#proposed diagnostic criteria
Text
Proposed Diagnostic Criteria for Daydreaming Disorder (Maladaptive Daydreaming)

A. Persistent and recurrent fantasy activity that is vivid and fanciful, as indicated by the individual exhibiting two (or more) of the following in a 6-month period; at least one of these should be Criterion 1:
While daydreaming, experiences an intense sense of absorption/immersion that includes visual, auditory, or affective properties
Daydreaming is triggered, maintained, or enhanced with exposure to music
Daydreaming is triggered, maintained, or enhanced with exposure to stereotypical movement (e.g., pacing, rocking, hand movements)
Often daydreams when feels distressed or bored
Daydreaming length or intensity intensifies in the absence of others (e.g., daydreams more when alone)
Is annoyed when unable to daydream or when daydreaming is interrupted or curbed
Would rather daydream than engage in daily chores, social, academic, or professional activities
Has made repeated unsuccessful efforts to control, cut back, or stop daydreaming
B. The disturbance causes clinically significant distress or impairment in social, occupational, or other important areas of functioning.
C. The disturbance is not due to the direct physiological effects of a substance (e.g., a drug of abuse, a medication) or a general medical condition (e.g., dementia) and is not better explained by autism spectrum disorders, attention-deficit/hyperactivity disorder, schizophrenia spectrum disorders, bipolar I disorder, obsessive–compulsive and related disorders, dissociative identity disorder, substance-related and addictive disorders, an organic disorder, or a medical condition.
Note. Current severity defined as follows: Mild - experiences mainly distress, no obvious functional impairment; moderate - one area of functioning is affected (e.g., work); severe - more than area of functioning is affected (e.g., work, school or social life) (p. 180).
-
MD is associated with social anxiety and addiction (particularly internet addiction) (p. 177), as well as dissociation, obsessive-compulsive behaviour, and inattention / attention deficit (p. 181).
People who seek treatment for MD are misdiagnosed with a variety of conditions; "...professionals were unfamiliar with their problem and provided various diagnoses, including depressive disorder, anxiety disorder, obsessive-compulsive disorder, posttraumatic stress disorder, borderline personality disorder, and dissociative disorder" (p. 178).
"MD is uniquely characterized by a kinesthetic component, a need for evocative music, and an addictive yearning to compulsively engage in this mental behavior" (p. 184).
-
From Somer et al., 'Maladaptive Daydreaming: Proposed Diagnostic Criteria and Their Assessment With a Structured Clinical Interview', Psychology of Consciousness: Theory, Research, and Practice (2017), Vol. 4, No. 2, pp. 176-189. DOI: 10.1037/cns0000.
Another interesting & related article is Somer et al., 'Representations of Maladaptive Daydreaming and the Self: A Qualitative Analysis of Drawings', The Arts in Psychotherapy (2019), Vol. 63, pp. 102-110. DOI: 10.1016/j.aip.2018.12.004.
#my emphasis in bold#described#described in post#described in alt text#maladaptive daydreaming#maladaptive daydreaming disorder#daydreaming disorder#proposed disorder#proposed diagnosis#proposed diagnostic criteria#dogpost
14 notes
·
View notes
Note
what are your thoughts on ocpd? i generally think these behaviors are harmless or at least not distressing and wouldn't benefit people much to have classified as a personality disorder.
hmmm i could post more nuance abt this at a later time so giving this response might be kicking a hornet's nest + leaving- please please please keep in mind that i believe all ppl's suffering is valid + in need of healing + i am questioning the history, purpose + impact of personality disorder dx, NOT the lived experiences of ppl diagnosed with them
while i think all psychiatric diagnosis is suspect, i find personality disorders in particular to be laughable, even by dsm standards. they are a hodgepodge of "types of ppl we think are bad". the words "unusual" + "dramatic" are used to describe supposedly objective pathologies. if anything, these disorders serve as a massive red flag that psychiatry is far less wedded to science than its proponents want to believe it is. i think our attempts to 'destigmatize' this absolutely dogshit collection of disorders instead of questioning their use or existence has been a horrible error within the mad community.
many of the criteria are absolutely seeping with moral judgements + christian ideology. several are blatant repurposings of hysteria. they are frequently diagnosed in ppl who have no desire to 'heal' from them (not viewing the behaviors as a problem is often part of the dx). things like disregarding the rights of others or exploiting others for your own gain are side by side with things like the desire to not be around ppl or intensely believing in aliens. most of them can be directly linked to traumatic experiences in childhood + yet they persist in portraying them as disorders of individual, unchangeable pathology. if ppl expanded their view of trauma, i'm willing to bet that basically all cluster b + c + a decent chunk of cluster a ppl would qualify as having experienced significant trauma.
fwiw, i definitely meet the ocpd criteria but i find the word ocd to be a more useful tool for me. my father also meets this criteria + i would say it has been a deeply destructive pattern of behavior in his life for himself + his loved ones. i can't say this is the case for everyone meeting this criteria, tho.
i just don't think the concept of diagnosing anyone with having a "disordered personality" is healing. some things classified as pds are extremely distressing experiences which ppl deserve support for, but i would like to see those placed in conversation with trauma, politics, + community. classifying intense trauma responses as permanent disorders of the self leaves a horrible taste of blood in my mouth. how many of us already believe that we are inherently broken because of what happened to us?
like u said, other things classified as pd diagnoses can be pretty harmless differences. i often see ppl in my communities responding to the widespread belief that ppl diagnosed with pds are immoral or evil (which is shitty!) by trying to 'destigmatize' them, but i propose, after a careful evaluation of the history + current usage of the diagnosis, that the concept of personality disorders was + is intended to classify ppl who are seen as morally corrupt or 'unusual' as being diseased. the original purpose of this diagnostic category was to stigmatize people. is this really the concept we want to seek liberation through, or can we find new ways of understanding any suffering that may come from the experiences currently labeled as personality disorders?
211 notes
·
View notes
Text
What is Idiopathic Mast Cell Activation Syndrome?
Idiopathic Mast cell activation syndrome (MCAS) is one of several mast cell disorders. MCAS occurs when there are a normal number of mast cells in a person's body but they over-release mast cell mediators causing random allergic reactions in multiple systems of the body. MCAS is incredibly common being present in an estimated 17% of the population.
Symptoms
MCAS symptoms are incredibly varied and always occur in multiple systems of the body. Anaphylaxis is common.
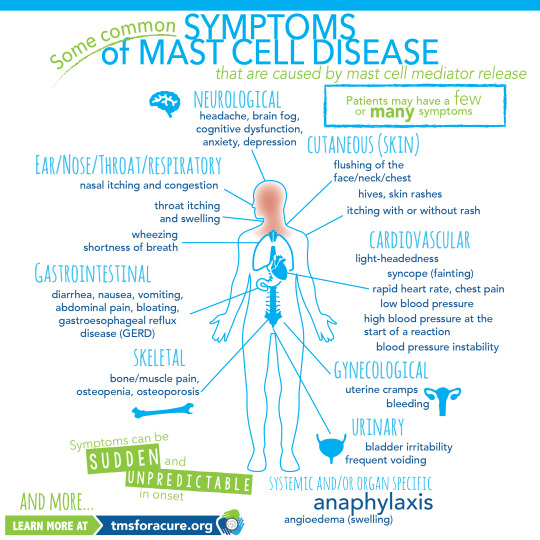
[ID: A graphic labeled "Some common symptoms of Mast Cell Disease" A graphic of a person standing in the center with multiple organs visible is shown. Around the person are lines pointing to specific areas of the body labeled with the body system and symptoms. Clockwise these read "Neurological headache, brain fog, cognitive dysfunction, anxiety, depression Cutaneous (Skin) flushing of the face/neck/chest, hives, skin rashes, itching with or without rash Cardiovascular light-heartedness, syncope (fainting), rapid heart rate, chest pain, low blood pressure, high blood pressure at the start of a reaction, blood pressure instability Gynecological uterine cramps, bleeding Urinary bladder irritability, frequent voiding Systemic and/or organ specific Anaphylaxis angioedema (swelling) Skeletal bone/muscle pain, osteopenia, osteoporosis Gastrointestinal diarrhea, nausea, vomiting, abdominal pain, bloating, gastroesophageal reflux disease (GERD) Ear/Nose/Throat/Respiratory nasal itching and congestion, throat itching and swelling, wheezing, shortness of breath and more" In the bottom left corner "Symptoms can be sudden and unpredictable in onset learn more at tmsforacure.org"]
MCAS symptoms are specifically not allergies. the reactions may look like allergies but the two are not the same and MCAS is not a condition meaning "many allergies" While MCAS can have some consistent triggers one of the defining features of the disease is that reactions are random and happen unpredictably.
Anaphylactic shock is not a requirement for diagnosis.
Diagnosis
MCAS is diagnosed by an immunologist. It is in part a diagnosis of exclusion and requires ruling out both allergies and systemic mastocytosis as well as other conditions such as certain types of tumors.
Diagnostic criteria for MCAS is debated. Some immunologists follow the symptom-based diagnosis approach in which case the diagnostic criteria are:
Recurring and severe anaphylactic-like episodes that involve more than one organ system
and
Positive response to mast cell stabilizing or mediator medications anaphylaxis-type symptoms
Others follow diagnostic criteria based on laboratory findings. In this case the diagnostic criteria are:
Episodic symptoms consistent with mast cell mediator release affecting two or more organ systems evidenced as follows:
Skin: urticaria, angioedema, flushing
Gastrointestinal: nausea, vomiting, diarrhea, abdominal cramping
Cardiovascular: hypotensive syncope or near syncope, tachycardia
Respiratory: wheezing
Naso-ocular: conjunctival injection, pruritus, nasal stuffiness
and
A decrease in the frequency or severity; or resolution of symptoms with anti-mediator therapy: H1 and H2 histamine receptor antagonists, anti-leukotriene medications (cysLT receptor blockers or 5-LO inhibitor), or mast cell stabilizers (cromolyn sodium)
