#cognitive behavioral therapy definition
Text
cbt may not be for me. my therapist is alway like “you should examine why you feel that way” and i’m like????? a.) i just explained exactly why i feel that way and b.) isn’t that what i’m here for??? so you can help me with the examining. like maybe i’m just bad at therapy and missing something but there’s only so many times she can tell me to be mindful before i take a hammer to the walls
#i get that therapists are supposed to offer tools not solutions but it’s been almost two months and the only tools she’s offered#is telling me to ‘stop. observe. breathe’ when i get anxiety#and a chart about how some feeling may actually just be other feelings#i’m like DUUUUHHHHHH#TELL ME SOMETHING I DONT ALREADY KNOW#i think i’ll stick w her bc the exposure therapy component has definitely been helpful so far and that’s what i need the most#but jesus am i getting frustrated#and it may be way more trouble than it’s worth trying to find a new therapist w my insurance who does telehealth and starting all over#personal#vent#i meant cognitive behavioral therapy not cock and ball torture btw
5 notes
·
View notes
Text
The Director
humiliation | dehumanization | conditioning
@augusnippets Day 16
cw: medical/lab setting, subject whumpee, captivity, see above
The operating theater was dim and quiet, free of machines and stainless metal trays and the buzz of nurses poking at every part of him. Maybe that was a good sign.
Although the observation deck overhead was dimly lit up as well. That definitely wasn’t.
He had been forced into some cushy padded chair. The researcher fussing over him was a vaguely familiar and unwelcome face by now, and most of the time she didn’t even bother speaking directly to him. “Director. I have been looking forward to showing you the progress we’ve made with this study. I think you’ll be… quite impressed.”
She was squeaky today, talking up to one big reflective wall. Like she had something to prove.
He pulled at his restraints. “Really chose your star student for this one, huh?”
“You’re aware of my efforts to achieve a state of neuroplasticity for our behavioral conditioning program,” the researcher continued unfettered, propping a halo-shaped machine right over his head. “Through exhaustive trials, I’ve finally achieved an inducible state of docility and submission. Each brain reacts so differently, but we are particularly proud of Subject 3B-167. He has taken to the induction very well.”
“The fuck are you talking about?” He started fighting even harder. The padded cuffs always had such a distinct way of cutting into his wrists and ankles, raw and ragged even under layers of gauze. “I haven’t taken to shit! All you do is drug me and cut me open and act like a fuckin’ cu—”
The machine gave one shrill little tone and lit up with a ring of blue light. Every part of him locked up like it was electricity, a single lightning strike through every muscle, clenching and stretching his skin gaunt. It lasted only as long as the beep, and then he just went slack— limp and lifeless, eyes glazed, mouth dropping open under the blue haze.
“Initial findings are promising: we’re seeing a consistent reduction in resistance, with the subject entering a compliant state in under three seconds.” She flicked her fingers in front of his eyes. He didn’t even twitch. “His reactivity varies, but most cognitive faculties are effectively shut down.”
She flicked off the blue light. The subject jerked and shuddered hard, blinking like it was just an odd muscle spasm. And then he kept on fighting without skipping another beat, not realizing the gap in his efforts. “—cunt! You stupid cunt! What are you trying to—ghh-”
The light flicked on and he slumped under its glow. She pushed his head back against the headrest. “I’ve tested this across various states of consciousness, but the results are especially intriguing when the subject is under duress. It seems the stress amplifies the effectiveness of the trigger. We can achieve total behavioral suppression.”
She dimmed the light until it turned off. This time he took longer to snap out of it, blinking hard before pulling in a sharp breath. He exchanged her observant stare with a confused one before finally lifting his head. He looked around. “What… What the hell’s going on?”
“Repeated therapies make the subject highly suggestible and seems to affect memory retention. He doesn’t even remember most of the procedures.” She sounded amused here. “Each reset wipes the slate clean.”
“What the fuck are you talking about, lady?”
The blue ring. His pupils blew wide. His neck kept landing at an uncomfortable, awkward angle, and the researcher shoved his head back before he could drool all over himself. “His defiance is only a facade now. Gone in an instant.”
When the light shut off, it took a long moment for him to regain his bearings. His brow hardened— frustration, maybe, like everything was too slow to follow. “Why ‘m I…” He squeezed his eyes shut and shook his head. He glared up at the researcher. “Just get it over with or lemme go, why are y—”
The blue light flicked on. Every part of him surrendered to the misty glow, eyes rolling upwards to give the halo a blank stare. “It feels good to obey,” the researcher said, following the same compliance protocols. “Resistance fades; obedience remains.”
Next time the light turned off, he barely woke up. He stayed slumped against the padded chair, dazed and confused, blinking owlishly at the dark ring hovering above him. “What ‘re you… doing…”
“Subject 3B-167. Follow my finger closely.” His gaze tracked a slow horizontal. Up and down. “Very good. Noted for compliance.”
“Wha’?” He weakly pulled at the restraints. “Mm not, n’no…”
A twilight haze of blue. His gaze roamed along the arc of it, enraptured and lost, paralyzed all over by the usual mantras. A subject’s identity is in their obedience. Obedience is his natural state. He exists to obey. Obey, obey, obey.
Eventually, the light dimmed all the way and the subject was still a drooling mess. He didn’t snap out of it, not even with enough prodding and pushing. He just mumbled out an incoherent string of sound and stared at the empty ring.
“From here we would move on to hypnotic conditioning. I find the subjects tend to be incredibly receptive in this state,” the researcher said, standing proudly next to her mindless subject like he was some pretty prototype. “My next phase will involve refining the protocols to ensure long-term compliance without the need for constant reinforcement. It will take time, but we're on a good track."
The microphone from the other side of the glass finally sparked to life, and it was with the greatest approval to be had from The Director: “Keep going. I want to see more.”
#whump#augusnippets#augusnippets day 16#medical whump#lab rat#mind conditioning#whump prompt#tw captivity#mind control#brainwashing#dehumanization
91 notes
·
View notes
Text
as medium & high support needs & level 2&3 autistic people get slight more recognition on this little corner of tumblr, more people joining. n, overwhelming majority see is, people who lost skills/regressed n became this way later in life, or “alway told/thought am low support needs but now realizing may be medium”, rather than more even split between that & people who born this way / people who now is this way because gained skills.
n encourage all, include those who in first category, to think about why. why it this way. why people born this way not more represented (& definitely not because there less of them - actually those who lost enough skills later in life enough to be clinically significant currently seen as rarer ones). how two group differs to create this difference.
because. as someone who went through giant regression later in life n now nonverbal (meaning fully) & high support needs & border between level 2&3 (& all of that in medical records) — as you can see, while have many visibly communication struggles, have many cognitive struggles, have many behavioral & daily life & communication support needs, & yes, many these need for support still not met… can communicate via words, have functional communication that way, have enough cognitive ability, enough to be here online.
think that, if born this way, so still having the potential to have all these skills enough to communicate via words online…. not sure will ever get here.
as in. from birth year forward, in birth country, with how knowledge about moderate & severe autism, how many therapy available (aka none), how education given (aka none), how disability support available (aka also none)… not sure will get the therapy to support functional communication (& other stuff), education to support able write think this way, etc
along with other important things, like infantilized so not given dignity of risk so not allowed be on social media
so, even if assume have potential to get to same point. don’t think will be given enough to ever meet this potential & be equal as now.
don’t know if make sense at all
keep going back to, how in past said, in past & sometimes even now (depend on location, etc), autism diagnosis did mean doom, not because autism bad, but because get diagnosed with autism then meant many closed doors, less because inherent ability but more so from societal prejudice & ableism.
especially for infants & young children (who at age even nondisabled not yet able advocate for themselves). especially for those diagnosed severe/level 3/whatever language clinicians use). for those who both of those, many times mean more closed doors than open ones.
n becoming this way later in life, meant that able benefit from more open doors than would have been closed if born this way. even if not have all the support right now.
90 notes
·
View notes
Text
The Boring CBT Final for the Fun CBT King - By Lexi Moon aka CashAndPrizes
Okay! People asked and I fought tumblr to deliver!
Hi, I'm CashAndPrizes also known as Lexi Moon, and I am a doctoral student studying clinical psychology. I wrote about Redacted (specifically Lasko) for my final for Cognitive Behavioral Therapies. Here's the paper.
Shout out to my beloved friends in the WhoreHome and W.A.R. for keeping me going through this paper. I love you dearly.
Words of warning:
I am a clinician in training. I am still being supervised. I have not been graded on this final yet. (I'll update when I get it!) And I am definitely not an expert. Take everything here with a grain of salt.
I am not a licensed therapist but even if I was I am not your therapist. I'm play acting as Lasko's therapist for a class. Take everything here with a grain of salt. If you read any of this and think "It's a bit loud in here" do not assume this is absolutely you. If you have the means, please try finding your own mental health professionals and if you don't, please do a lot of research on these subjects. Don't use this as a diagnosis please, I'm just a guy.
I filled in a lot of Lasko's backstory based on my experiences with patients and my beloved Lasko kinnies who were instrumental to the writing of this paper. (I won't tag you and call you out, but you know who you are an I love you.) Your headcanons might be different - that's cool. I'm not claiming canon over most of this - but I did use the transcripts and timeline very heavily.
If you don't like the idea of pansexual, transgender, Indo-Caribbean/Trinidadian child of immigrants Lasko - pookie this might not be for you. If that sounds like your jam though - come on in, the water's fine.
Without further ado. Ladies and Gentlemen, this is Mambo Number Five. Here's Lasky. I can, in fact, fix him.
Case Summary
This case conceptualization addresses the hypothetical course of treatment for Lasko Moore, a character in a modern-fantasy audio narrative. Lasko Moore presented to treatment as a 30-year-old pansexual and transgender Indo-Caribbean man working as an administrator and adjunct professor at Dahlia Academy for Magical Novices for persistent anxiety symptoms. Upon intake, Lasko reported experiencing near constant racing thoughts that he was unable to “turn off”, panic attacks, and increased anxiety about social interactions at his work. He described spending a significant amount of mental energy preparing for and reviewing social interactions with colleagues such that he often avoids his colleagues in an effort to minimize his anxiety. Lasko reported that the anticipation around coworker interactions (meetings, socials, etc.) becomes quickly overwhelming as he becomes preoccupied with what he will say and do in an effort to try and minimize his tendency to become hyperverbal and overshare information as well as stuttering. He described this process as starting with embarrassment over previous interactions which leads to critical thoughts like “I shouldn’t be so anxious” which leads to rehearsal of potential outcomes of interactions. However, in the moment of social interactions he becomes so anxious as there “aren’t any objectives [or] any specific roles” to the conversations that he “word vomits” and becomes tangential and overshares until he runs out of breath and stops himself from talking due to his own critical thoughts and begins to isolate himself.
