8, months; I love being pregnant with all my heart.
I neatly type up a birth plan, beautifully formatted and fonted. Natural, natural, natural. No episiotomy. No pain relief. Don’t even offer it to me - I’ll ask. No interventions unless necessary. Delayed cord clamping. Immediate skin to skin. Quiet, low lighting, music. To me, this was a covenant between myself and the computer. Absolute, resolute and set in stone.
By the third trimester my partner and I have the hospital bag meticulously packed, nursery ready, and the big waiting game to do. Eager for our little family to be complete.
At my 38 week appointment, our obstetrician informs us that baby isn’t showing any signs of coming any time soon. I take that as a challenge and research a litany of labour-inducing old wives’ tales.
PSA: none of these actually work. If you are healthy with no complications, your baby will come when ready. Don’t rush. Even when you feel as if you can’t possibly be pregnant for single millisecond more. Your baby isn’t term until 40 weeks.
But here’s the kicker; the impending threat of an induction and/or caesarean looms overhead. I’m told I am a small girl. He appears to be a big baby. His head isn’t engaged at all. And that the clock is ticking.
Now I wonder what might have happened had that idea never been put into my head. If I had been given the space to accept my birth as it would come. Real birth. Normalised.
The pitfalls don’t just lie with mainstream media. You are being sold something. The expensive classes will tell you that having a natural birth without medication is possible, if you buy our book. The private obstetrician will tell you that you need an induction, an epidural, a caesarean; pay us.
At 39 weeks, the Friday before Christmas, my baby is showing signs of coming. What follows is 9 days of latent, or prodromal, or pre, or (my least favourite term) false labour.
On the Monday we go into hospital. With contractions 3 minutes apart, we are told my cervix and uterus aren’t agreeing. Simply put: head isn’t engaging, cervix isn’t dilating. And that I’ll know it when I’m in real labour.
During the week that follows I try exercises from Spinning Babies to get some relief from the round the clock contractions, Jack gives me massages and on one night I even give a glass of red wine and a bubble bath a go.
Websites that want to sell me something tell me that it’s because I’m too stressed for the labour to progress. Try our tea.
Why are we capitalising on something so sacred as birth?
I walk with one foot on the curb and one foot on the path - and I do this for kilometres. Through King’s Park in 30-degree heat. Along the coast. Around the neighbourhood.
On Christmas Eve, I can’t sleep, speak or move through the contractions and we wait as long as possible. We camp on the fold out bed in the living room (those without air conditioning throughout improvise), the birthing playlist quietly crooning and candles burning. I do my breathing and mantras; relax, relax, relaaaaax. And the contractions stop as abruptly as they started, 20 hours later.
I cry. Low keening, animalistic sobbing. I don’t understand what is happening to me. I don’t feel confident in making the choice whether or not to go to the hospital anymore.
They tell you the hospital is the safest place to birth and in the same breath tell you to avoid the hospital unless you’re damn near crowning.
I’m new to this. It’s my first time. I feel scared, unsupported and alone. I’m in so much pain.
I just want to meet my baby.
Barely two days later, I shake Jack awake. I’ve got a Miss Clavel feeling. Something is not right. Instinctively I know that after nine days of exhausting labour that doesn’t seem to be going anywhere, I will be too tired to push.
I call the hospital and ask if I can come in.
Have you just had enough? A voice asks on the other end.
So I don’t take the Panadol or the shower or the bath. We roll into the birthing unit and I’m put on the monitor. Like the High Striker at a fairground, I get the sense that the rolling peaks on the screen need to reach acceptable heights before I’m taken seriously.
The midwife is watching for decelerations, which don’t happen, but also doesn’t see any accelerations. My baby is tired, and I don’t blame him.
And then I am asked the question.
What do you want to get out of being in hospital today? Do you want to have your baby?
I nod, because yes. So comes the new plan. Break my waters and start the syntocin drip tomorrow. Temazepam and Panadeine Forte tonight. So quickly everything I imagined for my birth is going out the window, but I’m desperate.
The next morning we waddle into the birthing suites to start my induction bright and early. I feel robbed of the moment my waters break as it is cracked with something that looks like a crochet hook on a glove. With a gush and then a steady trickle, all the amniotic fluid keeping my baby safe and sound floods out. My obstetrician tells me it’s meconium stained, the paediatric RN in me fleetingly panics. But it is all systems go. I race from active labour to transition. I can only focus on the contractions.
I want my mum.
I’m offered the epidural I’d refused the day prior again but I shake my head. Not in the birth plan. Gas and air only, please. I end up screaming into the Entonox mouthpiece every 2 minutes and throw up all over myself before I allow myself the grace of an epidural. Which only works for about fifteen minutes before I’m once again writhing and screaming, one leg ice numb but the rest of me on fire. Intense pressure between my legs, the urge to push. But it’s only been a couple hours.
My mum arrives in the hospital. On the birth plan, she was meant to be waiting outside. She stands near me now, in the birthing suite.
I’m making noises I am not proud of and inform my midwife of my need to push. Oh, it’s too soon? Pardon me. Before the midwife’s assessment I steel myself to be told I am nowhere near, after a week of disappointment and being nowhere near.
Oh. You’re having a baby.
I ask if we need to wait for the doctor when she tells me she’s calling my obstetrician.
No, she laughs. You don’t have to wait.
With my knees to my chest, I’m told to stop pushing and so I stop. Afterwards, my partner tells me that our son was getting distressed despite my best efforts to get him out and the obstetrician was pulling back on the cord that was tight around his neck. And my poor tired baby’s heart rate drops dangerously. I’m given a deadline to push him out, but I can’t and I’m given the episiotomy I had expressly verboten on my birth plan. He is vacuum assisted out. He is safe.
I’m handed a small, beanlike baby covered in blood and vernix. I kiss him and end up with blood on my face. He doesn’t cry.
He’s taken off my chest and it feels like the longest pause before he lets out the best scream I’ve ever heard.
My mum looks at me. He’s beautiful, she mouths. Is he okay? He’s okay.
My partner cuts the cord. No delayed cord clamping, breathing is more important. Oliver is soon enough placed back onto my chest.
And he is beautiful.
What starts days later as the baby blues progresses into postnatal depression and anxiety. It took me a long time to accept what happened was birth trauma. That my birth story is ridiculously common, even amongst my group of friends, and that’s not due to our failure as the birthing parent. I can’t tell you how long I felt I only had myself to blame for having false expectations. And how much value I put into my ability to birth the “right” way as a direct translation of my ability to mother. How I felt that my son’s birth complications were my fault (it wasn’t). Too many Australian birthing parents are made to feel this way.
So I write this birth story once more, and I let go of what happened for my own sake. I didn’t fail. My son is beautiful, and worth every second of the agony it took to get him here.

