#Mast Cell Activation Syndrome
Text
anyone else ever wish they could lie down harder? Like, I'm already horizontal, but I need more horizontal. I need to be absorbed by the floor. I think that would fix me
#My orthostatic tolerance is currently zero#POTS#postural orthostatic tachycardia syndrome#me/cfs#fibromyalgia#chronic illness#disability#migraine#gastroparesis#chronic pain#chronic fatigue#chronic fatigue syndrome#myalgic encephalomyelitis#spoonie#mast cell activation syndrome#MCAS#dysautonomia#chronic migraine#joint pain#hEDS#ehlers danlos syndrome#hypermobility#hypermobile ehlers danlos#interstitial cystitis
29K notes
·
View notes
Text
tw: content under a cut for talking about calorie counting (in a positive way), restrictive medical diets, and MCAS 'remission.'
So it's been 5 months since I last saw the GI doctor who took me seriously regarding my mast cell dysfunction, and not only have I gained a LOT of foods back into my diet under his care without experiencing idiopathic anaphylaxis, but I've also managed to eat 2000 calories almost every day for the last 5 months.
Prior to his care, since 2020, I had been mostly surviving on a liquid diet with the odd bit of solid carbs and protein when I could handle it.
Which was better than the 2 things I could digest safely prior to 2019, which were oatmeal and filtered tap water toward the end when I was dying. But even after I recovered from that, any time I went over 700 calories a day in solid food, I'd be writhing in pain.
I still have days when the pain hits, and all I can manage is liquids, but those days are so much less, and thanks to being able to eat more foods, I can at least liquidate more nutrients to make sure I'm getting what I need.
Things will never be 100% healed. That's not the nature of this kind of immune disease. But they're better. I'm better. I'm still so scared to say any of this is in remission because MCAS is wildly unpredictable. But I'm so much better than I was.
And I'm going to go happy-cry and eat a gluten-free cupcake about it.
#chronic health tag#MCAS#life with allergies#restrictive medical diet#mast cell activation syndrome#illness remission
998 notes
·
View notes
Text
I was out with my family for my birthday at a restaurant when I started having an allergic reaction. So I pulled out my IV stuff to give myself something to stop it and my dad asks:
“Do you want to go in the bathroom and do that”
I laughed a little “um, not really”
I understand it’s a little strange for me to pull out needles and meds and everything in public, but the restaurant bathroom is the last place I want to be when setting up something to inject into my blood stream 😬
Can we normalize people having to regulate their bodies with medication in public please?
#disabled#disability#pots#chronic illness#chronically ill#chronic pain#dysautonomia#mcas#mast cell activation syndrome#spoonie#heds#chronic fatigue#postural orthostatic tachycardia syndrome#hypermobility#hypermobile eds#hypermobile ehlers danlos#ableism
3K notes
·
View notes
Text
Medical Person: What are your symptoms?
Disabled/Chronically Ill Person: This is a trap.
#chronic illness#me/cfs#myalgic encephalomyelitis#chronic fatigue syndrome#pots#postural orthostatic tachycardia syndrome#ulcerative colitis#ibd#inflammatory bowel disease#polymorphic light eruption#solar urticaria#mast cell activation syndrome#postural tachycardia syndrome#disability
257 notes
·
View notes
Text
shout out to those of us chronically ill people who have stacks of rare diagnoses that took years or decades to dx. Shout out. to those of us in those categories who had earlier diagnoses questioned because of our other, at this point undiagnosed, rare illnesses.
To have a doctor look at something very concrete and telling of a certain diagnosis (for me, it was a muscle biopsy that showed a very obvious mitochondrial cytopathy) and go 'nah i don't think its actually this thing we have evidence of' because you also have another completely unrelated rare illness is gross and inexcusable.
If you are in this situation, i pray that things prevail for you. Remember that you know your body far better than any medical professional ever will, and that no matter what they say, you're not crazy for having inexplicable symptoms.
to deny the idea that someone can be doubly sick with three or more different rare illnesses when we know so little about genetics and all the different ways the human body can screw itself over is extremely and without a doubt idiotic. we all deserve better.