and
Evidence of an elevation in a validated urinary or serum marker of mast cell activation: Documentation of elevation of the marker above the patient’s baseline during a symptomatic period on at least two occasions; or if baseline tryptase levels are persistently >15ng, documentation of elevation of the tryptase above baseline on one occasion. Total serum tryptase is recommended as the markers of choice; less specific (also from basophils) 24 hour urine histamine metabolites, or 11-beta-prostaglandin F2.
and
Primary (clonal) and secondary disorders of mast cell activation ruled out.
These are not all proposed diagnostic criteria as the subject is heavily debated. Generally, a laboratory-confirmed MCAS diagnosis is considered more legitimate.
Treatment
MCAS is a very treatable condition. Generally treatment follows a path from antihistamines -> mast cell mediators -> biologics.
Epipens are given to MCAS patients with a history of anaphylaxis.
Antihistamines are divided into 2 categories: H1 antagonists and H2 antagonists. These categories are determined based on the histamine receptor each one targets.
H1 antagonists mostly deal with systemic and cutaneous symptoms. H1 antagonists are also further divided into first and second generation antihistamines. first generation antihistamines include diphenhydramine (Benadryl) and Hydroxyzine. These tend to cause drowsiness. With second generation H1 antagonists cause fewer side effects and include drugs like loratadine (Claritin) and cetirizine (Zyrtec)
H2 antagonists primarily affect the gastrointestinal tract and include medications like famotidine (pepcid)
Typically when treating MCAS a person will be put on both a second generation H1 antagonist and an H2 antagonist.
When antihistamines do not treat symptoms well enough the next step is a mast cell mediator. The most common mast cell mediator is cromolyn sodium which is available by prescription only. (this is technically available OTC but it is at 1/50th the dose used for MCAS) Mast cell mediators work by preventing the degranulation of mast cells in the first place.
When both antihistamines and mast cell mediators are insufficient someone with MCAS might be prescribed a biologic such as Xolair to treat their remaining symptoms.
Sources:
American Academy of Allergy, Asthma, and Immunology
Mast Cell Hope
Mast Cell Activation Syndrome: Proposed Diagnostic Criteria
#mast cell activation syndrome#mcas#mast cell disease#mast cell activation disorder#mcad#chronic illness#chronically ill#physical disability#physically disabled
48 notes
·
View notes
Note
wait you’re literally so right abt bipolar wilson. begging you to talk about it more tbh bc yeah. Yeah.
oh absolutely, one of my favorite Wilson Subjects.
um wilson having bipolar 2 is something i think of as essentially canon. it would have been potentially problematic for him to be on mood stabilizers as a physician (medical licensure is.. really ableist...) which imo serves as an explanation for why he is on antidepressants- also makes depressive episodes objectively canon.
(hypo)mania leads him to make a lot of weird ass decisions! he's got impulsivity problems that would look a lot worse if he didn't have house around to make him look comparatively normal, with two great examples being in birthmarks- the broken mirror in new orleans and when house pisses him off at the funeral home.
he's got relationship habits that are pretty bipolar-typical; he gets in emotionally intense and often sexually-driven relationships (bonnie says as much) that burn out fast. this isn't like, bipolar diagnostic criteria or anything, but it's a common experience.
imo one of his most manic incidents in the show is his 2nd relationship with sam: he gets in this relationship on a whim and then KICKS HOUSE OUT about it. he PROPOSES TO HER AT SOMEONE ELSE'S WEDDING, a decision that just about anyone can recognize as a huge social faux pas! something HE would usually say is a stupid choice and a bad idea! this immediately explodes in his face.
also.. the paper he wrote about euthanasia! another vaguely manic decision. house kind of saved him from the fallout of that one.
oh, yeah and the fucking CHEMO DUDE FUCK!!!! severe black-and-white thinking moment from him that leads him to make a decision that is actually completely detached from reality. he is manic for this entire arc which would not on its own contribute to a bipolar dx due to clear and obvious stressor but as a character i already think of as having it... contributes. kyle, especially.
there are like. more examples. i cant think of more off the top of my head but there are. i am going to make a tag on my blog for this so that i can add to it as i think of them.
28 notes
·
View notes
Text
Adrien Agreste and Borderline Personality Disorder
DISCLAIMER: I've been a bit low on spoons this week, so I haven't gathered as much evidence as I probably could have. Also, I am but a humble student in clinical psychology. This is mainly a thought compilation for @moonieratty!
To introduce the topic, without going into it too much, personality is described by features and behavioral patterns, or traits, consistent across situations and across time. Personality disorders are therefore enduring patterns of highly maladaptive traits evaluated in personal and sociocultural context (Dozois, 2019, p. 290).
Like other disorders, personality disorders have diagnostic criteria. The DSM is used primarily for diagnosis in the US and Canada while the ICD is used more widely in Europe and other places. I'm more familiar with the DSM, but I've included a brief section on the ICD to be comprehensive. It ended up a bit longer than anticipated, so let's go below the cut. Warning for discussions of abuse, self harm, and suicide, and a brief mention of substance use.
Overview of Borderline Personality Disorder
BPD is prevalent in a small percentage of the population, about 1-2% by varying estimates, and is characterized by instability across domains of emotions, identity, interpersonal relationships, and behavior. Its onset is usually in late adolescence or early adulthood and symptoms may diminish with age, after one's thirties or forties, especially with therapeutic intervention. Along with ASPD, it has been the focus of a lot of clinical research; it is unfortunately associated with high rates of non-suicidal self-injury and suicide (APA, 2022, pp. 754–755; Dozois, 2019, pp. 308–309).
Etiological factors for BPD include both biological and environmental disturbances. Of note to our discussion is the heightened risk for BPD in cases of child abuse or neglect, as well as growing up with another family member with a serious mental health condition (NHS, 2022). It's been well established that Gabriel is emotionally neglectful if not outright abusive toward Adrien in multiple ways, so this is a clear risk factor. In addition, although I won't argue definitively for Gabriel having a psychological condition, he did keep Emilie's body in the basement, so there is clearly some kind of disturbance going on.
From a cognitive-behavioral perspective, Linehan argues that BPD stems from families who consistently invalidate childhood emotional experiences and "oversimplify the ease with which life's problems can be solved," which may cause children to learn to seek attention and communicate with others through emotional outbursts (Dozois, 2019, p. 297). This rings true for Adrien and Gabriel as well.
I have to apologize for my son, Ladybug, he's like his mother. Way too overly dramatic. (Jackady)
It doesn't seem like this is the first time Gabriel has thought this, and labeling an emotional reaction as being overly dramatic is very much invalidation of it. As for emotional outbursts, Adrien has had quite a few, mostly as Chat Noir. More on this later.
To round out this first section, attachment theory proposes a connection between poor parent-child attachments and BPD relationship difficulties. Specifically, maladaptive behavior in relationships may stem from childhood development of an anxious-ambivalent attachment style, where intense fears of abandonment interfere with a strong desire for intimacy (Dozois, 2019, p. 310). You can clearly see this in Chat Noir's relationship with Ladybug, and I'm sure other people have discussed Adrien's attachment style more in depth, but suffice to say I think this is an apt description.
Argument from DSM-5-TR
In the DSM, personality disorders are primarily diagnosed on a categorical model. There are a few general criteria which I won't be going into, but I will highlight that personality disorders are stable and pervasive, and would be diagnosed only if they were leading to significant distress or dysfunction. Adrien's mental state is not great, so the latter shouldn't be a problem, but this show does not always pay attention to consistency, so I'm going to be speculating some. Everything in this section is cited to the relevant DSM entry unless otherwise stated.
The DSM characterizes BPD with instability in relationships, self image, and affects, as well as marked impulsivity. It has no exclusion criteria, so BPD can be and frequently is comorbid with other disorders like mood disorders, PTSD, and ADHD. Of the below criteria, five need to be met in order for a diagnosis to be made.
Frantic efforts to avoid real or imagined abandonment
Hey, where're you going? . . . So you're allowed to know her true identity, but I'm not? (Syren)
You're not really replacing me with a turtle, are you? (Anansi)
A lot of people have delved into Adrien's abandonment issues, which feature most prominently in his relationship with Ladybug. His fears of being replaced result in him seeking reassurance from Ladybug, and he can lash out if he does not receive the response he hopes for. Ladybug is his world, and he wants to be hers, so anything infringing on that feels to him like a threat of being abandoned, and he does not like it very much.
Impulsive behaviors like giving up his ring can be interpreted under this lens: he can avoid abandonment by doing the abandoning first. Then it will be him leaving, and not the other way around.
I also interpret Adrien's nightmare (Le Marchand de Sable) as being a fear of being alone as much as it is a fear of being trapped.
