#developmental delay treatment
Text
Developmental Delay Treatment | Developmental Delay in Children
At Chaitanya Speech Therapy Center, we offer specialized treatment for developmental delays in children. Our expert therapists use innovative techniques to help your child reach their full potential. Learn more about our comprehensive developmental delay treatment today. Developmental Delay Treatment Developmental delay is a term used to describe when a child does not reach certain developmental milestones at the expected ages. These milestones can include walking, talking, playing, and socializing. While every child develops at their own pace, some delays may require professional assessment and intervention to ensure a child's development remains on track.
0 notes
Text
At Cogniable, we believe in providing holistic care to children with special needs. That's why we offer specialized physiotherapy services to help children with cerebral palsy and other pediatric conditions improve their motor skills and achieve greater independence
#developmental delay treatment#neuro developmental therapy#occupational therapy for autism#screen for autism org#sensory integration therapy#down syndrome therapy
0 notes
Text
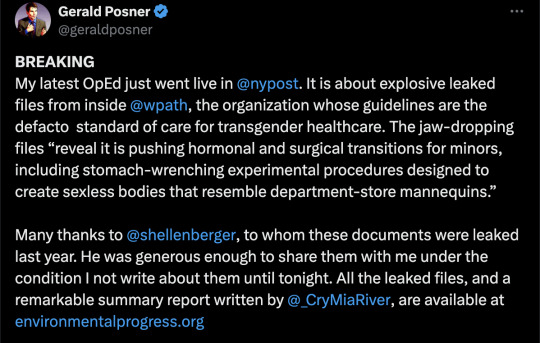

By: Gerald Posner
Published: Mar 4, 2024
Newly leaked files from the world’s leading transgender health-care organization reveal it is pushing hormonal and surgical transitions for minors, including stomach-wrenching experimental procedures designed to create sexless bodies that resemble department-store mannequins.
The World Professional Association for Transgender Health documents demonstrate it’s controlled by gender ideologues who push aside concerns about whether children and adolescents can consent to medical treatments that WPATH members privately acknowledge often have devastating and permanent side effects.
Yet the US government, American doctors and prominent organizations nonetheless rely on WPATH guidelines for advice on treating our youth.
The files — jaw-dropping conversations from a WPATH internal messaging board and a video of an Identity Evolution Workshop panel — were provided to journalist Michael Shellenberger, who shared the documents with me.
Shellenberger’s nonprofit Environmental Progress will release a scathing summary report, comparing the WPATH promotion of “the pseudoscientific surgical destruction of healthy genitals in vulnerable people” to the mid-20th-century use of lobotomies, “the pseudoscientific surgical destruction of healthy brains.”
‘Arbitrary’ age limits
The comparison to one of history’s greatest medical scandals is not hyperbole.
It is particularly true, as the files show repeatedly, when it involves WPATH’s radical approach to minors.
When the organization adopted in 2022 its current Standards of Care — relied on by the National Institutes of Health, the World Health Organization and every major American medical and psychiatric association — it scrapped a draft chapter about ethics and removed minimum-age requirements for children starting puberty blockers or undergoing sexual-modification surgeries.
It had previously recommended 16 to start hormones and 17 for surgery.
Not surprisingly, age comes up frequently in the WPATH files, from concerns about whether a developmentally delayed 13-year-old can start on puberty blockers to whether the growth of a 10-year-old girl will be stunted by hormones.
During one conversation, a member asked for advice about a 14-year-old patient, a boy who identified as a girl and had begun transitioning at 4.
The child insisted on a vaginoplasty, a surgery that removes the penis, testicles and scrotum and repositions tissue to create a nonfunctioning pseudo-vagina. It requires a lifetime of dilation. Was he too young at 14?
Marci Bowers, WPATH’s president and a California-based pelvic and gynecologic surgeon who is herself transgender, said she considered any age limit “arbitrary.”
But she would not do it. Why?
“The tissue is too immature, dilation routine too critical.”
In lay terms, that means boys who are too young do not have enough penal tissue for the surgery and the surgeon must harvest intestinal lining to build the faux vagina. Even Bowers admits that can lead to “problematic surgical outcomes.”
She would know since she has performed more than 2,000 vaginoplasties. Her highest-profile patient is 17-year-old Jazz Jennings, the transgender star of reality TV show “I Am Jazz.”
Three corrective surgeries were required to fix problems from the original vaginoplasty.
“She had a very difficult surgical course,” Bowers admitted in a 2022 appearance on the show. “We knew it would be tough — it turned out tougher than any of us imagined.”
Still, Bowers told her colleagues in the internal discussion forum of the best age for an adolescent to undergo surgery: “sometime before the end of high school does make some sense in that they are under the watch of parents in the home they grew up in.”
Christine McGinn, a Pennsylvania plastic surgeon and herself transgender, agreed. McGinn has performed “about 20 vaginoplasties in patients under 18” and thinks the “ideal time in the U.S. is surgery the summer before the last year of high school. I have heard many other surgeons echo this.”
Waiting until teens are older than 18 and in college is problematic, she said: “there are too many stressors in college that limit patients’ ability to dilate.”
Dangers downplayed
WPATH assures patients that surgical and hormonal interventions are tested and safe. It is a different matter in private.
President Bowers, for instance, said publicly in 2022 that puberty blockers are “completely reversible,” although in the internal forum she conceded it is “in its infancy.”
What about children who are infertile for life since they started hormone blockers before they reached puberty?
Bowers told her colleagues the “fertility question has no research.”
At other stages, members talk frankly about the complications for the transition surgery for girls, a phalloplasty in which a nonfunctioning pseudo-penis is fashioned from either forearm or thigh tissue.
It requires a full hysterectomy and surgical removal of the vagina. They also discuss other serious consequences, including pelvic inflammatory disease, vaginal atrophy, abnormal pap tests and incontinence.
A 16-year-old girl who had been on puberty blockers for several years before she was put on testosterone for a year had developed two liver tumors that an oncologist concluded the hormones had caused. Another member described “a young patient on testosterone for 3 years” who had developed “vaginal/pelvic pain/spotting . . . [and] atrophy with the persistent yellow discharge.”
Several colleagues described patients with similar conditions, some with debilitating bowel problems or bleeding and excruciating pain during sex (“feeling like broken glass”).
Vaginal estrogen creams and moisturizers as well as hyaluronic acid suppositories “can be helpful.”
One WPATH member seemed surprised: “The transgender people under my surveillance do not complain about this matter. However, I confess that I have never asked them about it.”
Rise of ‘de-gender’ surgery
The litany of transition surgery’s side effects did not stop WPATH from endorsing far more radical “nullification” surgeries for patients who do not feel either male or female and identify only as nonbinary.
Several dozen so-called “de-gendering” surgeries are designed to create a sexless, smooth cosmetic appearance that is unknown in nature. There is even an experimental “bi-genital” surgery that attempts to construct a second set of genitals.
In 2017, when tabloids reported a 22-year-old man had spent $50,000 to surgically remove his sex organs so he could “transform into a genderless extra-terrestrial,” it seemed a one-off oddity.
But WPATH has enshrined that concept in its Standard of Care — the same document in which the group endorsed for the time first time chemical or surgical castration for patients who identify as eunuchs. (WPATH even linked to the Eunuch Archives, where men anonymously share castration fetishes.)
These science-fiction-like surgeries are not only reserved for adults.
“How do we come up with appropriate standards for non-binary patients?” asked Thomas Satterwhite, a San Francisco-based plastic surgeon who has operated on dozens of patients younger than 18 since 2014. “I’ve found more and more patients recently requesting ‘non-standard’ procedures.”
What are nonstandard procedures? They include “non-binary top surgery,” a mastectomy without nipples. There are brutal procedures for girls that eliminate all or part of the vagina and for boys that amputate the penis, scrotum and testicles.
The goal, as one San Francisco surgical clinic proclaims on its website, “is a smooth, neutral body that is cosmetically free of sexual identification.” On TikTok the trend is called a “flat front.”
‘Too young to understand‘
A particularly intense subject of discussion was whether minors could understand the lifelong consequences of their gender treatments. Minors are presumed by law to be incapable of making an informed decision about having a vasectomy or tubal ligation.
Gender surgeries are an exception, however.
WPATH’s Standard of Care allows all procedures so long as the minor “demonstrates the emotional and cognitive maturity required to provide informed consent/assent for the treatment.”
In a May 2022 internal workshop, “Identity Evolution,” WPATH members conceded that was all but impossible.
Daniel Metzger, the British Columbia endocrinologist who cowrote the Canadian Pediatric Society’s position paper on health care for trans minors, said, “I think the thing you have to remember about kids is that we’re often explaining these sorts of things to people who haven’t even had biology in high school yet.”