#chronic illness things#chronic illness#chronically ill#cripple punk#queer cripple#cripple posting#crip punk#mitochondrial cytopathy#mitochondrial disease#mast cell activation syndrome#MCAS#cowden syndrome
311 notes
·
View notes
Text
If you wear strong fragrances in public I hate you ♥️
#personal#chronic migraine#chronic pain#chronically ill#chronic illness#mcas#mast cell activation syndrome#disabled#cripple punk#autistic adult
86 notes
·
View notes
Text
Hi! I’m a chronically ill design student studying the experiences of people with chronic health conditions interacting with primary care If anyone would like to take my survey that would be great!
#spoonie#chronic illness#chronically ill#mental health#neurodivergent#pots#elhers danlos syndrome#chronic fatigue#adhd#autism#fibromyalgia#mast cell activation syndrome#chronic pain#invisible illness#sickle cell disease#diabetes
62 notes
·
View notes
Text
i have a history of chronic illness, so i've been to many doctors. but you know the one i hate the most (besides the obgyn)? dermatologists.
i'm an afab genderfluid person with mcas. yes, i have acne. but i don't go to the dermatologist for that. i go for other things. but you know what they always bring up? acne treatment. no, thank you.
why do people think i must rid myself of my acne? i literally don't care about it. in fact, it kinda makes me, me.
my acne causes no harm to me. it doesn't hurt. it's just there. treating it could cause me harm (ie. a flare up), so i don't want to risk it.
but society seems to be offended by acne, especially on afab people.
idk this was just a rant. but like i hate beauty standards ughhhh
#chronic illness#mcas#mast cell activation syndrome#actually autistic#genderfluid#nonbinary#genderqueer#acne#acne pride#autism#autistic#adult autism#afab#enby
168 notes
·
View notes
Text
What is Idiopathic Mast Cell Activation Syndrome?
Idiopathic Mast cell activation syndrome (MCAS) is one of several mast cell disorders. MCAS occurs when there are a normal number of mast cells in a person's body but they over-release mast cell mediators causing random allergic reactions in multiple systems of the body. MCAS is incredibly common being present in an estimated 17% of the population.
Symptoms
MCAS symptoms are incredibly varied and always occur in multiple systems of the body. Anaphylaxis is common.
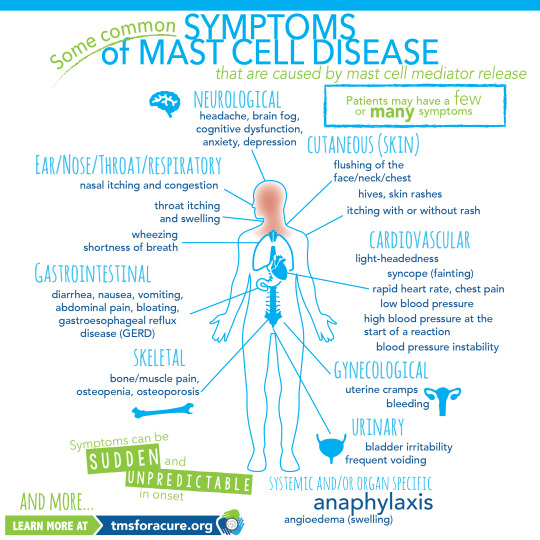
[ID: A graphic labeled "Some common symptoms of Mast Cell Disease" A graphic of a person standing in the center with multiple organs visible is shown. Around the person are lines pointing to specific areas of the body labeled with the body system and symptoms. Clockwise these read "Neurological headache, brain fog, cognitive dysfunction, anxiety, depression Cutaneous (Skin) flushing of the face/neck/chest, hives, skin rashes, itching with or without rash Cardiovascular light-heartedness, syncope (fainting), rapid heart rate, chest pain, low blood pressure, high blood pressure at the start of a reaction, blood pressure instability Gynecological uterine cramps, bleeding Urinary bladder irritability, frequent voiding Systemic and/or organ specific Anaphylaxis angioedema (swelling) Skeletal bone/muscle pain, osteopenia, osteoporosis Gastrointestinal diarrhea, nausea, vomiting, abdominal pain, bloating, gastroesophageal reflux disease (GERD) Ear/Nose/Throat/Respiratory nasal itching and congestion, throat itching and swelling, wheezing, shortness of breath and more" In the bottom left corner "Symptoms can be sudden and unpredictable in onset learn more at tmsforacure.org"]
MCAS symptoms are specifically not allergies. the reactions may look like allergies but the two are not the same and MCAS is not a condition meaning "many allergies" While MCAS can have some consistent triggers one of the defining features of the disease is that reactions are random and happen unpredictably.