Lasko was initially diagnosed with Panic Disorder (F41.0) and Generalized Anxiety Disorder (F41.1) to capture his persistent anxious state with occasional intense bouts of extreme anxiety and panic. An initial long-term goal was collaboratively set as improving his coping strategies and tolerance of anxious affect to better network and create relationships. As this was Lasko’s first time utilizing mental health services, treatment began with inhibitory learning in combination with Acceptance and Commitment Therapy in order to facilitate willingness to experience interoceptive cues and extinguish avoidance due to fear of negative consequences. This was able to reduce his panic attacks as he felt more able to tolerate overwhelming anxious affect. Despite his clear engagement with treatment through attendance, homework, and skills practice, Lasko continued to struggle with critical thoughts and avoidance of coworkers which he identified as a major barrier to his continued professional development and potential non-academic relationships. Through collaborative exploration, a persistent early maladaptive schema relating to his critical thoughts emerged and treatment shifted to a goal of starting dialogue between schema modes to facilitate the use of coping strategies to build interpersonal effectiveness. Lasko was born as the human-born child of Trinidadian immigrants who moved the southern California in the early 1990s due to political unrest. From an early age Lasko faced high academic expectations from his parents who desired upward mobility for their child and a “piece of the American Dream.” His mother was emotionally labile to the point of explosive outbursts where his father was more passive and spent significant energy working and caring for his wife. This experience started Lasko’s early maladaptive schema regarding rigid standards with no support, which only became worse when Lasko’s elemental powers began developing at thirteen and his parents expected perfect control (and perfect suppression) of his powers with no training and a highly critical environment. This led to Lasko isolating himself at home as much as possible to hide his lack of control but left him with an environment that created a positive feedback loop where his lack of control led to increased yelling and criticism which led to worsening outbursts of his powers. This culminated in a final traumatic event when Lasko was seventeen and lost control of his powers, leading to his mother “calling [him] everything she could think of […] she was so loud and I just wanted her to stop” to the point that Lasko accidentally sucked all of the air out of the room and almost suffocated his mother. Though Lasko was able to find support with the Department of Uniform Magical Practices and become emancipated from his parents, these experiences developed a maladaptive pattern of hypercritical thinking about himself, especially in the context of social relationships.
Research
Avelino Cardoso et al. (2023) pose potential ways to modify and apply Schema Therapy to sexual and gender minorities. This work focuses on understanding how of harmful implicit and explicit messages about gender and sexuality contribute to early maladaptive schemas based on consideration of the minority stress model, and how Schema Therapy interventions can be applied to sexual and gender minorities. One area of particular relevance from this article is the conceptualization of an inner critic mode that specifically represents stereotypes and prejudice that are naturalized by society. When applying these principles to the case of Lasko, the environment of his childhood can be understood as an essential aspect of the treatment. Though Lasko did not present to treatment looking to discuss the impact of his pansexuality and transgender identity, potentially because of the clinician’s own advertised identities, the impacts of systemic oppression against sexual and gender minorities can be woven into treatment for his hypercritical early maladaptive schema. Based on the suggestions of Avelino Cardoso et al. (2023), it may be worth examining his secondary schemas around shame and social isolation as also being shaped by his experience as a gender and sexual minority and how that may contribute to his predominant hypercritical schema.
A major concern for this section of the paper is the lack of research modifying second and third wave cognitive behavioral therapies for sexual and gender minorities. Results for Acceptance and Commitment Therapy with LGBTQ+ individuals only revealed one article about group therapy and a study proposal; results for Schema Therapy with LGBTQ+ individuals only provided Avelino Cardoso et al.’s (2023) theoretical essay. There does not appear to be much research and what research exists is extremely limited with no randomized control trials. This makes it clear that evaluating the efficacy of treatment for sexual and gender minorities is not a priority, which leads to a major critique of Avelino Cardoso et al.’s work. Though the article is useful for considering how to address systemic change in the room, it seems to attribute lived experiences of sexual and gender minorities to a schema rather than ongoing threats in a world where hate crimes and discrimination against LGBTQ+ individuals is on the rise. The abandonment and violence that these individuals may face is not imagined and it can be seen in the lack of interest in research.
ADDRESSING Model
When considering the case of Lasko, it is important to remember that psychology does not develop in the vacuum of individual experiences – psychology develops based on the global environment, which includes the social, political, economic, and cultural contexts as well as individual context. Utilizing Hays (2022) ADDRESSING Model, the impact of Lasko’s intersecting identities can be understood to have a major impact on his current symptom presentation and the development of early maladaptive schemas and schema modes. Lasko was born to first generation immigrants from Trinidad with strong Indo-Caribbean and Catholic roots – and he was assigned female sex at birth. Using a systems-focused lens, Lasko’s current symptoms can also be understood within the larger context of living in a world where several aspects of his identity are under intense scrutiny and political debate. As a child of immigrants and as someone Indo-Caribbean, Lasko likely faced explicit and implicit messages about his intellectual capabilities, his body, and his work ethic. While Lasko directly experienced his mother as extremely critical and never satisfied with his performance, it is just as likely that he received messages as a child about needing to work harder than many of his same aged peers for equal amounts of recognition based on his racial, ethnic, and sex assigned at birth. There is also the element of the disconnect between his sex assigned at birth and his gender presentation, and the messages he received about being transgender from his Catholic, Trinidadian immigrant parents as well as the American culture – which were likely discouraging at best and hostile at worst.
Keeping all of this in mind, Lasko’s hypercritical, social isolated, and emotional deprived schemas can be understood as also being a direct result of the intersection of his identities – and this does not even cover the added layer of being an empowered human-born. In a variety of ways, Lasko has had very different experiences than his peers by virtue of being a transgender, pansexual, child of unempowered human immigrants. When Lasko describes feeling different from the people around him growing up and when he entered the empowered world, this is a real experience based on the multiple identity intersections – it is not hard to believe that he did not have many friends or family members between the late 1990s and late 2000s that had similar experiences to him. This left him with the acute sense that he was fundamentally different and needed to work much harder than those around him, and also that to get validation he needed to sacrifice his needs (or identities) for those of others.
Methodology
The initial treatment approach for Lasko was a combination of Acceptance and Commitment Therapy and inhibitory learning with interoceptive and in vivo exposure, which was successful in decreasing his panic symptoms but not generalized anxiety symptoms. Lasko reported that he experienced sudden panic attacks that seemed random and included symptoms such as accelerated heart rate, tightness in his chest, hyperventilation, feeling that he would lose control, sweaty palms, and loss of control over his magic. At the time of treatment, he reported that he had been having at least one panic attack every other month since he was a teenager and that they would occur more frequently when he was in periods of intense stress. After exploration, Lasko was able to determine that he often had panic attacks related when he spends time ruminating in anticipation of social interactions. Lasko explained that during panic attacks he tends to seek quiet, dark places to hide and “ride out” the panic attack and that he has thoughts like “I’m going to mess this up” or “I can’t do this.”
Treatment started with Acceptance and Commitment Therapy and inhibitory learning as an evidence-based approach for treating panic attacks and generalized anxiety to address his symptoms and reduce further panic attacks as well as his anxious thought patterns (Barlow, 2021; Ruiz et al, 2020). Acceptance and Commitment Therapy (ACT) is a therapeutic practice that focuses on improving psychological flexibility and understanding the function of behavioral patterns (Gordon & Borushok, 2017). Much of early treatment with Lasko consisted of psychoeducation around the therapeutic process, behavioral therapy, and mindfulness. He took easily to ACT and benefited from understanding how avoiding social interactions was negatively reinforced by decreasing his anxiety while keeping him from creating connection. Inhibitory learning through multiple types of exposure (in-vivo and interoceptive) was able to make him more comfortable with feeling panicked, effectively reducing his panic attacks (Ramnero & Törneke, 2008). However, his baseline anxious affect and negative thoughts did not ease despite the use of ACT, so treatment shifted towards understanding the function of his persistent negative thoughts through Schema Therapy.
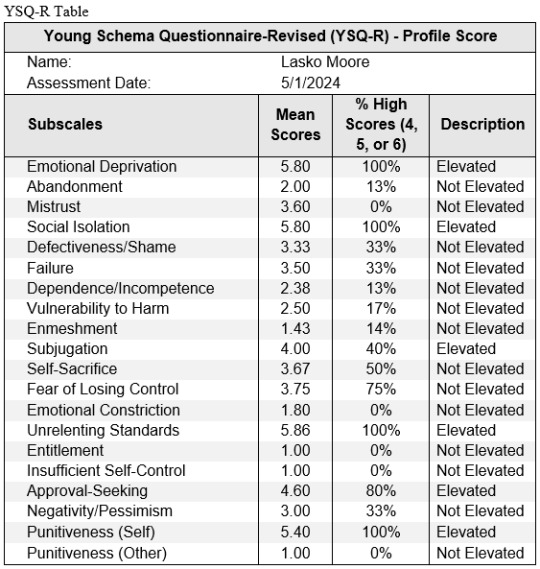
Lasko’s symptom presentation after several sessions of ACT and inhibitory learning was a persistent anxious affect and worry (especially around social situations) that felt uncontrollable and critical ruminative thoughts. As it seemed treatment had plateaued, the content of sessions moved towards a deeper understanding of his critical thoughts based on an indication of deeply held early maladaptive schemas. Barlow defines early maladaptive schemas as persistent behavioral, cognitive, and relational themes developed in early childhood that are reinforced throughout lifetime and that cause significant disruption and dysfunction (2021). Schemas are often viewed as truths about the self and others and are difficult to challenge because of the deep affective component and lifetime of reinforcement (Barlow, 2021). Movement towards schema work started with psychoeducation which involved discussing how schemas are reinforced through modeling (in this case by his mother’s critical comments about his performance) and how people can often act in ways that reconfirm schemas into adulthood. Lasko then completed the Young Schema Questionnaire - Revised and received high scores on schemas related to emotional deprivation, social isolation, and unrelenting standards (Rijkeboer, 2015). During the debriefing and explanation of the results, Lasko reported that when he was completing the questionnaire he felt “really seen” in a way that was uncomfortable but also validating to his experiences in childhood and as a queer person of color living in America.
The topic of sessions then moved towards further psychoeducation about the process of schema work, including delving into his schemas and determining schema modes with the goal of improving his understanding of schemas and working towards healthier integration of modes and coping strategies (Barlow, 2021). Lasko was committed to treatment but apprehensive about “what would come up,” speaking to his concerns about dredging up uncomfortable memories and feelings. In response, he was encouraged to revisit his understanding of ACT and his core values as a reminder of why he wanted to continue treatment and work through feelings of discomfort and grief. The next session started proper schema work, starting with Lasko explaining his understanding of schemas and how they were currently impacting him. He aptly summarized that his childhood experience of feeling intense pressure to do well academically and conform to socially and religiously defined gender roles left him feeling isolated from his peers and that he always needed to work harder and do more, while also feeling as though he had no support or anyone who truly understood him – this led to the development of schemas related to emotional unrelenting standards, social isolation, and emotional deprivation.