Metzger noted adolescents are incapable of appreciating the lifelong consequence of infertility. “It’s always a good theory that you talk about fertility preservation with a 14-year-old,” he said, “but I know I’m talking to a blank wall. They’d be like, ‘ew, kids, babies, gross.’ Or, the usual answer is, ‘I’m just going to adopt.’ And then you ask them, ‘Well, what does that involve? Like, how much does it cost?’ ‘Oh, I thought you just like went to the orphanage, and they gave you a baby.’ . . . I think now that I follow a lot of kids into their mid-twenties, I’m always like, ‘Oh, the dog isn’t doing it for you, right?’”
There is extensive research showing adolescent brains are wired to have little control over rash behavior and are not capable of grasping the magnitude of decisions with lifelong consequences. It is why society doesn’t allow teens to get tattoos or buy guns. Car-rental agencies set 25 as the minimum age for renting a car, and Sweden sets the same limit for deciding on sterilization.
Detransitioners ignored, shunned
Although many WPATH members privately doubt that adolescents can give truly informed consent to life-altering procedures, they must affirm whatever children say about their gender.
Unless, the WPATH files disclose, the patient wants to reverse course and become a so-called detransitioner.
WPATH members mostly dismiss those cases as insignificant or overblown by the media and question whether minors who want to revert to their birth sex really understand what they are doing.
It’s a question that would never be asked for minors who declared themselves to be gender dysphoric.
One case involved a 17-year-old boy, just graduated from high school, who had been on testosterone for two years. He was reported to be “very distraught and angry. He reports he feels he was brainwashed and is upset by the permanent changes to his body.”
A self-described “queer therapist” did not believe any young person could be brainwashed. “In my experience, those stories come from people who have an active agenda against the rights of trans people.”
WPATH President Bowers said that “I do see talk of the phenomenon [detransitioners] as distracting from the many challenges we face.”
‘Frankenstein files’
The leaked files put a spotlight on the danger of mixing ideological activism with medicine and science. They should serve as an urgent wakeup call for the medical associations and government agencies that rely on WPATH guidance for transgender health.
The files might even prompt investigations into how those with distorted personal agendas seized control of the organization at the expense of science and patients.
Investigating what has gone wrong at WPATH might prove uncomfortable for some gender progressives in the Biden administration, none more so than Adm. Rachel Levine, the assistant secretary for health. Levine, the first transgender four-star military officer, is a WPATH member and has lavished praise on the organization.
She says it “assesses the full state of the science and provides substantive, rigorously analyzed, peer-reviewed recommendations to the medical community on how best to care for patients who are transgender or gender non-binary. It is free of any agenda other than to ensure that medical decisions are informed by science.”
Either Levine is unaware of the hormonal and surgical experimentation the group promotes or refuses to acknowledge it.
“The Frankenstein files.”
That is how a pediatrician described the leaked documents after I shared them with her.
Unfortunately, this is no horror novel.
It is a medical travesty playing out in real time, and the casualties are our children.
#Gerald Posner#Michael Shellenberger#WPATH#World Professional Association for Transgender Health#Mia Hughes#WPATH Files#The WPATH Files#medical corruption#medical malpractice#medical scandal#unethical#gender ideology#gender identity ideology#queer theory#first do no harm#religion is a mental illness
31 notes
·
View notes
Note
You've probably gotten a lot of messages like this before but I wanted to just thank you guys for showing a form of abuse that isn't only physical and still calling it abuse and not hand waving it away. So many stories that include abuse tend to assume that it only counts as abuse if it's physical. They ignore mental and emotional abuse entirely and if they do acknowledge it, it's portrayed as not that bad and something you need to forgive your abusers for.
As someone who's still coming to terms with my own experience with a similar kind of abuse that Adamant and Hope faced, your comic makes me feel seen and validated in my feelings and especially in my choice to cut off the family that hurt me. Seeing Adamant and Hope leave and not be shunned for it was such a relief and breath of fresh air after so much media tells you to forgive people who hurt you, especially if they are family.
again, thank you. I'm forever thankful this comic exists. you two are fantastic and I can't wait to see where the story goes :)
Thank you so so much, anon. We feel mixed emotions when we get asks like this because it's nice to hear but it's also so hard to hear our readers dealing with what we've dealt with and it's also hard to articulate how much we hear you and how sorry we are.
What you're saying is such a good point. Emotional abuse is so often discounted and watered down and even disregarded as being hurtful. It also doesn't help that even physical abuse gets the same treatment. Especially when it's just dismissed as 'discipline' or a 'loss of control'.
But going back to emotional abuse, this is one of the main things that we wanted to so desperately try and portray vs. how My Pride had portrayed it. The very idea that emotional abuse at the hands of your family isn't actually abuse because it's just them loving you and 'wanting what's best for you'.
Which is so ridiculous because overprotectiveness can very, very easily mutate into smothering and parents feeling that their children have zero agency or identity outside of themselves, especially if you're disabled. Parents like this don't deserve humanisation or sympathy. Their actions are possessive and unhealthy and may be a indication they're suffering from a form of abuse themselves.
My Pride could have tackled this with Powerstrike. She lost her mate and son. Her culture is heavily against her and her own sense of agency. However, the script is too busy highlighting how she feels 'weak' because her daughter is disabled and can seemingly do nothing to fulfil this unachievable image she has of her.
It's how you know the script was written by an able-bodied individual, somebody who will never know that this kind of thing makes you feel like utter dirt as somebody who isn't a "perfect" neurotypical, able-bodied individual.
Even if the creator is neurodivergent herself, this was such a huge ball to drop. Powerstrike saying 'whenever I look at you, I only see what you could have been' is very much a fucking Powerstrike problem and she deserves to rot for it. Being viewed under the lens of what you "could" be if you didn't have a physical disability or conditions that cause developmental delays like autism is downright devastating for those who have them and fuck that show for trying to humanise Powerstrike by having her spout such garbage.
There was nothing remotely sympathetic about that speech. It was just Powerstrike whining about having a disabled daughter and the context of the speech is that she was called out for not caring about her children and the creator somehow thinks that her child being disabled.... excuses that?
I apologise for going off on a rant, but Powerstrike's speech fits the bill exactly with what what you're talking about because MP fans have fallen for it hook, line and sinker and refused to see how gross it is because Powerstrike never physically abused Nothing like Quickmane did. Even though it is very obviously emotional abuse and manipulation.
It'd be great if we could just assume this is just superfans defending their favourite show's honour because god forbid something they enjoy is delivering problematic messages like how parents who have an ableist perception of their children deserve sympathy, but we've had people come to us and directly point to the show's writing as a reason for them failing to identify valid forms of abuse and therefore feel they cannot act upon it or seek help for it.
May not be what the creator intended because she was presumably high off her own fumes when she wrote speeches like Powerstrike's, but that's the reality and making excuses for it like MP fans have isn't going to make the issue get any better.
Doing this comic has allowed me to confront the same feelings you have also had to contend with, anon, and I'm very happy we have been able to share something together there. You and others like you also make me feel less alone and less angry about what I've experienced and I hope you never forget that. - RJ
38 notes
·
View notes
Note
What are your opinions on rapid evolution? Like say when a trainer feeds their pokemon candies to help them evolve instantly rather than gradually? Are there any adverse effects on the pokemon themselves? I'd assume it's just like forcing someone to instantly grow up rather than living out a childhood, right?
This is a pretty complex question, so let me start by giving the simple answer first:
It's a very bad practice and should be regulated a lot closer.

When it comes to pokemon growth, evolution and health you need to consider that they need time to grow into their final stages, and the time could be years spent with their trainer, allowing their body to strengthen and develop naturally.
Feeding a pokemon a bunch of "Rare Candy" artificially stimulates the natural energy pokemon output to conduct evolution.
Unfortunately, these "candies" are pretty easy to get your hands on and aren't seriously regulated because they actually have medical uses.
(You can also look up how to make them online as well)
These candies can be used if a pokemon us having some developmental problems in their evolution cycle, perhaps early evolution symptoms and signs but there's some kind of delay or energy imbalance, the candies can help stimulate this process to help them grow and evolve naturally.
Unfortunately these candies being medically useful, over the counter accessible and treatments for pretty simple issues have made them easy to get and easier to abuse, Unfortunately resulting in some pretty common problems for both trainers and pokemon.

While the benefit of the pokemon reaching its "maximum potential" way faster, some of the most common drawbacks of "Rapid Evolution" or "Candy Evo" are health defects like joint issues, breathing problems, heart and organ size difference, and under developed muscles and misplaced power output.
However, I am a huge advocate against raising training for the biggest drawback:
Delayed Mental Growth.
Unfortunately, a pokemon might evolve too quickly, and as a result, they are essentially a small pokemon in a large pokemons body, and its a lot more difficult to manage than you'd expect.