Anaphylactic shock is not a requirement for diagnosis.
Diagnosis
MCAS is diagnosed by an immunologist. It is in part a diagnosis of exclusion and requires ruling out both allergies and systemic mastocytosis as well as other conditions such as certain types of tumors.
Diagnostic criteria for MCAS is debated. Some immunologists follow the symptom-based diagnosis approach in which case the diagnostic criteria are:
Recurring and severe anaphylactic-like episodes that involve more than one organ system
and
Positive response to mast cell stabilizing or mediator medications anaphylaxis-type symptoms
Others follow diagnostic criteria based on laboratory findings. In this case the diagnostic criteria are:
Episodic symptoms consistent with mast cell mediator release affecting two or more organ systems evidenced as follows:
Skin: urticaria, angioedema, flushing
Gastrointestinal: nausea, vomiting, diarrhea, abdominal cramping
Cardiovascular: hypotensive syncope or near syncope, tachycardia
Respiratory: wheezing
Naso-ocular: conjunctival injection, pruritus, nasal stuffiness
and
A decrease in the frequency or severity; or resolution of symptoms with anti-mediator therapy: H1 and H2 histamine receptor antagonists, anti-leukotriene medications (cysLT receptor blockers or 5-LO inhibitor), or mast cell stabilizers (cromolyn sodium)
and
Evidence of an elevation in a validated urinary or serum marker of mast cell activation: Documentation of elevation of the marker above the patient’s baseline during a symptomatic period on at least two occasions; or if baseline tryptase levels are persistently >15ng, documentation of elevation of the tryptase above baseline on one occasion. Total serum tryptase is recommended as the markers of choice; less specific (also from basophils) 24 hour urine histamine metabolites, or 11-beta-prostaglandin F2.
and
Primary (clonal) and secondary disorders of mast cell activation ruled out.
These are not all proposed diagnostic criteria as the subject is heavily debated. Generally, a laboratory-confirmed MCAS diagnosis is considered more legitimate.
Treatment
MCAS is a very treatable condition. Generally treatment follows a path from antihistamines -> mast cell mediators -> biologics.
Epipens are given to MCAS patients with a history of anaphylaxis.
Antihistamines are divided into 2 categories: H1 antagonists and H2 antagonists. These categories are determined based on the histamine receptor each one targets.
H1 antagonists mostly deal with systemic and cutaneous symptoms. H1 antagonists are also further divided into first and second generation antihistamines. first generation antihistamines include diphenhydramine (Benadryl) and Hydroxyzine. These tend to cause drowsiness. With second generation H1 antagonists cause fewer side effects and include drugs like loratadine (Claritin) and cetirizine (Zyrtec)
H2 antagonists primarily affect the gastrointestinal tract and include medications like famotidine (pepcid)
Typically when treating MCAS a person will be put on both a second generation H1 antagonist and an H2 antagonist.
When antihistamines do not treat symptoms well enough the next step is a mast cell mediator. The most common mast cell mediator is cromolyn sodium which is available by prescription only. (this is technically available OTC but it is at 1/50th the dose used for MCAS) Mast cell mediators work by preventing the degranulation of mast cells in the first place.
When both antihistamines and mast cell mediators are insufficient someone with MCAS might be prescribed a biologic such as Xolair to treat their remaining symptoms.
