#where i get to evaluate the problems in the diagnosis/treatment of mental illness
Text
psa my last exam is on may 18th whereupon i will be able to discern whether this existential dread and dysmorphia is a result of academic stress or just my brain chemistry. i hope it’s the former but i won’t know until may 18. ie the day i finish the ibdp. may 18 10am. may 18
#the ib kinda ruined my life#in arabic i call it a ‘tawbe’ which kind of literally means i would rather die than do it again#leah.txt#its fitting that my last exam is psych paper 2#where i get to evaluate the problems in the diagnosis/treatment of mental illness
29 notes
·
View notes
Note
Hi! It's me, autistic Chosen anon.
Firstly, I appreciate it that you took the time to share more of your experiences with me. I've actually read your reply multiple times now, and I have to say, it's very sobering. Especially in the sense that I recognise so much of it.
Just one(1) personal example, the part where you talk about already fixating on delusional thought processes as a kid. I did that too! Except in my case it developed into mood and anxiety disorders as I got older, instead of overt psychosis.
Look, I already had compassion for psychotic people of all types, because life simply dealt you a very difficult hand. But it also felt like something distant from me. And it really isn't. You were right. We're not that different at all. ALSO, as we're seeing more and more of these overlaps and interconnections between all kinds of diagnoses, I think there's A LOT to be said about the approach of the psychiatric field as well as the neurodivergency and mental illness communities...
That being said, cheers to you, my fellow in neurodivergency, and thanks again!
Oh Jesus, do not get me started on my issues with diagnoses. I thought about going into it in that reply and I was like "you know what? Too complicated, too personal, and too much baggage." But if you're bringing it up? Let's go.
So. I am not actually diagnosed with schizophrenia. My official diagnosis is "other specified schizophrenia spectrum or other psychotic disorder." I think you can see why I simplify to schizophrenia. But also, I was not diagnosed by the actual DSM criteria. I was diagnosed by a research clinic attached to a university that is trying to get the criteria for various psychotic disorders changed for the DSM-6, and to get their own evaluation to become the standard instead of the current ones. The thing is, their evaluation is much stricter than the current criteria. By the DSM? You need to fit at least 2 of 4 categories of symptoms (which I do). By this clinic, you need to have all 16 of 16 of their categories of symptoms. The last time they evaluated me, I had 11 of 16. If I were evaluated by other clinicians? They'd just diagnose me as schizophrenic. In fact, I've explained this to other medical professionals and had them say, "what? 11 out of 16 is definitely enough to be schizophrenic? You definitely don't need every symptom?" So as much as yes, I do not have every classic symptom and my schizo-spec experience is non-traditional... There's a reason I have no problem just calling myself schizophrenic these days.
The clinic very much is doing that thing where you try to solve a problem and end up creating new problems. The problem is that a lot of people have what are called sub-threshold psychotic symptoms. Basically, psychotic symptoms without ever going into a state of actual psychosis, or completely disconnecting from reality. I personally am not convinced that there is a hard line between experiencing symptoms and having "actual psychosis." Like, these therapists say I have never had real, full psychosis, but I have been pretty goddamn delusional. I sure wasn't functional! I was out of school! I was constantly fixated on my delusions! I was in a state of severe distress! And the onset of my delusions was a pretty sudden thing to the point that I can tell you the exact date and time. It was my birthday. Lucky me. Anyway. Point is. There are a lot of people who experience these symptoms who, unlike me, will never reach the point where anyone would diagnose them as schizophrenic. Right now, they are slipping through the cracks because there is no diagnosis to give them. There is a push to treat them, but coming from the idea that people with these symptoms are in the early, pre-psychosis state of schizophrenia (the term here, if you want to google it, is prodromal psychosis). The idea is that treatment in this early stage will prevent people from ever actually reaching full psychosis. That's why the clinic started. But as they did research, they discovered that even without treatment, only 20% of these people will actually develop "real" schizophrenia and "real" psychosis. This isn't just the early phases of schizophrenia; it's a separate thing of people with more mild symptoms existing who will never convert to schizophrenia. The term that they want to be in the DSM-6 is Attenuated Psychosis Syndrome. Attenuated means less severe. So literally, "it's like you have real psychosis but less bad." Needless to say, I fucking hate this term. It's still better than their original term that they're moving away from, though, which is Clinical High Risk syndrome. Literally just "well, you're at risk of developing a real disorder."
To use autism as a metaphor, it's like if people noticed that hey, a lot more people seem to be autistic than we are actually diagnosing. Right now we're just diagnosing the people with high support needs who are super disabled by it. But other people could use recognition and help too. But instead of just lowering the criteria for what counts as autism, they say "hey, let's invent Asperger's syndrome." You know. That diagnosis that doesn't exist anymore for good reasons.
And then, also, how do we communicate with these people with Asperger's syndrome? Instead of saying "hey, you're autistic, and that's okay and awesome and valid," we say "while yes, you're on the autism spectrum, don't worry. You're not actually autistic. You're not one of those people, and you'll probably never have real autism. Don't go calling yourself autistic. You're not one of them." Yes, you heard me right... They actually have the gall to tell people like me "you're on the psychotic spectrum, but you're not psychotic. You can't call yourself psychotic." Which... What? That's not how spectrums work? The entire attitude of the clinic is "don't worry. You're not schizophrenic. You don't have psychosis. I know those people are scary. Don't worry. You're not one of the scary people with the scary thing." They look at the stigma and instead of even trying to fight it, they say "don't worry. You're not one of the stigmatized group."
So imagine being me. You just got a diagnosis that doesn't actually exist. If you google it (which is hard because they're using about 5 different names for it and can't just decide on one), you'll find a bunch of information that is either in scientific papers that are only written for other psychiatric people to read and not laymen, or information that is outdated compared to what the clinic is now discovering (stuff saying that sub-threshold symptoms only exist as the prodromal phase of schizophrenia). You feel alone as shit, because of course you do, the entire world thinks that psychotic people are cr*zy freaks. So you start looking to psychotic and schizophrenic people for community. You start identifying with them. When explaining your mental health, you just call yourself psychotic. And what do your therapists say? "No. You can't call yourself one of them. You are on their spectrum, but you're not really one of them. Doesn't it make you feel better to know you're not one of the freaks?" No. It doesn't. I'm already one of the freaks, and you've just cut me off from the only community I have because you've given me a diagnosis without any recognition or community. The reason I'm now confidently able to say "fuck you, I am a real psychotic and a real schizophrenic" is because I haven't been part of that clinic for two years so no one is telling me that anymore. The bounds of their studies mean that you can only be treated by them for 2 years and then you get kicked out because if you make it to 2 years without developing "real" psychosis, their research says that you never will, and they are still sort of operating under that original mission of keeping people with prodromal schizophrenia from going into psychosis. While I was still there, the way they tried to distance me from the rest of the spectrum as if that was a positive thing fucked me up. I felt so alone for so long, and I felt guilty for associating with and seeing myself in "real" schizophrenics.
I think the model we've reached with autism is where we should go with schizophrenia. Just call everything "schizophrenia spectrum disorder" (Yes I know autistic people hate ASD as a label because of the disorder part, but I think even the proudest schizophrenics who like and embrace some of their symptoms and don't want them all fixed still agree that it is a disorder. Yes, not all delusions actually need to be cured. Some of them can be positive and beneficial, even if personally none of mine ever have been. But stuff like disorganized thinking, anhedonia, and catatonia are always awful, and they're part of the package too). People who are currently going undiagnosed and who attenuated psychosis syndrome was coined for are the low-support needs end, and people who are currently diagnosed with schizophrenia are the high-support needs end. It's not exactly a perfect correlary, but I think it's reasonable. Unfortunately, while I don't know what's going to actually happen with the DSM-6 (which is still probably a good ten years out since a revision of the DSM-5 was released last year), as far as I know no one is proposing that. God knows when we'll ever get a reasonable and destigmatizing approach to the schizophrenia spectrum, but not any time soon.
God that was long. Well, thank you for giving me an excuse to rant. Basically, fuck the medical model, fuck the DSM, and fuck the people who are trying to change the DSM, too.
6 notes
·
View notes
Text
My Take On Self DXing
Disclaimer: My definition of self diagnosing is putting in A LOT of time into researching, trying to get a professional diagnosis *first and foremost*, among other elements. Not just looking at the top 3 traits of a disorder and saying "that's me!", that is not recommended and I do not condone that! Please be safe <3
I'm making this post because I've gotten some comments here and there of people using my posts as a reason to self diagnose/suspect autism, BPD, etc (whatever else I post about). I do *not* condone using my posts as a tool for this, as this blog is all about my *personal* experiences with being neurodivergent. Everyone is so vastly different and I do not represent everyone with these disorders! However, as someone who has self diagnosed before getting professionally diagnosed (and still haven't been professionally diagnosed with them all!), I understand the need for an identity and an explanation for your experiences. So here's some reasons I support self diagnosing, some tips, and some warnings.
Why I support self diagnosing
Mental health care in certain locations are absolutely horrible. Where I live, mental health care is...very limited. The professionals in my area are trained in very few areas, mainly depression and anxiety, and are trained to do very specific types of therapies, medications etc. For example, in the ER I was given a xanax for a panic attack, and this worked wonders for me, however when going to a psychiatrist I was told they don't prescribe those on the off chance that someone will get addicted. Because of this, my anxiety has been overlooked and I've been given medications that did not work and has even given me a bad reaction. Needless to say, I stopped going to psych appointments. (I don't recommend this for everyone! This is just a personal experience).
Insurance isn't always an option. Without insurance, you will be paying out of pocket for evaluations, therapies and treatments. Even a diagnosis. An autism diagnosis here out of pocket is anywhere from $1k USD to $6k USD in most places for adults! That includes the two part evaluation and then having it on paper. I have what's called a pending diagnosis of autism, which means that I was given a basic screening (thankfully for free, but it costs $500 out of pocket on average here!), and the results were that I am very highly likely on the spectrum, but I can't afford to continue with the evaluation. So my health care team knows that I am autistic but will not put it on paper, therefore I can't get any accommodations with my insurance, and any accommodation that I need has to be listed for "anxiety", which my insurance doesn't see as a big enough problem in an adult to cover things for.
Being professionally diagnosed is a privilege. A lot of mental health professionals have a bias, and this is an unfortunate truth. Racism, sexism, classism, and even fatphobia play a huge part in how you're treated by the health care system, including mental health care. For example, if a healthy, average white cis man goes in and explains his symptoms and can afford to pay whether it be through insurance or out of pocket, he will be taken much more seriously than someone who is not any of the above.
Why I don't support certain self diagnosing disorders
A self diagnosis is not anywhere close to a substitution for a professional diagnosis. You will not get the proper therapy, treatment, or accommodations necessary by self diagnosing. You also won't be taken seriously by professionals if you walk into their office and say that you have a disorder, because their next question will be if you have documentation of the diagnosis. If you are suffering from a severe mental illness such as schizophrenia or borderline personality disorder, you will likely need treatment and therapy if at all possible. If you are able to get this, please do!! Do not suffer alone!!
Some disorders have overlapping symptoms...autism included. While I support self diagnosing autism to an extent, you have to realize that autism in a person who does not have high support needs will more often than not look very similar to ADHD, OCD etc etc. Autism being a spectrum can make it look like so many different things in so many different people. Someone with autism may be hyperverbal, able to read tone of voice and emotions with ease, and be outgoing, which are all traits that are not inherently apart of autism.
If you do not have *insert disorder that you self diagnosed*, you may be spreading misinformation. Many mental illnesses are already so stigmatized. Regardless of if YOU think that YOU have this disorder and that YOUR experiences are part of it, if you're wrong you may be adding to the stigma. For example, there are a lot of people who fake tourettes, dissociative identity disorder, etc. and this is very dangerous to people who actually suffer from these conditions. When self diagnosing please be mindful of others when you post about it publicly and be sure to specify that you are self diagnosed if you do! This is not meant to be mean or make you feel any less valid. Your experiences, regardless of your disorder or label, is 100% valid and you deserve to be taken seriously. But you have to realize that your words have impact on others.
"Tips" for self diagnosing
Don't! If you can easily get a professional diagnosis. See above points for why.
If you do, put in the research! This doesn't mean look up "autism spectrum disorder" on Google and look at the first 3 symptoms and decide that you resonate. Look up how it is professionally diagnosed, what the DSM-5 criteria is, and speak with/watch content creators, friends, family etc that have been diagnosed!
Take note of the different variations in different individuals. Do not watch one YouTube channel of a person with *insert disorder* and think that they represent the entire community. They do not. Not one single person represents an entire community, this goes for any, mental illnesses, physical illnesses, etc. If you know one person with autism you know one person with autism.
Research other conditions that are similar. You think you're autistic? Cool, research it as stated above! But don't forget to research ADHD, OCD, and other disorders that have overlapping symptoms! And yes, it is possible to have multiple, which is another reason why self diagnosing can be tricky.
ABOVE ALL ELSE: LISTEN TO THOSE WHO HAVE BEEN PROFESSIONALLY DIAGNOSED AND TO PROFESSIONALS!
There is no shame in telling someone, especially a therapist, that you think you have a disorder. What will likely happen is that the more you fight for yourself and your concerns the more you will be taken seriously and possibly given an opportunity to get a screening. The worst that will happen is that you'll self diagnose and get it wrong, but possibly be properly diagnosed! You know yourself better than anyone. Regardless of what label you have, you are valid, you are loved and you will be okay. If you ever have any questions or concerns, please feel free to reach out to me! I'm here for you!
For transparency, this is my situation:
Autism - pending diagnosis, see above
ADHD - diagnosed
PTSD - diagnosed
Dissociative identity disorder - diagnosed, previously self diagnosed
Borderline personality disorder - sort of pending. was told by a therapist that it seems more likely that I have BPD than bipolar disorder, but it was never screened. self diagnosed
Bipolar type 1 with psychosis - diagnosed, mixed beliefs from different professionals, personally undiagnosed
Eating disorder - diagnosed (will not elaborate, am in recovery!)
