#Musculoskeletal Trauma
Text

Explore Healix Trauma Care's revolutionary approach to treating orthopedic and abdominal injuries. Discover advanced solutions for optimal recovery.
Do Visit: https://www.healixhospitals.com/blogs/beyond-bones:-healix-trauma-care-revolutionizes-treatment-for-orthopedic-and-abdominal-injuries
#Orthopedic and Abdominal Injuries#Trauma Care#Orthopedic Injuries#Abdominal Injuries#Emergency Medicine#Injury Treatment#Trauma Center#Fracture Management#Soft Tissue Injuries#Internal Injuries#Emergency Room#Trauma Surgery#Sports Injuries#Musculoskeletal Trauma#Critical Care#Surgical Treatment#Rehabilitation Services#Advanced Care#Injury Rehabilitation#Medical Emergency#Abdominal Trauma
1 note
·
View note
Text

#Motion Energy gel is a promising joint-pain solution that has a natural composition. It reduces the stiffness and limited motion in joints b#Spain#and Italy state that the bio-active cream helps in cases of arthritis#osteochondrosis#and joint trauma. Motion Energy joint cream also increases muscle mobility and improves the function of the musculoskeletal system as a who#motion_energy#yoga#exercise#yogamat#exercisemat#salute.
0 notes
Text
alas my physio loosening my joints has not helped my whatever-the-fuck-my-ribs-or-smth is doing :(
#*deep space noises*#there is /something/ musculoskeletal going on at least#particularly around my second to last floating rib#she said it could be a slipped rib but that she’d expect it to be more painful#especially when twisting#and that doesnt rly affect whatever is going on with mine#although if its due to laxity/hypermobility rather than trauma i imagine it would be less painful? idk#anyway theres. not rly much i can do#apart from try an support it when it does flick and keep tabs on what sets it off if anything
0 notes
Text
Musculoskeletal Diseases Market - Industry Analysis, Market Size, Share, Trends, Application Analysis, Growth And Forecast 2022-2027
Musculoskeletal Diseases Market Size is estimated to reach $7.9 billion by 2027 and is poised to grow at a CAGR of 6.9% over the forecast period of 2022-2027. Musculoskeletal disorders (MSD) are injuries or disorders of the muscles, nerves, tendons, joints, cartilage, and spinal discs. The Department of Labor's Bureau of Labor Statistics defines MSDs as a musculoskeletal system and connective tissue diseases and disorders when the exposure or event that caused the condition was repetitive motion, overexertion, or bodily reaction such as bending, climbing, crawling, reaching, or twisting. Disorders caused by falls, trips, slips, and other similar events are not included in MSDs. The three most prevalent musculoskeletal diseases, according to reports published by bone and joint disease organizations, are arthritis, back pain, and trauma. Each year, patients seek treatment for these conditions in hospitals, emergency care, and physician practices. Major musculoskeletal diseases are more expensive to treat than many other common medical conditions as they frequently cause long-term pain and disability. According to a recent review of Global Burden of Disease (GBD) 2019 data, 1.71 billion individuals worldwide suffer from musculoskeletal disorders such as rheumatoid arthritis, osteoarthritis, low back pain, neck discomfort, fractures, and other injuries. Such global prevalence of musculoskeletal disease and their increasing cases with most of population in majority of countries turns towards older age contribute to new research and development in musculoskeletal disease. Some major groups like Zimmer Biomet holdings, Inc., Stryker Corporation, Medtronic, Wright Medical group and others contribute to the growth of the Musculoskeletal Disease Industry over the forecast period 2022-2027.
The report : “Musculoskeletal Diseases Market Forecast (2022-2027)", by Industry ARC covers an in-depth analysis of the following segments in the Musculoskeletal Diseases Market.
By Type : Rheumatoid Arthritis, Osteoarthritis, Osteoporosis, Psoriatic Arthritis, Ankylosing Spondylitis, Fibromyalgia, Tendinitis, Carpel tunnel syndrome, Bone fractures, Osteomalacia, and Others
By Medication : Acetaminophen, Nonsteroidal anti-inflammatory drugs (NSAIDs), Anti-neuropathic pain medications, Corticosteroids, Biologics and biosimilars, Osteoporosis medications, Gout medications, Fibromyalgia medications, and Others.By Treatment: Biologics, Corticosteroids, Parathyroid Hormone, Protein Therapy, Selective Estrogen Receptor
Modulators, Synthetic Bone Graft, Composite Grafts, Demineralized Bone Matrix, BMPS, Therapeutic massage, and Others.
By Musculoskeletal System : Joints, Ligaments, Muscles, Nerves, Tendons, Cartilage, and Spinal discs.
By End Users : Hospitals, Diagnostics Centers, Urgent Care Centers, Physiotherapy, and Clinics.
By Distribution Channel : Hospital Pharmacy, Retail Pharmacy, Online Pharmacy, and Others.
By Geography : North America (U.S., Canada, Mexico), Europe (Germany, United Kingdom (U.K.), France, Italy, Spain, Russia, and the Rest of Europe), Asia Pacific (China, Japan India, South Korea, Australia, and New Zealand, and Rest of Asia Pacific), South America (Brazil, Argentina, Chile, Colombia and Rest of South America), and Rest of the World (the Middle East, and Africa).
0 notes
Text
What Can Passing the hEDS Criteria Look Like?
To pass you must meet the requirements of all 3 criteria sections. This is what my assessment looks like for reference! Reblog to help spread awareness.
Criteria 1: 8/4-9
First is testing for hypermobility. Most often used is the Beighton Score (which isn't perfect). The Beighton Score is a quick method to test for hypermobility. You must score 4-6+ out of 9 depending on your age.
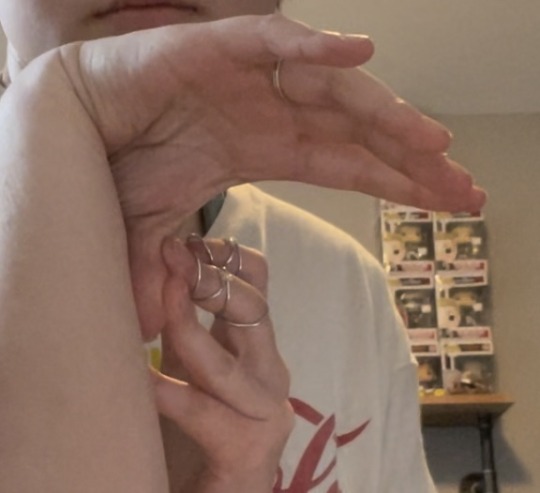
1. Each pinky finger you can bend 90+ degrees backwards gives you one point.