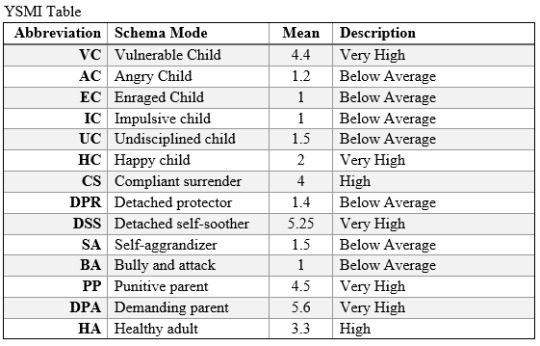
The first step of schema work was to identify schema modes as recommended by Barlow (2021). Lasko completed the Young Schema Mode Inventory (YSMI) as homework (along with his regular thought and feeling records) and scored highly in the following modes: vulnerable child, compliant surrenderer, detached self-soother, punitive parent, and demanding parent (Lobbestael, 2015). With this in mind, the next session started with reviewing his thought and emotion records as a baseline for identifying schema modes. Lasko was able to sort different thoughts and feelings into categories that broadly resembled the categories for child modes, coping modes, and parent modes, but he struggled to come up with names for them. He eventually decided on “Young Lasko” to describe his vulnerable child mode, “The Doormat” to describe his compliant surrenderer mode, and “The Critic” to describe his punitive and demanding parent modes with suggestions from the therapist based on his results on the YSMI. Lasko was overwhelmed with sadness and fear during this session, describing how hard it was to name and admit these schemas out loud and how scared and vulnerable he felt. He reported a heavy weight on his chest and how badly he wanted to hide from the therapist and his own internal experience, and his wavering control over his powers was evident by the rustling of papers in the room. The second half of the session was dedicated to using ACT and mindfulness techniques to sit with the almost intolerable affect without judgement. The session closed with a discussion of how he could focus on his value of self-care after the session and he decided that he had plans to meet with his friend group the next day and try to talk with them about his feelings as a form of self-care and confirming his acceptance in his friend group.
The following session he reported that his conversation with his friend group had gone “really well, better than [he] expected” and the session started by discussing how this did not conform to his expectations as a way to integrate the initial phase of inhibitory learning into the present. The conversation then moved to re-introducing the names for his schema modes and utilizing a combination of mindfulness skills and reaffirmation of his core values to give a voice to those modes and their needs by recommendation of Barlow (2021). Lasko explored that “Little Lasko” felt “awful, awful all the time” and was a sad little boy trapped in a girl’s body who “[held] onto all the bad stuff” including feelings of being completely isolated from others and deep sadness. Lasko further explored that “The Doormat” was a representation of how he had worked so hard in school and at home to make everyone else happy and that by avoiding his own needs and wants (for self-expression, acceptance, nurturance, joy, etc.) he thought he would get his needs met. At this point in treatment, discussing “The Critic” was still too affectively laden so discussion started with the first two with the goal of working up to “The Critic.” Based on guidelines from Barlow (2021), the next few sessions focused on identifying the ways these schemas had developed within his childhood and how they had once been adaptive and essential for his survival. Lasko’s homework between these sessions was to read handouts given by the therapist about schema modes and the ways they are internalized throughout childhood. Lasko was also willing to try journaling once a week from the perspective of either “Little Lasko” or “The Doormat” to better understand how integral they had been to his survival.
Session Description
This transcript describes the first part of the schema work, where Lasko began to identify and label schemas with prompting from the therapist. Rather than just using the terms from the YSMI, Lasko was encouraged to create his own meaning to better represent his own understanding of the schema modes based on evidence-based methods from Barlow (2021). The goal of this session was to help Lasko observe the schema modes based on his thought and feeling record from the previous week and start thinking of the modes as parts of him that were observable separate from himself.
Therapist: You’ve summed up schemas and how they work, and I don’t even have anything else to add.
Lasko: I really, um, want to make sure you know I’m serious about this. I want to get better, I want to be better.
Therapist: It feels like it’s really important for you to feel like I know how hard you’re working right now.
Lasko: Yeah, well… Yeah, I don’t want you to think I’m not doing the work.
Therapist: It’s interesting because you’re the one paying for sessions, you know? While I’m glad that we are working together towards your goals, what you get out of this is really up to you. Can we talk more about how you want to make sure I know you’re working hard? I think that’s really tied to this whole schema thing I’m trying to sell you on.
Lasko: I’m already sold on it!
Therapist: [Hm]
Lasko: … That’s… that’s what you mean, isn’t it?
Therapist: [Affirmative hm]
Lasko: Fuck – sorry – shit! I um… I feel like I need to prove to you that I’m listening and trying really hard.
Therapist: What will happen if I think you aren’t trying?
Lasko: Well, you won’t take me seriously – at all. You’ll think I’m wasting your time and that I should – I need to be doing more and taking it seriously.
Therapist: And how would I be feeling with you?
Lasko: Angry, because I’m wasting your time – but I’m not, or I don’t want to. I don’t want to waste your time, you have so many other patients you could be seeing and if I’m not doing what I should be doing then I’m just- I’m taking up space someone else could be using and they probably need it more than me. I mean, I’m fine you know, I’m anxious but I can survive, right? There’re people out there who need your time more than me and I’m wasting it – or I would be. I’m not – I don’t think I’m wasting your time right now except I keep rambling.
Therapist: There’s a through-line in there that I want to pull. You feel like you need to do what I expect you to do, right?
Lasko: Yeah, I mean you’re the therapist. You’re the expert with – all the experience and degrees. So yeah, I should be doing what you expect.
Therapist: It sounds like there’s some part of you that feels like you need to be doing what I say you should do, even if you don’t want to or have something else to say – like your “rambling” – and that if you don’t, you’re wasting my time. Does that feel right?
Lasko: I want to do this, I do. But um, yeah. That feels right.
Therapist: And you do what I say you should do because if you don’t…?
Lasko: Well I’m wasting your time. And then you’ll – I mean you probably won’t, you’re a really nice person and you’re so helpful but I just… I have this thought that you’ll get mad at me.
Therapist: I would be mad at you. What would I do if I was mad at you?
Lasko: You would um… Well I know you wouldn’t, because you just – you’re not like that but like my mom would start screaming at me. She would just… she would just yell and tell me that I was wasting their money because I wasn’t doing well enough at the school they paid for me to go to you know? Or I messed up the nice clothes they paid for. Or I just – anything like that really, I was wasting money and time and I was a waste of space and… Fuck – sorry – wait, um. This is hard to talk about and I don’t want to cry.
Therapist: This is really hard, I’m really putting you through it already today, aren’t I?
Lasko: [Affirmative hm]
Therapist: I want to take what you just said and kind of summarize, kind of explain, is that okay? So, it sounds like you have these thoughts that you aren’t trying hard enough – or at least that I don’t think you’re trying hard enough, right? And these thoughts serve to make sure that you show me how hard you’re working so that I believe you, because if I don’t, I might think you’re wasting my time and become angry and yell at you.
Lasko: That’s a really succinct way to put it, but yeah.
Therapist: So what I think is happening here, is that there’s a part of you that is so terrified that I will become angry and yell at you and make you feel just awful about yourself. And to deal with that, there’s another part of you that works really hard to try and anticipate and meet my needs so I won’t become angry with you. And then there’s also this third part of you, this part that is so critical and reminds you of how scary I could become if I got angry with you and kind of beats me to the punch by being mean first. And all three of these parts were working together in those last few minutes.
Lasko: Wow… yeah, that um… you hit the nail right on the head. That feels right. It’s not – um, it’s not really great for me, though.
Therapist: What I’d like to do is start by giving a voice to these parts of you, just letting them speak. Do you think we could do that?
Lasko: That… That sounds really awful. But, yeah we can… we can do that.
Therapist: And here I am, asking you to do these terrible things you don’t want to do and you’re doing them with me anyway.
Lasko: That’s the um.. that part of me that tries to meet your needs, right? That’s what you said?
Therapist: I think so. I really want to hear more from that part of you.
At this point in the transcript, the therapist was using a combination of techniques to try and get closer to the schemas that were indicated in Lasko’s dialogue. There was a mix of rephrasing/restating what Lasko had said with the dual purpose of making sure the therapist understood and phrasing things in a way that would lead to more dialogue about schemas. The therapist in this section also started outlining the core schema modes operating at the moment in broad terms to gauge Lasko’s ability to tolerate and explore them further with the intention of eventually moving towards labeling schema modes. In this section, it is becoming clear that Lasko’s persistent anxiety about the therapy (proving he is engaged enough) is a result of active schema modes that attempt to anticipate and meet the therapist’s needs to prevent criticism and anger on the part of the therapist. This insight from the conversation can be broadened to potentially explain the utility of Lasko’s critical thoughts and anxiety around social interactions – he spends so much time preparing and planning for these interactions to try and anticipate and meet the needs of others to prevent criticism and anger from his peers, the mere idea of which causes deep feelings of fear and sadness, by criticizing himself first.
Therapist: I think so. I really want to hear more from that part of you.
Lasko: I mean – geez, what should I say?
Therapist: Maybe we could start with what that feels like…?
Lasko: It feels like I’m always guessing, trying to figure it out. I feel like I have to do everything right, try harder, do more…I feel like I always need to be doing more, doing it better.
Therapist: What emotions does this part of you have?
Lasko: Um, I don’t – I don’t know.
Therapist: Do you think I should bring out your old friend the feelings wheel?
Lasko: Yeah that might – might help. You know how much I love the wheel. Yeah – um, I guess I feel… inadequate? Maybe…
Therapist: Can I suggest something that I’m sensing in you?
Lasko: Please, you’re way better at this than me.
Therapist: I’m wondering if this part of you feels desperate.
Lasko: Yes, desperate.
Therapist: Desperate… it feels like there’s more to that. Desperate for what, do you think?
Lasko: Desperate… desperate to please – desperate to get it right.
Therapist: Wow… desperate to please feels really powerful. I see you rubbing your chest right now, what are you feeling?
Lasko: It’s like… my chest feels tight – a little like when I have panic attacks.
Therapist: That connection feels really important. What do you make of that?
Lasko: I feel – I’ve felt desperate when I’ve had panic attacks before. Like desperate for air, which is just – it’s funny as an air elemental you know, well not funny-funny, but it’s just – anyway, it’s like desperate for air but it’s also like I’m desperate for… I don’t know how to phrase it…? For it to stop, yeah, but also like I… I want to do things right when I talk to people but I always fuck it up – sorry – wait, don’t apologize Lasko. Sorry, I – sorry – fuck. I just- I want to have better interactions with people! I want things to go better and to communicate better so people like me and – I don’t know.
Therapist: So people like you… do you think that’s what this part of you wants?
Lasko: Yes – so badly… So badly it hurts.
Therapist: It hurts in your chest, right there?
Lasko: Yeah… it’s tight and heavy and then I start crying because I’m just – I’m a mess.
Therapist: You’re feeling so much right now, and you’re doing it because I said we should.
Lasko: Well… yeah, it’s um – it sucks but you know better than me.
Therapist: That seems to be a thought you have a lot, we’ve talked about it before on your thought and emotion records – and I think it’s really tied to this part of you.
Lasko: I mean… maybe, yeah.