Unstable and intense interpersonal relationships alternating between extremes of idealization and devaluation
We'll be united, more powerful and free. We'll defeat Hawk Moth, then we can both run away to an island! Far away from everything. We will live off nothing but fruits, and we will have a little pet hamster and we will name it— (Le Patineur)
I just can't do this anymore. I give up… on everything. Even you . . . If I become Chat Noir again, Ladybug will just end up rejecting me, over and over. (Kuro Neko)
Even though Adrien mostly keeps his head on straight regarding what he's owed and not owed by other people, his relationship with Ladybug is full of highs and lows. He thinks Ladybug is the most amazing girl, but this can recoil quickly into feeling as though Ladybug doesn't care about him enough or isn't meeting his needs.
Furthermore, he developed this idealization of Ladybug as a potential lover or caregiver at one of their first meetings (Cœur de Pierre), and continually sought to spend time together and share the intimate details of their secret identities early on. These are all common to individuals with BPD, as is the switch from idealization to feeling as if the other person "does not care enough, does not give enough, or is not 'there' enough." Ladybug is the only person Adrien consistently projects this instability and intensity on, which might be something interesting to explore.
Identity disturbance: unstable self image or sense of self
When I was a kid, I always wanted to be what my parents wanted me to be! (Exauceur)
But, does that mean Chat Noir is who I really am? Deep down inside? (Kuro Neko)
With all the secret identities, it isn't surprising that Adrien fits this criterion, but canon even explicitly draws a link between Adrien's unstable sense of self and his childhood experiences. He doesn't know who he is, and he distracts from this by being Chat Noir, only to struggle even more when he feels useless and underlooked as his hero self. His behavior shifts dramatically between trying to prove himself with grand gestures and refusing to participate or lashing out. There is definitely something to discuss on this front.
Impulsivity in at least two potentially self-damaging areas
Giving you some extra time . . . I trust you to bring me back, m'lady. (Gamer 2.0)
There are only two liars left in Paris and one of them knows the ultimate way to catch her attention . . . Crazy about you, m'lady. (Mensonge)
This is walking a thin line between impulsivity and suicidal behavior, which would be excluded from this criterion, but I'll list self sacrifice here because I can see an argument for Chat Noir's impulsive behaviors being out of love or the desire to be useful. There may still be some self injurious intent or euphoria, but Chat Noir does have faith in Ladybug to bring him back eventually. Nevertheless, this is impulsive and unhealthy. Chat Noir jumps too quickly to this option to have thought it through.
I can't think of another area, because Adrien isn't old enough for reckless driving, spending, substance use, or sex. This is also a kids' show. Just presenting these options for fanfiction writers out there.
Recurrent suicidal or self mutilating behavior, gestures, or threats
I... I don't know what to do! (Chat Blanc)
This is all our fault . . . Cataclysm. (Culpabysse)
By itself, what happened in Chat Blanc would not be solid evidence, as that was an unprecedentedly traumatic situation. Combined with Culpabysse, though, there is a strong case to be made for at least passive suicidality for this to be able to come up as an option.
You could also interpret the self sacrifice in this category. Suicidal behavior in individuals with BPD is often preempted by fears of rejection or abandonment, so an interesting analysis could be made on this front.
Affective instability due to marked reactivity of mood
He's still only thinking of himself! I just want this terrible day to be over and done with! I hate Christmas! (Pire Noël)
Sorry! Sorry! I didn't mean to make you so mad. I get it. You're sick of me . . . No one can help me, Kagami. (Glaciator 2)
Adrien's prolonged episodes of anger and despair reflect a high reactivity to emotional stressors, especially interpersonal ones. In general, he just doesn't feel very well unless something is actively bringing him joy. Most of his outbursts are brief, though, and I will discuss them as part of a later criterion.
Chronic feelings of emptiness
I'm not Adrien, so I wouldn't know if this is the case, but I can say he has experienced at least one depressive episode (Kuro Neko) and emptiness would not be unfamiliar. You can look at him and decide.
Inappropriate, intense anger or difficulty controlling anger
How was your amazing evening with your "friends"? . . . What do you think? (Glaciator)
Why not? No one'll know if I quit. No one'll care! (Syren)
A two-person plan?! There's only one two-person plan, and that's Ladybug and me! (Sentibulleur)
Give me a break, Miss "I can't even come up with a superhero name"! (Hack-San)
Anger in individuals with BPD can manifest as bitterness, sarcasm, or recurrent verbal outbursts, which Chat Noir absolutely exemplifies. These outbursts are often followed by feelings of shame or guilt and contribute to a feeling of being bad. Chat Noir apologizes after being harsh in Glaciator, and I wouldn't be surprised if he felt badly about the other times. Again, these outbursts are often precipitated by interpersonal fears and perceived threats of abandonment. Unlike other symptoms, this specific one tends to be unique to BPD.
Transient, stress-related paranoid ideation or severe dissociation
I cannot recall any evidence for this but headcanon away, my friends.
All in all, I think Adrien has a strong case for BPD presentation according to the DSM. Canon is not always consistent, but I think it presents an interesting and mostly coherent narrative for this lens. From this perspective, Adrien's behavior reflects a deep intolerance of being alone and a dependence on other people to define the self.
As a corollary, BPD behavioral patterns are frequently linked to self sabotage and self undermining right when a goal is about to be realized, which could manifest as dropping out of school right before graduating or ending a relationship when it seems to be going well. Food for thought. Individuals with BPD may also feel more secure with transitional objects like pets than with interpersonal relationships, which could reflect in Adrien's relationship with Plagg.
To add some subjective understanding to this clinical mumbo jumbo, I've added a source of genuine BPD experiences below (Mind, 2022).
Argument from ICD-11
With the release of the ICD-11, a dimensional model for diagnosis of personality disorders became the new standard. What this means is that individuals are no longer labeled as having 'histrionic' or 'dependent' or, indeed, 'borderline' personality disorders, but are rather assessed as having any form of personality disorder on a sliding scale of severity and with trait domain specifiers (Swales, 2022). To put it more simply, people are diagnosed only with a general personality disorder or personality difficulty which can be optionally specified as deviating on one of the personality traits in the Big Five model, which is well established in personality psychology.
This move has several benefits. Stigmatization related to particular personality disorders can be reduced, and differential diagnosis and comorbidity between personality disorders becomes irrelevant. However, people retain access to treatment and support. Evidence-based treatments like dialectical behavior therapy are particularly well established and crucial for BPD; for this pragmatic purpose, the ICD contains one additional specifier for borderline pattern personality disorder (Bach et al., 2022; Swales, 2022).
The DSM and ICD are designed to be compatible with each other in many ways, and in this case, the borderline specifier in the ICD is directly lifted from the criterion of the DSM (WHO, 2023, 6D11.5). Based on our previous discussion, Adrien would be equally qualified for a diagnosis in France. I would likely describe his personality disorder with moderate severity, where multiple areas of functioning are affected and self harming behaviors may be present, but not all areas or relationships may be equally impacted and traits are not as rigid and inflexible (WHO, 2023, 6D10.0–6D10.2).
Interestingly, the ICD includes three additional manifestations of borderline pattern which are optional and may vary across time (WHO, 2023, 6D11.5).
A view of the self as inadequate, bad, guilty, disgusting, and contemptible
An experience of the self as profoundly different and isolated from other people; a painful sense of alienation and pervasive loneliness
Proneness to rejection hypersensitivity; problems in establishing and maintaining appropriate levels of trust in relationships; frequent misinterpretation of social signals
I'm fascinated by the number of adjectives in here. I simplified very slightly, as I did with the DSM criteria, but I had to keep all these adjectives. Anyway, I won't elaborate for too many more paragraphs, so let's say sentimonster moment and leave it at that. I will spare you my mirrored Félix essay. For now.
Qualifications and Limitations
First of all, Adrien is a teenager. The distinguishing factor between a personality disorder and regular adolescent difficulties would be longevity and identity concerns beyond his developmental phase (APA, 2022, p. 758). Second of all, Adrien has a uniquely terrible home life and magical problems. Some of his behaviors could be normal considering his experiences and sociocultural context, and this matters when it comes to psychological evaluation. Take everything with a grain of salt!
More generally, the categorical model of the DSM has several issues, not to mention diagnostic issues related to culture, gender, and stigma. Some but not all of these issues are addressed by the dimensional model it includes in a later section, which shares theoretical foundations with the model of personality disorders in the ICD. Even so, issues remain. Diagnosis, access to treatment, and political statements are intrinsically linked in complex ways. I won't get into all of the nuances, but be safe, remember this is a fictional character, and keep an open mind.