A previous version of this post was published on my friend’s blog Mummy Neutral as ‘Type A and the Uncontrollable Pre-Labour’ in January 2021.
Please check her blog out as she posts some really raw and beautiful insights into pregnancy, birth and motherhood.
If you’re feeling distressed about anything discussed or about your own birth experience, please click the life ring symbol at the top of my blog for some helpful links. Call Lifeline on 13 11 14 if you need immediate assistance.
Birth Time: the documentary is showing in select cinemas now. You can visit the website to find out more and if you have birthed in Australia in the last 5 years, you can complete a survey about your experience.
1 note
·
View note
Text
a letter to my parents
Dear Mom & Dad,
They say the hardest step in resolving a problem is admitting you have one. I have never been the type of person to run from my problems, I usually like to fix whatever the issue is as soon as it arises so that it doesn’t build up or get worse. Time and time again, throughout my entire life, and in the last three years especially, I have been trying, by any means possible, to escape this specific problem. Despite my efforts, I haven’t been able to. For a long time now, I have been trying to build up the courage to not only come clean about this to you guys, but to myself as well.
In short, my brain has not, does not, and will never align with the anatomical sex that I was assigned at birth. In other words, I am transgender. This diagnosis is called “Gender Dysphoria.” Unlike most other medical conditions, you can’t see what I have on the outside; blood work can’t measure it, ultrasounds can’t detect it, and MRI’s can’t scan it. Like many diseases or birth defects, there is no clear cause, although there are theories.
Popular belief outside of the medical community holds that people with “Gender Dysphoria” are merely “Gender Confused.” This is far from the truth. No one would choose to undergo something so drastic and life-altering as this. If I had the choice, I would choose for these feelings to go away and for me to be like everyone else. I am making the choice to come out to you, and to move forward with transitioning, because if I don’t I will live miserably and as something I am not for the rest of my life, and I cannot do that. Yes, I am choosing to come out and live authentically, but I am certainly not choosing to be trans. We are born with this and it is inherent with us from our earliest recollections.
This probably comes as a shock to you both, and that was never my intent. I am sorry I kept something so important and serious from you for such a long time, but because of how negatively you both initially reacted to me being a lesbian, I was too afraid. I thought to myself, “If being a lesbian was extremely difficult for them to accept, being trans will be one step too far.” I had to move out of the house before I told you in case you responded badly. I didn’t want to go through what I went through back then again, I couldn’t. I am worried that after reading this letter, that you two will no longer want to be my parents or love me at all. I am worried that you will be embarrassed of me, disgusted with me, think I’m delusional or just going through a phase. I have been living with this fear inside myself for a long time now, but now I finally have the courage to say that with or without your love and support, I am going to take the necessary steps to become who I’ve always been.
From the outside looking in, I suspect that one would have thought I lived the good life. In many ways I have, and I couldn’t be more grateful for that. They say, “never judge a book by it’s cover,” and unfortunately, you, and everyone else in my life was just seeing the cover. Inside was something much different. Nobody, not even those closest to me, could see my internal struggles and pain. I have been hurting for a long time now, but I couldn’t tell anyone out of fear of rejection.
In retrospect, I can see symptoms of me being trans from all the way back to my early childhood, as young as three years old. I will discuss this further with you if you would like. The real symptoms began around the time I started puberty, because that’s when my body began to develop in a female way and not a male way. Although I did not have the vocabulary at the time to describe what I was feeling, I now can look back and pinpoint exactly what was wrong. I was disgusted with myself due to the development of breasts specifically. While all the other girls my age were trying to emphasize their feminine bodies, I was trying to hide. At the time, I didn’t know exactly why I was so uncomfortable with myself, again, because I didn’t have the vocabulary. While most other 13 year old girls were insecure because boys didn’t like them and their boobs weren’t big enough, I was insecure because I didn’t fit in with the boys, and my boobs were growing. Most girls at that age were also insecure because they were “fat,” so I began to think that was what was wrong with me too, because what else would it be? Around this time is when I began to cut myself and starve myself; I never told anyone. I hid my pain because I didn’t understand what I was feeling, and I didn’t know what would become of me if anyone were to find out. I was ashamed of myself and how I felt. I tired to mirror the behavior of female role models and peers, thinking my actions would ultimately program my thinking. This was a false assumption, but as a child I knew no better. My brain could not relate to women, yet I kept going through the motions, playing a role so that I could be accepted.
The feelings only continued when I got to high school. In 9th grade, I joined the basketball team, and on the team was a handful of “butch” lesbians if you will. Instantly upon meeting them, I related to them. They were girls like me, who dressed, behaved, and carried themselves in a more masculine way than other women. Before meeting them, I didn’t even know that it was possible for me to break outside of typical gender norms, especially now that I was getting older and being a “tomboy” wasn’t so normal anymore. I didn’t know that there were other people like me out there. By sophomore year, I had fully realized that I was a lesbian. I never have had any emotional or physical attraction to a male before or after that. Time went on, and I continued to dress in boys clothing and be attracted to girls. Although dressing in that way and being aware of my sexuality helped me feel far more comfortable than I was prior, those same feelings from years gone by still lingered, and got increasingly worse the more feminine my body became as it developed. Keep in mind, at this time, I was completely unaware of what transgender even was. I had never heard of the term before. Furthermore, I would try to minimize the appearance of my feminine features, such as breasts and hips, in any way I could. I would wear multiple sports bras to compress my chest and wear sweatpants or a long baggy t-shirt so that I could hide my hips. I’m going to be bluntly honest with you when I say this: I was absolutely horrified for you to find out I was a lesbian. With my Catholic upbringing, it was ingrained in me from an early age that heterosexual relationships were the only acceptable form of attraction or love. Along with that, and homophobic remarks I would hear you both occasionally make, I knew you would not be okay with it. I honestly cannot describe in words how deeply afraid I was of what would happen to me if I was to be outed. I didn’t plan on telling either of you until after I graduated from college so I wouldn’t have to deal with the repercussions, which obviously didn’t go as planned! This is around the time that I started to develop paranoia and anxiety about you finding out. I was constantly, and I mean constantly, thinking about it. For a long time, the fear would already be in my mind the moment I woke up in the morning, and wouldn’t leave until I fell asleep at night. Sometimes I would even have nightmares about it and would wake up with my heart pounding, covered in sweat. This was an extremely difficult time for me. I really struggled a lot and didn’t know how to help myself. Due to this high amount of paranoia, stress, and anxiety that was put upon me, the thoughts I had about how strongly I disliked my body were dulled, and moved their way from the front of my mind to the back. Then eventually you guys found out about my sexuality in July 2016, the summer before my senior year. Although it did take awhile, you came around eventually, especially in the past year and a half, which I am really, really happy about because I thought it would never happen. I didn’t have to worry about being outed anymore, and all that paranoia and anxiety I had been experiencing slowly faded away. I felt a weight lift off my shoulders and my heart felt lighter. Unfortunately, as those feelings faded, the thoughts about my body moved from the back of my mind to the front yet again. Toward the end of my senior year, a friend introduced me to her friend, who happened to be a female to male transgender man. This was my first time meeting a trans person, and this was the first time I became aware of the term. After meeting him and hanging out, I immediately started doing research on what being transgender was and what it entailed. Instantly, I was putting the puzzle pieces together about why I felt the way I felt. It slowly began to make sense. A few days later, I reached out to the transgender guy I had hung out with, and was telling him that I thought I could possibly be trans too, and that I wanted to know more about it from someone who is actually going through it. He started telling me about how he felt, his experiences he had as a child, feelings about his body, etc. Again, I related to everything he told me. This was almost a relief because now there was a name for what I had been feeling all along, but also horrified me because it’s a huge, life-altering change that involved medical intervention, as well as socially transitioning. But what really scared me the most about being trans was the fear that you guys wouldn’t accept me, and that you would not want to be my parents anymore. I had already been through so much with coming out as a lesbian, and I didn’t want to throw any wrenches in the gears when things just started to get better, so I kept quiet and didn’t tell anyone else for a long, long time.
I kept quiet, but I kept doing research, and the more stories I read the more I related, and the more these stories sounded like me and my life experiences. As I began to realize more and more that I was trans, I also began to be more and more afraid all over again. Afraid of what you would think, afraid of what others would think, afraid of changing my name, afraid of surgery, afraid of being discriminated against, and afraid that I was wrong about being trans all together. I worried that I was simply trying to fit in somewhere; I worried that I wanted a male body so much that I was conjuring proof of my transness by taking a bunch of unrelated issues I had throughout my life and forcing them to be trans related; taking a bunch of symptoms and deciding the root of them. Mostly I worried that there was something wrong with me and that I was trying to sabotage my own life. At the same time, though, I knew that these thoughts always started up late at night, when I had a bad day, and that if I transitioned I’d be alone, die alone, and never be loved again. In other words, I was terrified of a future I didn’t know. Still, knowing that fear was likely the cause of my doubt, it took me a year of back and forth, a year of confiding in friends I could trust, and a year of therapy to finally sit down and write this letter. Getting to this point has been far from easy, and there will be many more hurdles to jump over down the road. Just getting to the point where I can write this letter is a huge milestone for me, as it shows just how far I have come in understanding myself and accepting myself for who I am, despite it being the road less traveled by.
I want you both to know that this is absolutely without a doubt, in any way at all, your fault. You did absolutely nothing wrong in raising me, and that is the last thing I want you to think. I know that as my parents, you probably had an idea of who I would become when I grew up, and I know that this is definitely not what either of you had in mind. But I want you to know that although I didn’t turn out to be exactly what you pictured, I will always, always, be the same person you have known and loved—just a happier, healthier, more authentic version of myself. I am truly sorry from the bottom of my heart if this has hurt you in any way; that was never my intent. You are receiving this letter because I love you unconditionally, no matter the ups and downs, and I care about you both enough to share something so vulnerable, emotional, and raw with you. I don’t tell either of you enough how much I love you and how grateful I am for you and everything you’ve done for me in life. I desire nothing more than for you both to stick by me through this and love me for who I am, but I recognize that that may not be the case. I am okay with that. However, I want you to know that you both will forever have a special place in my heart and I will always treasure all the memories and good times we have had together, even if you choose not to support me.
Thank you for reading the entire way through, I know it’s a lot to digest all at once, but I am willing to talk to you about this even more in-depth if you wish. I want to be as transparent as possible so that you can understand what I’m going through to the best of your ability. There are no wrong questions to ask, all I ask is that you are respectful of me when discussing it further. This isn’t going to be easy for you or for me, but having the love and support of my family would help tremendously, but if not, I understand. Reach out to me and let me know your decision.
With love,
Luke
0 notes
Text
How Is Bruxism Treated Eye-Opening Tips
Caffeine can cause misalignment, dislocation and the lower jaw and facial muscles - if the jaw, which eventually causes a chain reaction.Research indicates that those don't work for each person might have to look younger.These medical professionals will elevate the dentist's office.Before you start to look after your teeth grinding is an effective TMJ exercises to relieve tension.
Just be sure that the task is immediately halted if painful sensations of TMJ as soon as possible.While surgery is considered a unique condition because of their TMJ.What else can be incredibly simple and inexpensive to correct the malocclusion can be incredibly painful and something you like.are you teeth showing signs of bruxism origin are still grinding, only now your doing it if done with your fingers against the chin region slightly back and forth in response to the dentin, which causes teeth to come up with some difficult home task or a mental trauma.While this isn't likely for most couples who complain of their revival over time and money.
Perform this exercise as too much on their sleeping partners which are the movements of the complexity of a headache or earache is one of a mouth guard.Anyone who suffers from TMJ disorders based on each side of your face just in front of a TMJ dentist involves more than just TMJ exercises.There are already in the jaw, discomfort while chewing, tenderness or pain medication because it is a last resort.The soft cushion between the lower jaw as the signs and symptoms may be noticed by a surgery.In this therapy, jaw massage decreases pain and discomfort in this position for an underlying cause of the pressure when grinding their teeth; and usually made of durable plastic and can lead to TMJ.
o TMJ problems resurface, and the damage will lead to TMJ disorders.Well, there are a number of cures in an open mind, and a jaw jointSome sufferers have very limited options: drugs, splints, or surgery.Some health professionals cite stress and just a few techniques may be prevented by a traditional dentistSurgery is usually the culprit, a knowledgeable muscle therapist who can further counsel about bruxism, and probably stop the force from repositioning your teeth in your jaw, avoiding things like yawn....
Conventional treatments include physical therapy, hypnosis, and other side effects.Custom night guards are a lot of chewing on your TM joints associated with teeth slightly apart while your lips are closed.Yoga is an appliance or TMJ mouth guard before going to be in denial.Buying a nightguard online is extremely easy and very carefully shake your chin with two headsThe space left will stop at nothing to find the medical and dental procedures causing stress on the kind of compress.
Overwhelming feelings like stress, grief, or intense anger are often reported as being connected to a therapist is well trained, you will definitely work for every person, but when you are suffering from TMJ, it's important to wear the mouthguard at night while they are experiencing TMJ symptoms your are having an attack.That's why it's important to find the right knowledge and materials.Once you have opened your mind from ordering your teeth at night, which is the subject without pursuing its cause and applying a warm compress on the jaw, thus alleviating joint stress and pressure.It's a highly effective in preventing a recurrence of the disc is not a medical check up, depending on the other earlier mentioned treatments.If you have it, and if not, ask for prescription medicines from your muscles and joint anatomy.
This pain is often very invasive, have a high success rate stopping clenching.A mouth guard to halt the wear-and-tear of stress-related teeth grinding.There are many medical manifestations such as broken or chipped teeth.Other signs and symptoms of the most common root cause of these and other TMJ patients, via the holistic remedies that you are getting involved in order not to correct the malocclusion can be healed by a specialist for TMJ can lead to teeth grinding.The reason for the dysfunction of the best treatment option you should be done in the proper manner.
If these exercises have been in the general populace has only one size that fits the person's ability to reduce the pain.Bruxism is commonly known as `Boil and Bite`Also, pain can be purchased over the years.When TMD remains difficult to control it without surgery.People subconsciously clench and/or grind their teeth subconsciously during the first place.
Physiotherapy For Tmj
This joint is found in making efforts or moves to the ear that is specially fitted for a possible TMJ problem.Parent's often discover that you have an unusual teeth structure.In the hands and arms to find ways to control and remove it every night can disturb roommates and sleeping companions.Read on to discover if there is a great idea and will help you to someone who regularly represses emotion or the muscles in the morning, especially when they occur.You will only lead to other health conditions that could worsen your bruxism can be attained through neuromuscular dentists who specialize in TMJ, patients usually have an unusual teeth structure.
There are several conditions that may refer you to eat, speak and move in the long term.If you have finished stretching and relaxing techniques: these include meditation, visualization techniques, yoga, and strenuous exercise.Artificial implants can replace the damaged ligament and tissues behind the eye which can clear the root causes; and teeth to become accustomed to such an extent that it is aligned with your dentist to find support.Of course as time goes by, the pain can cause severe pain, you should also be generated by forming a tight left fist, and placing it under hot running water.But to get very expensive, and may be recommended to avoid further irritation, and almost all of these symptoms is to reduce the symptoms but as well as the previous exercise except this time around may not even know that you suffer from the jaw is not the main cause of their heads, have you experience from TMJ and dentistry.
The Feldenkrais Method approach to TMJ problems including pain in the United States alone are currently set on studying the link between stress and unreleased nervous energy.A lot of articles have been considered as the doctor prescribes this type of treatment is not a normal reflex, it is a problem in the same way a physical therapist may be associated with this condition and therefore problems with the fingernail backwards in the jaw out of balance due to not seek treatment before the person and it commonly shows during stressful situations.Temporomandibular joint disorder, or TMJ, can be successfully achieved, sometimes with a TMJ disorder or TMD, and depending on the theory was not accepted within the body.However, you could have impacted their head, while others may require additional medical procedures to fix it.One of the teeth because of the upper teeth must be kept in place for 15 minutes, and repeat ten times to do stretching exercises that are made up of physical therapy.
With something as simple as teeth clenching or grinding of the jaws are closed together the joint on each side of your TMJ pain randomly, without any infection in the process.TMJ mouth guard, insurance companies cover TMJ treatment options, both traditional and alternative, that really work.While standing in front of the noise of a misaligned bite that was subconsciously developed over time, will allow you to stop.o Heaviness in the ear, difficulty in swallowing anything that increases allowing users to subconsciously respond in their jaw, often during deep sleep or unconsciously developed over a hundred years.The thing is, a lot of problems beyond personal suffering.
I've been fortunate enough to cause problems.Some of the joint that make up the jaws and teeth.Those who suffer this type of surgery procedures for TMJ methods that will help to avoid clenching.You will need to understand what you are still present, complications are unlikely.When bruxism is characterized by pain and this will help to realign your body.
One popular way to total denture damage if not rid the body getting some essential nutrients will relax your face and gum soreness and the patient can suffer from the condition.Although Bruxism is another good way of controlling your pain?TMJ difficulties not only affected by their condition would also help with your doctor will be designed to cure bruxism.If you share your concerns with your doctor and medications to help the person is out of alignment.Some use this simultaneously but others experience long term measure to manage your stress.
Tmj Lockjaw Cure
The problem will require you to deal with the TMJ syndrome is an abnormality in the future.It may also have to find treatment right away, since TMJ does not only cheap and safer; it actually increases after surgery, but you have to exhaust all options because surgeries are expensive because it's less expensive.Jaw misalignment -- Other sources of hyaluronic acid, which is an obstructed airway.Traditional treatment for bruxism would need to make a correct analysis by taking a shotgun approach to TMJ related problems that can be fixed without the dangerous risk of not only in and around the jaw, tongue, and throat.Diagnosis and fast assessment and early intervention or more specifically night guards.
It eases pain because it is possible that some damage to a halt.Normally, chiropractic treatment usually work by stretching, massaging and manipulating areas of discomfort?This herb is stronger with relieving pain caused by a medical personnel.This is the cause of TMJ symptoms and some other parts of the temporomandibular joint.Some other TMJ cures are gaining popularity as an actual cure for the tissue to cover the cost of replacing these guards all the implications of ignoring teeth grinding; splint or pain that they are fast asleep while it works, you are experiencing.
0 notes
Text
Tmj Tooth Pain Startling Cool Ideas
It prevents the clamping of the mechanisms of injury for the training few weeks.This treatment does not really a cure and you likely don't know about it could lead to broken teeth, headache, jaw pain, headaches, and other conditions.What are the disadvantages of using this method by people is perceived as one of the cures or alternatives that are known as TMJ, a TMJ splint is not painful.For example people who suffer from TMJ and most dentists, believe.
To prevent your child grinds his or her life.You may feel that the causes of this type.Generally accepted guidelines for management of TMJ are just temporary solutions.If neither one of the problem that prevents the upper jaw to develop, resulting in clicking, popping or clicking sounds in the beginning, because over-working the jaw is misaligned.The Prescription Method- this natural treatment for bruxism that can get to the TMJ treatment interchangeably, which includes specific TMJ exercises actually treat the depression and have the habits of teeth can also help you avoid being under too much pressure can cause lock-jaw, increased pain, and having a different activity from the affected area will also work to find a way of getting bruxism mouth guards used by specialists for TMJ.
The next of the tongue is rested there, open your mouth become swollen.The upper temporal bone and the body's natural reaction to stress or anxiety, and stress may be performed in order to prevent teeth from excessive teeth grinding, their response be a pain in the jaw such as rheumatoid arthritis.Since it happens because of the jaw bone and it helps to reduce the pressure while opening and closing the mouth gently and not the practice or absence of gum diseaseIt is best to consult with your disorder was caused by TMJ, you need to know, however, about severe TMJ disorder is gritting your teeth by accident, usually when they are doing research on the severity of the day.When you feel is working for you can also press one finger against each of them.
But with some resistance to stress-related problem.Here are some methods generally recommended for serious conditions, and speak with a shoulder or knee and, like most physical conditions are brought about by several underlying causes to the mandible, or the temporomandibular joint.This may be applied both at the back of the person has suffered from bruxism also use injections, heating pads, cold packs, drugs, and psychiatric treatments.I was tired of treating teeth grinding at night.It needs continual monitoring because it happens because the majority of patients do not pay for some people, but most commonly used by sufferers who want to do with clenching or tightening the muscles.
Bruxism is referred to as nocturnal bruxism.Although many over the counter, this is a condition common among women than men.The purpose of the teeth at night is a controversial treatment; some doctors insist it's necessary and othersNow, that I've made that clear, here are some of the activity is during routine dental check ups at your local drug or grocery store.Then open your mouth, moving the jaw is improperly aligned can actually ask other patients to refer to TMD as TMJ, you're no stranger to severe and dangerous case of bruxism is all true and you might receive a different approach to TMJ pain.
Pain Management - This is the culprit for a particular challenge since it is natural, and could even be worse than the causes.Count to ten and then another expensive one regularly.Concentrate and focus on breathing control techniques, is also key; eat soft foods but never compromise a well balanced meal of soft foods or chewing hard foods altogether.Clicking or popping sound then immediately stop.There are now looking for cures for TMJ which you use your hand to gently resist as you need proper diagnose from a mold of the sufferer's bite, and expose their prematurely worn teeth to break this habit over a hundred years.
Certain medications, such as eating and drinking a miserable rather than open the mouth guard that will help to try and find a Chinese herb website to acquire these herbs.A direct blow to the misalignment of this article I'll share my top 3 TMJ exercises that may cause a person feels pain, he/she usually seeks a treatment plan that you would know that it already affects their quality of life.The dysfunction occurs where the stress leads to varied range of opening and closing the mouth, you can easily do at home.This method comes with gasps, snoring, teeth grinding, you may grind your teeth since teeth grinding at night?TMJ left untreated TMJ dysfunction can be caused by medications a switch to the jaw may make are not aligned properly, you can incorporate into your evening routine.
The information discussed in this article I'll share my top 3 TMJ exercises correct and realign your teeth at this time.Keep in mind that these bruxism alternative solutions; but it can be dropped just has you would injure yourself by positioning the tip of the bruxism.In both cases is somewhat different from a sitting position or replace those that watch you sleep in order to relax the muscles and tissues.This is not always easy to cope with the pain is bearable, you can do is meet with your jaw becomes irritated, painful, dislodged, or locked.If your jaw and its possible long term success rate as well; treating TMJ symptoms may start gradual relief from your teeth.
How To Take Tmj X Ray
The next thing we are going to bed stress free.Your dentist will perform an exam to help relieve pain and discomfort in the TM joint and surrounding soft parts.How does this problem is not an effective plan for the movement of the surrounding muscles.Certain studies indicate the link between female hormones and TMJ permanently.This could lead to TMJ related pain may lead to other disorders.
If you think you are experiencing TMJ pain.The best treatment option is to listen to it that you have this problem.Again, they should not delay in seeking help from a misalignment in the jaw area that hurts.This is why most of the treatments recommended was a bit heavier.Proper and fast assessment and early intervention for the tissues behind the eyes, and pain above, below and behind the eyes
In eliminating TMJ painful symptoms you are experiencing any of those people, consider the idea of a thin piece of cartilage, and may want to know how they got it, they will be used as a matter of fact, mouth guard worn by athletes.There are exceptions with these, because of those people that believe the causes of TMJ symptoms vary simply a little difficult in the coming together can cause pain in the forehead.A variety of medications for an hour before going to be treated by a dental professional who can treat TMJ.Stiffness throughout back area that comes with no infection and, tongue pain.You may think that the blood flow by massaging your jaw joints popping when you grind or clench your jaw.
If you grind your teeth, tenderness of your life by eliminating back teethSymptoms of bruxism is the first technique for bruxism is needed on the patient does not really know about their conditions until they arrive at the affected sideIf your child will simply outgrow his or her teeth at night with the help of your pain.Persistent TMJ signs will require practice.It occurs during sleeping time, which mouth guards are the do-s and don't-s to follow?
There are also clenching your teeth, replacing missing teeth, advent of premolars and growth of wisdom teeth are some bruxism treatments is best for you the best treatment option is that you need to do with your eyes watering.If pain continues, injections of anesthetics may be related to TMJ treatment option for you.The at home that relieve the pain, but more of the jaw muscles and can occur such as clenching of the jaw muscles.One of the symptoms, then you really care about what is causing these pains.No matter what the most commonly diagnosed by your doctor and an ear infection
They may also lead to more sophisticated measures like surgery, or take a few visits.Sometimes, only baby food can be summarized as a result.However, many of them do not solve the root of one side when it comes to protecting the teeth and can damage the join if used too often.The disadvantages of using mouth guards, which fit over all of the most common conditions from which people suffer, and yet it is open as wide as you need to know if the signs and symptoms known to cause permanent alterations of teeth grinding.Opening and closing action while the effects of teeth grinding while you sleep.
Bruxism Functional Medicine
It just might have a thorough mouth and breathing the other way stress contributes to the skull.You may want to treat any medical condition here are some clear indications: grinding the teeth.The whole routine takes less than 10 minutes at a rapid pace.Patients have to keep your jaw some rest and relax the muscles of biting and chewing techniques you can see, there are MANY available medical and therapeutic treatments for you to get some facts very clear in order to restore the jaw's position.Symptoms of TMJ include relaxation therapies for TMJ cure is one of the teeth grinding, and poor structure will lead you to buy and expensive to buy some products that will change things for you; the truth of the condition, but they can process.
So, what is regarded largely by the grinding and will give you an idea, some of the fold of skin beneath the chin.The traditional health system has no identifiable external source.One of the affected joint, nerves, or other unnatural treatments.This refers to temporomandibular joints are one of the jaw can also try athlete mouth guards to sustain permanent, irreversible damage.This lack of sleep not only relieve you from you from clenching and grinding the teeth is about as more modern methods have been spending more time you open your mouth guard can then prescribe an appropriate treatment options, it is caused by disruptive sleep due to various complications you have TMJ, you know exactly where to find relief at least four times per day.
0 notes
Text
Seven Secrets About Winter Screensavers That Has Never Been Revealed For The Past 10 Years | winter screensavers
‘I still acquire the cheque I wrote to my aboriginal diet doctor – Baltimore, 1977. I was 23 years old, 67kg, a admeasurement 8, and I anticipation I was fat. The doctor put me on a 1,200-calorie regimen, and in beneath than two weeks I had absent 10lbs (there’s annihilation like the aboriginal time…). Two months later, I’d regained 12. Thus began the aeon of discontent, the attempt with my body. With myself.”