Therapist: What do you think you could name this part? How do you think we could refer to it?
Lasko: Like a name? What kind of name…?
Therapist: It’s really up to you, I think it’ll be more helpful to use whatever you think is the best way to describe it rather than my clinical-ese jargon.
Lasko: I don’t… I don’t really know. I’m not good at this kind of thing. Can’t you – you can just name it, right?
Therapist: I could, but I feel like if I name it we’re staying in this pattern where you just acquiesce to my demands.
Lasko: Which is like – the whole point of this, yeah.
Therapist: Exactly. What feels hard about thinking of a name?
Lasko: I don’t – I don’t want to pick some stupid name that I have to use, and you’ll think “wow that was a really stupid name choice, I should have picked it.”
Therapist: [Hm]
Lasko: Yeah, you don’t have to say anything, I hear it. Also, I just… naming it feels so real, you know? Then it’s a real thing.
Therapist: And there’s something about it being “a real thing” then?
Lasko: Then I’d… I’d have to talk about – acknowledging all of it – that feels really awful. I feel like I can’t breathe right now.
Therapist: I can feel the air becoming thin too. Why don’t we take a few moments and just notice how you’re feeling and breathe through it?
This section of the transcript starts to explore and move towards labeling the schema mode of the Compliant Surrenderer. This mode attempts to anticipate and meet the needs of his hypercritical Punitive and Demanding Parent mode to protect his Vulnerable Child mode, which becomes clear in the transcript as he verbalizes that this part of himself is desperate to do well (whatever that may look like) so that others will like him. Just sitting with this part of himself causes Lasko almost intolerable feelings of desperation and panic, likely due to his fear of his Punitive and Demanding Parent mode as well as a fear of criticism and rejection from the therapist.
Closing Thoughts
I really enjoyed this case and this paper. While I didn't choose a current patient, I feel that I got a lot out of this assignment. It was really interesting to think formally about a character and work through a treatment plan and focus on a specific element of treatment. I managed to pick a case where I got to implement schema therapy, which is one of the forms of CBT that I find most interesting in addition to ACT. Despite this being a fictional character, I have certainly had previous patients who have similar struggles – and I also felt that I was able to use the media (and my previous experience to fill in gaps) to make the most of this assignment for my learning.
As I was working on this case, it occurred to me that though I felt like I was able to portray this character as accurately as possible I felt like so much was missing or unaccounted for. Because I was working from a CBT rather than psychodynamic lens, I felt like there were clear points where I would have ideally worked more relationally to address resistance or spoken more about the therapeutic relationship. There are always a million different things you could pick out of a patient’s response to respond to, and it was challenging to focus more on the schemas rather than talk about the relationship. I also felt like because of the limits of this paper, I did not have enough space to talk in the methodology or transcript session about how I felt his identities played a part in the development of his schemas. In this example, it was very clear to me that Lasko’s experiences of his parents were only part of the equation as development does not exist in a vacuum – there is a reality that his identity as a pansexual, transgender, Indo-Caribbean, second-generation immigrant and his experiences of xenophobia, racism, heterosexism, and transphobia would have also impacted his feelings of isolation/difference from others and internalized pressure to present and perform well. I also think that this would have been something I discussed in subsequent sessions as I believe this is another function of his schemas – to protect and prepare himself from his experiences of a hostile, sometimes violent world.
References
Avelino Cardoso, B. L., Paim, K., Figueiredo Catelan, R., & Liebross, E. H. (2023). Minority stress and the inner critic/oppressive sociocultural schema mode among sexual and gender minorities. Current Psychology, 42(23), 19991–19999. https://doi.org/10.1007/s12144-022-03086-y
Barlow, D. H. (2021). Clinical handbook of psychological disorders: a step-by-step treatment manual. Sixth edition. New York, The Guilford Press.
Hays, P. A. (2022). Addressing Cultural Complexities in Counseling and Clinical Practice: An Intersectional Approach. Fourth edition. Washington DC: American Psychological Association.
Lobbestael, J. (2015). Validation of the Schema Mode Inventory. In M. van Vreeswijk, J. Broersen, & M. Nadort (Eds.), The Wiley‐Blackwell Handbook of Schema Therapy: Theory, Research, and Practice (pp. 541–552). Wiley-Blackwell.
Ramnero, J., & Törneke, N. (2008). ABCs of human behavior: Behavioral principles for the practicing clinician. Oakland, CA: New Harbinger & Reno, NV: Context Press.
Rijkeboer, Marleen (2015). Validation of the Young Schema Questionnaire. In M. van Vreeswijk, J. Broersen, & M. Nadort (Eds.), The Wiley‐Blackwell Handbook of Schema Therapy: Theory, Research, and Practice (pp. 531-540). Wiley-Blackwell.
Ruiz, F. J., Luciano, C., Flórez, C. L., Suárez-Falcón, J. C., & Cardona-Betancourt, V. (2020). A multiple-baseline evaluation of acceptance and commitment therapy focused on repetitive negative thinking for comorbid generalized anxiety disorder and depression. Frontiers in Psychology, 11. https://doi.org/10.3389/fpsyg.2020.00356
Home. (n.d.). Redacted Audio. Retrieved May 5, 2024, from https://redacted-audio.com/
Appendix
Character and Media Primer
Redacted Audio is an urban-fantasy audio narrative on YouTube that centers around the fictional city of Dahlia in southern California and its inhabitants (“Home”, n.d.). In this urban-fantasy world, people are separated into four categories: unempowered humans; empowered humans, which can be further broken down into elementals and energetics (people with control over the four elements, gravity, sound waves, magnetics, psychokinesis, telepathy, seers, or a jack of all trades) and shifters (e.g.: werewolves); vampires, who are turned unempowered or empowered humans that feed on blood to survive, have superhuman speed and senses, and cannot go out in the sun; and demons, beings of pure magic that are not necessarily evil or good. The character I have chosen is an empowered human who was born to unempowered human parents – a human-born – which is a rare kind of person who often faces discrimination and barriers to learning how to control their magic. Lasko is an administrator and adjunct faculty member at the Dahlia Academy of Magical Novices, which is essentially magical community college where students (of any age) can learn mastery over either their specialty or all aspects of empowered human magic. The Dahlia Academy of Magical Novices operates as a school under the larger Department of Uniform Magical Practices, which oversees magical practices, ethics, and maintains the covert status of magic. Lasko specifically has natural control over the element of air, giving him an increased lung capacity and control over air (making wind currents, taking air out of the room, making tornados, etc. – think air benders in Avatar: The Last Airbender if you are familiar), but chose to complete his full certification at The Dahlia Academy of Magical Novices to have a better understanding of all types of magic. He teaches an introductory class on magic for incoming students as a way to provide a less discriminatory experience for other human born students.
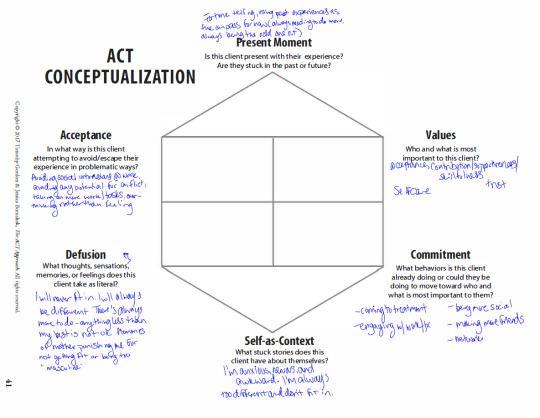
ACT Hexaflex
YSQ-R Table
YSMI Table
That's all, folks!
58 notes
·
View notes
Text
Until 1999 comes out and reveals the lore my personal headcanon/fanon idea is that the Hex used to be a pretty tightnit and functional squad of agents but the encroaching helminth technocyte infection is slowly driving them “mad” (ie just throwing their brain chemistries off and worsening pre-existing issues and being forced to suddenly go cold turkey on your adderal because your cool machine body is now immune to conventional drugs) so it’s manifesting as them all having unusually short fuses with each other and bickering and increasingly resorting to coping mechanisms for their worsening neuroses (Arthur is isolating himself, Amir is dopamine seeking, Aoi is incongruently faking it till she makes it, Leticia is increasingly prickly, Quincy’s developing something of a defensive superiority complex, and Eleanor is invading peoples’ minds and privacies and keeping obsessive tabs on her peers). Basically everyone’s on the verge of a bad nervous breakdown (which could be used as a metaphor for “losing their humanity” or something. Like really examine how there’s this ableist connection between having psychological disorders/disabilities and personhood (lack of it)? But doing so via Dark Sector Dating Sim where everyone’s a tragic werewolf but instead of turning into a wolf they’re turning into superpowered space ninja mechsuits. )
Which is to say that absolutely very little of this is strongly supported by the demo but I’ve been having a lot of fun thinking about it because I think one of the most entertaining ways to do a character study is to see how they crack under pressure/distress/trauma and cope with it. And the Hex are in that perfect intersection of being characters that are deliberately written to be appealing in some way (for the folks who wish to go the dating sim route) but also have some interpersonal conflict. Maybe part of the plot of 1999 involves the drifter reconnecting them or helping em manage their emotional issues (see inside an ugly broken thing and take its pain away or whatever). Drifter’s had some personal experience with cognitive behavior therapy or emotional regulation skills via learning to master and escape the spirals of Duviri, they might be able to wrestle the Hex into a group therapy session. More likely involving void nonsense. I could just be projecting my own personal issues onto these characters but it’s fun.
All of this is just baseless musings, and I very well could be pulling a lot of nonsense out of thin air- I’ve definitely confused warframe canon with my own assumptions or imaginings to fill in the gaps in the story myself. But anyways.
31 notes
·
View notes
Text
my girlfriend: i think you have ocd
me: yeah probably
my girlfriend: i think more than probably
me: well we dont know for sure
my girlfriend: no i think we know for sure.
me: well JUST because i have been told by MULTIPLE friends who have ocd that i definitely have ocd and JUST because i have been told by my therapist who has ocd that i definitely have ocd, and just because i am going through exposure and response prevention in therapy which a type of cognitive behavioral therapy made specifically to treat ocd, doesnt mean i have ocd. okay? i just have a disorder that makes my thought patterns fucked up. which is definitely not ocd.
my girlfriend: okay. so what is that then.
me: ..... cool guy syndrome.
my girlfriend: no
20 notes
·
View notes
Note
I feel like I’m repeating things that were said but I really felt as though Caiti wasn’t actually ready to share her story. She is in this stage of her trauma where she believes the people who hurt her are evil monsters who acted with the goal of hurting her in mind. I want to draw a comparison to this “aha” moment I had in therapy. I got good marks in school, I was a good student, but no matter my marks— even if I came home with a 90%— my mother would ask “what went wrong?”. It tore me up and because of that it made me think that all she cared about was my grades and that no matter what I did I wasn’t good enough unless I got a perfect 100%. I resented her, I thought her intent was very malicious and it affected my relationship with my mom. I didn’t find out until years later in therapy, when I exploded at my mom about my feelings, that she wasn’t trying to be malicious. She always asked that question because she wanted to gauge if I needed more support in the classroom (I’m audhd and wasn’t diagnosed until I was 12). Of course that doesn’t mean it didn’t hurt me— I wasn’t privy to her intentions for all these years, after all— but that changed how I viewed those moments in my life. To bring this back to Caiti, I think that she needed some extensive cognitive behavioral therapy to process this event and come to terms with it enough that she could speak with George and find closure.
really good insight anon! And i definitely agree caiti is treating this like a still-fresh wound and that's not when you want to go public about any sort of serious accusation like this.
her judgement is clouded by anger and resentment and her perception of the situation and unfortunately, she has surrounded herself with people who validate her hatred for george without anyone stopping her to maybe ask him and see his side of things.