2. You can also gain a point for each thumb that can touch the inside of your forearm like this.

3. Each elbow that hyperextends beyond 10 degrees gives you a point.


4. Each knee that hyperextends beyond 10 degrees gives you a point.


5. And if you can place your palms flat on the grounds without bending your knees you can gain one point. (this is the only one I can't do)
Criteria 2: 2/2-3
Feature A: 5/5-12
Feature A looks at certain indicators of a connective tissue disorder. You have to have 5 or more out of the 12 listed to pass.
1. Unusually soft skin. Every EKG I've had, the cardiologist had been unable to keep the stickers on me because of how soft my skin is.
2. Unusual or unexplained stretch marks. These stretch marks are unexplained because they appeared before puberty.



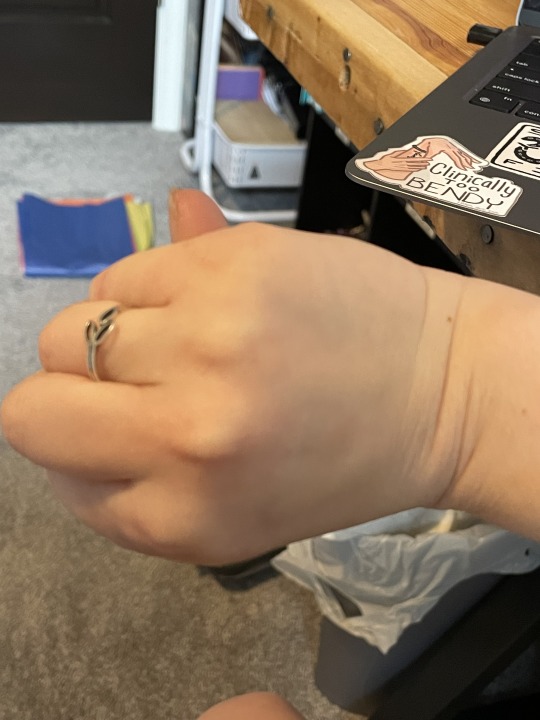
3. Arachnodactaly by a positive thumb sign. This means both hands, when I make a fist, the entire nail of my thumb extends past the edge of my palm.