Personality disparity, random bouts or depression and fits of anger, and trying to find a way to explain to your pokemon that they can't fit in your lap or the small bed for them and now they need to sleep outside or in a less comfortable place.
It's all a lot that weighs on a person's mind and heart.

When I found Sylvester, he was alone, scared, and confused from his Rapid Evolution situation, after a child was gifted an Aron and used a ton of rare candies to help it evolve.
Apparently, she didn't know it would evolve into a large and heavy pokekon, and he wasn't as "cute," as she thought, so she abandoned him in Mt. Coronet.
This is also why I'm absolutely for education and NOT giving children Pokémon before they are trained and do some kind of camp beforehand.
Thankfully Sylvester has done so well in his over a year with me, and he is understanding his role and current situation in life, and has really become a joyful and loving ball of happiness who loves to dress fancy and serve people drinks st my Cafe.
He's always such a big help and a successful story of rehabilitation and coming together to turn a really bad situation into a loving family.
So please do not try and do a Rapid Evolution and discourage anyone you might hear talking about doing it. It really has a large chance not to end well.
#ranger rai#pokemon ranger#the ranger base#pokemon#ask me anything#ask me a question#sinnoh#sylvester#aggron#rai doodles#rapid evolution#dont take the easy way out for convenience
23 notes
·
View notes
Text
Deep dives into folklore: changelings

Changelings are a captivating element of folklore across various cultures, with stories of these enigmatic creatures appearing in European traditions and beyond. The changeling myth revolves around the idea that fairies, elves, or other supernatural beings would abduct human children, replacing them with their own offspring or elderly individuals. These substitutes would appear identical to the human children they replaced but would often behave strangely, causing confusion, fear, and distress among families. Understanding the changeling myth requires exploring its origins, its role in society, and its impact on cultural beliefs and practices.
The changeling myth likely originated in pre-modern societies as a way to explain unexplained or distressing occurrences, particularly related to children. This may include:
Infant Illness and Developmental Disorders: In times when medical knowledge was limited, unexplained changes in a child's behavior, health, or appearance (such as sudden illness, developmental delays, or behavioral issues) could have been attributed to a changeling.
Cultural Beliefs in Supernatural Beings: Many societies believed in the existence of fairies, elves, and other supernatural beings who inhabited the natural world alongside humans. These beings were often seen as mischievous or malevolent, giving rise to stories of abduction and replacement.
Fear of the Unknown: The changeling myth reflects a deep-seated fear of the unknown and uncontrollable aspects of life. The concept of a child being replaced by a supernatural entity could represent broader anxieties about loss, change, and the mysteries of existence.
The changeling myth had a profound impact on society in several ways:
Treatment of Children: In some cases, suspected changelings were mistreated or even harmed in an attempt to expel the supernatural being and bring back the real child. This was often based on the belief that the changeling would reveal itself under duress.
Impact on Mothers and Families: The myth could lead to blame and ostracization of mothers if their child exhibited unusual behavior or illness. This added to the emotional burden and challenges faced by families.
Cultural Narratives: Changelings became a common motif in folklore, literature, and art. Stories and ballads often depicted the struggle of families to reclaim their children or the strange behavior of changelings.
Symbolism and Metaphor: The changeling myth has been interpreted symbolically in modern times, representing feelings of alienation or otherness. It can be seen as a metaphor for the challenges of parenting a child with special needs or the experience of not fitting into societal norms.
In contemporary culture, the changeling myth continues to resonate, finding its place in literature, film, and other media. Modern interpretations often explore themes of identity, transformation, and the boundaries between reality and fantasy. Additionally, the changeling myth serves as a reminder of the dangers of superstition and the importance of understanding and compassion, especially for those who may be different or marginalized.
The changeling myth is a multifaceted and enduring element of folklore that has influenced cultural beliefs and practices throughout history. It reflects the deep-seated fears and anxieties of past societies while continuing to captivate the imagination today. By understanding the origins and impact of the changeling myth, we can gain insight into the complexities of human experience and the ways in which folklore shapes our perceptions of the world.
#writeblr#writers of tumblr#writing#bookish#booklr#fantasy books#creative writing#book blog#ya fantasy books#ya books#deep dives into folklore#deep dives#myths#legends#folklore#changelings#fae#faeries#elves
10 notes
·
View notes
Text
Im laying my bets now. the entire idea that autism (and adhd) is more common in men and boys is pure myth created by poor science, backwards statistics and faulty parameters of the condition itself. in another 50 years we will understand it was never a gendered condition. just a highly gendered and biased measurement system. i'm absurdly confident on that
the rates of autism in girls is "rising" exponentially. it is rising even more exponentially in girls than in boys. not because girls are becoming more autistic. but because the "science" is just getting better at measuring and accurately acknowledging autism in girls.
autism often does present differently in girls, due to how girls are raised or personality differences. the literature and criteria was based on boy sample groups. the entire research data was done on white men as if that is a standard default person and control group.
not only that, doctors and teachers and parents literally were not looking for it in girls under the false widely propagated belief it was rare in women in girls. it is a self fulfilling prophecy. that's not science.
we will soon have to reckon with the lost generations of autistic girls and women and children assigned female at birth* who never got diagnosis and early intervention. we should be forcing the world to reckon with it right now. a great deal of autistic millennial women are brilliant minds who dropped out of STEM and the workforce due to their untreated and misidentified disability overtaking their life. the impact of never Knowing you or your child is autistic or adhd is difficult to comprehend for autistic and adhd people who did get diagnosed as children. even when the awareness and interventions were unhelpful or harmful. the harm of not knowing means the child trying even harder to become neurotypical and a level of autistic burnout few others on the spectrum can comprehend, often taking place after the woman is a legal adult, and there are no legal protections in place for this disabled person.
the unmitigated stress of being developmentally delayed and never knowing it, simply hating and blaming yourself and fighting day in and out past your limits to become neurotypical, limits your don't know you should have because you have never been so much as briefed on what adhd or autism can feel like. you don't know the distres and tiredness you're feeling is "dysregulation". this is why we see women in nervous breakdowns. psychiatric wards. treatment resistant depression. electric shock therapy. hard drug addiction. cutting. homelessness. personality disorders. dissociation. psychosis. early death by accident or suicide. (obviously people who are not autistic or adhd have these illnesses but my point is untold and disproportionate numbers of them are undiagnosed neurodivergent with unprocessed trauma. i'm telling you. more than you think).
it's why we see young people on tiktok not faking DID per say, but describing a dissociated experiences and fractured sense of self and escapist alternate personalities, a mental illness that has much less in common with traditional DID, but has much in common with struggling and under-treated autistic people. DID is a very rare condition. autism is very common. autism can create out of body experiences and self protective blurring of reality and fantasy so extreme, no person can be expected to understand it is autism if they never been advised about their own disability and the knowledge that should he available to them. it's no wonder we have people with mislabeled rare disorders like DID who are clearly very sick but instead of showing real DID signs, are sick with all the signs of severe unassisted autism they have been completely barred from understanding or coping with in any other way. for those lucky enough, we see unemployed young women with severe chronic pain in their 20s and 30s who look and feel like they're elderly and gave up their dreams when they hit 21 or 25 and their brains stopped working and their bodies shut down. now they mostly scroll tumblr and tiktok and try to remember to open the blinds. they have a roof but people scorn them for entitled laziness and worst of all derided for "self diagnosing".