REFERENCES:
American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders (5th ed., text rev.). https://doi.org/10.1176/appi.books.9780890425787
Bach, B., Kramer, U., Doering, S., di Giacomo, E., Hutsebaut, J., Kaera, A., De Panfilis, C., Schmahl, C., Swales, M., Taubner, S., & Renneberg, B. (2022). The ICD-11 classification of personality disorders: A European perspective on challenges and opportunities. Borderline Personality Disorder and Emotion Dysregulation, 9(1). https://doi.org/10.1186/s40479-022-00182-0
Dozois, D. J. A. (2019). Abnormal psychology: Perspectives (6th ed.). Pearson.
Mind. (2022, September). What does BPD feel like? https://www.mind.org.uk/information-support/types-of-mental-health-problems/borderline-personality-disorder-bpd/experiences-of-bpd/
National Health Service. (2022, November 4). Causes - Borderline personality disorder. https://www.nhs.uk/mental-health/conditions/borderline-personality-disorder/causes/
Swales, M. A. (2022). Personality disorder diagnoses in ICD-11: Transforming conceptualisations and practice. Clinical Psychology in Europe, 4(Special Issue). https://doi.org/10.32872/cpe.9635
World Health Organization. (2023). International statistical classification of diseases and related health problems (11th ed.). https://icd.who.int/
#miraculous ladybug#adrien agreste#ml meta#don't worry i read through far more sources than listed here#it's just standard citation procedure to include only in-text references and not readings for general subject comprehension#🌃#🌖#i'm using a hybrid parenthetical citation model which i think is most efficient and informative so just note this down#i can't believe i referenced kuro neko three times... what an episode#ml simon says#ml syren#ml anansi#ml sandboy#ml frozer#ml kuro neko#ml stoneheart#ml wishmaker#ml gamer 2.0#ml lies#ml chat blanc#ml guiltrip#ml santa claws#ml glaciator 2#ml glaciator#ml sentibubbler#ml hack san
84 notes
·
View notes
Text
Some Thoughts on Aspec Identity, Pathologization, and Disability
A lot of asexual and aromantic activism involves dismantling the notion that being asexual and/or aromantic is NOT a mental illness or medical condition, and while this is 100% true, it’s important that we in the aromantic and asexual communities recognize how our community is intrinsically linked to the disabled community. The fact of the matter is that, even though there is nothing inherently pathological about aromanticism or asexuality, our identities have historically been pathologized by society and are still often pathologized to this day.
The very first time I heard the word “asexual” used in mainstream media was in 2012 in an episode of House M.D., titled “Better Half.” For anyone who hasn’t seen it, the episode featured a side plot where an asexual couple comes into the clinic for a bladder infection, and the protagonist, Dr. House, decides that he wants to find a “medical cause” for their asexuality. This isn’t entirely unusual for the show, since a major part of House’s character is that he’s somewhat of an asshole who says a lot of blatantly offensive things and attempts to find medical causes for anything and everything. However, what makes this notable is that the subplot was resolved by House actually finding a medical cause for the patient’s asexuality and curing him of said asexuality. It was then revealed that the patient’s wife had been lying about being asexual to make her husband happy.
This was before Yasmin Benoit (an alternative fashion model who is among the most prolific asexual and aromantic community activists) publicly came out as aroace. This was before Bojack Horseman and Koisenu Futari and the 2015 Jughead comics (i.e., the ones where Jughead is confirmed to be asexual). For many people, this episode of House M.D., where asexuals are portrayed as being either liars or people who can and should be “cured,” was their first exposure to the concept of asexuality.
While this was just one episode of one tv show, it is a symptom of a much larger issue relating to the pathologization of asexuality and aromanticism. Take, for example, Hypoactive Sexual Desire Disorder (HSDD) which was defined by the following criteria in the DSM IV-TR:
A — “persistently or recurrently deficient (or absent) sexual fantasies and desire for sexual activity”
B — “marked distress or interpersonal difficulty.”
There are certainly plenty of cases where HSDD is unrelated to asexuality and is something that causes very real struggles for the person suffering from it; I won’t deny the experiences of these people by claiming that HSDD is “just asexuality” and shouldn’t be considered a disorder at all. The reason I bring up HSDD, however, is because it has often been used to pathologize asexual patients. It wasn’t until 2013 that the DSM-5 was released and changed the diagnostic criteria to include the caveat that “If a lifelong lack of sexual desire is explained by self-identification as ‘asexual,’ then a diagnosis of female sexual interest/arousal disorder would not be made.”
While this is a step in the right direction, the addition of this caveat has not people from pathologizing asexuality. A 2015 study (linked at the bottom of the post) by Dr. Lori A. Brotto, Morag A. Yule, and Dr. Boris B. Gorzalka notes that “Various theories have been proposed to explain how asexuality should best be classified, and some have maintained that asexuality is an extreme variant of hypoactive sexual desire disorder (HSDD)—a sexual dysfunction characterized by a lack of interest in sex and significant distress. To date, this has never been empirically examined.” (The study in question sought to empirically examine this very issue and found that “there are notable differences between AIS >40 individuals (those likely to identify as asexual) and those who meet diagnostic criteria for HSDD.”). Another article (also linked at the bottom of the post), which was written by Dr. Lori A. Brotto and Sonia Milani, states that “Various theories have been proposed to classify asexuality as a mental disorder, a sexual dysfunction, or a paraphilia.” This is all without even getting into older ideas like the concept of “sexual frigidity,” which also may have led to many asexual and aromantic people being seen as disordered.
While there is much less information on how aromanticism, specifically, has been pathologized, it’s pretty well known within the aromantic and asexual communities that people outside out our communities often group us together or consider aromanticism a subset of asexuality, so the pathologization of asexuality also affects the way aromantic people are perceived. Not to mention the fact that, historically, people who chose to remain single, and especially women who chose to remain single, were often seen as deviant or unnatural.
Regardless of whether or not we, as individuals, are actually disordered, we are often viewed as being disordered solely on the basis of our aspec identities. Furthermore, there is a lot of actual overlap between the aspec community and the disabled community. While similar research has not yet been conducted in relation to aromanticism (in fact, there is very little research at all on aromanticism), studies of asexuality have found some evidence that asexuality may be associated with both autism and schizoid personality disorder. (And, not to bring up anecdotal evidence or anything, but I have often noticed myself that the vast majority of people in online schizoid communities seem to be asexual, aromantic, or both.)
Additionally, disabled people, particularly those who are physically, intellectually, and/or developmentally disabled, are often desexualized by society and assumed by default to be incapable of having romantic and sexual relationships, experiencing sexual or romantic feelings, or understanding sex and romance. As a result, they are affected by many of the same stigmas as asexual and aromantic people, regardless of whether or not they’re aromantic and/or asexual (in addition to all the other forms of ableism that they face).
All this is to say that the asexual and aromantic communities share a lot of common ground with the disabled community. This makes it all the more important that we fight against ableism and stand in solidarity with our disabled siblings, both inside and outside aspec communities. Moreover, this makes it all the more important that we recognize the prevalence of disabled people in the asexual and aromantic communities and acknowledge the ways aspec identity and disability can intersect.
So, here’s to all the disabled aces and aros out there. Here’s to the disabled aspec people who have been treated as broken or pitied. Here’s to the nonpartnering disabled aspecs who need caretakers or otherwise can’t live alone and are struggling to navigate what that may mean for their futures. Here’s to disabled aspecs who do want a relationship, sexual, romantic, or otherwise, but who struggle not only with finding a partner who will accept their sexual/romantic orientation(s) but also with doing so with a disability that affects their relationships. Here’s to alloaros who want sexual partners but struggle with disability-related issues that affect their sex lives, such as touch aversion, incontinence (including ptsd induced bedwetting and bladder/bowel motor tics), body dysmorphia, fatigue, and/or limited mobility. Here’s to d/Deaf, hard of hearing, low vision, blind, and d/Deafblind aces and aros, who are sick of being treated as though they’re “missing out” in more ways than one on some “fundamental” part of the human experience, (namely sight and/or hearing and sex and/or romance). Here’s to the developmentally and intellectually disabled aces and aros who are tired of being treated like children as grown adults. Here’s to disabled aces and aros. You are wonderful and it is such a privilege to share a community with y’all.
Edit: @arrows-for-pens pointed out that I forgot to add the links. (Thanks for that!) So, here are the links to the articles that I mentioned in the body of the post.
#disability pride month#disability#aromantic#asexual#ace#aro#aspec#aroace#long post#cw ableism#cw pathologization#cw aphobia
89 notes
·
View notes
Text
Mikan Tsumiki has Histrionic Personality Disorder