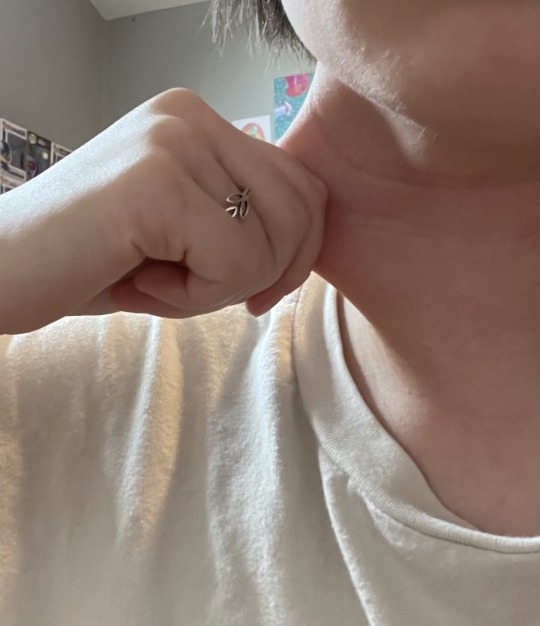
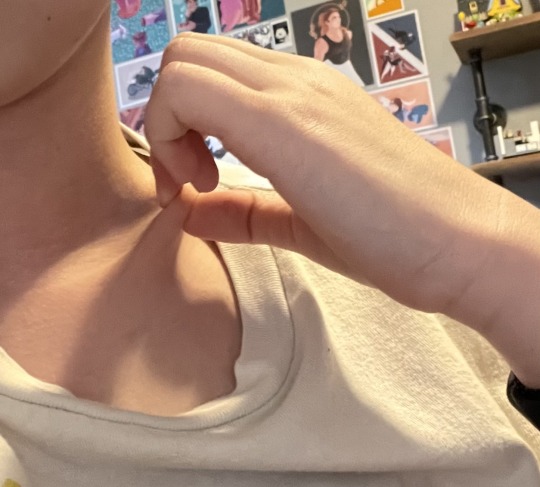
4. Mildly stretchy skin. This is most prominent on my biceps, neck, and collarbone.

5. At least 2 sites with atrophic scarring. Here are the major scars that qualified in my assessment. Though I have tons of these all over my body from various nicks and cuts.