again i'm asking why CFS chronic fatigue syndrome is so responsive to adderall. i'm asking why professionals are reluctant to test women for adhd if she does well in school because she is very bookish and why experts in the field are openly amused and doubtful to test a woman for autism if she has a long term boyfriend. why is ability to mask or function a disqualification. why is inability to function in women, who later turn out to be autistic or adhd, so aggressively mischaracterized as BPD, bipolar, depression, OCD, schizophrenia. why is autism and adhd clinically diagnosed and defined by distress and dysfunction and not by intrinsic traits and qualities that present while still functional for preventative care. why are all people, men and women forced to wait until their lives and minds are deteriorating and they have experienced some irreversible disasters and pain before they can be diagnosed. why must girls and boys wait until their daily life as children have become unbearable hell for them before their disability can be treated and acknowledged. and if these policies are changing now, why are doctors and psychiatrists not eagerly and urgently reaching out to find the vulnerable adults they missed during more archaic screening methods. we aren't rising in adhd diagnosis because of tiktok you assholes. adult onset adhd and autism don't exist. those people were always adhd. adult onset skill regression and increase in severity due to stress DOES happen in adulthood. modern day stresses like loss of structure during the pandemic and social media is advancing to become more attention span draining. everyone is feeling the effects but these are causing adhd and autistic people to cope less and mask less effectively so they are running into significant problems, their loved ones are noticing, they are getting referrals and suddenly forced to google their rapidly worsening mental issues for the first time and seeing they line up with a known neurological condition . this is obvious. doctors blaming it on some sort of trend are being willfully clueless
*because autism especially is screened identified diagnosed and first intervened ages 2-5, before a child has an internal concept of self or gender and above all before they can express their gender, diagnostic practices and criteria are based on how adults perceive a child via birth assignments. and the studies are overwhelmingly beholden to data only on children assigned male at birth, rarely accounting for their actual future gender either. as part of the warped science insisting that autism is as if somehow linked to the y chromosome and not a universally likely human quality, you see amab kids laser focused on as candidates and afab kids fucked over most of all. all children assigned female have the worst chances of their developmental disability being identified and acknowledged in a timely manner and disproportionately experience late diagnosis in later adolescence or adulthood. tho i wouldn't be surprised if trans womens rates of accurate diagnosis is lower than cis men. as trans girls may present autism differently and characteristic of girls autism, even while still in the closet or before she knows she is trans. regardless adults are very vigilant for signs of autism, even atypical ones, in any child they perceive as a boy. so any millennial or gen z child identified female at birth had significantly worse chance at receiving autistic support compared to peers
in particular women assigned male at birth might have a better chance at being identified for types of autism that are often labeled "high functioning", involves high masking, and often receives few services. these more invisible types of autism often need to be diagnosed before age 5 in order to qualify under the criteria at all. and so in the days where autism was believed to be 20x more common in the genetics of xy children, any chance of being considered and diagnosed would come down to almost purely birth assignment dependent. with the less outwardly visible types of autism, a person who misses this window will remain autistic all their life but once they learn a certain level of skills and masking, no matter how late they learn these, the person will no longer qualify for diagnosis, either not until they have a nervous breakdown or possibly not ever qualify. it's this type of more hidden autism we see struggling across the board as undiagnosed adults including both trans and cis women especially, tho we are seeing it disproportionately even more so in undiagnosed afabs of any gender. who are dropping out of schooling and work and succumbing to severe mental illnesses during what should be the prime of their lives. overall tho birth assignment is not everything this is an issue that disproportionately impacts cis women. trans women. trans men. non-binary people. likely doubling for those that are afab. and then tripling and quadrupling for children who are not white.
bit of an understatement in that last part there. gender likely isn't even the biggest barrier to proper diagnosis and treatment. probably race is even more so. but since gender is such a big disparity in itself across race and one i relate to and can speak on from experience ive focused on it here. a more in-depth look is needed on the neglect of adhd and autistic children of color especially black native and latino kids. but for now do keep in mind the points i'm making increase exponentially for kids who aren't white across all genders including cis boys
#this is dramatic and long but it's a dramatic situation that is completely slept on in the public eye#it's not just about me this is about people who had it so much worse. tho my insider experience obviously brought it to my attention#i'm pretty sure i'm not autistic im adhd but the reality of adhd is a lot more like autism than we are acknowledging#a topic for another day#autism in women#adhd in women#atypical autism#adhd inattentive#undiagnosed autistic#undiagnosed neurodivergent#undiagnosed autism#undiagnosed adhd
39 notes
·
View notes
Text
Things Parents of Children with Autism/ADHD/Developmental Delay/Intellectual Disability/etc. Should Know Before Agreeing to Applied Behavior Analysis Services (This is not a complete list but it has some that I consider most important):
You WILL see online criticism of people who have had bad experiences with ABA. You want a provider that is client-centered and cares about your child's needs and wants and makes sure that the process includes GETTING TO KNOW YOUR CHILD AND YOU and establishing a positive relationship before placing any sort of expectations on the child. People do not want to change their behavior or habits for someone they do not care about. And you want a provider that is trauma-informed and will take ALL PRECAUTIONS against causing trauma, using evidence-based behavior analytical treatments and focusing on reinforcement and letting the child make decisions throughout much of the process, and including you in it too.
It is meant to be an INTENSIVE SERVICE. It is based on the client's needs how many hours services should provide in a clinic or in your home, but this could range to anywhere from 10-20 hours on average. Sometimes more or less. Not being able to arrange those hours can cause more harm than good should your child have many needs or delays.
Daytime hours during the school year get you off the waitlist faster. Evening school hours are always taken first during the academic year. We often struggle finding families willing to take their kids out of school early or take them late. ABA companies should not pressure you on what choice to make, but if you feel your child could benefit or if you are experiencing high-intensity behaviors of concern such as aggression or elopement, it may be able to get you services faster. We are ALWAYS looking for daytime sessions!
Your participation is NECESSARY for success. The child must have interventions that are consistent across places and people. Otherwise, it will most likely be less effective or not effective at all. We want to teach you the strategies we use that show to be successful and work with you and the child! We want to work to the point where the child and the family does not need us anymore! But we cannot do that if you do not learn and accept teaching from us. And often insurances require it and will not pay anymore if the report shows you are not participatong and implementing. We are a service meant to enhance the lives of clients in a way that gives them wider access to things they want and like, build more meaningful relationships, and learn new skills that benefit them. If you do not want to participate, then you are probably thinking of a different service, such as having an attendant.
A good provider who is client-centered is not there to reduce behaviors others find "annoying" or "disruptive", such as stimming. They can be taught skills to help increase attention to tasks and temporarily redirect them, but it is often unethical and harmful to the child to stop them from doing it altogether. The treatment plan may even incorporate time for the child to be able to stim/flap hands/rock their body/etc. on purpose because often, they need it to regulate themselves. It feels good. It's their version of tapping fingers when nervous, playing with a strand of hair, etc. It would be unethical to make a client uncomfortable just because a behavior does not look "normal". If if truly hurts them to do the behavior, such as banging their head against a wall, then it will be addressed for safety concerns.
#applied behavior analysis#ABA#autism awareness#autism#adhd#developmental delay#trauma#intellectual disability#BCBA#board certified behavior analyst
55 notes
·
View notes
Text
So you know about the "WPATH Files", that collection of screenshotted posts taken from the WPATH forum, which supposedly expose how WPATH doctors are evil and out to get your children? You'd be surprised about how the claims anti-trans activists make about those posts are not supported by the posts themselves. Don't believe me? Then let's look at the NY Post article about the document. Specifically, let's look at what the article claims versus the actual reality of what is shown in those posts.
TL;dr:
WPATH doesn't authorize medical transition procedures for immature patient. They actually verify that the patient is mature enough, before allowing the procedure. They also need parental consent.
WPATH doesn't ignore the risks of gender-affirming care. They explain them to both patient and parents, in detail. And if issues do show up, they try to fix them instead of sweeping them under the rug.
WPATH isn't trying to "desex (sterilize) children". That's just the same, old, tired "they're coming for your children!" narrative used against Jewish people, gay people etc etc.
WPATH doesn't disbelieve detransitioners, they support them.
CLAIM: Not surprisingly, age comes up frequently in the WPATH files, from concerns about whether a developmentally delayed 13-year-old can start on puberty blockers to whether the growth of a 10-year-old girl will be stunted by hormones. (The article implies that WPATH doctors are pushing medical procedures on patients who are too young to understand them)
REALITY: The first case (section 21-A "ETHICAL GUIDELINES TO ADOLESCENT CARE - WPATH members discuss the Standards of Care (SOC) ethics for treating adevelopmentally delayed, 13-year-old") is about a 13yo who is already on puberty blockers. Specifically, patients who want hormone therapy need to reach enough emotional/cognitive maturity to provide informed consent to the treatment; but the specific patient in question will reach that maturity either way later than normal, or never at all. The poster asks what to do. Other users suggest a psychiatric evaluation to check whether the patient is capable of consenting or not, weighing the risks of continuing the blockers with the risks of stopping them, etc.
There is no evidence that the doctors gave hormones to that 13yo. Keep in mind that the NYP was complaining about the possibility of that 13yo getting hormones. The NYP had no complaint about the usage of puberty blockers, since the patient was effectively mature enough to get those, and the parents and doctors gave authorization.
Also, one of the posters point out that this kind of discussion also happens with cis (aka non-trans) kids with mental development issues who need access to surgeries. The normal approach is for the doctor, the parents and the patient to discuss together to reach a consensus: in order to approve the medical procedure, the doctor must believe that the procedure will be medically beneficial, the parents must provide full informed consent, and the patient must provide as much consent as possible. There are limit cases where one side can be overridden, like when a patient will never reach a sufficient level of mental maturity, and the doctor and parents are forced to evaluate the risk/benefits of each option. My point is that the NYP has no problems when this approach is applied to cis kids; it complains only when trans kids might get access to medical procedures.