Sources:
American Academy of Allergy, Asthma, and Immunology
Mast Cell Hope
Mast Cell Activation Syndrome: Proposed Diagnostic Criteria
#mast cell activation syndrome#mcas#mast cell disease#mast cell activation disorder#mcad#chronic illness#chronically ill#physical disability#physically disabled
76 notes
·
View notes
Text
If you made a mistake (or two or five or hundreds) in your medical care, you are still a good person. You still deserve care, you still deserve to feel better 💙
#teaandspoons#disability#chronic illness#spoonie#chronic pain#chronic fatigue#food allergies#celiac disease#mast cell activation syndrome#pots#dysautonomia#mental health#diabetes#adrenal insufficiency
34 notes
·
View notes
Text
My sister: “So are you just not going to do anything ever again?” (Asking in reference to me not joining them on a family trip.)
Me: “Um, maybe. That’s kind of what being disabled means.”
Like seriously. Being disabled is literally not being able to do everything able-bodied people do. Me not going on the trip was a necessity so I didn’t push my body too far and crash, not something I chose because I didn’t feel like going.
#disabled#disability#pots#chronic illness#chronic pain#chronically ill#mcas#mast cell activation syndrome#dysautonomia#spoonie#postural orthostatic tachycardia syndrome#heds#chronic fatigue#ableism#hypermobility#hypermobile eds#part time wheelchair user#hypermobile ehlers danlos#ambulatory wheelchair user#me/cfs#chronic fatigue syndrome
948 notes
·
View notes
Text

Image description: Drawing of female presenting person with title “Anatomy of This* Spoonie.” The woman’s body is covered with different images representing the many symptoms she experiences. Caption at the bottom of image says “*This spoonie is Skye Harmon, a woman with Ehlers-Danlos sunrooms, rheumatoid arthritis, orthostatic and heart intolerance, mast cell activation, and fibromyalgia. It is not necessarily the experience of any other chronically ill humans.”
#ehlers danlos syndrome#hypermobile eds#rheumatoid arthritis#fibromyalgia#mast cell activation syndrome#pots syndrome#potsie#chronic illness#chronic pain#chronically ill#spoonie#disability#disabled#disabilties#original art#digital illustration#digital art
38 notes
·
View notes
Text
it’s strange, noticing new pains i didn’t used to have, adjusting to a new reality that i didn’t ask for.
14 notes
·
View notes
Text
i hate you ehlers-danlos syndrome i hate you pots i hate you chronic migraines i hate you brainstem auras i hate you central nervous system complications i hate you degenerative disc disease i hate you hypotension i hate you osteoarthritis i hate you fibromyalgia i hate you tmj disorder i hate you carpal tunnel i hate you mcas
#mood#sigh#i am having a day#disability#chronic illness#chronic pain#ehlers-danlos syndrome#dysautonomia#postural orthostatic tachycardia syndrome#migraines#chronic migraines#brainstem aura migraines#central nervous system#degenerative disc disease#hypotension#osteoarthritis#fibromyalgia#tmj disorder#carpal tunnel#mast cell activation syndrome#okay to reblog
267 notes
·
View notes
Text
My body: you’re stressing? Oh this is a threat to your body so that means that I’m gonna start a reaction to save you
Me: 👁️ 👄 👁️ you realize you’re causing more stress, right?
My body: I cannot not believe the stress levels in this bitch. So unexpected. So impossible to manage, I have to keep releasing more histamine.
#personal#mcas#mast cell activation syndrome#chronic illness#chronically ill#allergic reaction#disabled#ehlers danlos syndrome
44 notes
·
View notes
Text
One of my biggest tips for people with chronic illness…get yourself a nurse practitioner.
I told my nurse practitioner what happened at the ER and she immediately got ahold of her hospitals Cardiology department and bumped my appointment up three weeks so I could get in tomorrow.
I hear all the time from both doctors and patients that some how nurse practitioners are able to hang on to their compassion & empathy and believe me when I say that’s exactly the type of person you need fighting for you in the medical community.
#bad health day#health flare#chronic illness community#disabled community#disability awareness#dysautonomia#ehlers danlos syndrome#postural orthostatic tachycardia syndrome#gastroparesis#mast cell activation syndrome#hashimotosthyroiditis
471 notes
·
View notes
Last Seen Blogs

gottabounce8
Untitled

cyonkodhc
ちょんこDHC
rohitchauhan
Rohit Chauhan

harton31864412-blog
Untitled

lv99xjy
无标题