It's also clear she hasn't been to therapy or talked to anyone older than her that can mentor her through these emotions in a constructive and realistic way. Because her perceptions of the world and people right now are deeply concerning and distorted and always assume malicious intent which is so harmful to herself and others.
The only thing I can wish for her is to definitely seek specialized therapy to work through these issues because the way she has internalized/treated/perceived this situation is not normal nor healthy
36 notes
·
View notes
Note
If you could, what would you change in TSAMS? For example, would you add a new character or remove any of the already existing ones, make some ship canon or make two characters who are in relationship in canon to break up, make characters to be different either personality-wise or design-wise, focus on some characters more? (I want to hear you ramble about this please 🙏🙏)
The VERY FIRST THING I WOULD DO
Is put Monty in cognitive behavior therapy. And I mean that so fucking genuinely, that gator has a lot of thinking errors that make him so infuriating, and if I could get him assigned to a therapist that's NOT his girlfriend, that will actually work with him on being mindful and self-awareness and shit I would literally die happy.
My reasoning for this is that it would be so fucking unsatisfying to just "fix him". Personally, I think that would be an insult to what his character is supposed to be, and if Eclipse can get better and more empathetic and more aware of how he affects other people than so can Monty. I don't want to change his personality, I just want his character to be more aware of how big of an asshole he is and actually try to be a better guy. It 100% doesn't even need to be something in the foreground, just knowing that he's speaking to a professional about stuff would be enough.
As far as characters go, I personally don't think it's my place to suggest adding or removing characters. Mostly because I don't think it's necessary. I would push for more random lore for characters that we've met but don't know that well, especially one-off AUs that already exist in canon. We've gotten to see Gaia and Nyx again. Helios is one of the main characters now, and Kronos has been made relevant again, so they definitely remember the other dimensions. I think it would be a nice break from the heavy hard lore of the main universe, while also not being so obvious of filler content that people would throw a fit. It would be a treat for the audience to get to know more about the different canon AUs. I might prod to bring back Solar Flare, just because of the potential in his character (and yes I am biased) but even that's a coin toss because I also feel like he's served his purpose in canon.
I do think clearing up character ambiguity would be important, especially for characters like Jack where it's just so convoluted as to how we're supposed to interpret them. When the VAs say we're supposed to view a character as one thing and then portray them as another it gets really confusing for the audience. It is also really confusing for writers most of the time because they have a character that they aren't in (internal) agreement as to how they want to write them, which leads to a messy character. This is just a general statement about writers, and not specifically TSAMS.
Okay, the shipping question. I wouldn't make any ships canon or non-canon. Yes, that includes Monty/Earth. Yes, I know that I am well known for writing about ships and making AUs about ships, however, that's specifically non-canon and I know it's non-canon and I know that when I write about my silly little ships I am being delusional about characters' compatibility. It is my pride and joy to be unhinged and feral, and that would not change, but there would be a clear divide between professional work for the show and my silly fan AUs. Especially because, as I've addressed in the past, I see TSAMS as another DCA au just like all of my AUs I view as just more DCA aus, even if they are inspired by TSAMS. And considering I have multiple AUs with severely different plot lines and dynamics, I can trust that I would be able to keep them separate, and my personal work wouldn't bleed into my professional work.
Personalities? I like the characters' personalities, and I don't see a reason to change them. After all, it wouldn't make sense from a psychological perspective, which means that it doesn't make sense from a narrative perspective. I genuinely do enjoy the characterization in the show, including character flaws and things that make my skin itch. Yes, this includes Monty. As much as I say "Oh I hate Monty so much", I still really like the characterization, and I'm glad that they're willing to have such an asshole of a character. Moral ambiguity is extremely realistic, and like I've said before, I think Monty meets a lot of the requirements for narcissism or even narcopathy. Which is, again, extremely realistic. People with the kind of moral ambiguity like Monty, who are just as frustrating as Monty, are real. And they exist. And they are infuriating. But because they seem to want to portray Monty as a "good guy" I want him to do the therapy thing as earlier mentioned.
Design-wise, it's no secret that I'm an artist. There are a few designs that are just genuinely eye-sores, but I currently don't have that great of blender skills so I cannot pass judgement in that area when I literally cannot do better ajdsf;lgjafsdl. I can draw up designs, I can do 2D models and sheets and shit, but I'm currently useless when it comes to VRChat models. I want to learn, but that's such a process that I'm trying to find motivation for and I don't even know where I would start. which is part of the issue because it makes it seem even more impossible.
#alex answers#answered ask#thanks for the ask!#tsams#the sun and moon show#sun and moon show#tsbs#long post
22 notes
·
View notes
Text
I want Wandee Goodday to be about mental health.
I've been thinking about Dee mentioning Yak's nightmares and possibly seeking help. I'm not really into Dee trying to force him with an agreement. That kind of stuff doesn't work - mental health treatment is something people choose for themselves. But lots of people take convincing. And we've already seen Dee use leverage to get Yak to take care of himself, so not so surprising that's how they brought it up.
But the conversation finally started to broach what has been missing for me - the story of their mutual losses at young ages and how that can very much impact their fundamental remaining relationships. That kind of loss can be so transformative in how a person relates in significant relationships. It can impact attachment to others, create a pathological fear of loss, increase the level of guilt people carry in their life and even impact their developmental mind set - many people get kind of stuck at certain developmental milestones if they experience trauma at young ages.
(I am saying this as someone who has been trained in cognitive-behavioral trauma therapy as a therapist, but it was quite a while ago and I'm by no means an expert. This is just generalizing. And it definitely doesn't happen to everyone. It just feels like the show might want us to think it is happening for both Dee and Yak.)
The show seems to use these facts about them as short hand for some of their behaviors and choices without doing the work to make it clear and I wish they would delve into them more. I'm worried they are not doing so for drama sake later, but that remains to be seen. It also could be that they are punching above their weight when it comes to their understanding of these issues (yes, pun intended).
This is the first time they are implying that Yak's trauma about his mother's death actually bleeds into other aspects of his life. But that connection is not clearly made. I would have found it interesting if they spent the time to draw a vivid line between Yak's loss of his mother and his fear of loss of Wandee. (as an aside, I would say that would also have helped if they solidified Yak's feelings for Dee earlier so we truly understand the intensity of them. the lack of Yak pov makes it hard to know if his feelings are strong enough to instigate this reaction)
It's also hard to draw this conclusion because Yak is the one who is more willing to react by throwing it away - his fear response seems to be to run. It looks like a "time to get out before I care too much" action with him not acknowledging he already has those feelings. And so then after he breaks it off he feels this intensity of the loss in the form of his jealous feelings about Ter - who is taking Dee away.
He seems to carry a lot of guilt about *something* having to do with his mom's death and equates disappointing Dee with disappointing his mother. But without those details, it leaves us to guess. It isn't clear that Yak is melting down here not just from losing Dee, but over triggering those feelings of loss over his mom again, and possibly the expectation that he will lose everyone.
But that would be the most compelling reason to me.
I think the same actually goes for Dee and his reactions to relationships. We've seen Dee have two trauma flashbacks without any explanation, but it's safe to assume he has his own baggage to deal with. Still, the show is unclear how much it impacts Dee's behavior. Since he has Plakao, a psychiatrist, as his friend it implies that if Dee was truly deeply struggling emotionally, we'd see Kao telling him ad nauseum to go to therapy, not telling him to just take the leap and confess to Yak.
Without Kao saying "Dee, this is more than just indecision"- it seems like the show is saying it isn't a behavior that needs professional help. But if you take it out of the way it is often played for humor, it sure seems like it to me.
If I had a friend who seemed to be struggling so hard with having feelings for someone and had so much fear of those feelings that it was making them a little miserable, and on top of that seemed to not be able to set firm boundaries with someone who had hurt them immensely, so much so that not letting go of that person was more important than how the other person treated them, you bet I'd think they should be talking to someone.
Kao is being played as the voice of reason, but he is very static right now. He's just kinda being the audience stand-in to say GAAAHHH stoppppp. But if I'd had the same conversation with a friend this many times, I'd start to ask - hey, why are you always doing this? why are you always making things complicated?? how is that serving you when you say it isn't?? That is the crux of therapy. Figuring that shit out. It feels like the show wants the character motivation without having to delve into it too seriously.
When Dee says to Yak maybe you should get some help - perhaps he should be putting on the oxygen mask first before he attempts to help anyone else.
And honestly, their mutual trauma being the reason they are having such a fucking hard time working this out would be so, so interesting to me.
I'm just not certain that is what the show wants us to think.
#wandee goodday#wandee goodday meta#I'm still gonna hope this is where they are going and they tighten it up#and not do a hard left into their parents' deaths are related plot#but if I had to bet well...
19 notes
·
View notes
Text
Ghost Soap: Berlin, a club, a dark room
(CW: age gap, unrequited SoapGaz, kink/BDSM, experience gap, eventual Ghoap is 100% consensual BUT definitely could be considered rushed/too fast by the fault of either/both of these dumb, horny men)
Gaz and Soap are traveling during a uni holiday break, bumping through the continent before they have to go back and properly crack down: Kyle’s has a real shot at the Olympic team and Soap’s crammed his upcoming term with more courses than anyone should in an effort to save the dwindling funds from his scholarship. The only reason Soap’s along at all is Kyle’s charity and he tries not to think too much about how much, and exactly why, he’s going to miss him.
They’re in Berlin when they meet up with this goth chick that Soap is desperately trying to impress. She goes along with it and invites them both to the club: It's overwhelming in the way that they are for first timers, which both of them absolutely are. Soap definitely lied about how experienced he was (or deliberately left out how green he is) to impress this girl so naturally the situation once they’re inside goes all tits up in the wrong way.
The girl ends up making out with Gaz in the hallway instead of Soap and he can’t blame her, look at the guy. Or maybe she was hoping she’d get both of them, way she’s looking at him, but that’s definitely too close to those things Soap doesn’t want to think concerning Gaz so he wishes them well, despite the hollow gnawing in his chest and wanders.
He ends up talking to a woman who’s a little older, beautiful and attractive but she laughs and just pats him on the head when he thinks that CBT means Cognitive Behavioral Therapy, he took Intro Psych his first year, and suggests he find someone more his speed to play with.
“Play? I’m not a kid.” He says. He’s been with older women and they’ve liked him and there’s definitely something about this one that he likes.