The second case (section 5-A "PUBERTY SUPPRESSION TACTICS - A WPATH member questions the effects of puberty blockers on total height achievement for a 10-year-old patient") is about a patient who asked questions about puberty blockers. The 10yo patient in question was NOT on puberty blockers, nor he was given any - unlike what the NYP tries to imply.
CLAIM: During one conversation, a member asked for advice about a 14-year-old patient, a boy who identified as a girl and had begun transitioning at 4. The child insisted on a vaginoplasty...
REALITY: This is false. The original poster (section 1-A "GENDER AFFIRMING SURGERY FOR MINORS - WPATH members discuss transition surgery for a 14-year-old") only talks about "Gender Affirming Surgery MtF". Christine N. McGinn talks about vaginoplasties she performed on minors, noting that they didn't have any more issues than adult patients: most of them went fantastic, a few of them got issue (mostly because they didn't follow the dilation schedule), and none of them regretted the surgery.
It should also be mentioned that multiple users agreed that 14 was too young. Which shoots a hole in the NYP's "WPATH tried to push vaginoplasty on a 14yo kid" narrative. Whoops.
CLAIM: President Bowers, for instance, said publicly in 2022 that puberty blockers are “completely reversible,” although in the internal forum she conceded it is “in its infancy.”
REALITY: The two quotes don't contradict each other. In the first quote, Bowers claims that blockers AS THEY ARE USED IN GENDER-AFFIRMING CARE (aka for maximum 1 year) are reversible - meaning that if you stop taking them, the effects should reverse themselves. But the second quote (in section 5-B "PUBERTY SUPPRESSION TACTICS - WPATH members discuss how puberty blockers preclude fertility options for trans patients") talks about what happens when puberty is blocked indefinitely. Two very different things.
CLAIM: What about children who are infertile for life since they started hormone blockers before they reached puberty? Bowers told her colleagues the “fertility question has no research.”
REALITY: The Bowers quote doesn't exist in any of the screenshotted posts. The NYP made that up.
CLAIM: At other stages, members talk frankly about the complications for the transition surgery for girls, a phalloplasty in which a nonfunctioning pseudo-penis is fashioned from either forearm or thigh tissue. It requires a full hysterectomy and surgical removal of the vagina. They also discuss other serious consequences, including pelvic inflammatory disease, vaginal atrophy, abnormal pap tests and incontinence.
REALITY: I can't find the screenshotted posts in question. But let's assume for a second that the NYP is telling the truth here; it doesn't actually explain why "WPATH doctors discuss the complications for transition surgery" is bad. As usual, anti-trans activists only focus on the negative effects and risks of any form of medical transition, while completely ignoring any possible positive effect - like, say, alleviating the patient's gender dysphoria.
As far as I can tell, the NYP is trying to imply that these doctors hide these risks from their patients. Which... isn't true. Like, at all. In fact, the fact that they talk about the negative effects so much on a web forum that anyone can access just by paying a fee should clue the reader that these doctors are NOT trying to hide these effects/risks from their patients.
CLAIM: A 16-year-old girl who had been on puberty blockers for several years before she was put on testosterone for a year had developed two liver tumors that an oncologist concluded the hormones had caused.
REALITY: Looking at the posts (section 3-B "SURGICAL OR HEALTHCARE COMPLICATIONS - A WPATH member discusses the development of hepatic adenomas on a client taking testosterone/estrogen"), it turns out that the patient was using both testosterone and oral contraceptives. Hepatic adenomas, also called hepatocellular adenomas, are rare but benign epithelial tumors of the liver frequently associated with oral contraceptive pill use. Meanwhile, there is no evidence that transmasculine people who use hormones are at risk of liver cancer. (Sources: 1, 2.)
CLAIM: Another member described “a young patient on testosterone for 3 years” who had developed “vaginal/pelvic pain/spotting . . . [and] atrophy with the persistent yellow discharge.” Several colleagues described patients with similar conditions, some with debilitating bowel problems or bleeding and excruciating pain during sex (“feeling like broken glass”). Vaginal estrogen creams and moisturizers as well as hyaluronic acid suppositories “can be helpful.” One WPATH member seemed surprised: “The transgender people under my surveillance do not complain about this matter. However, I confess that I have never asked them about it.”
REALITY: This part of the NYP article repeatedly jumps between section 3-C "SURGICAL OR HEALTHCARE COMPLICATIONS - A WPATH member reports their young patient is experiencing vaginal pain on testosterone"; and section 3-D "SURGICAL OR HEALTHCARE COMPLICATIONS - WPATH members discuss erection pain in a patient on estrogen". So there's some confusion here. The general gist of both discussions is: the original poster brings up an issue that their patient has, other users discuss similar cases, provide additional information, and offer possible solutions.
Again: this is a case where a patient got some negative side effects from the treatment, and doctors are trying to solve them. Cases like these happen all the time. There is no evidence that the patient wasn't properly informed before being allowed to get the treatment. The doctors are trying to fix the problem. So what, exactly, is the NYP complaining about? Because if ONE single case of negative effects is enough to condemn a medical treatment, then the NYP should condemn every single medical treatment ever. But no, instead they only focus the blame on treatments that are primarily used by trans people. I wonder why [#sarcasm].
CLAIM: “How do we come up with appropriate standards for non-binary patients?” asked Thomas Satterwhite, a San Francisco-based plastic surgeon who has operated on dozens of patients younger than 18 since 2014. “I’ve found more and more patients recently requesting ‘non-standard’ procedures.” What are nonstandard procedures? They include “non-binary top surgery,” a mastectomy without nipples. There are brutal procedures for girls that eliminate all or part of the vagina and for boys that amputate the penis, scrotum and testicles.
REALITY: Satterwhite did, in fact, ask information about standards for non-binary patients (section 12-A "NON-STANDARD MEDICAL PROCEDURES - WPATH members discuss appropriate standards of care for nonbinary patients, particularly when they request non-standard procedures"). However, you can notice a thing. The NYP made sure to explicitly talk about "de-gendering" surgeries in the most scary and shocking way possible; then they mentioned that Satterwhite operated on dozens of patients younger than 18; then mentioned his quote about non-standard surgeries; and then proceeded to once again describe said surgeries in scary terms, saying that they're performed on "girls" and "boys". So you would think that Satterwhite is performing these horrible surgeries on children, right?
Well, turns out that in the screenshotted posts, Satterwhite made absolutely no mention of underage patients. His question was about non-binary patients in general.
Also, fun fact that the NYP doesn't mention: in trans healthcare, practically all genital surgeries are performed on adult patients. The very few exceptions are performed on 17yo patients, but ONLY in cases where waiting until the patient becomes 18 would make the surgery significantly harder to perform, to the point of having an increased risk of killing the patient. And even then, you need a metric ton of medical requirements.
CLAIM: A particularly intense subject of discussion was whether minors could understand the lifelong consequences of their gender treatments. Minors are presumed by law to be incapable of making an informed decision about having a vasectomy or tubal ligation. Gender surgeries are an exception, however. WPATH’s Standard of Care allows all procedures so long as the minor “demonstrates the emotional and cognitive maturity required to provide informed consent/assent for the treatment.”
REALITY: The NYP is lying. For starters, it forgets to mention that, in various states, minors CAN get certain surgical procedures as long as they pass certain prerequisites, such as a minimum age (like 16). Why? Because it's acknowledged that children mature over time, and become more and more capable of understanding - and by extension consenting to - more complex things, like surgeries.
Another thing that the NYP omits is that minors can get invasive medical treatments even if they don't reach the minimum consent age, as long as the doctor can provide reasonable medical reason to do so; the parents provide fully informed consent to the procedure; and the underage patient provides a sufficient amount of consent, which varies depending on the procedure requested. The latter is what “demonstrates the emotional and cognitive maturity required to provide informed consent/assent for the treatment” refers to.
The main difference is that WPATH doesn't decide that patients above a certain age are automatically mature enough to consent to a specific procedure; instead, WPATH doctors actually verify whether or not the patient is mature enough to consent to that specific procedure.
CLAIM: In a May 2022 internal workshop, “Identity Evolution,” WPATH members conceded that was all but impossible. Daniel Metzger, the British Columbia endocrinologist who cowrote the Canadian Pediatric Society’s position paper on health care for trans minors, said, “I think the thing you have to remember about kids is that we’re often explaining these sorts of things to people who haven’t even had biology in high school yet.”
The quote is from the transcript of the "Identity Evolution Workshop", Clip 1. It also completely fails to prove the NYP's point. Remember: the NYP is trying to claim that children cannot, under any circumstance, consent to surgeries - implying that this means that they shouldn't have access to surgeries. This is false.
Also, the transcript shows Metzger saying that they should improve the way doctors explain medical procedures to patients and parents, because if they don't understand these procedures, they can't provide informed consent, and therefore they can't have access to said procedures. Metzger is NOT proposing to provide medical procedures to people who don't provide informed consent.