Feature C: 3/1-3
Feature C assess if you have problematic or painful chronic symptoms.
1. Musculoskeletal pain daily for 3+ months in 1+ limbs
2. Widespread pain for 3+ months
3. Recurrent joint dislocations/instability in the absence of trauma
Criteria 3: 3/3
Because hEDS is diagnosed based on exam and exclusion, it's important that there is no other explanation for the symptoms. This means you must pass all three of these requirements.
1. No unusual skin fragility (could be Classical EDS)
2. No other heritable or acquired connective tissue disorders that could explain symptoms.
3. No other diagnosis that include hypermobility like other forms of EDS, Marfan Syndrome, etc
Some other things that factored into my diagnosis:
Diagnosed Postural Orthostatic Tachycardia Syndrome
Mast Cell Activation Syndrome symptoms
Chronic digestive dysfunctions and issues
Very easy bruising
Very flat feet
Daily partial dislocations of hips/shoulders and multiple rib dislocations
Extreme and chronic fatigue
Very high tolerance to general anesthesia
Odd reactions to medications
Life long sleep disturbances
Very slow wound healing
#heds#hypermobile ehlers danlos#ehlers danlos#ehlers danlos syndrome#ehlers danlos awareness#hypermobility#joint hypermobility#ehlers danlos zebra#chronically ill#chronic illness#connective tissue disorder#disabled#physically disabled#actually disabled#diagnosis#diagnosis journey#disability awareness#chronic illness awareness#cripple punk#pots#postural orthostatic tachycardia syndrome#spoonie#chronically suffering
211 notes
·
View notes
Text
What is AMPS?
ampflified musculoskeletal pain syndrome is a neurological disorder that affects the brain as well.
Essentially, amps starts from a trauma(physical and/or mental) taht the brain cannot cope with alone.
The brain panics and shuts down the body(either the hole body or specific parts). This means that the traumatized part of ourselves will not be listened to. Especially concidering our trauma is stored in the body.
The body attempts to be listened to by sending a bunch of fight or flight signals to the brain. We have a difference in our nervous system that causes a short circuit or amplification loop and can quickly spiral out of control. The brain can intruprit this singal in many ways, including pain, nausea, numbness, or really any symptom you can possibly think of.
Amps pain, because of the amplification loop, and get as high as beyond child labor pains. This is because the problem is within the nervous system, not from an external factor or a “true” injury.
People with amps are generally hyper vidulent, suffer from ptsd, have a fear of exercising, etc.
Because AMPS is essentially body PTSD, exposure therapy is key. That means intense workouts daily and intense talk therapy sessions.
The psysical therapy helps teach us that exercising will not, actually, make our body explode and die! What a consept! If I were to describe how amps PT can be, it would probably be like if your doctor siad that the onyl way to cure migraines was to look directly into the sun and blast heavy meatle in your headphones during an attack, lol.
That being said, there is no cure for amps. There is only making peace with our body, mind, and trauma. This stops attacks from happening less and less, and dampens the amplfiication.
#disability#amplified musculoskeletal pain syndrome#amps#medical conditions#physical disability#cripple punk#spoonie#chronic pain#chronic illness#actually disabled#awareness
33 notes
·
View notes
Text
October is Craniocervical Instability Awareness Month!
Craniocervical Instability (CCI) is a condition affecting the cervical spine. CCI happens when the vertebrae in the cervical spine are unstable, this can be caused by pre-existing conditions like Ehlers Danlos Syndrome and inflammatory arthritis as well as trauma to the C-spine.
Craniocervical instability typically consists of a mixture of musculoskeletal and neurological symptoms. Some CCI symptoms include neck pain, feeling of having a "bobble head," trouble swallowing, seizure-like activity, drop attacks, symptoms of dysautonomia, instability, poor coordination, tingling and numbness, vision changes, dystonia, and much, much more.
Craniocervical Instability can be diagnosed several ways. The most common method of diagnosis is a flexion-extension x-ray of the cervical spine followed by a rotational CT if the X-ray shows nothing.
Treatment for craniocervical instability includes physical therapy, neck bracing, and in severe cases, cervical fusion. Of these treatments, only physical therapy is without its problems. Neck bracing can lead to muscle atrophy and a worsening of symptoms so it should not be attempted without a doctor's supervision.
#chronic illness#chronically ill#cripple punk#physical disability#physically disabled#cripplepunk#ehlers danlos syndrome#craniocervical instability
87 notes
·
View notes
Text
Atlantis Expedition: Science Division Departments - Medical Department
Continuing from my starting post here, I'm now breaking things down by department, beginning with the Medical Department.
I did end up heavily revising this department after the commentary on the general departments post, and also after a lot of looking up of the actual divisions of medical specialties. So, first, the (new) numbers:
> Head: Carson Beckett (later, Jennifer Keller, later, whomever)
> Contains: Surgery, psychiatry, physical therapy
> Function: Maintaining health of expedition members
> Examples of function: surgeries, medical prescriptions, recuperation from injuries, mental stability
> Personnel quantity: 1 (Head) + 10 (surgical team) + 5 10 (nurses non-surgical team) + 1 (psych) + 1 (phys. therapy) + 1 (anesthesiologist) (grouped under non-surgical team) = 19 23 total
> A/N: Nurses have training in medications and physical therapy, surgical team also doubles as general practitioners
Information carried over from the first post, with struck text indicating revisions. The new total is 23, and the author's note is now irrelevant in light of new information. Mostly.