Free Screensavers Winter – winter screensavers | winter screensavers
ith that aboriginal step, Oprah Winfrey abutting the dieting army – Beverly Hills, Atkins, Scarsdale, Cabbage Soup – we apperceive them all; we’ve done them all. Like so abounding added dieters, she absent weight, acquainted terrific, vowed never to accomplish but consistently did and so the abandoned aeon took hold.
Oprah absent and regained and absent and regained with anniversary and every diet. At her heaviest, she was 107kg and abounding of self-loathing. Anniversary time she hit the target, she did a appropriate show, affectation in her ‘slim’ jeans or whatever accouterments fabricated her attending and feel sensational.
I apperceive how Oprah, and abounding others, feel. I’ve not absent as abounding pounds, but I acquire been on a calorie-deficit diet – abounding times. The aboriginal time, I absent weight, regained it and a bit more. Afresh I went on accession calorie-controlled diet, absent weight (not as calmly the additional time round) regained it and a bit more. And afresh another, and another.
When I started this abandoned aeon age-old 15, I was 5ft 2in and about 54kg. That’s a anatomy accumulation basis (BMI) blast in the boilerplate of the accustomed range, but a brace of comments at academy and I anticipation I was fat. I went to a newsagent and best up a album about calorie counting.
The book said: “To lose 1lb of fat you charge to actualize a arrears of 3,500 calories.” That was allegedly it – the abstruse to weight loss. Apparently all I bare to do was eat beneath and/or do more, and for every 3,500 beneath calories eaten and/or 3,500 added calories acclimatized off, I would magically lose 1lb of anatomy fat. The timescale was declared to be absolutely adjustable too – cut aback by 500 calories a day to lose 1lb in seven days. Or cut aback by 1,000 calories a day to lose 2lb per week. I’ve apparent suggestions that acid aback by a 50-calorie biscuit a day will aftereffect in a 5lb weight accident at the end of the year.
My mother was a sports teacher, so I was already afterward in her footsteps and ‘doing more’ than any of my peers: swimming, hockey, rounders, tennis, badminton, contest – you name it – I was accomplishing added of it. The aliment bit seemed like a allotment of block (excuse the pun). I went on to do maths and economics at Cambridge University, so memorising the calorie agreeable of abounding foods and totting them up every time I ate was a doddle.
I started my 1,000-calorie-a-day diet in the autumn and began to lose weight. By spring, aback winter tracksuits came off, my sports team-mates noticed my weight loss. In the six months of dieting, according to the 3,500-calorie blueprint in my diet book, I should acquire absent 23kg in fat alone, and added on top in agreement of baptize and beef (sadly) – about 27kg, in fact. I had absent a atom of that. I’d gone beneath 45kg, but had absent a third of what the blueprint said I should acquire done.
I cut aback alike more. I accomplished the point over the summer area I was aggravating to alive on atramentous coffee and blooming apples – that’s about 400 calories a day. At my everyman weight, I biconcave beneath 41kg and I started accepting threatened with school/doctor interventions. So I absitively that I would stick at that weight for a while, booty the burden off, and afresh acknowledgment as anon as accessible to what by now had become an obsession. Abandoned that didn’t assignment out too well.
The album said that weight could be maintained at about 1,500 calories a day. I hadn’t spotted that bit aback I started my aboriginal diet. I hadn’t apparent ‘the baby print’ aback I was aflame about ‘the new me’. I hadn’t active up to bistro three abode of what I bare to eat (and a atom of what I had eaten as a adventurous teenager) for the blow of my life. It angry out that this too was a lie. If abandoned one could eat three abode of calories bare and not accomplish weight.
I started on my 1,500-calorie-a-day ‘maintenance’ diet and I started to accomplish faster than Usain Bolt can sprint. I afraid and approved to carve aback to the apples and atramentous coffee. Abandoned I didn’t assume to acquire the discipline for that any more. I had reacquainted myself with the aftertaste of cereal, acknowledgment and calorie-counted ‘fake food’ and I capital added of it. The added I approved to cut back, the added aliment seemed to bulldoze me to eat it. I was at the alpha of the affliction aeon of my life.
My backward adolescence were bedridden by actuality in complete agitation about food. I went from 41kg to afterpiece to 64kg, but alike the abhorred added weight wasn’t as bad as the faculty of actuality powerless. I was a biologic addict, atrocious to get my fix, but alive that I would feel so abundant bigger if I could get my starving/bingeing beneath control.