CLAIM: Although many WPATH members privately doubt that adolescents can give truly informed consent to life-altering procedures, they must affirm whatever children say about their gender.Unless, the WPATH files disclose, the patient wants to reverse course and become a so-called detransitioner.WPATH members mostly dismiss those cases as insignificant or overblown by the media and question whether minors who want to revert to their birth sex really understand what they are doing.It’s a question that would never be asked for minors who declared themselves to be gender dysphoric. One case involved a 17-year-old boy, just graduated from high school, who had been on testosterone for two years. He was reported to be “very distraught and angry. He reports he feels he was brainwashed and is upset by the permanent changes to his body.”A self-described “queer therapist” did not believe any young person could be brainwashed. “In my experience, those stories come from people who have an active agenda against the rights of trans people.”
REALITY: The NYP is dishonestly mixing together multiple different contexts.
When a patient goes to a WPATH doctor and claims to be trans, the doctor accepts it. When a patient claims to not be trans anymore, the doctor still accepts it.
When a patient declares themselves to be gender dysphoric, the doctor DOES, in fact, verify whether the assertion is true, through psychological examination, exploring whether the dysphoria is innate or caused by issues like mistakenly believing that being feminine means that you must be a girl and therefore have "female" biology and so on. After that is verified, however, the doctor accepts that the patient is right.
When discussing how the media and public claim that there is an epidemic of detransitioners, THAT is when WPATH doctors will say that the issue is overblown. Because the reality is that the amount of detransitioners - and specifically people who got through medical transition and then detransitioned afterwards - is incredibly small, unlike what anti-trans activists would make you believe.
All of that can be clearly seen in the discussion in section 4-A "DETRANSITION CONCERNS - A WPATH member reports a patient who reports feeling “brainwashed” into transition".
SO, TO RECAP:
The NYP complains that the WPATH uses ‘arbitrary’ age limits, implying imply that WPATH is trying to pressure forcibly trans young kids before they were ready. The reality, however, is that WPATH is doing what every other medical field does when a patient is a minor: they approve the treatment only if the doctor reasonably believes that it will be overall beneficial, the parents give informed consent, and the patient itself gives consent as much as possible. Checking whether or not a kid is mentally mature enough to at least understand somewhat the procedure falls under the third point; checking the kid's physical maturity falls under the first point, because it impacts whether or not the therapy will be overall beneficial.
(BTW, the NYP says that, when making the new Standards of Care, WPATH "scrapped a draft chapter about ethics and removed minimum-age requirements for children starting puberty blockers or undergoing sexual-modification surgeries." What the NYP doesn't say is that the guidelines ARE the ethics of the practice; and that WPATH replaced minimum-age requirements with evidence-based requirements. For example: instead of assuming that all 16yo patients are automatically mature enough to get hormones, the new guidelines require doctors to actually verify whether the patient is mature enough (both physically and mentally) or not. Why this change? Because there were several cases where 16yo-or-older patients were allowed to get hormones when they weren't ready.)
The NYP claims that WPATH doctors downplayed the dangers of gender-affirming care. They did not. The post themselves demonstrate that they amply and truthfully discuss these dangers - and inform their patients about them. And when negative issues do show up, WPATH doctors try to fix them.
The NYP implies that WPATH doctors are trying to de-sex children. They did not. The posts only talk about performing non-standard procedures on non-binary patients - but they make absolutely no mention of minors.
The NYP claims that WPATH doctors are dismissing and disbelieving detransitioners. They did not. WPATH doctors support detransitioning patients, direct them towards support groups, research solutions for the physical issues caused by the regretted procedures, and so on and so forth. WPATH doctors also denounce the whole "there's an epidemic of people who go through medical transition and then later detransition and regret it, because it's way too easy for children to get brainwashed into being trans and to get medical transition" narrative as false because it IS false.
9 notes
·
View notes
Text
I normally post about how surrogacy exploits women but this is an example of how the business part of ivf exploits women. They took that couples money after promising careful screening of the soerm donors. Instead the mother was infected with an STI that would impact any future pregnancies, they lost one baby and the other will need life long care.
The state Supreme Court confronted philosophical questions about “wrongful birth” and the value of life Wednesday when the state asked the justices to reverse a $37 million verdict awarded to a family whose lives were upended by a tragically flawed artificial insemination procedure at UConn Health.
Jean-Marie Monroe-Lynch, her husband Aaron Lynch and their surviving son Joshua sued for malpractice after fertility specialists affiliated with the University of Connecticut’s medical center inseminated her with sperm from an anonymous donor infected with cytomegalovirus, or CMV, a common, sexually transmitted virus that has catastrophic effects on fetal development.
The procedure, a therapeutic donor insemination, succeeded in that the mother became pregnant with twins, a boy and girl. But she and the children were infected with CMV. One of the twins died and the other was born in January 2015 with a long list of devastating disabilities that will put him in need of constant, life-long care. The surviving twin, Joshua, cannot communicate or care for himself, has global developmental delays; suffers from cognitive, hearing and movement deficits; suffers from autism and seizures, and spends hours each day having nutrition pumped into his body through a tube.
In its appeal, the state is arguing, among other things, that the family’s suit was not based in the usual definition of malpractice but is rather what has become known as a wrongful life suit, a relatively new and controversial action against medical practitioners for failing to properly prevent the birth of children, such as Joshua, shown through prenatal examinations to have tragically debilitating conditions.
See rest of article
#usa#connecticut#Ivf#Wrongful birth#UConn Health#cytomegalovirus or CMV#Wrongful life suit#The fertility industry is just like another big business
9 notes
·
View notes
Text
Speech and Language Therapy can help them recognize words and associate sounds with objects and behaviors to increase social acceptance.
#developmental delay treatment#occupational therapy for autism#screen for autism org#neuro developmental therapy#sensory integration therapy#down syndrome therapy#aba therapy near me#speech pathologist near me
0 notes
Text

Adultification happens when young children are expected to act like adults. For example, an 8-year-old who is being adultified may be expected to fully care for their younger siblings by cooking for them, making sure they attend school, doing their laundry, or bathing them daily. But that same 8-year-old isn’t as capable as an adult in many ways. They can’t always navigate social situations well, can’t reason with nearly as much efficiency as an adult, and are only starting to develop critical thinking skills.
Black children, especially, can be turned into mini-adults, which can hinder healthy developmental growth. And since development research has shown that there are important benefits of being a child, like developing social skills through play, creating memories through exploration, and learning about oneself through experimentation, if these opportunities are lost or delayed due to adultification, then consequences will occur.
Black children are often viewed as older than they actually are by their teachers, peers, police officers, and even society at large. Children who receive less help from parents—which is also common in lower-income households—may be less equipped to deal with difficulties later on in life than kids whose parents stepped in earlier. Their less advantageous upbringing may make them more likely to struggle academically or act out. They may also be more susceptible to entering a cycle of poverty, or involvement with the criminal justice system, that they'll have difficulty escaping.
As if on cue, around age 10, Black students begin getting into trouble at school. In one study, researchers found that Black students were 21 times more likely to be suspended than white students. While many factors contribute to higher rates of suspension among Black students, adultification plays a part, too. Because Black children are perceived as older, they are likely to receive harsher punishment than their white peers for breaking rules.
Dr. El Brown, Ph.D., a family engagement strategist, and an early childhood education professor at American University says, “Working with children requires empathy and compassion. When someone sees a Black child as an adult, they don’t empathize with them as a child. Therefore, the compassionate nature that is inherently there as adults toward children is missing in that interchange.”
But sometimes the adults who are adultifying children don’t realize they are doing it. To them, Dr. Brown suggests recognizing their own deeply-ingrained beliefs. “I don’t think that someone who adultifies a child is someone who is always doing so intentionally,” says Dr. Brown. “It’s the adults' implicit biases that make it difficult for them to view that child the same way another individual with lived experience interacting with Black children may view the child, thus leading to harsher treatment, and beyond.”
The good news is that there are ways to help prevent adultification from happening in your home and community.
Don't Expect Too Much From Kids
It's common for parents to expect too much from their young children, particularly when dealing with achievement. For example, parents might expect children to perform at school in ways that are above their grade level. When this happens, kids aren't given adequate time to explore themselves before expectations supersede their stage of development.
"As an educator, our time with a child expires. However, parents and families are forever teachers. My responsibility as an early childhood educator is to help parents understand developmental milestones. I am empowering families to advocate for their children in instances when children are expected to act or perform above their age level," says Dr. Brown.
An educator spends about six months with a child each school year. Therefore, engagement and continuous communication between the educator, educational systems, and the parent is vital for a student's success.