I bet you thought I was joking about typing up a whole analysis on this. Let me preface this by saying I'm not histrionic myself, so please let me know if I make any mistakes when discussing this.
This is less of a headcanon, and more of a theory due to the large amount of evidence, that being said, if you dislike or disagree with it, that's a-okay!
A nice long analysis under the cut.
To those unfamiliar with HPD, Wikipedia defines it as "a personality disorder characterized by a pattern of excessive attention-seeking behaviors, usually beginning in early adulthood" which certainly fits what we see of Mikan in canon.
Here's a screenshot for evidence:
That being said, we should point out that Mikan's behaviours in high stress situations like a killing game isn't equivalent to how she'd behave normally.
That being said, lets get into the actual diagnostic criteria for HPD!

I think we can right away check off E, since deliberately falling in suggestive positions is one of Mikan's main character quirks. I could post the CG of her doing this as evidence, but lets not.
I also feel like D is another easy criteria to mark off, since most of Mikan's relationships are characterized by her desire for approval and appreciation. This is most notable with her abusive relationship with Junko, but we also see some shades of this during her FTEs with Hajime, implying it isn't specific to this bad relationship.

Mikan needs somebody in her life that forgives her existence, and every action, both positive and negative, she takes. But that isn't all the evidence that I have that Mikan is continuously seeking appreciation and approval from others, since its a large part of her talent.
A lot of ways Mikan gets positive attention from others is through nursing them back to health, and its one of the few areas in her life she feels confident in. That being said, in one of her FTEs she says some... questionable things about her patents.

And here it is again in Danganronpa S, showing it wasn't just her phrasing things oddly.
Her working as a nurse isn't completely altruistic, since she feeds off the attention and power she has over her patients.
I think that checks off
"continual seeking for excitement, appreciation by others, and activities in which the patient is the centre of attention" really solidly.
I have less evidence for the rest of the diagnostic criteria, but I believe they fit anyway.
I feel like she fits
"self-dramatization, theatricality, exaggerated expression of emotions;"
but its a bit harder to say for sure due to a lot of Danganronpa characters doing the same thing, so its unclear how normal Mikan's reactions are in her own universe.
Mikan has one of the more extreme breakdowns of the series, but she was not entirely in her right mind at the time, so idk if I should count it.
She also has a very extreme shot to the heart event compared to other characters, where Hajime must propose to her to get the best ending.
Here are some quotes where she has a very exaggerated emotional expression, for your consideration.
""Ah! I-I'm sorry for laughing so suddenly! I-It's just...I can't help it. I'm just so happy, I can't remember the last time I made any friends... Ah, not that you actually want to be friends with me! I'm soooo sorry I said something so...presumptuous! I'll do anything you say... Just...please don't hate me...!""
""Ah, so in the end...you're all just a bunch of bullies, huh? Justifying your actions with fancy words... M-Making excuses for why it's not really your fault... E-Everyone always treats me like that... Always... "It's all her fault..." "Sh-She's the one with the problem..." I...I'm done with that! You hear me!? I'm doooooooooone! It's not fair...It's not fair not fair not fair notfair notfair notfair notfairnotfairnotfairnotfairnotfair... Why won't you forgive me!? If you did something wrong...you'd forgive yourself right away...! What did I do!? Why won't anybody forgive me!?""
I also think there's a solid argument for her meeting the "over-concern with physical attractiveness." criteria! It is the main way she gets attention, after all. A lot of her comments have to do with her body, and a lot of the presents she likes are things she can wear.
So long as you belive one of the 'maybe' criteria, then she has enough for a proper HPD diagnosis.
45 notes
·
View notes
Text
PROPOSED DIAGNOSTIC CRITERIA FOR MALADAPTIVE DAYDREAMING
Below is the proposed diagnostic criteria for MaDD. Note that MaDD isn't an official disorder at the time of writing this and is still being researched, meaning you cannot be diagnosed with it.
A. Persistent and recurrent fantasy activity that is vivid and fanciful as indicated by the individual exhibiting 2 (or more) of the following in a 6-month period. At least one of these should include criterion (1):
While daydreaming, experiences an intense sense of absorption/immersion that includes visual, auditory or affective properties.
Daydreaming is triggered, maintained or enhanced with exposure to music.
Daydreaming is triggered, maintained or enhanced with exposure to stereotypical movement (e.g., pacing, rocking, hand movements).
Often daydreams when feeling distressed, or bored.
Daydreaming intensity and length intensify in the absence of others (e.g., daydreams more when alone).
Is annoyed when unable to daydream or when daydreaming is interrupted or curbed.
Would rather daydream than engage in daily chores, social, academic or professional activities.
Has made repeated unsuccessful efforts to control, cut back, or stop daydreaming.
B. The disturbance causes clinically significant distress or impairment in social, occupational, or other important areas of functioning.
C. The disturbance is not due to the direct physiological effects of a substance (e.g., a drug of abuse, a medication) or a general medical condition (e.g., dementia) and is not better explained by another disorder, e.g., Autism Spectrum Disorders, Attention-Deficit/Hyperactivity Disorder, Schizophrenia Spectrum Disorders, Bi-Polar I Disorder, Obsessive-Compulsive and Related Disorders, Dissociative Identity Disorder, Substance related and Addictive Disorders, an Organic Disorder or Medical Condition.
Specify current severity:
Mild: Experiences mainly distress, no obvious functional impairment.
Moderate: One area of functioning is affected (e.g., work).
Severe: More than one area of functioning is affected (e.g., work, school or social life).
#maladaptive daydreaming#actuallymadd#immersive daydreaming#maladapting daydreaming disorder#luka.txt#cirque de la queue#sometimes ill see someone ask abt madd symptoms or if they can get diagnosed#and i have to resist the urge to copy + paste the whole diagnostic criteria#i want to make more info posts for madd#but oughh the Energy that would Require....eugh...#madd info
46 notes
·
View notes
Note
Hey!! Do y'all know where we can find any resources/symptom lists/etc specific to osdd-1b?? We've been questioning whether or not that might be a thing we have going on, but when we try to look into it, most of what we're finding groups DID and OSDD together and emphasizes memory gaps, which we dont really have.
Hey, we’re not a clinician or expert, but from what we know about DID and OSDD:
- there’s really not a huge amount of difference between these two disorders. The differences may be minor or arbitrary, and honestly the difference in diagnosis may vary vastly from clinician to clinician.
- that being said, there’s likely even less of a difference between OSDD-1a and OSDD-1b. We’re not a clinician and we have trouble sometimes understanding clinical language, so researching the differences between these subcategories (without turning to community-created content) has been difficult for us. Vaguely, we understand OSDD-1a to mean a dissociative disorder with amnesia but no parts/alters, and OSDD-1b to mean a dissociative disorder with parts/alters but no amnesia.
These things being said, we’ll include the information we could find. Please don’t disregard resources that have information on OSDD along with DID! Like we said, these disorders are closely linked, so it makes sense that they’re often grouped together.
Trying to find accurate, reliable info on OSDD-1b if anything reminded us how horribly under researched dissociative disorders are. We couldn’t find much that isn’t unsourced in a wiki or written on a personal blog.
^ this is an ask we answered in the past. A lovely system reblogged it with their thoughts and info regarding OSDD 1a and 1b
youtube
^ we really love the CTAD clinic! This video may be useful, though the clinician speaking here does advise against self-diagnosis and proposes renaming OSDD as “minor DID” which we don’t entirely agree with.
Please use critical thinking and your best judgement when exploring these links. You know yourself better than anyone else!
We’re sorry we couldn’t find more up-to-date, reliable, and accurate information for you. This might be something best brought up in therapy or with a qualified professional. Still, we hope something in this list of resources might help you.
💫 Parker and 🐢 Kip
25 notes
·
View notes
Note
so which is it, schizophrenic or schizoaffective? since they're mutually exclusive



that's not what "mutually exclusive" means !! i'm both
i have been diagnosed with both over the course of visiting various therapists, psychologists and psychiatric hospitals in my time seeking mental health help, because schizoaffective disorder is far, far less researched and well understood than schizophrenia. often when you are discharged from mental hospitals and get diagnosed w/ schizoaffective disorder, you are given resources for both schizophrenia and your given mood disorder, and sometimes you just straight up get diagnosed with schizophrenia and depression or bipolar disorder.
some therapists do not catch on to my mood disorder because we do not get the time to discuss the symptoms of bipolar disorder, so they do not find out about my manic episodes, irritability, delusions of grandeur, feeling unstoppable/on top of the world, etc. so they only end up diagnosing me with schizophrenia, because i spoke of hallucinations, delusions, disorganized speech and thinking, alogia, and so on, and that was more important to them at the time. it has been proposed that the criteria of schizoaffective be heavily revised or straight up removed entirely from the DSM-V because it's so often misdiagnosed, and a bit superfluous, as as much as 50% of schizophrenic patients have co-morbid depression, and the criteria doesn't differ that much from schizophrenia, or the present mood disorder.