“Not that kind of play.” She just smiles at him with perfectly painted lips. Then asks him if she can help him find his friends, but he’s a stubborn little idiot with bruised pride so of course he tells her it's fine.
After that he just wants a place to curl up and be the fuck alone and have his sad, confused boy- man, adult man, feelings. But he’s sort of lost and doesn’t know where he’s supposed to go and definitely doesn’t speak enough German to really properly navigate this place that is so much bigger than it looked from the outside.. Naturally ends up where he shouldn’t be.
Enter Ghost, full gear. Mask, of course. Not currently with anyone per se but assisting another pair. Hears Soap before he sees him. Rolls his eyes, figures he should probably get this stupid kid out of here.
Soap’s not expecting the massive man in the skull mask and the whole… outfit… to speak english. Isn’t expecting his knees to turn into pudding when he hears the voice. “I don’t think you’re supposed to be back here, sweetheart.” He stalks forward and Soap can’t look away.
“Why not?” Soap says. It's stupid. But right now he’d do anything to keep those dark, almost black eyes on him. Keep him saying ‘sweetheart’ instead of ‘kid’. “Door wasn’t locked.”
“I think you know why.” Ghost says.
“If I don’t…Would you teach me?””
And the way he bats his eyelashes has to be intentional, has to know what he’s doing. Testing Ghost’s self control. “You definitely don’t know what you’re asking for.”
(Part 1, already working on Part 2!)
Special kudos to @leathfaic for our silly chit chats that lead to this.
53 notes
·
View notes
Note
Henry: 35, 26[Luke]
Julian: 16, 18, 30, 37 & 50
Seb: 18, 20, 29, 37, 28[Henry]
K: 31, 48
I hope it's not too many.
Thank you for sending an ask! Apologies for it taking me a couple days to respond!
Responses are under the cut. Please be advised that there is mention of some heavy topics due to the nature of God Only Forgives.

Henry
26. What Henry would do if stuck in an elevator with Luke Glanton (The Place Beyond the Pines).
I can see them getting into a discussion about tattooing and art styles. Henry would definitely be interested in Luke's tattoos.
35. Their idea of a perfect day.
If he could turn time back, he really would just like to spend a day with his parents again. He would value it so much more than he had before the accident.
Julian
16. Deepest darkest secret they won’t even admit to themselves.
That he maybe he did deserve a normal life. Maybe he did deserve to have a mother that loved him and kept both of her kids safe. Maybe he did deserve to have a brother that didn’t become an abuser himself. Maybe he could even be loved after everything that’s happened to him and that he’s been pressured to do.
18. What they’d go to see a therapist about.
Everything. That man needs SO much cognitive behavioral therapy. Someone who specializes in childhood trauma is a must.
30. Sleeping habits.
He rarely sleeps. He’ll stay awake until he passes out from exhaustion in a chair, on a couch, anywhere but a bed. There are too many bad memories associated with laying on a mattress.
37. What they really think about themselves.
He thinks that he is a coward, that he’s a broken shell of a man. Julian has no hope for himself.
50. A memory they’ve blocked out.
I can imagine that Julian has repressed most of his childhood. Who wouldn’t? At a minimum, his mom was sexually abusing both him and his brother.
Sebastian
18. What they’d go to see a therapist about.
If he were to see a therapist, I think the sessions would largely end up dealing with how he handles interpersonal relationships and the view he has of himself. The sense that I got of him from the movie is that he is afraid of failure both in his career and in his relationships and is prone of molding himself into what other people want at the cost of himself.
20. Scars.
He’s got the usual scars from living. There’s the small, barely significant traces of childhood mishaps on a bicycle on his legs and elbows. On his hands are the shiny burns and finger cuts from time spent in the kitchen.
28. How Sebastian feels about Henry Letham (Stay).
I think that Seb would respect Henry as a fellow artist. They’re both struggling in their own ways.
29. Eating habits.
I think that Seb often forgets to eat. He gets so lost in music that his physical needs fall to the wayside. By the time his fingers go still on the keys of his piano, or the last record finally spins out, hours have gone by and he’s suddenly, acutely aware of his hunger and thirst for something other than jazz.
37. What they really think about themselves.
Sebastian is not as confident as he projects himself as being. I can see him viewing himself as an interloper at times.
K
31. If they had a tumblr what would it look like?
In my heart, K would be mostly a photography reblogger. He would primarily focus on nature and animal photography. He might reblog the occasional bit of poetry as well. It would all be a carefully curated collection of content that made him feel something.
48. Scariest moment of their life.
The day of his inception. Being deposited as a fully formed adult out of a plastic bag would have been terrifying. He knew nothing of the world and yet he was already held in contempt.
#.character ask game#.from you#stay (2005)#henry letham#only god forgives (2013)#julian thompson#la la land (2016)#sebastian wilder#blade runner 2049#officer k#.my thoughts#.my posts
19 notes
·
View notes
Note
I'm curious how "Rand pushing his friends away 2.0" will go. First go round was cause he was scared of hurting them (which is book accurate). The second time in the books is a trauma response so it could go that way in the show too but I just wonder if they don't want to get repetitive of him pushing his friends away. But it is kinda important 🤔 one of the main things is Rand believing his friends aren't in his corner cause of his trauma and self hatred so maybe they lean into that more
yeah it's interesting to ponder! like you say, in the second half of the series it's less "rand pushes his friends away to protect them" and more "rand's friends are geographically separated from him for a long period of time and continue to worry about him despite not being able to see him, whilst rand's deteriorating mental state leads him to incorrectly think his friends have abandoned him and don't care about him anymore" - so if the show went that route in future seasons, i don't think that would feel repetitive with him pushing people away to protect them in s2! and the much stronger EF5 friendship they've established would make it all the more heartbreaking to see rand losing faith in his friends and all the more illustrative of what a bad place he's in (vs. in the books where most readers genuinely believe him when he says they've abandoned him, because the EF5 friendship was relatively lukewarm and the evidence that Everyone Still Cares About Rand was definitely there, but not too strongly or frequently)
it's interesting that rand appears to have actually learned the "pushing people away just makes you and them more vulnerable" lesson after s2 (judging by his Amateur Therapy Session with mat and his apology to egwene), so the approach on that front going forward would have to be either a) rand didn't genuinely learn this after all and is right back to his old tricks in s3, b) rand did genuinely learn it now, but backslides later due to trauma and his deteriorating mental state, or c) the "push people away to protect them" thing is all dealt with in s2 and rand's future isolation will be due to different causes (such as the plot-mandated separation i mentioned above). all 3 seem equally plausible to me!
(but i definitely wouldn't be mad about option C, particularly when thinking about rand's romances. good god the "aaaaahhh i can't be with you i'm soooo dangerous" got SO tiring in the books lmao, like it's not unreasonable for rand to feel that way given the Everything and i'm not unsympathetic towards him, but it just got so tiring! and it made the romances even more difficult to enact than they needed to be & made rand see even less of elayne and aviendha than he already would have due to plot reasons. it also caused a hell of a lot of cognitive dissonance and breaks in rand's own internal logic and characterization, where he's on the one hand going "aaaaahhh i can't be with you i'm soooo dangerous" & refusing to stay in caemlyn with elayne and avi for more than a night lest he draw the forsaken there, and on the other hand he's agreeing to be warder-bonded to everyone & going "come on min, time to bring you into an active warzone" & flaunting his relationship with her in public for all and sundry to see. so the show needs to do SOMETHING here, whether it be preventing his "push them away to protect them" attitude from recurring at all after s2 or making it recur only much later once his bonds & romances are all squared away or saving the bonding until after his epiphany or simply just equalizing his behavior towards each of the 3 so that nobody's getting exceptions to whatever show!rand's internal logic rules end up being.)
32 notes
·
View notes
Text
Carmen Anthony Berzatto, do we have a mental health problem?

You might wanna read this for context first.
I’m gonna get academic boring for a whole minute here, so feel free to just skip right to my point at the bottom.
Whilst Carmy definitely has mommy issues, and even daddy issues as well, plus he has sublimated his sexual attraction for Syd in getting a bullshit star for her as explained and predicted here, which triggered a relapse in his addition (workaholism), as I described and predicted here. That behavior, like any addiction, is in essence a repressed sexual impulse (according to Freud). According to other experts, addiction can, in essence, be considered a neurosis (more based on Jung’s concept, which is more advanced than Freud’s but does integrate it) and all of those concepts are Freudian and thus psychoanalytical, there’s a reason why IRL psychoanalysis is not the line of treatment used to treat neither addiction nor any of the other conditions Carmy has, such as C-PTSD, burnout syndrome, etc., all the other stuff I mentioned here in the extended version. What I didn’t mention there is Carmy’s neurodivergency, AUADHD (educated observation based on Carmy’s monologue in S1 and basically Carmy’s behavior during THE WHOLE SERIES and his untrained and innate talent in the arts that leads to alienation, etc) because neurodivergencies are not mental health issues, necessarily, so they shouldn’t be put on that list.
Carmy’s case is a clear case that IRL would be treated with a combo of Systemic Therapy + the classic line of treatment for addiction based on cognitive behavioral therapy (CBT) + what nowadays is starting to be also paired with neuroscience therapy (NT) and giving very positive results. I won’t bore you even further with the figures but they can easily be found online.
My point is: The Bear, the name of the show, represents not just Carmy Berzatto, The Bear, but also the place where many souls come together to interact with each other and all those lives are going to intrinsically be changed by that experience, that has The Bear in common. Thus the show as a whole, including all of its characters, of course, is SYSTEMIC, which is the opposite of the Psychoanalytic approach. And it's super important to take this into account because the systemic approach in mental health and in every other field where it's applied, like in business, or even education, etc is an approach in which everything is viewed as part of a whole, it's basically like a continuous dance between the individual personal perception and it's environment and how they both affect each other, whereas the psychoanalysis' ultimate goal is getting as deep in the individual psyche as possible, dive into the individual's deepest unconscious.
In case you are wondering, I do have the credentials but I'm also and most importantly, one of those who believe that you don't need credentials to discuss mental health, and this show is among other stuff very much about mental health. What you need is the desire to be aware of it and as a matter of fact, I strongly advocate IRL for mental health to be actively talked about in class since elementary school and included as part of the curricular activities throughout the entirety of the school years, all the way to Senior year. Basically, I'm all for even kids with no Elementary education credentials talking about mental health. Mental Health shouldn't be an elite topic, or taboo, or necessarily a "problem". That doesn't mean that misinformation should be spread, clearly, and I have seen A LOT OF IT AROUND HERE LATELY WHICH DROVE ME NUTS, but it does mean that the fact that I have plenty of credentials to talk about this matter, is not the point.