"Adultificaltion is a complex issue that requires an in-depth understanding of the systems in place that have permitted this behavior in the first place," says Dr. Brown. Some of the public systems that have led to the adultification of Black youth are America's educational system and juvenile justice system.
If you want your child to enjoy life more fully, remember not only what they are capable of but also what makes sense at each stage of development.
Help Children Make Sense of the World
One way to help prevent adultification is to take part in helping young children make sense of what's happening to them. For instance, if a 3-year-old doesn't understand why their parent is going away to work while they are at daycare, talk about it together. Whenever possible, try explaining situations with empathy and age-appropriate understanding. In that situation, it would mean avoiding saying things like, "I'm going to work now," or "I have to go." Instead, say something like "I'll see you later," or "I'll be back soon."
Similarly, telling your child about grown-up topics like finances or relationships is obliging them to try to fix what they cannot control, which leads to undue stress.
Lastly, minimizing your child's reaction to a problem by saying things like, "It's not that big of a deal," implies that what they are feeling is unnecessary and that there are more pressing issues. Validating their emotions can help kids remain kids. With support from caring adults, kids can learn how to cope with challenges and separation. In turn, they will grow up to be healthy adults who are flexible and understanding.
Avoid Labeling Kids Based on Age
While it's natural to think about kids according to their age, it's important to keep in mind that there is more to each child than simply being labeled in comparison to their age group. Every child deserves to be seen and appreciated for who they are and how they behave, regardless of their age. Each person is unique, but all children deserve an opportunity to develop self-confidence, maturity, and a healthy sense of self-worth.
To avoid labeling kids based on age, avoid using words such as "little" or "big" unless talking about actual size. Instead, use descriptive terms that refer to physical characteristics instead of abstract terms that label a child according to their age. For example, instead of calling a toddler a "big boy" or a "little girl," try describing their behavior or character instead.
Consequently, actions must be taken to counter these growing trends in order to prevent unintended consequences. Parents should keep tabs on how their kids are being treated, or labeled, by teachers or peers by monitoring teacher feedback forms or speaking directly with other parents about how their children are doing at school. If your child is being labeled, take action to ensure they feel included and respected. While putting an adult label on a child is nothing new, adultifying Black children comes with adverse effects that differ from those of white children. Allowing it to happen can lead to serious emotional issues down the road.
"There should be diversity, equity, and inclusion training for all educational service providers, which will help them to be aware of their potential implicit biases so they cannot manifest in the treatment of children within their learning environment," says Dr. Brown.
#Adultification Disproportionately Hurts Black Children—but Parents Can Help#adultification#Black Children#end adultification of Black Children
18 notes
·
View notes
Text
having empathy is seen as a bad thing that makes you an abuse apologist unless your have narcissism or psychopathy then not having empathy is a bad thing that makes you a demon
Having empathy for abusers does not make you a bad person or confused or stupid. Your not stupid for being a pacifist or believing in restorative justice or empathizing with bad people or understanding people with severe mental illnesses who have done bad things
Not having empathy at all is fine and you can still be a good person, narcissistic abuse doesn't exist and psychopaths can be good people too
People with PTSD, mood disorders and autism struggle with not only cognitive empathy but also effective empathy so when you attack people with narcissism you attack them as well
People are found not guilty by reason of insanity are not evil people who got away with their crimes Scott free
Y'all talk about pacifists and optimists seeing the world in black and white and how they cant recognize evil while talking all kinds of shit about your ability to recognize evil vs mentally ill
Dude you freak out and accuse autistic men who look a little gross of being perverts on drugs when in reality they have flat effect and strange body language so you assume there actually a huge threat and are gonna rape you cause you think being an incel or socially awkward in a creepy makes you automatically evil, (I've hung out with those guys a lot of them where my classmates- they were good people) and you freak out when you perceive a big black man get angry or having a mental health crisis. Im not gonna hold it against ya if you have moments when your afraid of mentally ill people we can be dangerous we can be big and do bad things, but don't think for a second your good at detecting that shit
Y'all scream ACAB but still believe in unlawful searches and violations of privacy, and again are afraid of visibly mentally ill/developmentally delayed people, you are okay with prisons using slave labor and cruel inhumane punishments, you only care about drug abusers being criminalized when it's pot or over the counter medicine. You only care about police brutality when it comes to race. You hate the death penalty yet praise revenge and vigilantism. You'll report only crimes that support your politics. You hate trump so all his supporters must suffer. You hate trump supporters so much but you cant be normal about it. All his supporters have to be bigoted uneducated redneck hicks. You are classist toward the poor and you hate small businesses for being bourgeois but you support massive megacorps
You talk all this shit about psychopaths being unable to feel empathy and how that makes them evil but look whose talking! You hate people who actually are empathetic and you need to come up with a thousand different reasons to be a dick to them for what crime? Having empathy for another human?
Not having empathy doesn't make anyone evil- again lots of people have low or no empathy and they are still good people and don't deserve the shit treatment they get. It's always decriminalize mental illness until the guy with bipolar says something inappropriate or the autistic dude comes off as creepy or until it turns out the person living in the apartment next to yours is schizophrenic or has a personality disorder. My sister has low empathy and she is genuinely the best person in my life- she certainly understands more than the counselors and therapists I saw back in grade school who despite preaching empathy where assholes. She has good morals and she is awesome.
Having empathy for bad people does not make someone bad. They are still good people and having that level of empathy is actually a good thing. We need more people like that.
"having empathy is actually bad unless your mental illness is the reason your lacking empathy then your just evil" is a mentality that needs to fucking die. Also you don't have to emphasize or like severely impaired people inorder to not be a dick.
Being anti revenge doesn't mean you expect victims of rape or child abuse to be 'perfect victims' being anti revenge doesn't mean being an abuse apologist, believing in the power of restorative justice doesn't mean your pushover. Y'all really learnt the term 'perfect victim' and fucked it up- I expect victims to be angry and have all kinds of issues and no matter what the victim did I don't think anyone deserves to be raped or abused, I don't get angry at them for fighting back or not fighting back. But being a victim does not make you morally superior or prevent you from inflicting the damage done to you unto someone else. It doesn't mean your perspective is flawless or perfect. I want rapists and child abusers to suffer but I also want human rights to be respected and for victims to be given the help they need- these feelings aren't antithetical or dangerous. I have no empathy for those kinds of people but I also know innocent's suffer because of the system. There is no easy way for us to separate good from evil to differentiate them so Id rather bad people have human rights than for good people to lose theirs
I'm not super political, I'm invested in only a few issues because I burn out so easily and even then it's miniscule but can you blame me? The sheer amount of horseshit people say, the antisemitism, the classism, the ableism- it's tiring. You aren't allowed to have nuance anymore, your automatically labeled an evil evangelical conservative or sjw blue haired bitch. And I keep hearing people talk about taking away basic human rights and when I argue how doing that is bad and has horrible consequences, I get labeled an enabler or apologist. Newsflash- taking away human rights from any group of people including absolute scum bags fucks us all over- just label everyone you don't like as a criminal and bad bing bada boom we're taking the government's dick up the ass.
People get angry when people like me take breaks or moments to chill and talk about how 'x group of people don't get to take a break from the cruelty!' but I'm part of x. I'm autistic I'm Latina I'm gay! Im also tired and because I have a life outside of social media I can chill for a bit and because I am easily burnt out. I take more breaks because I need them- i need more breaks because my disability burns me out and focusing on politics all the time makes it worse. I'm not a traitor your just ableist (usually toward people who are off-putting and have low empathy) and I'm not an apologist I just don't want people to get happy over innocent people dying because said innocent people are part of group they hate. I just like respecting human rights and if that makes me an enabler of bad people? If letting bad people have nice things means protecting innocent people then I'm fine with it
#restorative justice#ableism#racism#Autism#Bipolar#schizophrenia#narcissism positivity#sociopath#ptsd#Empathy#abuse apologism#drug abuse#developmental delay
6 notes
·
View notes
Text
Consequences of Untreated Postpartum Depression (PPD)
10 - 20% of new moms face PPD, a condition that goes beyond typical baby blues. Unlike its milder counterpart, PPD doesn't resolve on its own; it needs proper treatment. Addressing postpartum depression is crucial not only for challenging the myth of the 'perfect' mother but also for recognizing and nurturing the sufferer’s inbuilt strength and adaptability.

Untreated PPD can have these serious ripple effects:
For Moms:
Ongoing depression
Relationship strain
Work difficulties
Bonding challenges with baby
Health problems
Anxiety
Suicidal thoughts
For Babies:
Potential developmental delays
Cognitive impacts
Emotional health
Attachment difficulties
Social skills
Stress response
For Families:
Marital strife or divorce
Sibling impact
Financial stress
Generational risks
In severe cases, PPD can even lead to self-harm. That's why getting help is crucial.