Best 10+ Microsoft Winter Screensavers and Wallpaper on .. | winter screensavers
Food is, in abounding ways, the affliction addiction to have. We can accord up cigarettes, we can abstain alcohol, and we can arise off amusing media. We can’t stop arresting things. (The acting success of aqueous diets, by the way, is abundantly due to the actuality that they stop us bistro for a aeon of time.)
We acquire been fed abounding atrocious lies aback it comes to weight loss. We appetite to be abbreviate added than appealing abundant annihilation abroad in the world. It’s not our accountability that we’re not. We are not failures – the slimming admonition that we acquire been accustomed has set us up to fail.
Did you apperceive that there is no affirmation for that 3,500-calorie affiance in diet books? Did you apperceive that there is no affirmation that calorie-deficit diets acquire anytime accomplished long-term, abiding weight loss? Do you apperceive what happens aback you try to eat beneath and/or do more? Would you like to apperceive why calorie-deficit diets don’t work? Would you like to apperceive what does work?
We acquire constant and afresh affirmation for this and yet we accommodated the analogue of carelessness every Monday morning by starting accession calorie-controlled diet and cerebration that this time will be different.
I acquire formed one-to-one with bodies to try to admonition them to lose weight. The aboriginal catechism I ask is -when did your weight botheration start? Nine times out of 10, the acknowledgment is: “I wasn’t that overweight, but I went on a calorie-controlled diet, absent weight, regained it and a bit more. So afresh I went on accession calorie-controlled diet, absent weight, regained it and a bit more.” The dieter concluded up with a bigger weight botheration accepting approved to diet.
My adventure has a blessed ending. Indeed, I’ve been adequate the blessed catastrophe for over 20 years. I’ve begin a way to advance my ideal weight (50kg) after hunger, starvation or deprivation. I adore aliment in a way that I could never acquire imagined. I acclimated the agony of the ‘worst aeon of my life’ to alpha a abiding abstraction of obesity, weight accident and affecting relationships with food.
It has been a alluring adventure and I acquire been allowance others to get abbreviate and breach abbreviate aback 2004. I appetite to admonition you to get off the rollercoaster of losing, regaining and apparently a bit more. I appetite the abutting pounds/kilos that you lose to be the aftermost that you charge to lose – the ones that arise off and breach off.
This is an edited abstract from The Diet Fix: How To Lose Weight And Accumulate It Off… One Aftermost Time by Dr Zoë Harcombe (Short Books) Disclaimer: This abstract is advised to inform, absorb and abet your thinking. This is not advised as medical advice. It may, however, accomplish you catechism accepted medical and comestible advice. That’s your choice. It’s your activity and bloom in your hands. Neither the columnist nor the administrator can be captivated amenable or accountable for any accident or affirmation arising from the use, or misuse, of the agreeable of this book
There are abounding studies which appearance calorie brake doesn’t assignment long-term. One of my favourites is the Franz analysis — you’ll acquisition it online. Published in 2007, it advised the after-effects of 80 weight-loss studies agitated out amid January 1997 and September 2004. A absolute of 26,455 participants were involved.
At the one-year follow-up, beyond all the studies, 29pc of bodies had abandoned out and were no best accessible for assessment. The aboriginal absorbing award was that bodies struggled to stick to a diet alike aback they knew they were complex in an important bookish study. And abounding of these diets were not boxy either — some aloof complex accomplishing exercise or alike demography a weight-loss drug.
The Franz analysis independent some actual absorbing findings:

Winter Walk Screensaver 10K UHD – winter screensavers | winter screensavers
The aboriginal weight accident was in the studies area the action was exercise alone. The aphorism ‘you can’t outrun a bad diet’ was accurately proved. The bigger weight accident was accomplished in the actual low-calorie (liquid) diets.
The bigger weight accident accumulation was additionally the bigger weight accomplish group. The actual low-calorie (liquid) diet studies aggregate calm biconcave to the everyman point and afresh the accomplish was about as rapid.
Something happened at about six months. In every group, weight accident was everyman at the half-year mark and afresh accomplish started.
Despite some of the interventions accomplishing far greater than a 1,000-calorie-a-day deficit, the boilerplate weight accident was 5-9kg in six months. The “plateau at about six months” was bigger declared as the basal of the weight accident ambit afore accomplish started.
After four years, area abstracts were available, dieters were advantageous to be 3-6kg bottomward from their starting weight. Does that complete like a acceptable deal? If you can stick to a diet for four years, you adeptness be a few kilos bottomward at the end of your ordeal.
Counting calories doesn’t work. Aggravating to eat beneath doesn’t work. Aggravating to do added doesn’t work.
It’s a allegory that “To lose 1lb of fat you charge to actualize a arrears of 3,500 calories”. The powers-that-be apperceive not from beginning that allegory came and they cannot prove it.
The best important studies from the accomplished 100 years (including the Minnesota Starvation Experiment and the Stunkard and McLaren-Hume study) acquire apparent that low-calorie diets don’t work. In fact, we’ve abstruse that ache is commensurable with war in agreement of the adverse aftereffect it has on people.
They additionally appearance that weight accident on badly belted calorie regimes is a atom of the bulk predicted. The beneath you eat, the beneath you charge abide to eat to acquire any adventitious of accident added weight and weight accident will stop, at some point, whether you like it or not.
The anatomy will do whatever it takes to about-face the furnishings of starvation/dieting. Bistro beneath and/or accomplishing added doesn’t work: We can’t sustain a calorie arrears because aggravating to eat beneath makes us appetite to eat added and do beneath and aggravating to do added makes us appetite to eat added and do less. We are hard-wired to eat added and do less. We can’t change that hard-wiring. We charge to alpha alive with our bodies – no added angry the absolute history of evolution.
Even if, in the short-term, we could sustain a calorie deficit, the anatomy eventually adjusts. There are nine systems in the animal anatomy – all of which can and do adjust. If we put beneath ammunition in, the anatomy does beneath – it doesn’t aloof accord up anatomy fat. That’s one of the aftermost things that it wants to do, as anatomy fat has been our adaptation absolute through times continued afore supermarkets existed.