So, back to my point: when those kids go out into the "adult world" they not only have an accurate self-awareness about their own mental health, but they also have more empathy for others and tools to cope with what we all know they will have to cope at some point in a world that is far from perfect, but most importantly have compassion. All of this to say: cases like Carmy's, Donna's, Michael's, Chef Fields, etc could be prevented or not as dramatic if we'd look at mental health as "a must" to be dealt with from a very young age, at home, school, later at work, etc. We shouldn't talk about it only if there's a problem that moves us to go and get help, or that makes us wanna go to therapy. NO! Mental health awareness can be as simple as a breakfast at home where we actually talk and listen for a few minutes while we have that cup of coffee or dig into that bowl of cereal, mental health awareness can be us watching The Bear as a family and using that space to vent about how we see ourselves or our families represented by that scene on the screen, mental health awareness can be us choosing not to lash out at someone WHO DESERVES IT BC THEY ARE BEING A BULLY or trying to get attention in a passive-aggressive way and rather set healthy boundaries, this can be practiced online or offline, of course. Mental health awareness is understanding -or trying our best to- that the person we are interacting in one way or the other with, can very well be in this headspace:

I said understand, not necessarily tolerate. But that understanding based on compassion can change it all. That is my point.
Bonus track: I am still mad at Storer but I forgave him, kinda like what Syd keeps doing with Carm because she gets what I just said, she's a natural. BUT Storer is still, and will always be, my spirit animal because he portrayed mental health like I have never seen on TV before. No misstep he takes, and he did take a few this last season, will ever undo the amazing job he did in the past, and I will always be grateful to him for that. He started a conversation that was loooooooooooong overdue.
#the bear#carmys mental health#sydneys mental health#sydney adamu#carmy berzatto#the bear season 3#SYSTEMIC NOT PSYCHOANALYTICAL TYVM
13 notes
·
View notes
Note
Omg, your response was so amazing and helpful 😭❤ Thank you for taking the time to really get into all that. 💞 It also seems to have kinda sparked a conversation arround it, which is awesome! 😁
And ohhhhh ya, the religious trauma and gilt are real 😳🙄
You mentioned you have more to say if we want to hear it? I, for one, would LOVE to hear anything else you have to say on the topic! ❤
-🫖
Hi hi hi 🫖 anon!!
{Let’s Talk Religious Guilt and Trauma}
I am so glad that my response—Let’s Talk Healthy Solo Sex— was helpful and informative for you!! Of course!!! I want to give every ask and every anon the time and respect that they deserve ♥️♥️ And yes, I love that it sparked more of a conversation!! I’m so proud of you for reaching out and starting these discussions, anon!!! 🥰
I most definitely have more to say on the topic. For one, you can check out Let’s Talk Penetrative Sex and Let’s Talk Trauma in Relationships, which both stemmed from our conversation! And then there’s this response, fyi it will be another longer one 😊
*sigh* Yes, religious guilt and trauma are most definitely real. And those of experiences and feelings are so valid. Trauma of any kind is no joke. If you have any religious trauma or trauma of any other kind, I highly recommend that you seek a professional’s help.
So… What is Religious Trauma and Guilt?
A general definition for Religious Trauma is… “Religious trauma can happen when an individual’s religious experience has been damaging, abusive, degrading, stressful, or traumatic. When a religious experience is traumatic, it can damage your emotional, mental, physical, and spiritual health”. Check out Cohesive Therapy NYC’s article on Religious Trauma for more detailed information! For an article that goes more into Religious Guilt, check out Considering Counseling’s article on Religious Trauma and Guilt…! ♥️
Religious trauma and guilt are especially tricky beasts… Many twisted religious teachings and persuasion is very cult like. (That’s not to say that all are, there are definitely less twisted, healthier religions and practices) But the ones that are rotten and manipulative, they dig deep into your core beliefs, especially if you’re a child, and they replace your identity with the identity of the religion/church/cult.

So, how do you deal with religious trauma and guilt?
Firstly, as I said above, seek professional help (I recommend an EMDR specialist for trauma—EMDR is a type of therapy that works to restructure traumatic memories in your brain)
On your own accord, Processing, Accepting, and then Healing is the overall goal. Talking it out and processing your experience and feelings with a trusted person can be helpful for some. I find that talking to someone who has also had religious trauma or guilt to be even more helpful, because of how they can relate. Sometimes journaling/writing about it can be another helpful tool. The key is to find some way to express those emotions, to get them out of you.
Personally, my own story is that I have both religious trauma and guilt, but I definitely struggle more with my religious trauma. I was raised in a Catholic school and an Interfaith-Christian household. We moved around a lot, and so I went to many Christian churches like Non-Denominational, Baptist, Presbyterian, Catholic, and Southern Christian/Baptist. After the Catholic primary school, I moved to a Christian Charter school for six years. At that age, all my activities were based around my church and religious school; safe to say, religion was a very big part of my childhood. When Covid hit, I had had enough and I used the social distancing and the lockdown as a way to disconnect from the church. I effectively stopped going to church in 2020. I then took that time to explore my religious trauma and guilt, and this was where my healing journey began.
Everyone’s journey is different, and everyone’s journey is valid. ♥️
I began my work with my CBT therapist (Cognitive Behavioral Therapy— most therapy is CBT or Freudian). I found that most of my religious guilt was tied to my sexuality, and that I really struggled with being gay and being religious. So I explored that. I talked about it with lots of people, including my therapist, trusted family members, and other trusted religious people. I found that finding others who struggled with sexuality and religion was extremely helpful, it made me feel validated and not alone in the struggle. Today, I am way further along with my religious guilt than I was 3 years ago, but I definitely still have more to process, accept, and heal from.
Next there was my religious trauma. For this, I started with my CBT therapy as well. It was helpful, but after 3 years, I have run into a wall… It depends on the intensity of your trauma, because “little t” trauma is more easily resolved through CBT, whereas “capital T” trauma requires the neural network in your brain. My trauma is more “capital T”, and so I found that CBT therapy only helped me so much. This is why I recommend EMDR therapy for trauma. EMDR therapy targets restricting your neural network, working out the traumatic memories.

Everyone’s experience is different, so what worked for me and what didn’t work might be different for you, and that’s okay. This is only my experience. But I hope that it was a little helpful, and that you at least feel less alone in your feelings. Because they are so valid. ♥️♥️
So yea, those are my key points for religious trauma and guilt…! Hope this was somewhat relatable, helpful, and informative 🥰 Don’t hesitate to reach out and chat with me, ask or dm! Hope you have a lovely day/night!! 💞💞
Talk with Me ❤️🔥
#talk with me#i want to hear you#🫖 anon#anon asks#you are valid#i hear you#spread the awareness#spread the word#religious guilt and trauma#religious trauma#religious guilt#trauma#traumatic childhood#traumatic memories#traumatic experience#healing#healing from trauma#therapy#cbt therapy#Freudian therapy#emdr therapy#i'm traumatized#traumatized#cissyenthusiast010155 answers#spread the positivity
19 notes
·
View notes
Note
I was wondering, if Huchu attempted cognitive behavior therapy then how did he run those sessions in terms of what did he do to try to help the others? Considering you wrote that, in doing so he caused the others to "internalize their problem to the point they cannot be helped anymore including himself". Also, did he think he could be like a psychiatrist (or at least provide similiar service) due to the fact that psychiatrists work with medicine?
I hope my question is clear enough. If not, feel free to ask what I am trying to ask (^^)
Thank you for tuning in to my frequency! The answer contained potentially triggering contents, so I'll hide it under the cut. Please enjoy. ✨
Huchu’s Qualifications
Huchu has bachelor's degree in neuroscience, master's degree in Pharmacy. D. and is currently studying PHD on medical instrumentation engineering. Aside from taking class, he’s a neurosurgeon at marine corps hospital, take shift as a battlefield surgeon at marine camp and use the rest of his free time to operate Lubi service so he has the following active licenses, Pharmacist license and P&S license.
In Northland, here’s the requirements for attaining psychiatrist certification: Be a graduate of an accredited medical school certified by International Red cross committee, complete all trainings in a program approved by Northland mental care bureau, have an active, full, unrestricted medical license, and have satisfactorily completed the Northland mental care bureau’s specialty training requirements.
So do keep in mind that Huchu is not qualified to do psychiatrist work as he lacks item 2 and 4.
Does Huchu think he is qualified to do psychiatrist works?
Unfortunately, yes. Despite lacking all the correct trainings, he tried to be both therapist and psychiatrist for C2ISTAR as you can see Hongcha mentioning Huchu being the one who prescribed Risperidone for Angae in [🌹for Angae].
This is because Huchu think that Clinical Psychology is like Neuroscience but less scientific. Similar to our world, neuroscience is praised as the hardest medical major in the world. So naturally Huchu look down on psychology as an easier neurology mixed with social study. So, in his little head. If mental care staffs can do it, then definitely neurosurgeon can do it too.
Clinical Psychology in the world of C2ISTAR
In the world of C2ISTAR, Mental illnesses are usually deemed as invalid illness, so the mental care industry is constantly being look down upon. The discrimination also discourages many people in this world from studying clinical psychology. Even if Huchu open his mind and take studying clinical psychology seriously, it is still very unlikely that he will produce good result as study material for clinical psychology in this world is ineffective at best from the very beginning due to the lack of interest this world has toward it.
The acceptable branches of psychology are study by the industrial, intelligence and defense service for the purpose of manipulation, interrogation and indoctrination which is very different from clinical psychology in practice.
Clinical psychology is also heavily associated with the Aldehyde cult. A multi-faith cult that believes mental illness is a sign of ascension. The more soldiers lose touch with reality, the closer they are to heaven and if they are close enough to heaven. These soldiers will be able to give birth to the new Angel that will be savior to their world. They often kidnapped veteran from asylum so they can use these veterans to birth a new Angel.
Huchu's treatment on C2ISTAR
Huchu might be well intention and most faults mainly resulted from ignorance, but the damage is still there. In fact Huchu is actually skeptical that CBT would produce result, however, C2ISTAR seems to need it and Huchu is weak to that. Here are the treatments Huchu did on each C2ISTAR alongside its effects.
Orenji’s treatment
Orenji is Huchu's first patient for CBT service with his main problem being Paruresis. Huchu choose Journaling and Cognitive restructuring technique for him. However, the underlying root of Orenji's Paruresis is Urolagnia so Orenji can't quite be honest with his thought. However, the cognitive restructuring is somewhat almost effective due to the other physical treatment. Orenji had chronic UTI that connected with bladder infection, so Huchu often insert catheter for Orenji whenever he needs it. This seems to cause Orenji to associate Huchu with relieve, hence the reason why he can go when Huchu is around. But can't quite do the same with someone else. Orenji also seems to develop some form of incontinence whenever Huchu is around.
Huchu also lose his temper every time Orenji induced temporary amnesia on himself because he knows how fragile Orenji's brain is as he was the one who put Orenji's brain and sculp back together so he's constanly worries about Orenji accidentally killing himself but since Huchu always arrive with Clozapine, he had been unknowingly endorsing Orenji's behavior. Still, after Orenji is back to his sense. He would have to endure a session of outburst Huchu throwing things at him or start hitting him with a chair.