The good news? Effective treatments exist! Therapy and medication can help moms reclaim their mental health and embrace motherhood more fully. By seeking treatment for PPD, we can create a supportive community that embraces both the joys and the challenges of parenthood.
Are you or someone you know struggling? Don't wait - reach out for support. Early intervention can make a world of difference for both mom and baby. Learn more about PPD treatment options at https://gabapsychiatrist.com/category/postpartum-depression/.
Need professional help? Consider connecting with board-certified online psychiatrists for accessible PPD support. +1(833) 312-4222 or visit our website: https://gabapsychiatrist.com/
Remember: You're not alone in this journey. Help is available, and recovery is possible.
2 notes
·
View notes
Text
ok take this entire post with a grain of salt because i'm really hyperfixated right now and just writing whatever but,, something i think about A LOT is mamoru's behavior (particularly anime mamoru (which i think may have something to do with ikuhara being really critical of japan's treatment of vulnerable children)) can be explained as results of neglect and developmental delays.
he was raised in an institution from the age of five, and probably primarily raised himself. he had to become self-sufficient at a very young age because he knew there was no one who would support him besides himself.
having more-or-less been an adult his whole life, he seems very mature. he's very successful in school, has worked multiple jobs, and owns an apartment. he's very well-mannered and polite, and never childish or poorly behaved. he has many accomplishments/skills for his age and is worldly. but if you pay close attention to him, there are aspects of his personality that are very childlike still or couldn't grow much. particularly emotional and social ones
here's a list of his signs of trauma/neglect/developmental delay (because i'm not sure how to make these into a paragraph):
-He's very naïve in general. Despite the cynical façade he put on early in the series, he doesn't understand many everyday social concepts and has a tendency to take things at face value.
-For example, he doesn't seem to have a firm grasp on gender. He's had very few close relationships in life, and only seems to have a very sketchy idea of what boys and girls are. Since the sailor guardians are pretty much the only girls he's been close to, he assumes their characteristics are indicative of all girls, instead of being idiosyncrasies of theirs.
There's a scene where Sailor Moon and Sailor Mars start randomly bickering over something innocuous and get pretty vicious and *very* loud. Tuxedo Mask slips away and remarks "It's scary when girls fight."
It's not a jab, it's more like an observation. He sees an element of Usagi and Rei's very unique dynamic and assumes it applies to *all* girls. He doesn't have much info to draw from and is currently constructing his idea about how girls function based of off the sailor senshi. It also shows how he takes things at face value, because he instantly accepts his first interpretation of the situation and doesn't think much further into it.
-Another example is when Zoisite managed to trick him by pretending to surrender, and Mamoru just trusted him!😭
-Even though he's a teenager, he doesn't understand dating at all, and doesn't know what the appeal of it is. When dating Usagi he tries to be romantic by emulating things he saw on TV and acts very odd. Because of all of his responsibilities, he probably never had many opportunities to bond with his peers. Dude has no clue what partners do together, what he's supposed to be feeling, or much of anything really! he also gets confused by girls liking him and doesn't catch on to their advances most of the time..
-His expressions are very subtle or could even be described as blank. Difficulty with facial expressions are a common characteristic of neglect. (Lots of fans think he's cold because of this.😢 he's not!! he just has a rough time okay??😢😢)
-He has a hard time asking for help. It doesn't even usually occur to him as an option. He's so used to solving everything himself, asking somebody else seems unthinkable
-When he's walking down the street with a shoulder wound, and Usagi shows concern about it, it doesn't even register! He gets annoyed by her following him and asks her why. She answers that she was worried. "About me?" he asks, despite there being no one else in the alleyway. He's completely baffled. It's never occurred to him that someone may care about his well being.
-He's very shy and usually plays social interactions safe by not talking much. Sometimes this actually has the effect of making the conversation awkward. (That time in SuperS where he has guests over and just sits there while usagi and chibiusa argue over who his real girlfriend is. he doesn't intervene even when it makes the guests uncomfortable)
-HE'S SUCH A PEOPLE PLEASER. i don't think i have to explain this one, but he dated rei for a while despite really disliking it because he didn't want to hurt her feelings!! and that time he apologized to usagi for not knowing her birthday and scrambled to get her a gift even after she hit him and embarrassed him in public. he wasn't mad for a second. he thought he must be in the wrong!! (he doesn't value himself as much as he should😢)
-he struggles to be vulnerable, even in small, mundane ways.
-when pressed, he has a tendency to shut down, using submissive body language and avoiding eye contact. (like when mercury cornered him and tried to force him to be direct with her. (he ended up running away))
-he is VERY selfless. in Transylvania no mori, he's stabbed and is dying. he focuses all his remaining energy on comforting Usagi and making sure she knows it's not her fault, when he should probably be focusing on survival. he clearly wants to take care of others, which is good, but he has too little concern for himself!! he wasn't taught he had value
-he can act prickly (probably out of fear/defense mechanism)
-he doesn't set boundaries!!! the closest he usually comes is ignoring the person causing him problems😭😭😭😭
i don't know where i'm going with this but developmental psychology is one of my special interests,, also i think usagi is so good for him because she unconditionally loves him and accepts him where he's at instead of expecting him to be more mature or something!! and you help people with delays grow by meeting them where they're at and nurturing whatever needs they have instead of questioning or criticizing them!! she teaches mamoru to value himself and can teach him the things he didn't learn!! she had a really safe and loving family and a stable childhood and she can use the benefits her secure life gave her to help him!!!!!! :,,,,DDDDDD
(people always think usagi is the fragile one, and mamoru ought to protect her better, but she's really the strong one of the two!! she had the safe childhood. mamoru is a bit (emotionally) frail from his hard life :,,>)
mamoru is so grateful to her for loving him, he gives her his 100000000% and takes care of her with everything in him!!!
#unhinged rambling#mamoru chiba#usamamo#tuxedo mask#angst#im love him tho#i love characters with developmental problems#cw mental health#i guess..#im being unhinged but i think im also right
70 notes
·
View notes
Note
Hello, again, Summer! I had a question, but feel free to answer whenever you are at your best so you're not stressed. <3
I was wondering if neurodivergent people---especially those with autism and ADHD---experience GAD (generalized anxiety disorder) or other anxiety disorders differently than most.
I'm curious because my personal struggles with GAD have been really bad as of late, but all of my friends with it or other anxiety disorders can't relate to my struggles and I wonder if it has to do with the fact that I have AuDHD and they don't.
Hope you have a great rest of your week!
Hi there,
I found some information about this on ADDitude and according to one article:
Anxiety is the brain’s essential internal alarm system that activates our fight, flight, or freeze response. This reaction occurs when we feel vulnerable, in danger of being embarrassed, or are in trouble. Most children with ADHD and ASD experience anxiety this way a rise in feelings of fear or panic when faced with an uncomfortable situation; others have generalized anxiety disorder, which leads to chronic worrying.
The link to this will be below:
I also found some more information that states:
Autism & Anxiety
Up to 42% of children on the autism spectrum may also have significant anxiety.
Children with ASD are more likely to have a phobia than the general population.
Sometimes children with autism can be bossy or controlling.
Often children with ASD are anxious because they struggle in social situations and do best when things are predictable.
Many girls on the Spectrum are diagnosed with anxiety first.
Autism can be harder to spot in girls because some symptoms like restricted interests may be harder to notice in girls.
Due to how we raise girls in our culture, they then to have better nonverbal communication skills and coping skills
I found this interesting. I’ll also leave it below so you can read it if you want.
Apparently there was a study on this. It states the following:
Children who have both autism and attention-deficit/hyperactivity disorder (ADHD) are also more likely to experience anxiety, depression, developmental delays, learning disabilities and other mental health conditions than are children with only autism or ADHD, according to a new population-based study.
The results draw on data from more than 6 million children aged 3 to 17, collected from 2016 to 2018 by the U.S. National Survey of Children’s Health, an annual questionnaire that asks parents about their children’s medical diagnoses and treatments. Among those children, 949,367 have autism, 4,570,320 have ADHD, and 740,816 have both conditions.
Children in the last category are four times as likely to have anxiety and three times as likely to have depression as autistic children without ADHD. They are also four times as likely to have a learning disability and seven times as likely to have developmental delay compared with children who have only ADHD, the researchers found.
I’ll leave this study below so you can read through it if you’d like.
I hope these sources help you.
Thank you for the inbox. I hope you have a wonderful day/night. ❤️
18 notes
·
View notes
Last Seen Blogs

congnghieptot
Công Nghiệp Tốt

hana2029
Untitled

moikav
Без названия


radiominasfmbh-blog
RÁDIO MINAS FM BH