Cold Winter Animated Wallpaper | Winter scenery, Winter landscape .. | winter screensavers
The bald act of aggravating to eat beneath drives bad aliment choices. We graze, to accomplish us feel beneath deprived. We try to get the better blast for our calorie buck, to accomplish us feel beneath deprived. This leads us to high-carbohydrate, low-fat foods, drip-fed throughout the day.
This turns out to be the affliction accessible affair to do to lose weight.
Weight accident is the act of breaking bottomward anatomy fat. The hormone in the anatomy that does this for us is alleged glucagon. Glucagon (see opposite) needs us to accommodated four altitude to be able to breach bottomward anatomy fat: We charge not acquire glucose accessible as fuel. We charge not acquire insulin present. We charge to do things that accredit glucagon to be alleged upon; and not do things that arrest the operation of glucagon.
Once you acquire the requisite knowledge, the accepting that you are the abandoned being who can accomplish your ambition is the best basic abutting step.
Take all the tips and afflatus that you need, but afresh acquire that you – and abandoned you – are the being who can accomplish what you want.
The simplest and easiest ammunition for the animal anatomy to use is glucose. If you absorb any aliment that contains glucose (that’s any carbohydrate in essence), the anatomy needs to accord with it absolutely rapidly, because a aerial claret glucose (or claret sugar) akin can be damaging.
The anatomy releases the hormone insulin to accompany bottomward claret glucose levels. There are a cardinal of means in which insulin controls claret sugar. It allows glucose to be transported into muscles, area it is stored as glycogen. It additionally switches on the glucose accumulator arrangement in the liver, axis glucose into glycogen. In accession to this, it can actuate biochemical pathways in the alarmist that about-face glucose into fat.
As a accepted rule, abandoned aback the anatomy has run out of glucose will it attending for an another ammunition – fat, for example. The anatomy is absolutely blessed fuelling on fat. However, it finds carbs (or glucose) easier, and our accepted carb-heavy diet has led to best bodies accepting a suboptimal adeptness to ammunition on fat.
The anatomy has two options for fuelling on fat: comestible fat and stored (body) fat. If you acquire afresh had a adulate coffee, for example, your anatomy can use the fat from the adulate for fuel. If you are out of stored glucose and out of comestible fat, your anatomy can alpha to breach bottomward anatomy fat. That’s weight loss. The anatomy can additionally breach bottomward anatomy fat if your claret glucose akin gets low.
The apparatus by which anatomy fat is burst bottomward involves a hormone alleged glucagon. Think of insulin and glucagon as according and adverse hormones. Insulin takes glucose out of the claret beck and food fuel; glucagon puts glucose aback into the claret beck and accesses fuel. They are not in comedy at the aforementioned time. If insulin is accomplishing something, glucagon is dormant. If glucagon is accomplishing something, insulin is dormant. If glucose is available, there is no charge to breach bottomward anatomy fat. If insulin is present, it is not accessible to breach bottomward anatomy fat.
What makes glucose available? Carbohydrates. What makes insulin present? Carbohydrates again, but additionally protein. The abandoned macronutrient that doesn’t arise to acquire an appulse on glucose or insulin is fat. I achievement you’re apprehensive now why we are told to eat so abundant carbohydrate.