so, it's both. also keep in mind that most people do not know what "schizoaffective disorder" means, so often times i use "schizophrenic" to convey what i mean. almost everyone has some grasp of what "schizophrenic" means. it gets it across easier
i have no idea where you heard that information, if it's tiktok, twitter, or youtube, please read medical journals written by psychiatrists, articles from accredited medical foundations, and so on. NAMI, NIMH and Cleveland Clinic are excellent resources for mental health information. You can find articles that list the diagnostic criteria for schizoaffective disorder, as well.
please do more research before sending messages like this to complete strangers who very have complex medical backgrounds and have visited doctors, received diagnoses, and have done their own research into their health conditions, i have no idea where you got your information from but it that an extremely bizarre and wholly incorrect interpretation of what "mutually exclusive" means.
89 notes
·
View notes
Text
ROUND 3, MATCH 7


Propaganda under the cut!
Vyn Richter
Propaganda
hes just genuinely really manipulative and shady, like he is a walking red flag. the first time u see him in the game's dream-like prologue, its when hes taking u out of a hypnotic trance. and he says, and i quote, "that may have been a dream, but this may not be reality" WHAT?? plus the way he treats his patients (hes a psychiatrist) bothers me. to quote the wiki about a 10 year old boy, "Vyn Richter discovered after reassessment that Huey did not meet the diagnostic criteria for autism, but rather had learned to use the diagnosis as a defense mechanism to avoid social interaction." hes just gross and i wouldn't trust him with a pet fish, much less an autistic child (or myself! an autistic adult!)
Vyn IS manipulative af, but he's also overall a irresponsible doctor? It is said that he's pretty successful and apparently his methods work, but he divulges private information of his patients, especially to the MC. In his personal story Vyn allows the MC to visit one of his patients (a dancer who is very unstable and totally not up to see a random girl) who don't even know each other and with no authorization whatsoever. There's also this card's story where he exposes the MC to a violent and unstable patient. While I haven't read that story myself, I know Vyn takes a hit trying to protect the MC, the illustration being his arm with blood. iirc the MC then bandages his arm but still, why would you expose her like that? He also says he likes the MC because she doesnt feel shallow, or not like other people, which is basically giving different and new answers to his funky psychological tests. He has no reason to do that. It's not even an "i can fix him" situation bc none of these things are ever acknowledged not even as problems
Rock
Propaganda
He is just.. so useless.
Rock is such a fuck boiiiiiii. He's lazy as can be and flat out tells the farmer upon proposing that he will not work under any circumstances, and is truly one of the only marriage canidates in the game who won't help the farmer with any chores once they start living together. He's also really stupid, and not in a cute himbo kind of way. More like straight up irritating. He also tries to have this playboy charm about him, but it comes across as being more sleazy than anything. For a character that does nothing but talk about how awesome he is, there is NOTHING about him that backs it all up lol
19 notes
·
View notes
Note
Hello!
Last year I was diagnosed with Attenuated Psychosis Symdrome, but when I go looking for reading material to learn more about it, I mostly either get scientific articles (which I have trouble understanding) or debates on whether it's even real or not :(
If you have the time, would you be able to help find some reading material on the subject that has a bit of an easier reading level?
Hey friend!
I found an article that states:
“The main features of attenuated psychosis syndrome parallel of the prodromal phase of schizophrenia. The person has very low-grade symptoms that can include as delusions, hallucinations, or disorganized speech, and the symptoms have been present for short period of time and worsened, but the symptoms are below the level of severity that would warrant a diagnosis of a psychotic disorder, such as schizophrenia.
As this is a condition for further study and not an actual diagnosis, there is no information regarding its prevalence, any co-occurring conditions, or other information that would normally be included with the description of a formal diagnostic category in the DSM-5. The condition is considered to be potentially useful in determining a potential risk that someone may develop a full-blown psychotic disorder such as schizophrenia. Some individuals who meet the specifications for attenuated psychosis syndrome are eventually diagnosed with a psychotic disorder, and some are not.”
Reading on the National Library of Medicine states:
The proposed diagnostic criteria for Attenuated Psychosis Syndrome in DSM - 5:
At least one of the following of symptoms is present in attenuated form [having been reduced in force, effect, or value], and is of sufficient severity or frequency to warrant clinical attention:
Delusions
Hallucinations
Disorganized speech.
Symptom(s) must have been present at least once per week [over a month span]
Symptom(s) must have begun or worsened in the past year
Symptom(s) is sufficiently distressing and disabling to the individual to warrant clinical attention.
Symptom(s) is not better explained by another mental disorder, including: Depressive or bipolar disorder with psychotic features and is not attributable to physiological effects of a substance or another medical condition,
Criteria for any psychotic disorder have never been met.
It looks like its being less debated on being real and more so finetuned before being approved as a formal DSM5 diagnosis.
I don't know if this was made easier to read than the medical journals, so if you have more questions feel free to shoot them over.
#asks#attenuated psychosis syndrome#aps#schizophrenia#schizophrenic spectrum#schizospec#schizoposting#psychosis#psychosis awareness#psychotic#schizo spectrum#schizospeaking#schizoaffective
12 notes
·
View notes
Text