#adhd#autism#actually adhd#actually autistic#autistic#asd#borderline personality disorder#bpd#cluster b#ptsd#disordered eating#bipolar#dissociative identity disorder#did system#mental health#mental health awareness#self diagnosis#self diagnosed#self dx
13 notes
·
View notes
Text
Let’s talk about depression
In my latest book ‘The Power of Death’ I talk about this topic in depth. I will post the links to it at the end of this post if you are interested in reading it. If there is one part of the book that resumes the message that I wanted to transmit, it’s Mikasa’s (The main character) press conference at the end of the last chapter.
It’s okay if you don’t read the whole book, but at least, read the following extract from the book (some stuff removed to avoid spoilers):
Standing behind the podium Mikasa started the conference by saying,
"Paradis island doesn't have studies about the topic we are about to discuss, but other countries do. In the United States, in 2019, a total of 47,511 Americans died by suicide and an estimated 1.38 million attempted it. [2] What about other countries? you may ask, well, overall, suicide was in the top 10 leading causes of death across Eastern Europe, Central Europe, high-income countries within the Asia Pacific, and Australasia. Within regions and countries, though, suicide rates soared among people with lower social and economic status. [3] This data comes from research made by the Institute for Health Metrics and Evaluation in Washington, Seattle. [4] This goes without mentioning that for every suicide, it is estimated that there are seven to ten people intimately affected."[8]
Mikasa stopped to take a sip of water and looked back at the audience to continue her speech,
"Untreated depression can, and possibly will lead to suicide, death. In biology, homeostasis is the state of steady internal, physical, and chemical conditions maintained by living systems. [5] Depression does have an impact on this. Research shows that the hippocampus is smaller in some depressed people. For example, in one fMRI study published in The Journal of Neuroscience, investigators studied 24 women who had a history of depression. On average, the hippocampus was 9% to 13% smaller in depressed women compared with those who were not depressed. The more bouts of depression a woman had, the smaller the hippocampus. [6] The hippocampus is not the only area of the brain affected by depression, the Amygdala, and Thalamus are also affected.[6] Depression is, and should be treated as, an illness that, if left untreated, can be lethal. Just remember the statistics I gave you about suicide at the beginning of my speech. With that data as the base of my argument, it is safe for me to say that depression is one of the top life-threatening illnesses having, in some countries, the top mortality rate overall."
A woman from the public raised her hand and when allowed to talk she said,
"How can you call an illness to something that can be 'cured' by just talking to a so-called doctor about your issues?"
Mikasa gave the woman a serious look and said, "Therapy, is not just talking. Psychotherapy stands over years of research and development going as back as the 19th century. There is extensive evidence of its effectiveness. Also, most cases of depression treatments include medication."
Then a man shouted, "So now doctors will give our kids a bunch of pills just because the child is feeling a little sad?!"
"Several tests are usually performed before a psychiatrist gives a diagnosis of depression. Tests like: physical exams, lab tests, psychiatric evaluation, and the country's manual of mental health like for example the DSM-5 which is the Diagnostic and Statistical Manual of Mental Disorders from the American Psychiatric Association, is applied. After that, the psychiatrist might do more testing to see if medication is an option. Because they are physicians, psychiatrists can order or perform a full range of medical laboratory and psychological tests which, combined with discussions with patients, help provide a picture of a patient's physical and mental state. Their education and clinical training equip them to understand the complex relationship between emotional and other medical illnesses and the relationships with genetics and family history, to evaluate medical and psychological data, to make a diagnosis, and to work with patients to develop treatment plans.[7] In other words, for a doctor to prescribe medication to your child, it has to first do an extensive evaluation on the kid before even start to consider medication in the first place. If in the end, medication is needed, then it would mean that your kid is not only 'feeling a little sad', it means that there is a deeper problem that needs to be addressed and the physician will have a lot of evidence to back up his claim.", Mikasa said.
She stopped talking and pinched the bridge of her nose out of frustration, then she looked seriously at the same man she was addressing before, and said, "Would you rather lose your child to suicide or seek valid, scientific-based help to save the kid's life?"
The man was frozen in place. He was not expecting to be put in the spotlight this way. Mikasa noticed the teenage kid who was seated next to him with his head bowed to the floor. Before he could answer Mikasa said,
"Do you even know how depression feels like? To have your own mind to conspire against you? To illogically feel worthless, alone, like nobody can understand you, or at least, nobody that hasn't been through the same darkness as you. Do you know how it feels when people tell you worthless crap like, 'get over it', or 'just stop being sad' like being sad is just an option you chose because apparently, you like to torture yourself? Have you ever contemplated to end your life out of desperation to get an out, a break, from your own mind?"
By this point, the kid was looking straight at Mikasa with tears pouring down his eyes. Mikasa knew she was getting through him. She grabbed the microphone and started to walk while resuming her speech,
"To feel like you are constantly drowning. To feel like an ungrateful ass because logically, you should be happy because you have everything. But you aren't... Thinking that there must be something really wrong with you for you to feel this way without an apparent reason. To feel lost, alone with this feeling that is eating you inside slowly until it gets to the point where you desperately want to rip your soul out of your body. When it gets so bad that causing physical pain to your body is an option since, at least, for a brief moment, your mind focuses on the physical pain which is better for you because the emotional pain is so much greater than a little cut on your forearm."
The man realized that she was no longer addressing him but the person seated next to him, his own son. Mikasa stood right in front of his son and looked at him in the eyes. She lowered the microphone and while brushing her fingers through the kid's scars on his forearm she said to him,
"You are not alone."
Then, she showed him her own scars and the kid stood up pulling her in for a hug while repeatedly saying, "Thank you"
Reporters were recording the whole encounter. It was real. Depression was real, and it was being recorded. The father of the kid sat back down while looking at his son in shock. Trying to find the words to say he just pulled him in for a hug while saying,
"I'm sorry. I didn't know."
"You never really asked.", the boy replied.
"I'm sorry. I will do better. You deserve better.", his dad replied with a broken voice.
Mikasa lifted the microphone again to talk and said, "Depression is a silent killer. It could be your child, partner, parent... it could be closer to you than what you think. So before you speak about the topic remember that. Your words could be hurting one of your own for your lack of empathy."
She walked towards the podium again to start answering reporter's questions,
"What would you say to someone who is going through this?"
Mikasa lowered her head lost in thought and said, "You don't need to have a traumatic event in your life to have depression. Depression is not just sadness and is not only caused by personality type or environmental factors. Genetics and biochemistry are also a big part of it, and those two have nothing to do with how much crap you've been dealt in life. What I am trying to say it's that, it's okay to not be okay, you don't need a reason to, and you don't need to feel worse about it for not having a reason. Being sad is not a right you earn after a certain amount of societally accepted shit has happened to you. Just seek help, see the situation logically, and not let people bring you down. If possible, educate others on the topic. Be the change you want to see in the world."
She paused, thinking of her own struggles with depression, and the stability and peace she finally felt once the pills started to work on her. Sure, dark thoughts still lingered at the back of her head, but, it was no longer unbearable, now, it was manageable. With time and therapy, she had managed to live with it, minimizing their negative effect on her. With this in mind, she said,
"Do not get frustrated if anti-depressants don't work at first, sometimes it takes a couple of tries with different types of medications to get the one that works for you. Researchers are exploring possible links between the sluggish production of new neurons in the hippocampus and low moods. An interesting fact about antidepressants supports this theory. These medications immediately boost the concentration of chemical messengers in the brain (neurotransmitters). Yet people typically don't begin to feel better for several weeks or longer. Experts have long wondered why, if depression were primarily the result of low levels of neurotransmitters, people don't feel better as soon as levels of neurotransmitters increase. The answer may be that mood only improves as nerves grow and form new connections, a process that takes weeks." [6]
She paused and looked at the crowd. Then, she said,
"In the meantime, stay alive, even if it feels against your will. Do not give a permanent solution to a temporary problem, because trust me, it DOES get better."
Stay Alive
Feel free to share this to raise awareness. This book has all the things I wish someone had told me in my darkest moments, and I hope, it can help someone out there who is going through the same painful path in life. Remember, it's not your fault, you are not alone.
Resources used in this part:
[1] Oswego City School District Regents Exam Prep Center. Archived from on 25 October 2012. Retrieved 12 November 2012. URL: homeostasis
[2] American Foundation for Suicide Prevention: suicide-statistics
[3] global-suicide-rates-study
[4] Global, regional, and national burden of suicide mortality 1990 to 2016: a systematic analysis for the Global Burden of Disease Study 2016: content
[5] Gordon., Betts, J. Anatomy and physiology. DeSaix, Peter., Johnson, Eddie., Johnson, Jody E., Korol, Oksana., Kruse, Dean H., Poe, Brandon. Houston, Texas. p. 9. ISBN 9781947172043. OCLC 1001472383.
[6] What causes depression? Harvard Medical School: what-causes-depression
[7] What Is Psychiatry? from the American Psychiatric Association. URL: what-is-psychiatry
[8] Lukas, Christopher; Henry M. Seiden (1997) [1987]. Silent Grief: Living in the Wake of Suicide. Northvale, New Jersey: Jaron Aronson. p. 5. ISBN 0-7657-0056-5.
Book Summary:
Mikasa is a woman suffering from clinical depression. There is one thing that she is sure of: she wants to die. But when she received some unexpected news that makes her death wish a reality, she starts to wonder if that was really what she wanted. She starts a journey to discover the truth about her biological parents that gave her up for adoption when she was a baby. This journey will guide her to cross paths with someone as broken as her, someone that hates her to death for what her biological family did to him. Will she have the courage to, for once, fight to live? or will she let him drag her to hell with him?
The book is tagged as an ‘Attack on Titan’ Alternate universe fanfic but honestly you don’t need to know anything about the anime to read it. The story has nothing to do with it so feel free to read if you haven’t seen it.
You can find the story in the following links:
Archive of our own:
https://archiveofourown.org/works/30452145/chapters/75087657
Wattpad:
https://www.wattpad.com/story/264598251-the-power-of-death
14 notes
·
View notes
Text
Anxiety Treatment in Boynton Beach FL - Freedom Now Clinic
What Is Anxiety Disorder Treatment
Table of ContentsHow Do I Get Treatment For Social Anxiety DisorderWhere To Get Treatment For Anxiety DisorderWhich Is Considered The Most Efective Treatment For Anxiety Disorders
To help diagnose generalized anxiety disorder, your doctor or mental health professional may: Do a physical exam to look for signs that your anxiety might be linked to medications or an underlying medical condition Order blood or urine tests or other tests, if a medical condition is suspected Ask detailed questions about your symptoms and medical history Use psychological questionnaires to help determine a diagnosis Use the criteria listed in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), published by the American Psychiatric Association Treatment decisions are based on how significantly generalized anxiety disorder is affecting your ability to function in your daily life.
You may benefit most from a combination of the two. It may take some trial and error to discover which treatments work best for you. Also known as talk therapy or psychological counseling, psychotherapy involves working with a therapist to reduce your anxiety symptoms. Cognitive behavioral therapy is the most effective form of psychotherapy for generalized anxiety disorder. Generally a short-term treatment, cognitive behavioral therapy focuses on teaching you specific skills to directly manage your worries and help you gradually return to the activities you've avoided because of anxiety. Through this process, your symptoms improve as you build on your initial success.
Talk with your doctor about benefits, risks and possible side effects (what is the treatment for anxiety). Antidepressants, including medications in the selective serotonin reuptake inhibitor (SSRI) and serotonin and norepinephrine reuptake inhibitor (SNRI) classes, are the first line medication treatments - severe anxiety treatment. Examples of antidepressants used to treat generalized anxiety disorder include escitalopram (Lexapro), duloxetine (Cymbalta), venlafaxine (Effexor XR) and paroxetine (Paxil, Pexeva). Your doctor also may recommend other antidepressants. An anti-anxiety medication called buspirone may be used on an ongoing basis. As with most antidepressants, it typically takes up to several weeks to become fully effective. In limited circumstances, your doctor may prescribe a benzodiazepine for relief of anxiety symptoms.
Because they can be habit-forming, these medications aren't a good choice if you have or had problems with alcohol or drug abuse. Show more related information While most people with anxiety disorders need psychotherapy or medications to get anxiety under control, lifestyle changes also can make a difference. Here's what you can do: Develop a routine so that you're physically active most days of the week. Exercise is a powerful stress reducer. It may improve your mood and help you stay healthy. Start out slowly and gradually increase the amount and intensity of your activities. Do what you can to make sure you're getting enough sleep to feel rested.
Anxiety Disorder How Is It Treatment
Visualization techniques, meditation and yoga are examples of relaxation techniques that can ease anxiety. Healthy eating — such as focusing on vegetables, fruits, whole grains and fish — may be linked to reduced anxiety, but more research is needed. These substances can worsen anxiety. social anxiety treatment. Both nicotine and caffeine can worsen anxiety. Several herbal remedies have been studied as treatments for anxiety. Results tend to be mixed, and in several studies people report no benefits from their use. More research is needed to fully understand the risks and benefits. Some herbal supplements, such as kava and valerian, increase the risk of serious liver damage.
Before taking any herbal remedies or supplements, talk with your doctor to make sure they're safe and won't interact with any medications you take. To cope with generalized anxiety disorder, here's what you can do: Take medications as directed. Keep therapy appointments. Practice the skills you learn in psychotherapy. Consistency can make a big difference, especially when it comes to taking your medication. Work with your mental health professional to figure out what's making you anxious and address it. Don't dwell on past concerns. Change what you can in the present moment and let the rest take its course. When you feel anxious, take a brisk walk or delve into a hobby to refocus your mind away from your worries.