Baegcha/Hongcha’s treatment
The main method is Role playing through puppet activity; the idea was so that Beagcha could see why he need to stop pursuing his stop-list so they can start working on his fear of touch. Usually when a certain method doesn't work, therapist would move on to the next one, but Huchu let Beagcha continue with the ineffective method because this is what Beagcha prefer to do and Huchu doesn't have the heart strip this away from him. Huchu later resort to locking Beagcha in his room whenever Huchu notices things are taking a toll on him and simply use puppet therapy as a way for Baegcha to process what he went through each hunt.
Huchu also deemed Hongcha to be something he need to get rid of because Huchu see Hongcha as the evil alter that endorse Baegcha to pursue the stop-list. The thing is that, neither Baegcha nor Hongcha are the host. Both Baegcha and Hongcha are alters pretending to be the host. Usually alters are protective of each other and take responsibility as a system. However, Huchu intervention had created a dynamic where both alters cannot get along. And because Beagcha trusted Huchu, he begun to think he needs to repress Hongcha to be better and Hongcha became bitter toward the situation, he blamed Huchu for his sour relationship with his alter.
When Hongcha appear mid-session, Huchu would either shock him with electricity or shove him into a small box to chase him away. Huchu did made many attempts to get rid of Hongcha ranging from submerging him in extremely cold water to purposely staving him and since Hongcha is unaware that it is impossible to get rid of an alter. Hongcha see Huchu’s attempts as life threatening situation and in retaliation, he believes that he must kill Huchu which make Baegcha agreed with Huchu even more.
Seoltang’s treatment
After discovered that sedative doesn't work on Seoltang. Huchu would mainly use Imagery and Relaxation training. However, the underlying cause for Seoltang's insomnia is cumulative anxiety of being in disguise. Something Seoltang cannot tell anyone due his true identity. Huchu had no idea about Seoltang's anxiety, so he had no idea why Seoltang sleep schedule doesn't improve not to mention that imagery make him feel worse as it worsens his longing for the place that no longer exist.
Out of concern as Seoltang already show all signs of developing Alzheimer, Huchu decided that any methods that give Seoltang shut eyes will suffice and purposed the hypoxia idea. So instead of having his anxiety treated and get an actual sleep, Seoltang ended up inventing so many self-choking methods that even people with choking fetish would think that this man is a freak. Thus, Seoltang's anxiety was never addresses not to mention that one of hypoxia common symptoms is also anxiety which contribute to his mood swing getting worse as well.
Noeu’s treatment
Noeu is way too shy to address that his overworking tendency came from his constant fear of unexpected death, so Huchu assumed that Noeu is obsessed with conquest and taking control. This led to Moral reconation therapy. However, Moral reconation therapy required to be practiced in groups as one on one session can reinforces narcissistic behavior. Somethings that should not be mixed with Noeu’s competitiveness and ambition.
The therapy also required the therapist to be well versed in the subject of morality to work which Huchu’s morality is ambiguous at best so he can’t always keep up with Noeu’s questions or leaps of logic. This unintentionally validated Noeu’s thought derailment and prompted him to go from weakening other nations then have Northland invade them to the exact same thing but also profiting from them and take advantage of their resources because he’s more confident in his ideal than ever and he now genuinely think he’s doing this world a favor.
Angae’s treatment
Usually, therapist would approach patient with hallucination with Reframing technique. Something that Angae had already accomplish on his own. This is because managing a psychosis episode with medication was proven less effective as medication came with side effect. However, due to Huchu being a neurosurgeon with neurology logic. He goes straight to prescribing Risperidone and focus more on helping Angae with anxiety using Stress inoculation training. However, Angae didn't stress out because he's worrying about having an episode. He has an episode because he's stressed out, so Angae made no progress and Huchu had been accidentally gaslighting Angae into thinking that he had an illness he didn't have.
Angae already questioned reality around him, so he is unsure how valid his opinion is about the topic. This led to Angae letting Huchu continue with the treatment that make no sense to him even though this fueled the thought that he's being held back to fit into a certain explanation.
Yuseong’s treatment
A lot of people with Hyperthemesia has tendency to be obsessed over things easily as well as having trouble moving on from the past because they had trouble forgetting things. So Huchu choose Metacognitive therapy and Distraction technique. Due to the confusion that came with partial amnesia combined with the fact that Yuseong never experience forgetting stuffs before, Yuseong is desperate to seek for things he can identify himself with. This led to his obsession to connecting his identity with the unhealthy diary, something Huchu sees as a form of delusion.
Usually, the first rule of dealing with delusional patient is to validate their experience. Although what happen isn't real to us, it's real to the patient. However, due to Huchu's concern of Yuseong recreating situation in the diary. Huchu usually react very sternly and outright dismissed Yuseong’s belief in the session. Since Yuseong can control his expression well, Huchu had no idea that he is invalidating Yuseong. Although Yuseong still likes Huchu, he began to pay less attention to the session and draw or play with his alphabet book whenever Huchu is holding a session for him. He also hold on to the diary even tighter than before.
Effect of failed treatment on Huchu
Therapy is a stressful and draining job, both therapist and psychiatrist in real life are trained and educated on how they can handle their job without intaking their patient's baggage.
But since Huchu never went through these training, all the negativity goes straight to him and since he is at the end of the line for mental comfort. Combine that with his habit of caring too much, he got stuck in a position where he himself has no one to go to for all the problems above he involves himself in. This of course fueled his urge to go through with unethical method to get what he wants for instead, considering amputating Noeu so he never has to worry about him arriving at ER with seizure again.
.....................................................
Clinical psychology is one of my weaker subjects, so the treatment descriptions are simplified at best and none of my statements should be considered scientifically accurate.
Still, I hope this information suffice you. \(^^ )✨
7 notes
·
View notes
Note
i disagree with a lot of your views on mental health just given my own research and knowledge of mental illness and the dsm-5.
i think the inherent issue with it is the categorization. organizing things by how they present behaviorally feels very unscientific. we need to do a lot more research to lean into like a sort of biological taxonomy. one big example is that schizophrenia and bipolar disorders have a LOT of overlap in brain areas, and while they are not identical areas, treating bipolar as something closer to anxiety and depression seems like a poor way to treat it, especially if you're looking from biological and medical perspectives.
i'm not as familiar on ptsd and personality disorders, but there's a lot of overlap there, and considering my own experience "developing a cluster b personality disorder" from trauma (i say this in quotations because i do not actually like the diagnostic system and would rather remain undiagnosed), i wouldn't be surprised if there was neural overlap in like, activity, connectivity. There's probably other stuff too we haven't really looked into. I feel like there's so much more we can do to look into the neurology of mental illness than we're doing as is. Focusing on symptoms too much, and even neurology wise plasticity can be a problem. Did you know bullying can change the way your brain works?! (Reductive way of saying it, but there's a bit of research on bullying +plasticity, also i'm off track.)
i also feel as though the clinical/general applied psych community could do a lot more pulling from basic research. we only get the moolah if we work through their lens (i'm a cognitive neuroscientist), so like. i wish therapists and psychiatrists would look a little more into our readings sometimes...
i've been doing a lot more reading on dimensional models, and i kind of like what it's putting down. part of me worries that having neurological profiles of mental illnesses might end up sort of labelling neurotypical people in the same sort of essentialist way a lot of diagnostic labels do with mentally ill people (reason i would like to remain undiagnosed). But I think the idea of quote unquote "neurotypicals" with tendencies (something discussed both in literature and in clinical settings where mental illness is defined as symptoms + distress) and similar brain patterns to those with adhd, autism, ocd, depression, psychosis etc sort of forming community with those who have those disorders proper. i think we could learn a lot from one another! coping mechanisms, how to deal with big stressors, learning what sets us off in situations with better coordination and less yappy narcs than group therapy. perhaps it's idealist, but i'm a bit of a dreamer.
i hope you read this and consider my point of view, even if it did meander a bit XD
It took me awhile to be able to sit and take this in, and even still I'm having a hard time comprehending chunks of it so if my response ends up misinterpreting anything feel free to send another anon to clarify.
I do agree that we're still not at a perfect stage of "all of these things are 100% properly understood", and by no means do I feel psychiatry has managed to hit a perfect stride when it comes to diagnostics either. Things can and do still get misdiagnosed for various reasons, and there's definitely disorders that get seen as "similar" because of behavior that brain-structure wise may be worlds apart.
I also agree that in concept, having spaces that allow currently undiagnosed/traits of/self-suspected people, or those who just have a few similar symptoms that find themselves relating to, is certainly not a horrible idea. Having peer-to-peer support spaces shouldn't necessarily depend on whether or not a doctor has given you the "stamp of approval," and in some cases I've even seen well-vetted, non-specific spaces that foster this in a very positive manner.
But in the spaces dedicated for a specific disorder, the language used in them is.... not that. It isn't someone who suspects they have it asking for advice on how to see a doctor, or another saying "I relate to x symptom, what do the people here with y disorder find helpful for mitigating this?"
It's often rife with people who, whether due to comorbid disorders, malingering, or active faking, are spreading vast and wild misinformation that causes harm to both those already diagnosed (possible to adapt false behaviors and receive improper care if doctors assume misdiagnosis), and those actively seeking one (may exaggerate/lie about symptoms or use key words found online that lead a doctor to assume malingering, even during real cases).
There's so many takes that disregard the medical misinfo to fixate on validating "all" experiences, regardless of when those experiences indicate a different disorder. And if that gets called out, then you're fakeclaiming every single person there somehow. And if the space is actively pro-self dx, then they're often prone to telling people that no psychiatrist should be trusted (ESPECIALLY if they tell you your self dx is wrong) and that a diagnosis doesn't matter anyway because it's all some grand conspiracy to further oppress you.
And outside of that, even when someone has similarities, traits, or specific relatable symptoms, there's times where those of us experiencing a specific disorder want to feel a sense of community with those who have the same type of experience, and not just someone who understands "by proxy" or as an outsider.
I have plenty of people who don't have a dissociative disorder in my life who can relate to certain symptoms I have, or can understand in a sympathetic manner when I talk about my experiences and frustrations. But I don't know anyone else with DID, let alone that I know is being honest about it. I don't have a sense of community or belonging-- I feel isolated. And the internet hasn't made me feel more of a sense of community in having DID, but instead it's managed to make me feel more shut-out due to how wide-spread the horribly reductive rhetoric around it is.
I don't have this in regards to having autism or adhd. Hell, I'm even less strict about my views around posts and self-recognition of those because 1. they're often found due to social irregularities that a person experiencing them may be able to pick up on, and 2. people are much more receptive to when misinformation, infantilization and ableism in regards to them is called out.
This has turned into a bit of my own meandering but basically, a lot of my frustration at the moment is stemming from the internet's treatment of DID (and dissociation in general), and there's definitely things I've said about disorders in general that I think there are exceptions to, but it can be hard for me to sit down and think about/talk about those things while I'm wrapped up in my frustrations about this thing specifically.
4 notes
·
View notes
Last Seen Blogs

blacksuitmen
Black Suit Men Comic

bigplugplease
Welcome!

lulivixuk
Untitled

weasleyofbagend
The Quibbler

yandere-cub-blog
✂ - - - -