Practical: Observation of canon depictions
Slaanesi corruption, even in milder forms, often manifests as impatience and impulsiveness resulting from a desire for novel or rewarding stimuli. Paradoxically it also manifests both as obsession with specific activities/goals to the point of neglecting everything else AND as inability to meaningfully focus on anything for long or high levels of distraction, depending on the character (or even within the same). Deprivation of novel or sufficiently intense stimuli results in listlessness, irritability or depression-like symptoms.
Theoretical: Implications when compared to diagnostic criteria
Slaanesh effectively is giving most of her followers ADHD to some extent, and that's probably one of the earlier signs that manifests before, say, physical mutations.
Practical: Proposed course of action
I am going to start yelling about defying the powers of Chaos in my best mid-Atlantic pseudo-British accent when I take my meds in the morning.
(header image is one of my minis - the Contorted Epitome)
#head canon#fan theory#slaanesh#don't let the Inquisition read this post#miniature painting#wh40k#my minis#chaos
23 notes
·
View notes
Note
i want to chime in as another person- my mind was changed on NPD years ago but it was only because of like, real human people talking about their actual experiences that helped me realize it was not The Evil Disorder (TM) in the same way that I realized ASPD wasn't THe Evil Disorder (TM). I guess I was maybe more likely to realize something was up because i also hit a bunch of the diagnostic criteria for it but like, when literally all you hear is "narcissist just means someone is a self centered asshole" it's hard to realize that that's not actually what it is at all.
and they for real taught us that shit in school. we had a whole discussion about the myth of narcissus and how obviously that hurt ~everyone else~ more than narcissus, even though he literally starved to death and turned into a flower. it took me until i was like 17 and someone else went "hey thats kind of fucked up" before i was like oh yeah. that was probably not something he did for fun huh
idk where i'm going with this but i respect the hell out of you being willing to brave the internet goblins and be like "stop being an asshole about ppl with npd" because its gotta hurt way more when people are being an asshole about something you actually got. i made like one or two posts ages ago about the "narc abuse" ableist bullshit and i remember it being enough of a headache even when it completely and totally was not personal for me bc i do not have it
oh uh idk im sure you know this but for the people in the back sitting around, aspd is antisocial personality disorder and people with aspd are also not evil malicious serial killers in waiting or whatever the ~common interpretation~ is and people with aspd are just as capable of being good friends and normal ass people who don't run around cackling evilly or whatever and kicking puppies, just like anyone else. but buying into ableist mythology about people's diagnoses is absolutely going to cut you off from other regular people who are just living their lives and is also associated with higher rates of violence against other people :,) bigots kill
To be honest, a large chunk of the reason I get so vocal about NPD is because of how bad the ableism has wormed its way into my head. It's pretty much a daily occurrence that my housemates have to remind me that asking for help isn't manipulative and that I'm not being an evil little monster just for needing reassurance. Anti-cluster-B ableism curls up in your head and feeds on all your insecurities and struggles and it's so, so goddamn hard to deal with.
I can't ask for help getting out of bed on high pain days without getting paranoid that I've somehow manipulated my husband into being my reluctant servant. Doesn't matter how many times he reminds me that he's here because he loves me, and how helping me out of bed is an expression of that love. The internalized ableism still makes me so deeply fucking afraid that I'm the shitty one.
I have a daffodil tattooed on my head as part of my big floral scalp piece, and it's for Narcissus. Ovid's version of the story is the one that's always stuck with me the most, where Narcissus is tricked into his downfall by Nemesis. His worst crimes were "rejecting proposals from people who felt entitled to his body" and "being kind of an asshole, which is something that literally everyone is guilty of at times."
In the end, Narcissus didn't waste away because he was too self-absorbed for anything else, it happened because he was treated with trickery instead of compassion.
97 notes
·
View notes
Text
The medical field has a long, long history of naming different things after Greek myth, almost always using these to shuttle around some really unfortunate implications. Obviously, narcissistic personality disorder comes from the Greek figure Narcissus, which is very much a veiled insult bc Narcissus' whole story was that nobody liked him and that he was punished for liking himself so much.
HOWEVER. HOWEVER. If we must keep the theme, but we chose to give NPD a better name (and we really should), I have a much better proposal (imo at least):
Name it after Icarus in some way. An Icarian personality, or something. That story's always been framed as a tragedy, a boy that finally found freedom and over-estimated his own abilities. Yes, he died for it, but the myth was not so much of a condemnation (at least not to my interpretation). Basically every myth ends with the mortal dying, so you have to account for that.
But anyway, I feel like Icarus as a name does a way better job of capturing that constant feeling of needing to "reach for the sun" and be perfect in every way and constantly suffering for it, because THAT'S what NPD is actually about - not manipulation or vanity. We can participate in those things, sure, as can anyone, but that's not the crux of the disorder.
I think the crux of NPD is always reaching for the sun and then burning for it, and having to deal with having this disorder is definitely a tragedy. So, I'm saying, an Icarian personality sounds banger af and far more accurate and considerate of the internal symptoms that diagnostic criteria relentlessly ignores.
Thoughts from my narcissistic friends always welcome, of course <3
78 notes
·
View notes
Text
By: Dennis Noel Kavanagh
Published: May 22, 2022
[ Above: LGB Alliance making a point no charity should ever have to make ]
Of all the many absurd frauds perpetrated by gender ideology/biology denial the most egregious is the audacious lie “This is just like gay rights”, or the common riposte from the hard of thinking: “That’s just recycled homophobia”.
Such phrases are normally uttered by some risible gender borg, more often than not in answer to an actual homosexual daring to voice even a mild objection to the increasingly eccentric and dangerous demands of a creed whose main aim seems to be the re-medicalisation of homosexuality by force of gender.
Paradoxically, of course, Gay Rights 2.0 is actually the fight against biology denial, not for it and, with unerring symmetry, homophobia 2.0 is of course the fight to seriously sustain the argument that children playing with the wrong toys (normally gay) require surgical correction. For the sake of practicality and utility if nothing else, I propose here to set out why biology denial’s claim to our history, heritage and social position as gay rights activists is a fraudulent and sinister mockery of what our movement is, and what it stands for. Gender is a fraud by abuse of trust, most commonly a linguistic sleight of hand or a superficially plausible mapping of one issue onto another.
It’s easy to be fooled of course. Biology denial is a sort of hateful gay rights re-enactment society for bored bourgeois kids, some no doubt genuinely believe themselves to be fighting for “trans rights”, famously, none can specify the particular right when pressed. None can or do deal with detransitioners or inconvenient facts like homophobia being raised by the head of safeguarding at the Tavistock as a concern. Biology denial is a voluntary cyclops with one hand covering an eye which might otherwise survey the human collateral damage of this strange and failed aesthetic flesh cult. But then the acceptable casualties tend to be gay of course. That alone should provide you with a telling clue as to what is really going on.
[ Above: The absurd reconceptualisation of gay people as privileged beneficiaries with no history of pain ]
The 10 reasons biology denial is not Gay Rights 2.0:
(1) Biology denial regards gender non conformity as a medical issue
Biology denial position: Playing with toys atypical to societal gender roles should be regarded as the diagnostic criteria for experimental drugs with known results (underdeveloped genitalia, bone density deficits etc.) and as yet unknown results such that Nordic countries and France have now banned/seriously restricted their use. These drugs lock children into medical pathways with studies showing 97%+ graduation from puberty blockers to cross sex hormones.
Gay Rights position: Let children play with whatever toys they happen to like. Gender non-conformity is perfectly normal in our community. Children should not face lifelong medicalisation because homophobia is not taken seriously as a safeguarding issue at facilities engaging in gay conversion by gender.

[ Above: A mocked up satire on heterosexual MPs unwittingly supporting gay conversion by gender having not properly looked into the safeguarding of young gay people ]
(2) Biology denial is well funded, well connected and supported by left and right
Biology denial position: The profoundly religious and unevidenced suggestion that everyone possesses a gender soul enjoys huge corporate support and is also the de facto position of almost all trade unions in the UK. That consensus is largely mirrored in politics where the classic alignment of a political party is not a reliable indication of where it’s members stand on biology denial. While the right wing are in general terms more resistant to mass medicalisation of children, some of the most prominent gender borg acolytes in the UK are found on the Conservative benches. Ancillary to both is a monocultural charity sector where numerous “LGBTWTF” charities in effect act as proxies for one another. This leads to intellectual stagnation and discourse characterised by mantra like repetition of absurd phrases in place of arguments.
Gay Rights position: The gay rights of old and today is a grassroots phenomenon containing actual homosexuals. A comparison as between the funding arrangements for LGB Alliance, Gay Men’s Network, Lesbian Labour etc. and the leviathan biology denial outfits would be like comparing a local sports team to a televangelising mega church. Corporations and unions in the past had limited affinity with classic gay rights and support from both left and right was earned through open debate and discussion, rather than by diktat, shaming or dubious membership schemes requiring payment and adherence to a set of doctrines. Where BD is organised, lavish and entrenched in power structures the gay rights of old and today was and is a movement of private individuals giving up free time to fight homophobic hate.
(3) Biology denial rewrites science, language and history to appear organic
Biology denial position: Intersex/DSDs (Differences of Sexual Development) conditions should be dishonestly leveraged to argue sex is a spectrum despite such conditions being differences of either male or female development. Language control should become normal with a privileged class requiring forced/coerced language socially and in written communications. New words should be fabricated for an ever increasing range of biology denial identities and parties not adhering to new speech codes should be punished/ostracised/humiliated as “hateful”. Gay people may present a threat or object to the misuse of their movement as a vehicle for these aims so should be humiliated and demoralised by being told they owe all their rights to biology denial, their history should be extensively and audaciously rewritten to minimise/erase achievements by gay men and lesbians. History should further be raided and recrafted such that a claim to the long term existence of biology denial can be dishonestly made.
Gay Rights position: (Science) Human beings are not sequential hermaphrodites so cannot biologically change sex. Intersex/DSD conditions are not a debating prop nor is it fair or right to deploy these conditions when those with them loudly and repeatedly ask you not to. (Language) Coerced language is wrong and is simply a show of social power verging on bullying. In Gay Rights the advent of gay marriage was not accompanied by a demand that heterosexuals started saying “cis straight marriage”. Changing words is wrong and imperious. Homosexuals are not “homogendered”, nor is it morally acceptable to summarily redefine us in this way. The only language we’ve ever asked someone to accept is to get used to “his husband” or “her wife” and funnily enough most people are completely fine with that. (History) The achievements of lesbians, gay men and bisexuals should not and will not be forgotten. No social force/philosophy or cult has the right to rob people of their heroes. Our history should be accurately described according to facts, not rewritten to suit an oppressor class exploiting our movement and erasing our historical agency. Truth matters and gay history matters. We are a minority and minorities have more need of heroes that majorities. Children should not be taught lies about the Stonewall riots to suit the political objectives of biology denial and no movement should normalise the practice of trafficking in falsehoods.