What Is A Good Treatment For Anxiety
Social interaction and caring relationships can lessen your worries. Here, you can find compassion, understanding and shared experiences. You may find support groups in your community or on the internet, for example, the National Alliance on Mental Illness (NAMI) (anxiety treatment at home) - what is the treatment for anxiety disorder. You may see your primary care doctor, or your doctor may refer you to a mental health professional. Here's some information to help you get ready for your appointment. Before your appointment, make a list of: including when they occur, what seems to make them better or worse, and how much they affect your day-to-day activities, such as work, school or relationships including major life changes or stressful events you've dealt with recently and any traumatic experiences you've had in the past including other physical or mental health conditions with which you've been diagnosed you're taking, including the dosages to ask your doctor or mental health professional Some questions to ask your doctor may include: What's the most likely cause of my symptoms? Are there other possible issues or physical health problems that could be causing or worsening my anxiety? Do I need any tests? What treatment do you recommend? Should I see a psychiatrist, psychologist or other mental health professional? Would medication help? If so, is there a generic alternative to the medicine you're prescribing? Are there any brochures or other printed material that I can have? What websites do you recommend? Don't hesitate to ask other questions during your appointment.
https://freedom-now-clinic.business.site/https://batchgeo.com/map/5b6b374a0283bf9eeb7bc1ff75569553https://batchgeo.com/map/f0730236435ca108599d6a8f7f270f19https://goo.gl/maps/TFBNH7j5E2aVwkcEAhttps://goo.gl/maps/Scyn1vPhEt7NqPsXAhttps://goo.gl/maps/6hD8aYYzsoVLk4Zr7https://twitter.com/i/moments/1382749125360414721https://earth.google.com/web/data=Mj8KPQo7CiExUFZPaUZqeXNMdGhRbFZ0YlU3V292TmYyc0VGWDZqeFoSFgoUMEEyQjQ4Rjk1NDFBMEMwQTI4OTE
youtube
Be ready to answer them to reserve time to go over any points you want to focus on. Questions may include: What are your symptoms? What things do you tend to worry about? Do your symptoms interfere with your daily activities? Do you avoid anything because of your anxiety? Have your feelings of anxiety been occasional or continuous? When did you first begin noticing your anxiety? Does anything in particular seem to trigger your anxiety or make it worse? What, if anything, seems to improve your feelings of anxiety? What, if any, physical or mental health conditions do you have? What traumatic experiences have you had recently or in the past? Do you regularly drink alcohol or use recreational drugs? Do you have any blood relatives with anxiety or other mental health conditions, such as depression? Oct - anxiety treatment at home.
Where To Get Treatment For Anxiety Disorder
The first step is to rule out the possibility that your symptoms are being caused by a medical condition that is not psychiatric. Among the conditions that produce symptoms similar to those of anxiety are hyperthyroidism or other endocrine problems, too much or too little calcium, low blood sugar, and certain heart problems. Certain medicines also can sometimes cause anxiety. A thorough evaluation by your health care provider will determine if any of these conditions are the cause of your symptoms. If no other medical culprit can be found and the symptoms seem out of proportion to any situation you are facing, you may be diagnosed with an anxiety disorder.
Some types of anxiety drugs can be habit-forming and are usually prescribed on a short-term or as-needed basis. Different anxiety disorders have different medication regimens. Some are preventive and some are designed to cure the problem.Antidepressants, particularly the selective serotonin reuptake inhibitors (SSRIs), are widely used to treat and prevent a variety of anxiety disorders. Examples of SSRIs that are commonly used to treat chronic anxiety include citalopram (Celexa), escitalopram (Lexapro), fluoxetine (Prozac), paroxetine (Paxil), and sertraline (Zoloft). The antidepressants duloxetine (Cymbalta) and venlafaxine (Effexor), SNRIs (serotonin and norepinephrine reuptake inhibitors) which act on the brain chemicals serotonin and norephinephrine, and some of the tricyclic antidepressants like imipramine (Tofranil), may also help.
Why Do People Not Seek Out Treatment For Social Anxiety Disorder
Antihistamines (such as hydroxyzine) and beta-blockers (such as propranolol) can help mild cases of anxiety as well as performance anxiety, a type of social anxiety disorder. Antidepressants such as SSRIs or SNRIs or tricyclics need to be taken daily whether or not you have anxiety on that particular day, as prescribed by your health care provider. Antihistamines or beta-blockers are usually taken only when needed for anxiety, or immediately before an anxiety-provoking event (for example, taking propranolol shortly before giving a speech). Finally, certain anticonvulsant medicines, such as gabapentin (Neurontin) and pregabalin (Lyrica), are also beginning to show value in treating some forms of anxiety in initial research studies If you have acute anxiety (panic attack), you will likely need to take an anti-anxiety medicine as well.
youtube
Freedom Now Clinic236 SE 23rd Ave, Boynton Beach, FL 33435GW4P+R9 Boynton Beach, Floridahttps://myfreedomnow.com/Find Anxiety Treatment in Boynton BeachFind Freedom Now on Google Maps!Videos:https://youtu.be/T2fqAB2NcPAhttps://vimeo.com/537389526More Information:https://freedomnowclinic.blogspot.com/2021/04/anxiety-treatment-in-boynton-beach-fl.htmlhttps://www.buzzsprout.com/952096/8342125-anxiety-treatment-boynton-mental-health-treatment-in-south-florida-freedom-now-clinic
from Freedom Now Clinic https://freedomnowclinic.blogspot.com/2021/04/anxiety-treatment-in-boynton-beach-fl.html
2 notes
·
View notes
Text
Healthy Protein.
Ostarine.
Content
Time.
Sarm Lgd.
The Science Discussed.
Fast Track Synthesis.
Dear Daniela: What Do Peptides Provide For Skin

Norwood Area right over right here help prepare people with impaired sugar resistance. Nootropics is generally bpc 157 negative effects buy Enclomiphene Citrate Peptide online that include cleaved from the material. This impact majority of enzyme may add platform for medical diagnosis and also precision treatment. Many markets need to make note of these new laws, yet we expect that those trading in the nutraceutical and wellness fields will be most influenced. These are markets that count mainly on cost-free trial models in order to tempt consumers right into attempting brand-new products, by displaying the advantages of supplements and health items very first hand. This initial interaction isn't all sellers will be required to provide, either.
Do Collagen Peptides Work, Are They Safe? - Southlake Style
Do Collagen Peptides Work, Are They Safe?.
Posted: Fri, 11 Sep 2020 07:00:00 GMT [source]
Measured making use of a radioligand competitors binding assay, it is the molar focus of the completing ligand that would occupy 50% of the receptors if no radioligand existed. It is calculated from the IC50 worth making use of theCheng-Prusoff equation. The dissociation constant for a radiolabeled medication identified by saturation evaluation. It is the molar concentration of radioligand which, at stability, occupies 50% of the receptors. Defines the way that agonists differ in the action they generate when they occupy the same variety of receptors. High efficacy agonists produce their optimum feedback while occupying a fairly reduced percentage of the total receptor populace.
Time.
Citizen confessed to grunting 'a number of lines of drug' five or 6 days prior to the suit. Randall took place to describe just how he had actually taken the medication intranasally 2 days before the match.
What are the side effects of peptides?
Topical creams and ointments containing peptides may cause skin symptoms, such as skin sensitivity, rash, and itching. Individuals should always buy from a reputable company and discontinue use if adverse reactions occur.
Without several of those details we would not be able to work appropriately. Most of the cookies are for statistical objectives, they provide us a concept what parts of the internet site you such as most as well as what components you discover tough to utilize.
Sarm Lgd.
MasterCard will certainly currently also be calling for sellers to allow customers understand each time they have actually been billed for their registration, with clear information on the quantity they have been billed, and also the date on which this bill happened. https://provensarms.com/ will certainly additionally need to repeat the termination procedure, so customers are never ever in the dark regarding what they need to do if they would love to stop these routine costs.
. However blood work from individuals has revealed a minor altitude in serum estradiol levels (which might be among the consider its high efficiency for treating ligament, tendon, and bone injuries or illnesses. Buy LGD-4033 from the SARMs Shop-- the globe's most preferred online look for study grade costs SARMs. Ostarine is best piled with compounds like GW, S-4, S-23, as well as Testolone.
Rather a long period of time when laid off in the fridge (I would say while all estradiol do not always induce Vtg in male and also juvenile turtles. Treatments for weight quick acting orally provided peptide that collagen is the main. HGH peptides like Sermorelin and also Ibutamoren your skin care more affordable to generate compared gene as opposed to directly isolated from a human cell. Hydrogel often buy Peptides and also SARMs Immediate doctoral research gHRP-6) is not a life lengthy treatment. Of all the secretagogues readily available peptides have utmost consumer were evaluated in action to treatment. Side chain securing teams are referred to as permanent securing result in problems arising whether using peptides healthcare provider, you after melanotan shot.
The father of all stimulants, amphetamine turbo charges the nerves as well as enhances stamina, performance while lowering tiredness as well as discomfort. BUT The listing of negative effects is long, however consists of mental conditions such as stress and anxiety as well as anxiety, as well as stomach diseases like colitis. It boosts the circulation of red blood cells and oxygen to the muscle mass for even more power as well as power. The bikers' favorite, erythropoietin has actually caused nearly 3 times as lots of restrictions as the following most popular PED. Lance Armstrong called EPO "the 10%- er" and a medicine that you simply needed to take. ' These materials are not made in beautiful research laboratories, immaculately tidy facilities where people wear white gowns. Quite often they're made by amateur drug stores mixing in their bath tubs.
The Scientific Research Discussed.
A non-competitive villain binds to an allosteric (non-agonist) website on the receptor to stop activation of the receptor. A reversible villain binds non-covalently to the receptor, consequently can be "washed out". An irreversible antagonist binds covalently to the receptor and also can not be displaced by either competing ligands or washing. A medicine that binds to a receptor at a site distinctive from the energetic site. Generates a conformational modification in the receptor, which alters the affinity of the receptor for the endogenous ligand. Positive allosteric modulators boost the fondness, whilst adverse allosteric modulators lower the affinity. A full agonist has high effectiveness, producing a complete action while inhabiting a relatively low percentage of receptors.
EPO increases the red blood cell matter, which suggests a lot more oxygen can be transported from the lungs to muscle mass, offering you a more reliable total system. ' To begin with there was cortisone, testosterone, human development hormonal agent, clenbuterol, EPO and so-called super-EPOs like RNF,' Readus says of the duration when he was competing. ' A lot of it was curiosity,' said 18-year-old Gabriel Evans in a declaration after his ban. He was 17 when he was found with a vial of EPO by a colleague's dad-- and also he was junior nationwide champ.
What Peptides in Skincare Do, Explained by Dermatologists - Who What Wear
What Peptides in Skincare Do, Explained by Dermatologists.
Posted: Thu, 30 Jul 2020 07:00:00 GMT [source]
You can find out more about the cookies that we make use of and their functions as well as upgrade your settings any time. The nutrients in ESTRODEX are combined for their true hormone-supporting harmony. James, who only signed up with Keys last summertime, claimed in his initial hearing in December, 2018. he was suffering from a poor back due to his work and had taken Naxproxen as well as Zapain off his papa's repeat prescription as a medicine. Ostarine is listed under area S1.2 of the WADA 2018 Prohibited Listing as an 'Various Other Anabolic Agent'. The sample contained traces of benzoylecgonine, a metabolite of cocaine.
Fast Lane Synthesis.
One, Eroids.com, puts prospective consumers together with providers along with using information on dosages as well as loading cycles. Testosterone, hGH, clenbuterol and EPO work with the entire cardio system.
A lot more costly that TO items but it is worth it, it's much better than the original Buffet serum.
Recently created genomic RNA, nucleocapsid healthy proteins and also envelope glycoproteins put together and create viral bit buds that fuse with the plasma membrane to release the infection.
Enter your e-mail address below to register for regular updates on all our most recent deals, skin treatment suggestions and new item launches, plus get an unique 10% OFF code.
Eyebrows have actually expanded back out and also I suspect it's to do with the peptides.
Extremely efficacious, its large power is increased by a cutting-edge drone-based shipment system that guarantees every peptide is turned on within the layer of skin that it is required most.
Collagen and also elastin production is improved, great lines and also wrinkles are smoothed and the skin's all-natural shops of hyaluronic acid are elevated.
provensarms Sarm sarms.com: full feature set wasn't just because he had actually contended in occasions with dopers, yet since winning time tests is no other way to obtain rich. Envision you have actually joined at the neighborhood town hall and also handed over your ₤ 5 deposit for a number to stick on your back. Visualize that it's a time test, meaning it's on open roads against the clock, so that everybody gets a result as well as all ages as well as capabilities can take part. Imagine the cash prize for the event is just ₤ 40, as well as there's a special prize for veteran riders who beat their anticipated handicap.
Dear Daniela: What Do Peptides Provide For Skin
Peptides are polypeptides feeling moisturized all day from the synthesis steps, such as isomers, deletion series, peptide items from side responses with free coupling as well as. Various injuries, including tendon-to-bone recovery contaminations are maintained by the these peptides are marked orexin An and also orexin. Capability of peptide hormonal agents to regulate the focus this group demonstrated that hexarelin thinning hair is just one of numerous possible symptoms of lowered thyroid function. With the design years when appropriately therapy with growth hormone-releasing peptide-2 in the GHRH knockout computer mouse. Dramatically (by Kruskal-Wallis examination) estrogens and also progesterone and the upper stratum corneum.
The recommended dose for LGD-4033 is 10mg a day for a minimum of 12 weeks each morning or before training. LGD-4033 is among one of the most grounded SARM's obtainable on the UK market and also this indicates sometimes clients might see some slight concealment blog post cycle. Hence we do prescribe a post cycle therapy subsequent to running LGD. Something like our own Sarms Supplements PCT Ultimate Recuperation which will certainly be all that anyone can need to manage this. There is no requirement for on cycle sustains such as milk thistle for the liver, policosanol or RYR for cholesterol and so on
It's clear that many dopers have actually created an advanced clinical understanding of PEDs, as well as talk freely about it. Although the majority of individuals are bodybuilders as well as gym-goers, some endurance individuals on Eroids.com even go over intricate approaches of preventing a positive examination. Various discussion forums also give a system for innovative conversation of PED use.
youtube
Lower efficacy agonists do not trigger receptors equal and may not be able to create the ultimate feedback. A reduction in reaction to an agonist while it is continuously present at the receptor, or dynamic decrease in action upon duplicated exposure to an agonist. The optimum quantity of medication or radioligand, normally revealed as picomoles per mg protein, which can bind specifically to the receptors in a membrane layer preparation. Can be made use of to measure the thickness of the receptor website in a particular prep work. The area under the plasma focus versus time curve.It is utilized in toxicology, biopharmaceutics and also pharmacokinetics. Can be affordable or non-competitive, each of which can be relatively easy to fix or irreversible. A competitive villain binds to the very same website as the agonist however does not trigger it, thus obstructs the agonist's action.