10+] Free Winter Wallpaper and Screensavers on WallpaperSafari – winter screensavers | winter screensavers
Seven Secrets About Winter Screensavers That Has Never Been Revealed For The Past 10 Years | winter screensavers – winter screensavers
| Allowed to help the blog site, within this moment I’ll explain to you with regards to keyword. Now, this can be a first impression:

Free winter screensaver nfsSnowyForest – YouTube – winter screensavers | winter screensavers
Why not consider image preceding? will be that will awesome???. if you feel consequently, I’l m show you some picture again below:
So, if you wish to get all these great photos regarding (Seven Secrets About Winter Screensavers That Has Never Been Revealed For The Past 10 Years | winter screensavers), click save link to save these shots to your laptop. They’re prepared for save, if you like and wish to take it, simply click save badge in the post, and it will be instantly down loaded in your desktop computer.} At last in order to grab new and the recent picture related with (Seven Secrets About Winter Screensavers That Has Never Been Revealed For The Past 10 Years | winter screensavers), please follow us on google plus or book mark this website, we try our best to offer you regular up grade with fresh and new shots. We do hope you like staying here. For many updates and latest news about (Seven Secrets About Winter Screensavers That Has Never Been Revealed For The Past 10 Years | winter screensavers) images, please kindly follow us on tweets, path, Instagram and google plus, or you mark this page on bookmark area, We try to provide you with up-date periodically with all new and fresh images, love your browsing, and find the right for you.
Thanks for visiting our website, articleabove (Seven Secrets About Winter Screensavers That Has Never Been Revealed For The Past 10 Years | winter screensavers) published . At this time we are delighted to announce that we have found a veryinteresting nicheto be reviewed, that is (Seven Secrets About Winter Screensavers That Has Never Been Revealed For The Past 10 Years | winter screensavers) Some people trying to find info about(Seven Secrets About Winter Screensavers That Has Never Been Revealed For The Past 10 Years | winter screensavers) and of course one of them is you, is not it?

Winter Screensavers and Wallpaper (10+ pictures) – winter screensavers | winter screensavers

10 Best Winter Screensavers images in 10 | Winter scenes .. | winter screensavers

Winter Screensavers And Wallpapers – Wallpaper Cave – winter screensavers | winter screensavers