[ Above: A sadly accurate assessment of how biology denial repackages historic anti-gay hate ]
(4) Biology denial believes in cancellation, silencing and harassment
Biology denial position: Disagreement of any kind should be met with pile-ons, attempts to get people sacked/driven from their jobs through stress, doxing and dishonestly representing their positions in the worst light all the while simultaneously maintaining that “there is no such thing as cancel culture”. Women in particular, like Maya Forstater, Professor Kathleen Stock and Professor Jo Pheonix are to be particularly targeted as they will engage in a reasonable manner and attempt to show kindness. As many BD adherents are fundamentally cowardly by nature, they will just about be able to add to the voices harassing these women where they would likely steer clear of a biological male. Only in this field, paradoxically, will the faithful unerringly recognise the biological demarcation between male and female. These public humiliations should chill freedom of speech and people should be afraid to say what they want with accusations of “hate speech” or “phobia” being made at the least provocation and on a hair trigger in order to silence any dissent.
Gay Rights position: An equal age of consent, gays in the military, equal marriage and employment protections required precisely zero women to lose their jobs nor did they require that anyone who opposed these measures be cancelled. We engaged in freedom of speech and a debate which is healthy and proper in a democracy. We note two of the women (Professors Stock and Phoenix) named above are lesbians, that is no accident. Lesbians were the first target of the biology denial movement particularly in the form of the demand they stop being lesbians and start sleeping with male bodies persons. That is homophobic. Chilling freedom of speech more generally and harassing people brings the gay rights movement into disrepute and squanders the goodwill brave lesbians and gay men built up over decades as it recasts itself as a bullying, authoritarian enemy of free speech.
(5) Biology denial believes in legislative change by deception
Biology denial position: There is no popular mandate for medicalising mostly gay kids or introducing the concept of gender souls into legislation such that the concept of “woman” is reduced to a self-declared feeling. If the public are left with a normal functioning legislative process, most would be horrified about matters such as homophobia as a child safeguarding concern at gender clinics or the reality of female prisoners forced to share cells with male bodies persons. The democratic process should therefore be subverted and far reaching legislative changes should be snuck into the law by abusing the close and unhealthy connections biology denial lobby groups have with legislators. Speaking to the public or actual gay people should be avoided as gay people in particular are likely to recognise and highlight the homophobia of biology denial. A vivid example is Stonewall’s campaign for there to be no public consultation on the “conversion therapy ban” (in reality a charter for gay conversion by gender).
Gay Rights position: Legislation in a democracy should be made on the basis of evidence, not ideology and normal consultation processes should be followed. The public should know what legislation contains and debates should be open and clear about what is being proposed. When the Gay Men’s Network and many other organisations responded to the government’s consultation on the “conversion therapy ban” we made the case that it amounted to conversion by gender. This is what gay rights organisations should be doing - fighting homophobia wherever it threatens gay people. Any policy that has to be snuck through a legislative process is, by definition, a change with something to hide. Gay rights movements have nothing to hide and we have never had to lie or obscure our policy objectives.
(6) Biology denial targets children for indoctrination
Biology denial position: Despite there being no evidence for this proposition and its far reaching consequences, children should be taught at school that they have a gender identity and this spiritual belief should be reinforced across youth media and through as much mainstream television as possible. Children are pliant and impressionable and less likely to ask questions. They should get the impression biology denial is fun and fashionable and present in ever increasing numbers at gender clinics so this movement can sustain a moral civil rights / safeguarding claim. Any suggestions of social contagion or harm should be met with as per (4) above with the claim that such concerns are hate.
Gay Rights position: Teaching children unscientific pseudo-religious dogma about gender souls is morally wrong and tantamount to using education as a way of proselyting a new religion. It is no accident the number of children presenting at biology denial clinics has risen in the UK in one instances of 5000% and in Scotland 1000%. To imagine that this increase is purely coincidental with these matters being taught in schools stretches credulity far beyond breaking point. Many of the children targeted in this way are gay. It is homophobic to teach gay children that they have the wrong bodies because they do not fit a sex stereotype. This is thus simply another homophobic religious belief which has no place in schools and it amounts to a serious safeguarding concern.
[ Above: The CEO of Stonewall equating lesbianism with a “societal prejudice”. ]
(7) Biology denial is racist
Biology denial position: Black people are a subset of the sex class to which they belong. The interests primarily of a group of white men with biology denier related identities come first. Countries that were colonised did not have a concept of male and female before white Western imperialism and were in a noble state prior to such corruption. What they now need is a new group of (mainly white) biology deniers to explain this to them and they should be re-educated in the ways of biology denial.
Gay Rights position: Allison Bailey was right to say in her keynote address at LGB Alliance conference that she had never known racism such as that emanating from biology denial / gender ideology. Her quote “if black women can be women, why can’t I” is a shocking illustration of the obvious racism of this movement. The targeting of Allison Bailey , Sonia Appleby, Kiera Bell and the public vilification of Baroness Kishwer Falkner is beginning to suggest that women of colour who speak out against biology denial face particularly harsh consequences. White men adopting biology denial identities seem to be at the forefront of this movement and many of them appear to be heterosexual.
(8) Biology denial is misogynist
Biology denial position: The word “woman” has no fixed definition and anyone who says they are woman is one, except adult human females who may only say that they are “menstruators”, “cervix havers” etc. Women should have no sex-based boundaries at all from toilets to bathrooms to prison cells or rape shelters, women who challenge this position at rape shelters should be called “bigots” who should “reframe their trauma”. The concept “woman” should primarily be understood with reference to sexual stereotypes and the performance of a particularly porn-based understanding of femininity. Women in particular who dissent (see (4) above) should especially be targeted for cancellation and silencing.
Gay Rights position: A woman is an adult human female. As homosexuals, same sex spaces and boundaries are not just necessary, they are the existential framework of our minority community. It is demeaning and morally wrong to existentially acid strip meaning from the word “woman”. The male Gay Rights movement has no interest in, or desire to compromise, female sexual boundaries or spaces. The lesbian Gay Rights movement has no interest in, or desire to compromise, male sexual boundaries or spaces. That is what makes us gay. The fact biology denial is preoccupied with this quintessentially heterosexual endeavour makes it a straight rights movement, not a gay rights one. The open harassment and abuse of women that goes on in the name of biology denial should be a source of shame to it. The fact it is not demonstrates aptly the contempt in which it truly holds women.

[ Above: A statement so utterly homophobic of course the author wasn’t cancelled ]
(9) Biology denial is homophobic
Biology denial position: Gay people are second class members of the movement who lack the determination to embrace one of biology denial’s ultimate goal, the surgical transformation of homosexuals into ostensible heterosexuals. Gender nonconformity should be medicalised. Lesbians and gays who disagree with this should be cancelled and excluded from their movement, charities and any social spaces where they might organise. Those who go along with this should be rewarded and encouraged to engage in woke conversion therapy propaganda.
Gay Rights position: Homosexuality is not a medical problem, our same-sex attraction is in fact a protected characteristic pursuant to s.12 of the Equality Act 2010 in the UK. Gay people owe it to the next generation to speak up in the face of our political vehicles being taken from us and we must make our own new organisations where necessary and form such groups/alliances as are necessary to protect our community. Biology denial is an existential attack on our minority community and it regards us as second class citizens. We must challenge and defeat it. We have to.

(10) Biology denial makes only pornography, not art
Biology denial position: As this in an inorganic, top-down movement it stunts creativity and blunts free thinking because both are threats to cult-like religions. Self-expression is limited to pre-designed identities and flags, each of which constrain and categorise human creativity while giving the illusion of choice. Biology denial produces a vast army of adherents who check and double check each other’s language/adherence to the core doctrines so will produce endless videos as to categorisation (what one can and cannot say without causing offence for example) and identities. This will keep followers in a state of fear where the primary concern is regulation of thought/language all the time purporting to celebrate authentic expression while completely annihilating that by the bureaucratic allocation of people into pre-approved conceptual categories. Because adherents will be in a state of fear and incapable of art, they will have less sex than the generation before so pornography and anime should be deployed to fulfil such needs as obtain.
Gay Rights position: Every era of gay rights has produced artists, poets, playwrights, singers, etc. who have produced world-changing art, music and prose. Gay Rights has never encouraged or been of a mind which makes or recycles mediocre memes. The free expression most gay people treasure from their first ever trip to a gay bar is mirrored in the free expression many treasure in our words, paintings or music. We have nothing in common with a bureaucratic allocation exercise endlessly obsessed with labels and we are very far away from a world view which deprecates or diminishes the perfectly normal appetite for sex.
==
It should be unsurprising that the Gay Rights position mirrors liberalism, while the Biology denial position is explicity anti-liberal.
#Dennis Noel Kavanagh#gay rights#gender ideology#queer theory#biology denial#same sex attraction#homophobia#homophobia 2.0#homosexuality#LGB Alliance#woke homophobia#religion is a mental illness
28 notes
·
View notes
Last Seen Blogs

mie-yarn
a corner.

ecoviewwindowsmilwaukeewi-blog
Ecoview Windows of SE Wisconsin, LLC

little-chubstr
LittleChubstr

galedekarios
our very souls do echo
lastleggysee
Shamelessly Annoying