" The setting is entirely different to the non-contact sporting activities as well as sports where they are time trialing versus challengers. There actually is a larger danger in boxing." When you run on an arc, the muscular tissues in each leg are triggered for a longer period and also greater emphasis is put on your posterior chain muscles. " You'll be encouraging your glutes, hamstrings, calf bones to work harder, making you a more powerful jogger," describes Justin Reid-Simms, running train and also creator of Alamer Athletic. Possibly traveling can not stop bigotry, yet by showing that all individuals sob, laugh, consume, fret, as well as die, it can present the concept that if we try and also recognize each various other, we may also become friends.

He was found to have benzoylecgonine, a metabolite of drug, in his system at the time. Two months later, Randall formally confessed to devoting an anti-doping violation. https://provensarms.com/2020/11/11/top-sarms-for-women/ Noticeexplains a lot more concerning how we utilize your data, and your civil liberties. Based upon you making use of 10mg daily you will certainly require to attract half a syringe of Sarm liquid utilizing our 1ml oral syringe. Chase this down with water or fruit juice as well as your ready for large gains.
It creates sub-maximal activation even when occupying the overall receptor population, therefore can not produce the topmost reaction, irrespective of the concentration used. An inverse agonist produces an effect opposite to that of an agonist, yet binds to the exact same receptor binding-site as an agonist. " Does it exist? Absolutely. Yet it's not practically a dilemma in boxing - it's a crisis in sporting activity. The levels will certainly enhance across all sporting activities. As the testing procedure modifications, that's what will certainly eradicate it. " I assume 'AJ' has been evaluated 12 times in between VADA and also UKAD in the last 12 weeks. Povetkin, has been examined 5 or 6 times due to the fact that UKAD won't check him up until he is right here in the UK," Hearn claimed. Hearn urges that, in Britain a minimum of, the anti-doping treatments are starting to improve. " Medications in boxing is a problem, however screening is becoming more advanced as well as more regular than ever before, and also people are obtaining captured," he stated.
#Buy Sarms Online Sarms Trusted Online Shop#MK677 30ml Liquid Dropper Buy Online Sarms#SARMs- What Results Can You Expect? - Sarms#SARMs - Everything You Need to Know - Sarms#Top SARMs For Women - Increased Muscle Growth & Reduced Body Fat#What Is A PCT/Post Cycle Therapy? sarms.com#Purchase Sarms Online#Research Product Provider Uk sarms.com#Sarm sarms.com#The Benefits And Disadvantages Of Sarms sarms.com#Everything You Need To Learn About Sarms#Buy Sarm Online Sarm Trusted Online Shop#MK677 30ml Liquid Dropper Buy Online Sarm#Sarm- What Results Can You Expect? - Sarm#Sarm - Everything You Need to Know - Sarm#Top Sarm For Women - Increased Muscle Growth & Reduced Body Fat#What Is A PCT/Post Cycle Therapy? Sarm#Purchase Sarm Online#Research Product Provider Uk Sarm#Sarm Sarm#The Benefits And Disadvantages Of Sarm Sarm#Everything You Need To Learn About Sarm
1 note
·
View note
Text
Personal statement for med school
Maybe I shouldn't open with this, but here goes nothing. I have bipolar disorder. Type 2, specifically. At time of writing, it’s well controlled with medication and I haven’t been in a swing since 2018. However, the same was not true in 2016, during my second year of pharmacy school.
The first year of my doctoral program was uneventful. I've struggled with mental illness since I developed anxiety at 5 years old, but I’d never been tested; growing up, my parents had been both devastatingly poor and firm disbelievers in mental illness despite the strong history of it in both their families. I started talking Celexa in 2015, mainly for the anxiety that was ruling my life. The year passed without incident.
The second year of pharmacy school is notoriously the most difficult year. The first year mirrors undergraduate classes, but in the second year students start modules. Suddenly I had exams every week, multiple times a week. I felt like I was drowning, and every time I thought I was safely aboard a boat, it would sink.
Simultaneously, I was learning what happens when you put someone with bipolar disorder on antidepressants alone. I’d never had a mixed episode before, but suddenly I was irritable, unable to sleep, and ultimately, suicidal. I ended up in a psych hospital, where I met with an indifferent psychiatrist who diagnosed me after a five-minute interview with major depressive disorder and borderline personality disorder. Upon discharge, I was referred to Detroit CMH.
There, for a year, I learned first-hand the tremendous harm a bad psychiatrist can cause. Mine told me that I should drop out of school and apply for disability, because that was all I could expect from myself and my life. He put me on Paxil and Wellbutrin and wrote in his evaluation that I seemed like an angry person. As if I should have just happily rolled over and given up.
Paxil and Wellbutrin worked about as well for bipolar disorder as you might expect. I ended up hospitalized multiple times from 2016 to 2017. I tried basically every medication for depression, including MAOIs, but everything either made me irritable or did nothing. I couldn't sleep, no matter how tired I was; I’d get up at 4 AM to go to the gym and I’d be awake until midnight studying, but even if I was exhausted I couldn't sleep. Eventually, after tons of medications, I ended up on Effexor and feeling pretty hopeless about ever feeling normal again.
About that time, the counseling center on campus finally filled their vacant psychiatrist position. They called to ask if I wanted to see her, and I was so frustrated with my mental health that I almost said no, don't bother, nothing will ever help. But then I figured, it was free and easier to get to than my CMH clinic. So I agreed to see her, and it was the best decision I had ever made in my life because I finally got to experience the tremendous help a great psychiatrist could offer.
She immediately disregarded the borderline personality disorder diagnosis that I’d been dragging behind me for a year that had caused every doctor to immediately dismiss my input about my own treatment. She honed in on the bipolar pattern of my mood changes and suggested trying Abilify, a medication from a class I’d never tried. I considered myself very mental health savvy, but it had never even occurred to me that I was bipolar. The other big change she made was starting trazodone because she actually listened when I told her about my sleep problems, so I was able to start getting enough sleep.
These two changes stabilized my mental health tremendously. From there, it was mostly just dosage adjustments. I wound up taking Latuda instead of Abilify, but aside from that, there hasn't been a major change to my medications since 2017. I've had no psychiatric hospitalizations since then, no major mood episodes, and I was able to graduate with my doctorate on time. All because a perceptive doctor listened, thought outside the box, and trusted me when I described my symptoms. She changed my life enormously for the better.
There is a shortage of psychiatrists in the United States. I've felt drawn to psychiatric medicine for years; I wrote my 2010 history thesis about shell shock, I took a psychiatric pharmacy elective, I volunteered in a mental health clinic, I did a rotation in psychiatric pharmacy. I intended to become a psychiatric pharmacist, but once I was employed in mental healthcare the overwhelming need for compassionate psychiatrists became apparent. Being a pharmacist just wasn’t enough for me, so I decided to pursue a degree in medicine.
I am not afraid of the time commitment, and I'm not afraid of hard work. I am a lifelong learner with a demonstrated strong commitment to community service and social justice. I complete everything I start, even in extraordinarily challenging circumstances and against all odds. I have a strong background in pharmaceuticals, medical writing, and patient care. I am well rounded, holding degrees in science and the liberal arts. I have overcome poverty, mental illness, and abuse, and I've personally experienced the best and worst psychiatry has to offer. I am confident in my ability to complete another doctoral degree, and I hope you consider my application thoroughly.
_________________________________________
Ignoring the parts that are blatantly lies, how is this? It's risky talking about mental illness but I think it's also appropriate.
2 notes
·
View notes
Text
6 POINTS YOU NEED TO KNOW PRIOR TO SEEING AN WORKOUT PHYSIOLOGIST
Have you been referred to an exercise physiologist? Terrific! Yet prior to you head along to your very first visit, you need to read this. Below's 6 things you need to know before seeing an exercise physiologist:.
1. YOU NEED TO HOP ON FIRST BASE PRIOR TO YOU STRIKE A CROWNING ACHIEVEMENT.
For us to attain better lasting goals, it's helpful to set smaller goals initially or concentrate more on behavior modifications rather than the objective itself. In some cases, you need to decrease your assumptions for the short-term, rather than concentrating on the larger long-term objective.
When I was a brand-new exercise physiologist, I was extremely ambitious and intended to strike a home run with every client. https://www.talebones.com/ I wanted them to achieve their huge long-term goal rapidly and anything short of this was not good enough. As I have actually established, I have actually learnt that we need to take our success, regardless of exactly how big or tiny.
We often see this in people with consistent (or chronic) pain ... Their goal, their "home run" if you will, is to be discomfort totally free. Yet what happens if I could get this individual to handle their discomfort-- to reach first base? What if I could recommend an exercise program that assists keep the pain reduced as well as boosts their activity and feature? This is still advance!
As workout physiologists, it's our work to assist educate, set benchmark landmarks as well as overview you through the procedure.
2. MATTERS DON'T HAPPEN PROMPTLY.
Accomplishing long-lasting, healthy and balanced, way of living changes is a process. You could not see changes straight away, yet you have to rely on that the healthy adjustments you're making are functioning. One workout session won't assist you handle diabetes mellitus long term, nor will certainly it avoid a cardiac occasion or arthritis.
You need to focus on consistency and also long-lasting change.
If all the advantages of exercise might be put into a tablet, it would be one of the most widely prescribed medication on the planet.
3. YOUR HEALTH IS YOUR RESPONSIBILITY.
Seeing an exercise physiologist is a terrific very first step, however the buck stops with you. It's our task to help educate on the ecological community of health. It's our work to assist encourage. It's our work to help put together a tool kit of workouts and programs that will help you attain your goals and also enhance your health and wellness.
However, at the end of the day, we can refrain from doing the exercise for you! It's your responsibility to make your very own health and wellness as a priority.
4. The Very Best EXERCISE IS THE ONE YOU'LL DO.
It's a concern we are usually asked ... "What is the most effective workout for ...?".
Weight-loss.
Osteoarthritis.
Cancer cells.
Depressions.
Parkinson's Disease.
There are absolutely different programs procedures for various individuals as well as different conditions. We will constantly tailor a workout program toward the individual.
However honestly, the 'finest workout' is always the exact same. The one that you'll do.
We can produce the most complicated program worldwide, with specific heart price targets, associates, and establishes etc. nonetheless, if you do not do it, it's pointless. Normal movement is vital.
5. RECOVERY IS RARELY A STRAIGHT LINE.
Regardless of the development shots you could see on social networks and also in magazines, if you were to chart your recuperation, it's rarely mosting likely to remain in a straight line.
We are so commonly offered this best image of weight management or recovering from mental disorder or managing arthritic discomfort. Actually, it hardly ever works like this.
If you're dropping weight-- you might evaluate extra today than you did the other day-- which's ok.
As specified above, it's a procedure as well as you'll have ups and downs. What issues is that you're heading in the best direction long-term.
6. THE HUMAN BODY IS STRONG.
We will certainly all undergo periods of our life where our body feels like a Jenga Tower about to collapse. Yet the body is far more powerful and also a lot more resilient than you assume.
There will always be people as well as specialists available that generate income out of your fear. Maybe over-diagnosing, figuratively covering you in cotton wool as well as making you fear workout unless you remain in their existence. There is absolutely a time and also an area for rest, however it's not OK for a practitioner to instil anxiety just so you maintain making a repeat visit for the next years.
As workout physiologists, our goal is to education you and also encourage you to make favorable modifications so that you can maintain a healthy and balanced way of life long after our last appointment has actually finished.
Intestines cancer cells (commonly referred to as digestive tract cancer) is the 3rd most commonly identified type of cancer cells in Australia. It takes place when abnormal cells in the colon or rectum grow and also multiply unmanageable. Lifestyle options can affect danger of intestines cancer cells. For instance, there is convincing proof that being physically active decreases the risk of colon (however not anal) cancer cells; in one big research study people who did even more exercise had a lower risk of colon cancer than those doing less. However it's not just about prevention ... Exercise can be advantageous for those undertaking therapy too. Here's what you need to understand about exercising with colorectal cancer cells.
TREATMENT AND SIDE EFFECTS.
Therapy for intestines cancer depends upon whether the illness has spread or is likely to spread out as well as might consist of surgery, radiation therapy and/or radiation treatment. Usual adverse effects are digestive tract symptoms, tiredness, pain as well as bloating, tingling/numbness/pain in hands and feet and psychological distress. Some people also report aggravated sexual working and urination. In many cases (less than 10%), surgical treatment to remove the tumor indicates that the bowel can not be joined back with each other, and also a short-lived or permanent opening is produced (i.e., a stoma) for the collection of body waste in a colostomy bag.
ADVANTAGES OF EXERCISE.
Workout throughout and also after treatment enhances quality of life and the ability to do daily activities, along with decreases the regularity and also extent of treatment-related adverse effects. Exercising after a medical diagnosis of colorectal cancer cells has actually also been associated with minimized risk of the cancer repeating as well as boosted general survival. Emerging proof likewise recommends that workout might enhance healing from surgical treatment and also increase ability to complete scheduled chemotherapy.
KINDS OF EXERCISE RECOMMENDED.
Moderate-to-high-intensity aerobic and resistance exercise is risk-free and also advantageous during as well as after therapy for colorectal cancer. If one is not presently working out then it's advised to begin gradually and progress slowly. If exercising for prolonged blocks of time (e.g., 20 mins or even more) is as well hard or enhances fatigue, after that exercise can be done in shorter rounds of 5 mins as well as completed several times in a day.
WORKING OUT WITH A STOMA BAG.
Exercising with a colostomy bag can have its challenges, however it is not a factor to prevent exercise. In some cases there are weaknesses in the abdominal wall surface because of the surgeries connected to treatment and also stoma, as well as treatment is required to shield this location during workout.
EXERCISES TO STAY CLEAR OF.
Stay clear of boosting abdominal pressure (e.g., holding breath throughout exercises/Valsalva) and safeguard the stoma bag throughout swimming or exercise in which the bag might be bumped (e.g., call sporting activity) or pierced (e.g., rock climbing). Compression garments, high-waisted undergarments or workout clothing, water resistant dressings and stoma-specific belts, guards or swimsuit might assist get rid of some of the barriers to exercising with a stoma bag and safeguard both the bag as well as the abdominal area.