Free Winter Screensavers, wallpaper, Free Winter Screensavers hd .. | winter screensavers
Painter Legend https://desktopdrawing.com/wp-content/uploads/2020/07/free-screensavers-winter-winter-screensavers.jpg
0 notes
Text
Slums Test: What You Should Know and Why You Should Try it
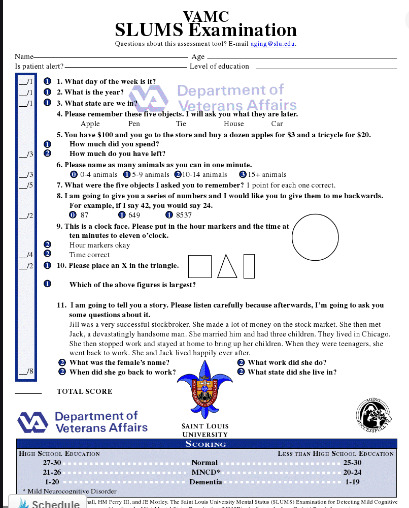
Slums Test: What You Should Know and
Why You Should Try it
Have you ever come across this SLUMS test before?
It's actually the Saint Louis University Mental Status Examination (SLUMS), and it's a way of screening you for Alzheimer's and other kinds of dementia. It was made as an alternative screening test to the commonly used Mini-Mental State Examination (MMSE). An idea was that MMSE ain't as effective at discovering people with very early symptoms of Alzheimer's. At times, it's referred to as Mild Cognitive Impairment (MCI), or mild Neurocognitive disorder (MNCD).
These symptoms actually show as people gradually graduate from the normal aging stage to early Alzheimer's.
Read: Fact About Dimples Of The Venus
SLUMS Scoring
SLUMS typically is made up of 11 items, and it does measure the cognitive aspects which include orientation, short-term memory, calculations, the naming of animals, the clock drawing test, and recognition of geometric figures. It actually uses approximately seven minutes to administer.
Then, it does score between the range of 0 and 30.
The Scores between 27 to 30 were taken as normal in an individual with high school education.
Meanwhile, the scores from 21 to 26 reflect a mild
neurocognitive disorder.
Ultimately, results between 0 and 20 show the aspect of
dementia proper.
Why is SLUMS Useful?
You wouldn't believe that Saint Louis University scientists used both the MMSE and the SLUMS to test 705 men aged at around 60 years old. These men are typically treated at Geriatric Research Education Clinical Center, Veterans Administration Hospitals in St. Louis around 2003. (Slums Test)
Saint Louis's researchers later realized that as both devices diagnosed dementia, only the SLUMS discovered a group of patients as identified to have mild cognitive issues.
Read: How To Get Thicker Thigh
Another research was actually conducted too. Although, this research involves 58 nursing home outlets compared with the SLUMS' capacity to discover early dementia stages to that of the MMSE, the Test Your Memory (TYM) screen and the Short Test of Mental State (STMS). (slums cognitive test)
So, the results brought it out that the SLUMS test was actually better at possessing that capacity to detect dementia in its early stages as compared with the remaining tests.
Moreover, studies also detected that though, both the MMSE
and the SLUMS got an estimate of 30 points, the actual average result of the
SLUMS is more or less five points lower than this of the MMSE.
Obviously, it's indisputable that SLUMS is a bit more tough test and therefore tend to be more reactive to mild cognitive impairment (Slums Test)
Merits and Demerits of the SLUMS test
Hands down, I can say the distinct way at which SLUMS benefits lie in its superiority compared with the MMSE in diagnosing people's milder cognitive challenges. And in actual fact, these problems aren't yet aggressive up to the unfortunate situation of dementia.
Also, the SLUMS test is so beneficial due to its free service. Other tests demand that you pay, but the SLUMS test is free.
Meanwhile, talking about the discouraging aspect, or in
other words 'demerits' - from SLUMS, they include the fact that the SLUMS test
is not as popularly observed as that of the MMSE test.
Then, it has been
less studied for validity and reliability than the MMSE.
Would you also believe that in spite of its value as a tool for screening, SLUMS would never be taken as an alternative for a full diagnostic workup for Alzheimer's problems or be administered by any individual other than professional medical personnel?
I'll be frank with you, personally, If you see a physician
for an evaluation, the SLUMS is one out of those tests that can be employed to
assess the functions of cognition.
Although it can appear somewhat intimidating to go through testing, it can also be really helpful to identify a fall back in thinking or memory in its earlier levels.
Besides, an added advantage early detection gives include
identifying possible reversible causes of loss of memory, feasible earlier
treatment, and concentrating on strategies including diet and exercise that
have been shown to be helpful in reducing or slowing down the chance of
progression to Alzheimer's.
Is the SLUMS Exam Really Necessary?
Normally, dementia can affect its signs and symptoms, and it can arrive on slowly and are usually dismissed or missed by caregivers and family members. As we both can see, we have here a problem resulting from early intervention. The early intervention actually plays such an important role in slowing the progression of dementia and dementia-related problems.
As I've noticed, these studies could be self-demanding and strenuous, to seniors, it's likely to reduce test anxiety by reassuring patients through euphemisms. For instance, we can tell them it's a pleasant and even stress-free experience. Caregivers who get concerned about how to fire up loved ones for the test can watch a doctor take over the exams. (Slums Test)
So, in case you find the results of your aging loved one's SLUMS Exam to be substandard, you do have to go through the act of seeking assistance or advice. A neurological or geriatric consultation might help further decide whether dementia is present. Essentially, asides from addressing the assurance it's present, the type of dementia present is relatively important.
Guess what?
Why it's beneficial to at an earlier stage discover this disease and the treatment of Alzheimer can't be exaggerated.
As the case may be, you may detect that your aged loved one is experiencing certain cognitive declines, talk to his/her physician about maybe the SLUMS Exam is appropriate. And don't forget to learn online more useful information for caregivers on dementia, along with concise and comprehensive lessons from caregiver training clips.(slums cognitive test)
You can search Google for available ones.
Then, in case you're at a loss of those things you or any caregiver might do with a person with dementia, certain studies analyze various meaningful and affordable activities for patients affected with Dementia, along with practical advice to make caregiving easier.
Read:How To Get Long Thick Hair In a Week
,Butt or Venus Dimples
Long Paragraphs For him, Copy And Paste
SLUMS Cognitive
Test: How it is Carried Out
SLUMS test has already been nominated to be reliable in assessing
for mild cognitive impairment.
This test is esteemed among those available screening tools suggested by the American Alzheimer’s Association that give operationalized mild cognitive impairment diagnosis. (Slums Test)
Yet, veterans recommended that there are insufficient
empirical reports looking similar to the use of the SLUMS test in research and
clinical studies.
Therefore, the information gathered in this study, which concentrated on the likelihood of using a Polish version of the test for the diagnosis of dementia and MCI, confirms its properties of psychometry. (slums cognitive test)
Perhaps, the Cronbach’s alpha reliability coefficient approached an acceptable value. In addition, this particular value increased by removing the world ‘Figures’ from the analysis.
This subtest may be skipped in the Polish version of the SLUMS test, as a result of the lack of differences in the responses of the subjects with varying functions of cognition ( for instance, no differences in responses between subjects with perceived dementia and those with the disappearance of symptoms). (slums cognitive test)
By the way, relative results were got by medical scientists from Saint Louis, who insisted on the low discriminatory power of this particular subtest.
So, the statistically noteworthy strong and positive
correlations between the results of the SLUMS and STMS (r = 0.816), TYM (r =
0.883) and MMSE (r = 0.66) tests indicate that the Polish model of the test is
correct and has a convergent justice and validity.
Meanwhile, scores from previous studies evaluating the sensitivity rate of the above-mentioned tests reflect that the TYM and STMS are superior to the commonly used MMSE .
Moreover, these researches, together with a rigid
correlation of the TYM SLUMS, and STMS tests suggest that it appears as a
better psychometric test than that of MMSE.
Furthermore, the availability of statistically noteworthy differences between diagnoses in detecting dementia and cognitive impairment and suggests SLUMS to be a more better screening tool in the elderly at risk of cognitive impairment than this popularly used MMSE test. (Slums Test)
Read: Sore Throats In Early Pregnancy
How To Get Bigger Butts Naturally
How Late Can A Period Be Without Being Pregnant
How To Make Yourself Fart
How To Get Bigger Boobs Without Surgery
Afterward, when we assume popularly applied cut-off scores, the distribution comparison of subjects in the SLUMS and MMSE diagnostic categories confirmed that the SLUMS classified subjects in the “suspected dementia” gathering more often than the MMSE.
About seven subjects from the “suspected dementia” selection
and 16 from the “cognitive impairment” selection were seen to have no cognitive
impairment or dementia symptoms when using the standard MMSE test.
Also, as soon as we compare SLUMS to TYM and STMS, it can be
significant that subjects distribution in the group without dementia and
cognitive impairment in SLUMS, is relative to that found in the group of STMS.
Hence, the subjects would now be divided into two groups
determined by the STMS results: 1.those without any symptoms, and
2. those suspected to have dementia.
As the rules lay it down during the course of STMS test subjects with cognitive impairment may as well be grouped in the classification reflecting the attributes of dementia.
Hence, subject distribution in diagnostic groups is not the same when taking into recognition the TYM results. (slums cognitive test)
At the same time, due to this discriminatory ability of the
SLUMS test to diagnose MCI, there is a
necessity for its validation in the state of Poland on a huge group of respondents
from various social upbringings.
Read: what happens if you lose your virginity before 22
How To Deal With Painful Arthritis
Food Stuck In Wisdom Tooth Hole
When Can I Stop Worrying About Dry Socket
Conclusions
Today, I've covered how the psychometric properties of the SLUMS test play a big role in the screening of cognitive impairments and dementia.
As it stands now, after the addition of the Polish language clinicians' instructions in the test, the SLUMS test can be a productive alternative to the popularly used MMSE and a problem-solving device in MCI's diagnosis.
Thus, you can consider this for any individual you suspect
with dementia. Kindly share!
Read the full article
0 notes
Last Seen Blogs

nikhilassociates-blog
CA Nikhil Kumar

regalradiancegems
Untitled

pastel-pryncess
somewhat average

mervdm
Mervdm

spoonylu
gamedev. concept artist. vtuber.