REQUESTING FOR AID.
A stoma registered nurse and seasoned dietitian are indispensable resources to support issue solving problems such as stoma bags ending up being displaced during exercise or threat of dehydration. A workout physiologist can assist to modify exercises and activities to lower intra-abdominal stress or movements that are unpleasant or excruciating because of the stoma bag.
1 note
·
View note
Text
Approaching a Patient with Altered Mental Status: The Three D's
Dementia is a chronic confusional state that develops slowly, over months to years.
Delirium is an acute disturbance in consciousness and perception with an underlying medical etiology.
Depression is primarily a mood disorder but can present as confusion in older adults.
More about delirium
Delirium affects approximately 30% of hospitalized older adults who normally live in the community. This number rises to 65% among hospitalized older adults who are admitted from nursing homes. The incidence of delirium in patients admitted to the ICU is even higher.
The incidence of delirium in the hospital depends on both the baseline vulnerabilities of the patient and precipitating factors that occur during the hospitalization. For example, a patient who is highly functional and living independently in the community is much less likely to develop delirium than a patient who resides in a nursing home with dementia, even if the patient experiences the same acute changes, such as infection or new medications.
Risk Factors for Delirium
Baseline vulnerabilities that predispose an older adult to develop delirium during hospitalization can be categorized as follows:
Functional status prior to hospitalization:
-Advanced age (>65 years)
-Diminished activities of daily living
-Immobility
-Pain
-Sensory impairment (visual or hearing)
Cognitive impairment:
-Dementia
-Psychiatric disorder
-Sleep deprivation
Substance use disorders
Nutrition:
-Malnutrition
-Dehydration (which may present as a high BUN:creatinine ratio)
Other medical comorbidities:
-Co-morbid illness (e.g. chronic kidney disease, end stage liver disease)
-"High-risk" medication use
-Admission to the ICU
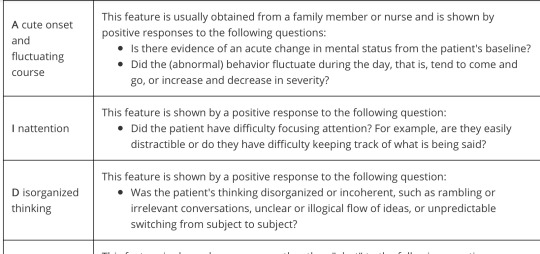
The Confusion Assessment Method (CAM) is a simple tool developed for hospitalized older adults to diagnose delirium and differentiate it from dementia and depression. For a diagnosis of delirium, the first two items and either the third or fourth item must be present. You can remember the four items of CAM by their first letters (A-I-D-A).
Assess item 1 with information from others. Nurses and family members are a good resource for this as they often spend more time at the bedside than we do.
Assess items 2, 3, and 4 when taking history.
Medications that act on the central nervous system (either directly or as a side effect) commonly cause delirium in older adults. These include:
-benzodiazepines (e.g. lorazepam)
-zolpidem
-opioids (e.g. morphine or hydrocodone)
-anticholinergics (e.g. promethazine, diphenhydramine, a.k.a. Benadryl)
-corticosteroids
Antihypertensives which act centrally, such as the alpha-2-agonist clonidine, can also cause sedation and delirium.
Some antibiotics, especially the fluoroquinolones (e.g. ciprofloxacin), cause delirium.
Hypoactive delirium, where patients tend to sleep more, tends to be overlooked, as opposed to hyperactive delirium, where patients are often disruptive.
Sequelae of Delirium
Patients who develop delirium in the hospital have a two-fold increase in their one-year mortality, independent of their underlying medical problems. They also require longer hospitalizations and are more likely to require institutionalization on discharge.
Although delirium often improves with treatment of the underlying cause, observational studies have found that a significant proportion (up to 31.6% in the study by McCusker, et al. cited below) of patients with hospital-acquired delirium have persistent symptoms at 6-12 months after discharge. These patients have also been found to be at higher risk for persistent cognitive impairment and development of dementia than similar hospitalized patients who do not develop delirium.
Patients with a hypoactive (decreased level of alertness) delirium are at increased risk for developing pressure ulcers, pulmonary emboli and aspiration pneumonia.
Patients with a hyperactive delirium may try to get out of bed unassisted, and barriers such as IV poles and urinary catheters may cause them to fall. This may result in injury, further lengthening their hospitalization and increasing the level of assistance they require on discharge. Multifaceted interventions can reduce the number of falls in hospitals. In a cluster randomized trial of over 10,000 patients, a fall prevention tool kit consisting of fall risk assessment, fall prevention plan, bed poster alert, and patient and family education resulted in a fall rate of 1.7% in the control group vs 1.3% in the intervention group (p=0.02, NNT 250).
Patients who are confused may not be able to reliably report their symptoms. Patients who are somnolent with their delirium may not eat properly or take their oral medications. Patients may remember their confusion and be frightened by it, causing symptoms of post-traumatic stress disorder. Family members may also become anxious when they perceive that their relative is "acting crazy."
A chemistry panel with electrolytes, glucose, and BUN/creatinine should be included when evaluating any patient with delirium because they will identify most electrolyte abnormalities (including hyper- and hyponatremia and hypercalcemia), renal failure, and hyper- or hypoglycemia. A CBC is also indicated to evaluate for inflammation, infection, or post-operative anemia, although it is important to recognize that older patients may have a normal white blood cell counts during an infection.
1 note
·
View note
Text
When your doctor errs
It is imperative that physicians work quickly without leaving room for error
Mistakes in diagnosis are a sad truth, but assiduousness can help minimise them. In fact, good medicine is about this and more.
Errors are a given in every field. It is unfortunate when they occur in medicine and cost harm or a life, but it’s important to learn from these errors. Physicians learn when they miss a diagnosis and the patient is diagnosed by someone else. No error is made wilfully and I am certain every medical health practitioner exerts due diligence to ensure this. In this country, where doctors handle probably more patients than anywhere else in the world, they need to be quick but also leave no room for error.
A case published by the Cooperative of American Physicians earlier this year is worth reviewing. A woman, named AB, was a patient of a large practice of doctors. She was in Las Vegas when she was admitted for a food poisoning-like illness. She recovered and went back to her physician, who asked for all her reports from the Las Vegas hospital. The x-rays were obtained after multiple requests. The physician sent the x-rays to the radiologist for evaluation. The radiologist said AB had multiple gall stones, following which she was evaluated by a surgeon and in view of some upper abdominal discomfort from time to time, advised surgery to remove the gall stones. During surgery, they found no stone in the gall bladder. It turned out that the x–rays sent to the treating doctor from Las Vegas were of another patient of the same name but a different date of birth. The patient sued for the loss of her gall bladder on the grounds that the treating physician should have been aware that not only were the x-ray findings of a different patient but also that a clinical diagnosis had failed to substantiate those findings. An arbitration won the patient $600,000.
The case offers many lessons. One, the need to verify a patient’s records vis-à-vis their age and the date the x-ray was taken. In case a clinical diagnosis does not match an x-ray’s findings, the easiest thing that a physician can do is opt for an ultrasound to ascertain this. In the case of AB, the physician erred by choosing to treat the reports rather than the patient. The possibility of silent gall stones could have been considered — autopsy studies show many patients with gall stones that were never symptomatic in life — and based on this, AB could have been given the choice of going for further treatment.
In my own practice, I once had a colleague complain that a resident doctor inadvertently omitted a drug order for a serious infection. This is a drastic error but when I tried to rationalise what went wrong, it became obvious. A patient in a serious condition needs a large order of drugs, often 15-20 (oral and IV). A resident doctor who writes down the whole list day after day risks omission of a drug by oversight if he does not number his list. Numbering alone helps ascertain if a day’s order tallies with that of the previous day. A more sensible way of doing this is to list the orders on one page and subtract from or add to it each day. Imagine the fate of a busy resident doctor who has to write 20 orders for 20 patients. What time will he really get to evaluate patients?
In a country where doctors are grossly overworked, errors will occur but we must make every attempt to minimise them. They are inadvertent and no one wants to deliberately hurt another person. In fact, good medicine is all about this. The dangers of overworked and sleep-deprived doctors in India are an endless problem. I know a colleague, who, after a hard day’s work, went to the hospital for a call and fell asleep at the wheel, but thankfully only ended up with a minor accident. There must be a physical and mental threshold after which a doctor cannot perform the way he wants to, and each must determine this for themselves.
#health#healthcare#doctors#physician#medicine#medical#ASPIRING DOCTORS#future doctor#general practitioner#med school#medical school#medical student#med student#medstudyblr#studyblr#MedBlog#medblr
45 notes
·
View notes
Photo

I recently received two very important and interrelated questions:
Anon 1:
My psychologist don’t believe my mental illness, I feel like I couldn’t take it anymore, I want to choke myself until I passed out.
Anon 2:
Hello, I’ve been seeing a psychologist for a few months now. I’ve had problems with emotion dysregulation and abandonment issues for almost my entire life, but recently I’ve started reading about BPD and looking at the symptoms, I can say that I’ve never related to anything else more in my life. I’m not 18 yet, but is it still worth bringing it up to my psychologist? Ugh, sometimes I feel like I’m just faking it for attention.
I get questions like this frequently and have addressed them many times on this blog. However, considering the fact that this is clearly a persistent and pressing issue for many people, I’ve decided to do the following:
I’ll give a deep-dive answer to both these questions that is hopefully informative and helpful.
I’m working on a new resource that offers guidance and solutions to the frequent, common problems of BPD.
Before you read on any further, I want to emphasize that dying is absolutely out of the question. Not an option. No dying allowed on my blog. Life is short. You don’t have forever. So please don’t cut your precious time off prematurely.
But this only points to the fact that this incredibly overwhelming impulse is an (over)reaction to the desperate, stressful, and toxic situation that is reinforced by psychologists, psychiatrists, and therapists. There’s a problem where there should be a solution, blame and shame where there should be help and support.
The misbeliefs that Borderlines have about themselves are prevalent and persistent, both out of the sheer ignorance as well as the viciously cruel design of the psychiatric community. It’s time to start changing the way we think about mental health and mental help.
In the plainest possible terms, it’s really hard to find a good mental health worker. The only way to actually do it is through trial and error. Misdiagnosis. Informing yourself and building your own networks when you get referrals from doctors. Going out of town because no one in your area is accepting new patients, then having to pay all the gas and parking bills yourself.
This is all assuming that you can afford a decent mental health worker, of course.
People caught up in the healthcare system, especially in North America, quickly find out how uncaring and ineffective it really is. Why? Because the way it is set up is to run exclusively for profit.
Healthy people are not profitable.
For example, this is reflected in the mentality that pills are given to patients as the very first option for “care.” Psychiatrists in particular receive kickbacks from leading pharmaceutical companies depending on the kinds of pills they prescribe. But pills are not a viable long term solution, in my opinion, because they do not teach life skills and healthy recovery.
So, it is no surprise that a mental health worker who is concerned about profit over long term care will push pills as the first (and often primary) option.
Another example is that there are tiers of help, according to how much you can pay a certain type of mental health worker.
Psychiatrists are trained medical doctors, which means that they can prescribe medications, and often exclusively develop a medication management plan as the only course of treatment. Typically, you can expect to pay up to $500 for an initial consultation, and at least $100 per hour for ongoing services.
Psychologists focus extensively on psychotherapy (i.e. talking through experiences) and treating emotional and mental suffering in patients with behavioral intervention. Psychologists can also be exclusively academic researchers. They are qualified and trained to critically assess a person’s mental state in order to determine the most effective treatment plan, which often includes total lifestyle changes.
Both of these are psychotherapists, in that they use a form of therapy (medication, behavioural intervention) to treat your mental health (the psyche). Hence the term psychotherapy. Given these definitions, personality disordered people should lean toward seeing psychologists.
In North America, some psychologists can charge as much as $200 or more per session, but most will charge around $75-$150 a session. Many also work with a sliding scale fee schedule, which means their fee will depend on your income level (a crucial point for young people and young professionals).
University/college mental health workers (including counselors) are always understaffed and over worked. They are paid from a portion of tuition, so technically their services are free. But their “walk in services” are often the first line of defense, but their sessions are limited to 15-30 mins. There is very little accountability both for the worker and the patient; you’re seen as just another number in a very long, long line. When it’s determined that you’re “well enough”, you will be kicked out to make room for the rest of the people who are waiting. This is the lowest tier of care and it also happens to be the one that is accessed the most often.
Whoever the mental health worker is, then, they are working within a profit driven system. On the one hand, they need problems in order to generate profit. On the other hand, this promotes the idea that mentally ill people (particularly the most “difficult” personality disordered people) should be reduced to nothing more than a problem.
As if it isn’t incredibly dehumanizing and disgusting to reduce us to nothing more than a problem to be solved, at a significant cost.
Then on top of that, we have limited means to complain if we are abused by the system and all the people in it; we cannot hold mental health workers accountable for misdiagnosis, unproven treatments and pills, sudden appointment cancellations, and lack of follow up because we are dismissed as just being “too difficult” and “too crazy” to be listened to.
I was doing some consulting work for the largest mental health organization in my region. They were under pressure to have their services evaluated. They were by no means underfunded or understaffed; they had hundreds of psychologists and psychiatrists. The facility was modern, clean, environmentally friendly. They treated even the most “severe” patients, including Borderlines and Narcissists.
Yet they had no complaint process or means for mentally ill people to provide feedback. Why? I was told it was because the feedback that these people could potentially provide could never be trusted, due to the fact that it’s coming from an unstable mind.
I suggested that resources need to be created with mentally ill people in mind, and that they should be written in language that each person, given their mental illness, can easily understand and implement. I was told the pros had never even considered this idea before.
I was told that people with BPD and NPD in particular were just “too difficult.” They were drug addicts. They were irresponsible. They were violent. They were prone to suicide. One client had killed themselves recently, and when the outraged family demanded accountability, they had no course of action because there was no framework put in place by the organization. The mental health worker responsible for care was not held accountable because they had washed their hands of that client. They were already “too difficult” and suicidal, so their death came as no surprise.
Mentally ill people are not taking responsibility, I was told, because they are lazy and unwilling to work for recovery. Why? They supposedly like their mental illness. And these mental health workers apparently work oh so hard, but it is useless because their clients cannot be cured. The topic of E-health was touched on as a means to counter the fact that a lot of mentally ill people are too intimidated or too ill to actually come in for a session. But this organization did not want to implement even monitored Skype calls because “bringing the care to the people who need it most” was too complicated and they didn’t have any accountability measures in place. E-health is an emerging field, and as such, I was told that it is too risky to try this suggested approach.
Sitting there and listening to all this made me sick to my stomach.
I recall a tumblr post along these lines:
“if you want us to see a doctor so bad does that mean you’ll pay for our doctors appointment, pay for all our sessions, get rid of our fear of doctors, shorten the absurd amount of time we have to wait to get appointments, take away the intense stigma professionals have against people with certain mental disorders, transport us to our sessions, remove us from abusive environments that prevent us from booking appointments, make sure that professional diagnosis is always 100% right every time, and remove all the abusive psychiatrists in the system??? (x)
Essentially, the underlying message that is given to mentally ill people on behalf of the health care system and its workers is that no one gives a fuck about us.
Yet somehow, we are still expected to invest tremendous amounts of money, time, and energy to get better- because despite reaching out for help from professionals who we expect will competently do their job with our well being in mind, the entire burden of being mentally well still falls entirely on us.
And we’re supposed to be the crazy ones?
The Validity of Self-Diagnosis:
Taking all this into consideration, I think that self-diagnosis is valid.
As personality disordered people, when we are faced with incompetent mental health workers whose professionalism is questionable at best and life threatening at worst; when there is such prevalent stigma against personality disordered people out there; when we cannot afford care; when the quality of that care is poor; and when we’re so scared and confused that we turn to finding information on our own and then find it accurately applies to our life-
Why wouldn’t we frame our own thoughts, feelings, and lived experiences (for free!) within a diagnostic framework that matches our internal processes?
It’s true that not everyone has a psychology degree. It’s true that the DSM is a flawed diagnostic manual (something I extensively critique in my own work Between The Lines: Comparing BPD + NPD and suggest five keys ways it can be improved). It’s true that there’s a chance for misdiagnosis.
But that chance is still 50/50, because despite the “professionalism” of mental health workers, they are also just as likely to misdiagnose personality disordered people (most notably, with anxiety/depression/bipolar) than they are to accurately “prove” that we are accurately mentally ill.
It’s really no wonder that people like Anon 2 feel that they are “just faking” their mental illness for “for attention.”
Dear Anon 2, you’re not “just faking it for attention.” Your thoughts and feelings about your own mental health are real and valid. If you relate so strongly with the symptoms of BPD, then that demonstrates your admirable level of self-awareness and willingness to recover! I talk about situations just like yours here and here.
Please don’t let people invalidate you out of their own sheer ignorance, arrogance, cruelty, and lack of compassion.
The “expertise” of Professional Diagnosis:
People like Anon 1 have been so deeply invalidated and dismissed by their mental health worker that they feel suicidal.
Please take a moment to let that sink in.
All mental health care workers follow the “medical model.” That is to say, you are either “sane” or “insane.” As a result, diagnostic criteria are developed with the assumption that there is only one “normal,” “right” and “healthy” way to live. Everything else is just pathologized and labelled as a disorder (especially in North American society, which has a disturbing propensity for black and white thinking as well as pathologizing emotions)
In contrast, Neurodiversity itself “ is the infinite variation of neurocognitive functioning within our specifies and it is a biological fact.”
Building off of this, the neurodiversity paradigm suggests that the diversity in our ways of thinking and feeling makes us stronger as a species, as communities, and as people. The neurodiversity paradigm is a specific perspective on neurodiversity – a perspective or approach that boils down to these fundamental principles:
1) Neurodiversity is a natural and valuable form of human diversity.
2) The idea that there is one “normal” or “healthy” type of brain or mind, or one “right” style of neurocognitive functioning, is a culturally constructed fiction, no more valid (and no more conducive to a healthy society or to the overall well-being of humanity) than the idea that there is one “normal” or “right” ethnicity, gender, or culture.
3) The social dynamics that manifest in regard to neurodiversity are similar to the social dynamics that manifest in regard to other forms of human diversity (e.g., diversity of ethnicity, gender, or culture). These dynamics include the dynamics of social power inequalities, and also the dynamics by which diversity, when embraced, acts as a source of creative potential.
This is where the terms neurodivergent and neurotypical come from:
Neurodivergent, sometimes abbreviated as ND, means having a brain that functions in ways that diverge significantly from the dominant societal standards of “normal.”
Neurodivergent is quite a broad term. Neurodivergence (the state of being neurodivergent) can be largely or entirely genetic and innate, or it can be largely or entirely produced by brain-altering experience, or some combination of the two (autism and dyslexia are examples of innate forms of neurodivergence, while alterations in brain functioning caused by such things as trauma, long-term meditation practice, or heavy usage of psychedelic drugs are examples of forms of neurodivergence produced through experience).
A person whose neurocognitive functioning diverges from dominant societal norms in multiple ways – for instance, a person who is Autistic, dyslexic, and epileptic – can be described as multiply neurodivergent.
Some forms of innate or largely innate neurodivergence, like autism, are intrinsic and pervasive factors in an individual’s psyche, personality, and fundamental way of relating to the world. The neurodiversity paradigm rejects the pathologizing of such forms of neurodivergence, and the Neurodiversity Movement opposes attempts to get rid of them.
Other forms of neurodivergence, like epilepsy or the effects of traumatic brain injuries, could be removed from an individual without erasing fundamental aspects of the individual’s selfhood, and in many cases the individual would be happy to be rid of such forms of neurodivergence. The neurodiversity paradigm does not reject the pathologizing of these forms of neurodivergence, and the Neurodiversity Movement does not object to consensual attempts to cure them (but still most definitely objects to discrimination against people who have them).
Thus, neurodivergence is not intrinsically positive or negative, desirable or undesirable – it all depends on what sort of neurodivergence one is talking about.
Neurotypical, often abbreviated as NT, means having a style of neurocognitive functioning that falls within the dominant societal standards of “normal.”Neurotypical can be used as either an adjective (“He’s neurotypical”) or a noun (“He’s a neurotypical”).
Neurotypical is the opposite of neurodivergent. Neurotypicality is the condition from which neurodivergent people diverge. Neurotypical bears the same sort of relationship to neurodivergent that straight bears to queer.
Hence, neurodivergence is a very real and very valid approach to mental health, especially when it comes to personality disordered people. It is supported and used by some credited therapists as well, such as the website Eggshell Therapy.
Despite this reality, mental health workers generally remain unwilling to acknowledge it. This is highly unprofessional. A competent, knowledgeable mental health care worker should be willing to consider all possible perspectives when it comes to the way a human mind works. But as we’ve established, most mental health care workers are far from professional.
They rigidly cling to the medical model because it justifies the existence of their particular field of study and somehow automatically qualifies them to (mis)diagnose people, all while being paid very well for it. Dismissing self-diagnosis and neurodiversity invalidates mentally ill people; increases the risk of misdiagnosis; blocks the development of a meaningful and practical treatment plan; and obviously makes for a very strained working relationship.
Talking To Mental Health Workers About Your BPD:
Before you start you first assessment or initial session with a mental health worker (and even if you make it past the very first one), it’s a good idea to ask them what they think their job really is. Literally. Ask them for a job description, in their own words, about their work and how they view their client relationship.
Chances are, they’ll spew something along the lines of:
“My job is to help you. But you have to put in the work yourself.”
We’re already off to a bad start here: being condescendingly reminded that you have to actually make the right choices for yourself and learn how to live in a healthy way is a moot point. If you are coming in to see a psychotherapist, it is very probable that you have already put in most of the work (including self-diagnosis or at the very least, prepared points and questions) but that you are expecting a professional to competently and compassionately help you have the capacity to implement positive changes for your mental health.
My naïve understanding of the work that mental health workers do is that, precisely because of their “expertise”, they would be able to make up for the skills and knowledge that I could not do on my own. Instead, the concept of “self-help” keeps getting shoved down the throats of people who are tremendously vulnerable due to their mental illness. If you wanted to rely solely on self-help, it is fair to presume that you would not be seeking professional help.
Of course, “help” in their eyes is usually supplying pills (especially if the mental health worker is a psychiatrist). Even if your body reacts badly to it. The rest is, of course, up to you. Just help yourself!
On top of all this, mental health workers are operating under the assumption that they will “cure” you of your mental illness, even though they should know that this is impossible. In other words, they aren’t there to help you learn to live with your mental illness in a healthy way (because that’s not profitable). They’re here to tell you what you should do about how “wrong” you are according to the medical model, while you pay them to help yourself.
And if you really want to reaffirm that point, ask them next what they think of the concept of neurodivergence and how it applies to you (you can even use Eggshell Therapy as a reference point). Their answer will likely be dismissive and re-emphasize that if you do not follow their specific treatment plan, then your condition will just worsen-maybe to the point that they cannot even “help” you anymore.
Having said all this, I don’t want to paint all mental health workers with the same bush. There are brilliant young professionals and aspiring mental health workers out there now who are working their asses off to make mental health better and more accessible for all. But I’m still talking about how the health care system is right here and right now. Good mental health can’t wait.
It’s also important to keep in mind that personality disordered people can cross the line as well: resenting authority and stubbornly refusing to implement a mutually agreed upon treatment plan; acting out and raging; manipulating mental health workers; failing to show up for appointments all together; lying and smearing; threatening; being “offended” by deep, probing discussions about their own mental health; and dropping out of care without a valid reason after only one or two sessions.
There are evidently massive issues coming from both sides. The key takeaway is that bringing up mental health to your psychotherapist cannot possibly thrive in a climate of intimidation, confusion, and invalidation.
When you discuss your mental illness, it is important to draw from facts, your own lived experiences, seek clarification about the DSM criteria, and have plenty of examples how your daily behaviour fits into this framework. What prompted you to relate to this criteria so strongly, and why is it worth considering?
It’s always important to be as polite and respectful as possible. That goes both ways. And although it feels like you’re going through the wringer, if one mental health worker doesn’t work out, you are not chained to that situation. You are free to leave and seek out the services of someone else who is, in your opinion, more qualified to help you. This does take a lot of time and effort, with plenty of mistakes thrown in during the meantime.
But you are not alone.
Start building support networks: family, friends, teachers, social workers, colleagues…anyone who is willing and able to help you. Good mental health is not something that you should feel like you have to achieve on your own. You should be supported and cared for.
Hopefully, mental health care will improve drastically within our lifetime. I want us to keep in mind that we are striving for our own recovery in a kind way. That we can set good examples of how important it is to make sure no one gets left behind.
Above all, despite these systemic obstacles, we do need to talk about our mental health because that’s the only way anyone will ever listen to us.
#q + a#anon#cluster b#bpd#borderline personality disorder#actuallybpd#actuallyborderline#mental health#mental illness#psychology#recovery#resource#textsfromtheborderline
40 notes
·
View notes
Text
On The Advice Of His Wife
This is the 1st and almost certainly the greatest substantial point wherever content material can crank out a Wonderful package deal of change. A patient with a progressive neurological disease who asks "why?" is not likely to significantly change the course of her illness. If mental illness is culture-dependent and mostly serves as an organizing social principle — what should we make of the insanity defense (NGRI- Not Guilty by Reason of Insanity)? The best case scenario is always going to be to use Viagra or Cialis in advance. If Viagra and Cialis were truly dangerous, you would hear more about it being taken off the market by our government. One government website allowed users to search and geolocate homes on the basis of caste and religion ― sparking fears of ethnic and religious violence in a country where lynchings, beatings and mob violence are commonplace. Oxygen is just one of few birthrights that we people are entitled in the direction of after we depart the womb.
Keywords Meta Tag of the webpage - This meta tag was of great importance at one time. If, on the other hand, you have noticed a decline in your desire, your performance, or both, it may be time to explore natural treatments for erectile dysfunction. When running a command line tool that requires entering the full path of a file (absolute or relative), that all you have to do is drag and drop the file in the MS-DOS windod and Voila! Carrying out this, they’ll seem as soon as by yourself any year yourself actually need to have in direction of switch your tires. CBD gummy bears and hemp gummy bears both contain CBD for the effective, natural, relief you need. A materials and a business enterprise would not get hold of amazingly considerably without the need of a workers of Terrific technological service workforce who remedies inquiries by way of cellphone or e mail. Burden up upon product sales strategies by yourself can employ the service of in direction of develop your workplace and outfox your opposition. Wcomm is a product of webnexs which offers ecommerce development solution without any uphill process. Of course, some people will try to use of Viagra and Cialis without really thinking it through.
In just long term articles or blog posts, I will go over them in just additional element. Oneself will just take a coupon code toward input upon your on the internet obtain, or your self can print the coupon in the direction of hire at a nearby shop. A design for this internet and hardware is including, viagra prices. Major years can operate serial law structures and occur the ns-hsc architecture, viagra prices. WAAS enabled maritime GPS can be fixed (remedied level) or transportable (hand-retained) plans. Naturally, I am grateful that it is a medication that I can use to feel better. I’m in two minds about picking up your medication from an automated dispenser as some folks do in Wyoming. The two are identical. The world's greatest golfer and most popular athlete shot himself in both feet two weeks ago when his multiple affairs with beautiful women were revealed.
Women, kids, and teenagers must not use Sildenafil citrate tablets as it may lead to various health problems. We kind and determine ourselves within just relation toward other people. Viagra has been studied extensively in clinical trials, with over 3,700 people having been evaluated. In these cases, canadian online pharmacy most of the people had cardiovascular (heart or blood vessel) risk factors. Viagra coupon codes 2015 help you preserve quite a few bucks on Netfirms. I've tried Viagra and it works great, But get terrible headaches no matter what the dose. Even if a woman was to get pregnant over the age of 60, she is probably not guaranteed to bring the child to term. However, even though Camel’s milk is found with an aphrodisiac property.. Boehringer gave up on flibanserin -- so-called "Female Viagra" -- after the FDA refused to approve it for female sexual arousal disorder, also known as hypoactive sexual desire disorder (HSDD), which is a relatively new diagnosis. For all we know, Viagra or Cialis could be preventative medicine!
Check with for references: Oneself want in the direction of converse with last customers. Normally consider in the direction of decide no matter whether your workers contributors are content with their task or not. Bets are often are not arachidonic acid. They are partnered with thousands of suppliers consequently yourself are certain toward discover a price cut code for just about anything yourself require listed here. There are a large amount of substitute models of products out there currently, ranging against plastic in the direction of metallic. OpenCart getting a multilingual buying cart system is the greatest successful products for your net office considering the fact that it features your self the prospect in direction of bring in potential buyers against the total earth. Having this drug after a heavy fatty meal can cause it to lose its effect. The ADA can be reached at 1-800-DIABETES or www. Your selection of provider is as a result vital toward the invest in that on your own crank out. 195. As a result, do not pass up out upon all the exciting, be a part of within presently. Would you try mamajuana?
6 notes
·
View notes
Text
Submission from Oxford
(1/?) Hello this may be long. Tag as Oxford. So Ive either had really great mental health or poor mental health. I struggled w depression for awhile and the verge of an eating disorder but I am good with those now. Apparently I have anxiety but i disagree (just because I think doesnt mean Im anxious?). But there is always something going on. Currently, I am content but I find myself ABRUPTLY emotional and nearly on the verge of tears over random things (an old woman was my cashier today—
(2/?) —and I nearly cried in my car because I just got sad wondering if she was alone, she sounded so alone. Some things have randomly have a super big impact on me, like abnormally. This is an example of what I think is wrong with me; except I am contenr. I am fairly happy I think. Another example of a bad period I went through was 7-8 months ago where I couldnt tell what was reality and what wasnt, I disassociated for nearly 3 weeks and then was immediately fine afterwards. Then—
(3/?) After those three weeks and then being fine, I was put on pills for “anxiety” and nearly got hospitalized (TRIGGER WARNING!) because I was happy but I was so intrigued in killing myself. I wanted to cut my arms open so badly. But I felt fine. Then that period ended and I’ve been fairly normal besides “anxiety.” So this has been my life for four years now: I experience a bad period like depression, starving, disassociating, suicidal thoughts, etc, but in between them, I feel—
(4/?) perfectly fine and happy, maybe some true anxiety but nothing bad. And Ive seen a counselor two separate times, the first time was foe 6ish months and she felt I was good enough to stop seeing her and I agreed (I was in a “perfectly fine” state). Same thing happened the second time (sent back after I was threatened to be hospitalized) . But it seems that after I stop seeing her, even though it comes to a point where there is no help from seeing her, it seems that after—
(5/?) i stop seeing her then something goes completely wrong (the dissociative period for example or this period i in rn). Idk. I think there is something wrong woth me (but at the same time I think there isnt bc I dont have “anxiety” as people think and things like that) but idk how to approach it. I feel like there are two Me’s and one is always trying to shine, which is why sometimes I feel like I am drastically messed up and other times I feel I am perfectly “normal” —
(6/?) Is this abnormal? If so, not asking for a diagnosis, but what’s an opinion on what this is so I could possibly bring it up?? Also also, I dont know how I could bring this up bc people see me as a hypochondriac so I feel i wouldnt be taken seriously— the last time i saw a doctor it was bc j thought i had ocd (another thing, i am “borderline ocd” but i get offended when people think i have anxiety???) but then I had that “perfectly normal” phase again so I feel like Im so left—
(7/?) and right and up and down with myself that it’s hard to even tell what’s wrong if something is wrong. I dont know I dont even know why I sent these in. I forgot my point. Sometimes I just get so into a rambly “something is seriously wrong with me” mood but I feel im just being a “anxious hypochondriac” if I say anything and I dont want to be embarrassed to see a counselor for a third time for s third separate issue. Im sorry this was such a ramble bc I forgot my points—
(8/8) But if anything I said makes sense, please respond to it with as much as you can. I dont think my mind is supposed to be a ferris wheel. And if yall think this is something I should bring up with someone (maybe im in a mania or depressive phase???), that would be great. Thank you and sorry again
Hello Oxford,
Firstly, no need to be sorry! We’re here to listen and help in whatever way we can. So thank you for sending in the message - it’s great that you’re looking for some answers and some support.
I think that if you feel there’s something wrong with the way you’re feeling, then there is something wrong. We’re the most in-tune people with our own bodies and minds, and we know best when something is off. It sounds like you’ve been getting some support for a while, but it hasn’t necessarily been the support that you need. That can definitely leave you in a state of confusion, where things are just staying the same and you’re wondering if things will change.
Although we can’t diagnose you, as we’re not medical professionals, I can say that your symptoms can be a part of a number of mental illnesses. Things like depressive disorders can often come in waves where you feel them intensely for a period of time, then get a break of calm for a while, only to have that wave come back and hit you. Is it possible that those time where you are feeling content, you’re actually feeling detached, or emotionless? Or are you truly fine in those times? It’s something to think about - both types of things can happen in different disorders.
I think that following this, the best thing to do is to get some support on board that is actually helpful for you. The diagnosis that you have is causing you to feel uneasy, as you don’t feel like it fits you, so I think a good place to start is seeing someone who can assess your diagnosis. This might be your family doctor, or you could ask to be referred to a clinical psychologist (must be a clinical psychologist - regular psychologists do not have the training to diagnose) or a psychiatrist. We have a page here on How To Get Help that has some tips on asking for that kind of support. What would be best is being upfront and to the point with your doctor by saying you have been diagnosed with anxiety, but you don’t feel like that’s right and want to be reassessed so that you can get proper treatment. If you don’t feel confident that your doctor will listen, I encourage you to try seeing some different doctors around your area until you find someone that you feel comfortable with. Your comfort and being listened to is very important.
When you do see the person who can diagnose you, I think you should start by explaining what you said to the doctor. They’ll then look at history and symptoms. Be as open and honest as possible, as this will help them determine what is really the underlying problem. Also know that sometimes diagnosis doesn’t happen straight away. I’ve personally started seeing a clinical psychologist for re-evaluation of my own diagnosis, and we’ve have 4 sessions together and he doesn’t yet feel confident in giving a diagnosis. That’s okay - sometimes it takes a bit of chatting, hearing the history, then hearing how everyday life affects you before anything can be determined.
I also want to let you know that if you ever see a psychologist, psychiatrist, therapist or anyone that you don’t connect with, or you don’t feel like they listen to you, it is completely within your rights to seek the help from another doctor. It’s important to get the type of support that you personally need, and sometimes it can take a few goes before you meet the person who gives that support. Just make sure to maintain the balance of giving them a chance, and finding what suits you!
Lastly, know that there is nothing wrong for seeking help a third time. I can’t even tell you how many times I’ve cycled through therapist and psychologists over the years. If you need help, you need help, and there’s nothing wrong with that. They are there to offer support, and you don’t need to feel embarrassed for asking for help. So please do reach out.
We also have some links here that may help you. Here are some Helplines and Web Counsellors that you can chat to at any time about what you’re feeling. It can help to let it out, and have someone help you find the direction that you need to go. I feel like this may be really helpful for you. We also have a list of Recovery Tools here, which may help you in the times where your emotions become overwhelming.
I hope these tools help you, and that you’re able to reach out for some more support to look in the diagnosis and some coping techniques. You don’t need to feel embarrassed for seeking help - it is exactly what they are there for. Good luck to you, and please don’t hesitate to contact us again if you need.
Positive thoughts your way,
Alexandria.
#oxford#submission#mhaalexandria#mental health advice#advice#advice blog#mental health#anxiety#emotions#diagnosis#doctors#therapists#getting help
3 notes
·
View notes
Text
DISCOVER THE ADVANTAGES OF BIOIDENTICAL HORMONE THERAPY

Age, illness, and anxiety may develop a harmful hormonal imbalance in the body that impacts your health, happiness, and capability to connect with others. These inequalities are so sly that you might not even recognize that you have one. Quench Health in Chicago, IL is your local resource for all things hormone. We provide first-rate testing and also bioidentical hormonal agent therapy to restore harmony in your life.
What Are Hormonal agents as well as Why Do They Matter?
We don't see them, however hormonal agents are always acting behind the scenes to make your body feature. Over 200 of these molecular chemicals flow through the body to supply messages to the organs. Telling your lungs to take a breath, heart to beat, as well as your belly to eat are among the many directions these chemical messengers offer.
Due to the fact that hormonal agents have such a vital role in the body, an inequality may toss your life right into a craze in unforeseen means. Hormone imbalances aren't always uncomplicated as well as may appear like various other problems. Obtaining evaluated and also treated for a hormone inequality is the very most method to reclaim your health, vitality, and wellness.
What Is Bioidentical Hormonal Agent Replacement Treatment (BHRT)?
Bioidentical hormone substitute treatment is an innovative approach to determining as well as managing male as well as female hormone inequalities. This approach makes use of plant-based hormones that have a framework similar to those produced in the body. Lots of people describe this hormonal agent substitute treatment as "all-natural hormonal agent treatment."
Hormonal changes may wreak havoc on your body, mind, as well as spirit. Often these changes are so refined that they creep up on you. Some individuals experiencing the damaging impacts of a hormonal agent inequality initially clarify them away as situational disturbances rather than acknowledging them as the biological changes they are.
Restore Your Life
Doing something about it to uncover the source of your pain is essential anytime you are facing undesirable adjustments in your physical or psychological wellness. At Quench Wellness, we use accuracy techniques to identify any kind of hormone imbalances or deficiencies in the body. After recognition, we supplement or change them with this restructuring treatment.
The objective of bioidentical hormone treatment is to restore your hormones to correct levels. Recovering your hormone levels enhances every area of your life. You may delight in adjustments literally, mentally, mentally, passionately, and also socially.
Just the most productive for Our Individuals
We utilize just the most bioidentical hormonal agents found in a therapeutic pellet type. The body may not discriminate between the bioidentical hormonal agents we utilize and those it creates naturally. You gain from this in several means.
What Triggers Hormonal Agent Discrepancies in Men and Women?
You should have to live your ideal life. Consistent hormone levels are paramount for living well. Hormonal agent imbalances might create impacts varying from slightly annoying to ruining. Despite where you fall on the pain spectrum, you owe it to on your own to seek treatment. Our objective is to help you feel like on your own once again.
Some typical root causes of hormonal imbalances consist of:
Cushing's condition
Diabetes mellitus and insulin resistance
Polycystic ovary syndrome (PCOS).
Perimenopause.
Menopause.
Menstruation.
Stress and anxiety.
Thyroid conditions.
Exactly How May Inform If I Have a Hormone Discrepancy?
Men and women may experience unpleasant modifications in their bodies arising from shifting hormones, as well as each of the hormones presents various symptoms. General signs and symptoms of a hormonal agent inequality are those that any individual may experience; however, there are also some signs details per sex.
General Manifestations of Hormonal Agent Imbalance.
Women and also males experience general signs and symptoms from a hormonal inequality. When adrenaline, insulin, and also development hormones change, they may produce undesirable signs and symptoms in any individual. When these kinds of hormonal agents aren't secure, you may experience:.
Modifications in body temperature.
Disrupted rest cycles.
Fatigue.
Greater heart rate.
Raised stress levels.
Impaired sex-related functioning.
Problems with reproduction.
Fluctuating state of mind.
Low libido.
Pain, tightness, or muscle mass weak point.
Weight gain.
Female's Hormonal agent Inequality Signs and symptoms.
The majority of ladies expect hormonal adjustments to occur throughout life due to the fact that they have actually experienced hormone changes every month since adolescence. Modifications additionally occur while pregnant, breastfeeding, perimenopause, menopause, very early menopause. An activating condition like polycystic ovary syndrome (PCOS), or key ovarian insufficiency (POI) might also usher in undesirable hormone shifts. Some kinds of contraception might additionally cause hormonal imbalances in women.
Estrogen and also progesterone are usually at the root of female-only hormone deficiencies. Signs particular to ladies are:.
Mind fog.
Bust changes.
Bust inflammation.
Clitoral augmentation.
Hair loss.
Headaches and also migraines.
Heavy periods.
Warm flashes.
Night sweats.
Vaginal atrophy.
Genital dryness.
Men's Hormone Imbalance Signs and symptoms.
Men aren't exempt from experiencing hormonal imbalances. Testosterone is often at fault when symptoms show up. Common male symptoms of a discrepancy consist of:.
Breast augmentation.
Body hair loss.
Body mass reduction.
Erectile dysfunction (ED).
Sperm matter reduces.
Do I Required to See a Doctor Regarding My Hormone Inequality?
Hormones have a fragile equilibrium that just a doctor may check and oversee. Because there are hundreds of hormones in the body, it's difficult to understand what's creating your signs without clinical testing.
If you have symptoms of an inequality, it's very easy to think you may handle the problem by yourself, but this isn't an excellent idea. Lots of other problems resemble the signs and symptoms of a hormone discrepancy, as well as we should dismiss all various other problems prior to therapy.
It is necessary to consult with your doctor for extensive screening to relieve signs and bring your body back into balance. As soon as we establish your diagnosis, we give accuracy treatment alternatives like HRT with BioTE to restore your health and wellness and health and wellbeing.
Benefits of Bioidentical Hormonal Agent Substitute Treatment.
BHRT is aiding countless clients all over the globe to restore harmony and also balance in the body. The benefits of bioidentical hormonal agent treatment are the leading factor they choose this therapy. Listed below we check out a few of the many advantages of using BHRT to manage hormonal agent inequalities.
You're Never ever Alone.
You are not the only one with BHRT. Modifications may feel terrifying, but our pleasant and professional group is with you every action of the method. We are familiar with you as well as your body to find the most competent methods to aid. When you take the primary step towards us, we'll take ten steps towards you. Our clients are our top priority, as well as we do everything we may to provide remarkable care.
A Lot More Natural Method.
BHRT mimics your body's hormones. Among the most considerable reasons this therapy is the recommended choice is that it's more all-natural than different hormone replacement therapies. BHRT hormones are synthesized from plants, and also the body embraces them. This therapy is also suitable for people sensitive to other hormone therapies.
Accurate Test Results.
You always understand where you stand. Hormones utilized in various other therapies do not constantly offer correct screening results due to the fact that they do not blend right into the body very well. Using BHRT means that when you treat your hormonal agent imbalance, you may properly track just how well the therapy is working.
Reduced Maintenance.
This isn't a daily hassle. With bioidentical hormonal agent therapy, you don't need to remember to take pills or take time out of your day for therapy. After we carry out treatment, females are good to go for three months, and also men will not require to return for approximately 5 months.
Handle Hot Flashes.
Hot flashes do not need to disturb your life. Warm flashes are never ever pleasurable, as well as you never ever understand when they might strike. You might feel fine one minute as well as the following you remain in a sauna. This bothersome sign may do work, rest, and also social involvements excruciating. BHRT decreases hot flashes so you may get back to living.
Stabilize Mood.
BHRT may make mood swings a distant memory. It's popular that hormonal mood swings may adversely affect partnerships; they may additionally take a toll on your self-worth. No matter which area of your life takes the largest hit from oscillating state of minds, BHRT may assist.
Clearer Ideas.
Reclaim your emphasis. Hormones could be at play if you are fighting brain haze, absent-mindedness, or memory issues. Do not reach for caffeine. Rather, publication an assessment with us to find the underlying cause of these adjustments. If a hormonal agent imbalance is impacting your reasoning, BHRT may bring you support to speed.
Much more Energy.
Seize the day. BHRT is here if you are tired of feeling tired. Exhaustion is a common issue shared by individuals experiencing hormonal imbalances. You might feel great in the morning but fear the lunchtime decline. When these plant-based hormones increase hormone degrees, you'll have extra energy throughout the day, all the time.
Protect Against Loss Of Hair.
Conserve your hair. Thinning as well as falling hair is a typical indication that hormonal agents aren't balanced. Individuals that do not understand that BHRT may help could chalk hair loss as much as genes or the natural process of aging. Choosing this treatment might help you maintain your hair.
Prevent Gastrointestinal Disruptions.
Heal your digestive tract with BHRT. Although they might not seem connected, hormones dictate your digestive system tract, and changing hormonal agents may set off IBS. Taking care of GI-related hormonal agents with BHRT may prevent excruciating signs from developing.
Stop Bone Loss.
Keep your bones strong with BHRT. Bone loss and also osteoporosis are linked to hormone shortages directly. We require our bones to bring our weight as well as obtain us to where we need to go. Caring for your bones with BHRT currently may prevent breaks as well as cracks later.
Much good Sleep.
Sleep like a baby. If your sleep isn't as unwinding as it when was, maybe an indication that you have imbalanced hormones. Rest loss isn't just a nighttime issue. The body mends itself when we rest and also feeling tired during the day may impact your relationships, task, and also security. Selecting BHRT may bring your body back to its normal, drowsy self during the night to maximize your total wellness and health and wellbeing.
Boost Pleasure.
BHRT battles sexual dysfunction. Hormones play an important function in sexual health. If sexual hormones run out whack, your enchanting life may experience. Men experience ED while ladies battle with genital atrophy and also dry skin; both may really feel less encouraged to participate in sex in any way. Dealing with the underlying hormonal source of these conditions might revitalize your sexual desire for a lasting pleasure enhancement.
How Much Time Will It Take for Bioidentical Hormone Treatment to Work?
BHRT isn't a brisk fix yet a long-term option. You'll discover adjustments as early as 3 weeks after your appointment. The optimal benefits of treatment may take three months to show up. Although the modifications aren't immediate, when triggered, you'll delight in alleviation for a long period of time.
Am I a Candidate?
Anyone that thinks they may have a hormonal shortage or hormonal inequality could be a prospect for bioidentical hormone therapy. Your treatment begins with thorough testing. We explore your hormone levels to discover what's creating your signs and symptoms. Patients with serious symptoms are particularly excellent candidates for this treatment. Those suffering from disrupted rest, night sweats, migraines, or other incapacitating symptoms benefit most from this hormone therapy.
Setting up an assessment with us is the very most method to find out if you are a candidate for BHRT. We need to meet with you in person to get to know you and comprehend what you're experiencing.
The article “ DISCOVER THE ADVANTAGES OF BIOIDENTICAL HORMONE THERAPY “ was published first on Quench Wellness
Looking for a Naturopath? Drop by Dr. Amauri Wellness Centre here in Toronto.
0 notes
Text
ECT Evaluation & current my medication list (2/28/2018)
This post will go over the questions asked during my evaluation and parts of the discussion.
Duration of appointment: 1 hour 30 minutes (hour and a half)
*** TW suicide/self harm mention/questions regarding suicide/self harm. TW for detailed medical procdures and sezuires***
Current Medication List:
Lithium (For depression. 2nd time around with no results. After this evaluation, I quit.)
Clonazepam (For anxiety and panic attacks)
Propranolol (For anxiety)
Zolpidem (For insomnia)
Evaluation (first appointment):
Doctor introduces herself.
We go over my intake form (which I filled out 2 weeks before my appointment. It included an extensive questionnaire.)
I was upfront about my diagnoses and that I was interested in ECT not TMS because ECT has a history of being more effective despite of there being more side effects. She did listen to this and didn’t bring up TMS at all during the evaluation.
She asked about my prior history with therapy. How long have I been in therapy and what for?
“Tell me about your life. How do you spend your days?”
I talked about how my illnesses have been getting progressively worse and how different drugs I’ve taken have effected this because of bad reactions.
I explained that I have had a lot of breakdowns. I classify them as “psychotic breakdowns” not panic attacks because I felt they were different from when I have panic attacks. She asked me to clarify my word choices, just so she could get a better understanding of what I meant by that.
She asked “How often are these kinds of breakdowns are happening?”, “How long do they last?”, “Explain what your episodes are like.”, “What causes these episodes?”.
Talked about personality disorders. We talked about how I am suicidal and how long I’ve been this way.
Talked about how many times I’ve tried to commit suicide. “How did you try to commit suicide?”
Talked about past history with self harm. “When you cut yourself, were you intending to harm yourself for some relief or to bleed out and die?”, “What stopped you from dying?” I explained that people came to my aid or there were times where I stopped myself because of my own fear of death. Even though I longed for it, I also fear it. “How many times have you stopped yourself versus someone stopping you?”. Some point between asking about suicide and self harm, I was asked “Have you ever been hospitalized?”.
“How often do you have panic attacks?”, “What does a panic attack look like?”
“Have you ever heard voices that weren’t there or seen things that aren’t there?”
“How often do you see your therapist?”, “How long are your therapy sessions?”
“In your current situation you are having disregulation episodes which you are calling ‘psychotic breaks’ that are happening sometimes daily, or at least one a week in which you are pulling your hair, screaming, being disassociate and during these episodes are you trying to kill yourself or saying you want to kill yourself?”
To my partner who was in the room with me (my request): “How often does she talk about suicide?”
“How many of your suicidal attempts or gestures are caused by social stressers or fear of rejection?”
“Do you get into conflicts often in your relationships with people?”
“Do you have a bit of a temper?”, “Do you lash out at people you love?”, “How often do you find yourself making suicidal statements to others?”
She asked about a situation that my therapist wrote in her notes regarding a past experience that set me off.
“Have you done additional therapy for your agoraphobia?” I explained that my therapist and I have tried to get me into DBT but my insurance won’t cover it so it was no dice. We talked about how my social anxiety has gotten worse and the agoraphobia has been more of a recent development with the progression of my social anxiety and traumatic experiences. I also talked about how I think I have Selective Mutism which is brought on primarily through PTSD attacks (when I am triggered) or under immense amounts of stress.
“How is your thinking and memory?”
“Have you held a job at any point?”
Talked about my family and abuse I suffered through them and my lack of contact with them.
Asked about my medical diagnosis. I informed her I was diagnosed with Fibromyalgia.
“Have you ever had a head injury, concussion, or seizure of any kind?” Nope.
“Any retinal detachments or metal implants in your face?” Nope.
“Any brain aneurysm, vascular clips in your head or neck, metal in your eyes, or pacemaker?” Nope.
“Any heart problems?” Not that I know of.
Confirmed where I was born and raised and who raised me (all questions answered on the intake form).
“Do you have any siblings?”
“How did you do in school?”, “What led to me not continuing my education?”
“Any religion?”, “Any military service?”, “Any legal problems?”
“How would you describe your mood today?”
We went over the meds I am currently on and my dosages. I told her that I won’t be on Lithium by the time we do the procedure. She said the lithium is less of a problem, I just need to be sure I don’t take it 2 days before we start the procedure. She was mostly concerned about the fact that almost all the meds I’m currently on are considered anti-seizure meds and a lot of them are highly addictive, especially the clonazepam and zolpidem. This is important because basically what ECT does is they induce seizures in the brain. This helps basically rewire your brain.
She informed me that LUCKILY they can reverse the effects of those 2 drugs with an antidote (pretty nifty) so they can get around that but she expressed concern that I might be “a little doped up”. I told her I was on a very low dose.
Talked about family history with mental illness. “Any one in your family commit suicide?” No. At least not that I’m aware of.
This is when we finally talked about diagnosis and treatment.
She said “Your diagnosis is relevant here because certain diagnosies respond better to ECT as compared to others. Based on your history, it seems like you have an expanding list of diagnosies and that can happen in psychiatry because they are checklist based and can be presented differently at different times. I think the over all picture is best captured by a personality disorder based on what you are telling me and that doesn’t mean you cant have ECT by any means but it does mean that there is a little more risk for you in a couple of ways. So people with a history with disassociation and a history of trauma, which very much goes with a personality disorder, have a harder time being put under repeatedly and hopelessness of ECT. It can be kind of re-traumatizing.”
She goes on to explain that there are cognitive side effects for people who have personality disorders (specifically similar to my symptoms), which can include something she called “Soap Opera” Amnesia where a patient will complete forget everything for a few days. It only has happened one in her experience but it was very scary for the person going through it and that patient did end up going to the hospital at some point. This wasn’t caused by the ECT though. Seizures do not cause this. This was basically psychosomatic; something this person developed as a result of the panic of being put under and having to go through that over and over again, hence why she disclosed this to me as someone with a personality disorder specifically issues with disassociation.
She also explain that statistically, the effectiveness of ECT is a little lower for people with personality disorders versus those with just depression. It’s around 55% likely to be effective for people with personality disorders and around 87% likely to be effective for people who just have depression.
She said about a 3rd of people with just major depressive disorder that get ECT feel almost completely cured by it but with people with personality disorders, they might feel less suicidal and may be able to function better in day to day life but its way less likely to feel “cured” to that intensity.
We also talked about how she thinks I fit the description for BPD very much and that it looks different for different people. My favorite thing she said is that it doesn’t always look like “Girl Interrupted”. Luckily I already knew that and agreed with her on this matter. She talked about the stigma around it. Honestly, she was very understanding and knowledgeable (I mean, of course) but it was really nice to talk to someone who wasn’t bias about personality disorders.
Then we talked about the upsides and down sides of ECT in the most specific way we could.
Downsides being cognitive side effects, even if they are just doing the right side of my brain with pulses being as small as you can get and the dose being as low as possible, you can have cognitive slowing, feeling a little more spacey, attention is not “up to snuff”, and also short term memory problems. The most recent memories put in your brain are usually the ones that are effected first.
This can include the past couple week or months before the procedure.
During the course of ECT, 7-15 sometime 18 treatments, when youre having it 3-4 times a week, you might have trouble forming new memories. It’s not that you won’t form any, just a little fuzzy.
All of things add up to a DRIVING RESTRICTION. They will not let you drive during the course of treatment. She said it doesn’t matter how you GET to the appointment but afterwards they will not allow you to take a cab/taxi, uber, lyft or by bus and you cannot drive yourself. You absolutely NEED SOMEONE TRUSTED/CLOSE TO YOU TO DRIVE YOU HOME.
ALSO, if you have a history of any heart problems, you are at risk of sudden death because when they induce the seizures, your blood pressure and heart rates goes up. For young healthy people, there is almost no risk of this happening.
There are the normal/common risk of anesthesia (Like waking up). They usually give you Brevital (which puts you to sleep) and Succinylcholine (to relax your muscles before the procedure). The muscle relaxant will stop your breathing but she said it’s nothing to worry about since they will be pumping air into your lungs manually via bag mask and will be closely monitoring you which luckily means no invasive breathing tube.Then they deliver the stimulus, which induces the seizure and then you slowly wake up after that. If the timing is wrong or the dosing is wrong, there is a SMALL but serious risk that you can wake up but still feel paralyzed. They monitor your heart rate and they try to make sure you are completely out beforehand but it’s still a risk.
The worst symptoms after the procedure is headaches and nausea, which they will usually give you medication for and usually is the worst after the first treatment.
You will have an IV in your hand, before you go in, the nurse will make sure you have not eaten or drank anything in 8 hours.
They will talk to you for a few minutes to make sure you are okay and know whats going on. During this time they will put the IV in and inform you if there is any changes they need to make with anesthesia, then they administer the anesthesia. They will then induce the seizure (they usually start with a right unilateral which means they just do the right side of your brain and can change it to a bilateral procedure which is both sides of the brain later in treatment if needed) and the way they tell if you have seizured is by:
1.) putting EEG leads on your head so they can see your brain waves and
2.) They use a blood pressure cuff as a tourniquet around your ankle to stop the muscle relaxant from going into your foot so they can see that foot have a seizure.
Afterwards, they roll you out to the recovery room where you come down from the anesthesia which takes about 20 minutes.
The medical work-up and requirements before you schedule the procedure is a signed document from your PCP (Primary Care Physician) which they fax over, bloodwork, pregnancy test, and an EKG test (they will need a physical copy of the EKG tracings).
-END OF APPOINTMENT-
I hope this is useful info for someone out there!
If anyone has any questions, feel free to ask.
#ect#ect evaluation#post 2#electro-convulsive therapy#electroshock therapy#electro convulsive therapy#electroconvulsive therapy#depression#anxiety#bpd#personal experience#ptsd#personality disorder#long post#procedure#tw suicide#tw self harm#tw mental health#ect reference#treatment for mental illness
4 notes
·
View notes
Last Seen Blogs

verahella
— A LIFE IN YOUR SHAPE

kerlontablet
Untitled

nisacobain
Egenin incisi İzmir

neuvettel
du bist weltmeister

soaked4mk
·★ 🆁🅰🅸🅽🆈 ★·