After doubling the amount of nurses, realizing "nurse" is a very broad category of medical professional with multiple definitions and aspects of job duties in multiple countries, I did a bit of renaming of the teams within this department: surgical, non-surgical, and miscellaneous (sorry guys).
Something I had realized was that this was not going to be a typical medical department (duh, in hindsight). These people are all going through the SGC, and the SGC quite likely not already has their own training protocols in place for dealing with SGC-specific situations, but also adapted technology from Goa'uld tech. What is Goa'uld tech? Appropriated Ancient tech, but without the gene component - fascinating, but also a post for another time.
This did inform how I revised which personnel to include, their specialties, and their duties. You're not exactly going to be shoving a whole MRI machine through a gate, so a radiologist isn't going to be a necessary specialty. Because of this, there's going to be a lot more cross-training, and more of a focus that's similar to what Atlantis would actually operate as: a forward operating base.
So, on to the teams (commentary included).
Surgical Team
> Personnel quantity: 10
> Minimum education: Doctorate in Surgery (ChM)
> All of these people are already trained in basic medical knowledge and practices, and also overall surgical practices in different areas of the body
Specialties
> Neurosurgery
> Dentistry | Oral and maxillofacial surgery
» In the US, trained to do general anesthesia and deep sedation
> Orthopedics
» Musculoskeletal
> Trauma surgery
» Can contain combat surgeons
» 2x of these
> OBGYN
> Urology
> Cardiothoracic
» 2x of these, by speciality:
⇛ Cardiovascular surgeon
⟹ "involving the heart and the great vessels"
⇛ Thoracic surgeon
⟹ involving the lungs, esophagus, thymus, etc.
> Surgical technologist
» "In the military they perform the duties of both the circulator and the scrub."
» Creates and maintains a sterile surgical environment
» Anticipates the work a surgeon needs to do
» Walking compendium of surgical techniques and stitches
I had wavered a bit on qualifications, and thus who to include - at the end of the day, it was probably going to be on an American standard, given the physical location of SGC. This meant I got to do a nifty thing of having my oral/maxillofacial surgeon be the dentist that's also an anesthesiologist, even if this is apparently considered odd in many other countries.
Mostly I wanted to go by section of the body, and see what kind of specialties there were, and what did and did not overlap. Surprisingly, it was more difficult to figure out who did abdominal surgeries than it was neurosurgery or dental surgery, hence two people in cardiothoracic surgery and two "general" surgeons in the form of trauma surgery because, again, forward operating base - they have no idea what Atlantis will be, so some assumptions will need to be made and better to err on the side of caution.
In a more delicate but still very necessary subject, one OBGYN (obstetrics and gynecology) and one urologist (aka urinary system and male reproductive system). For various obvious reasons, everyone's health in this area still needs to be taken care of, so it's better to have them on the team than politely handwave the idea.
Neurosurgery, for an obvious reason - it's highly specialized and without significant overlap, while also being a critical function on a surgical team with the demands the Atlantis Expedition will likely face.
Orthopedics are musculoskeletal, or deals with muscles and the skeletal system. A fair amount of what they do has overlap (see: trauma surgeons), but having someone specialized for the particularities of setting bones and handling surgeries on things like the joints is incredibly useful when presuming setting up camp in an active combat zone (which they really, really did).
Trauma surgeons are, more or less, the ones that you would see in an emergency situation - acute situations and their injuries are their specialty, and for this expedition likely the head of the surgical team by dint of their training to assess a patient quickly and develop a care plan very quickly. Because of this, I found the overlap of combat surgeons immensely helpful, which means that there's a significant probability that this surgical team has military personnel assigned to it. These surgeons are also the ones most likely to be SGC-imported, and trained to deal with things like injuries from Goa'uld and Goa'uld devices.
All these very highly-trained people, who are all probably very, very smart - who supports them? As it turns out, at least in the operating theater, not the nurses, but surgical technologists.
Surgical technologists main job, at least here, would be to set up the operating theater and anticipate whatever it is a surgeon needs in assistance. This includes things like training on a wide variety of surgical techniques (i.e. stitches), disinfection procedures, and medications such as anesthesia (ish). I included the quote about military duties because it saves money on how many people to include in the expedition, and penny-pinching is the backbone of any hiring process.
Now, the surgical team is all done! That's ten people right there, and on to the non-surgical team.
Non-Surgical Team
> Personnel quantity: 10
» 5 Technicians/Nurses, 5 Non-Surgical Medical Specialists
Nurses
> (Advanced Practice) Nurses
» 5x of these
» Registered Nurse
⇛ As the general minimum educational and experimental requirement
» Perioperative nursing
⇛ Assists surgical team, helps with pre- and post-surgical patients
» Emergency nursing
⇛ Can do triaging, suturing, casting/splinting, local/regional anesthesia, and other doctoral skills as needed
⇛ Likely the SGC training model incorporates all of the above, and also training on medical technology adapted from Goa'uld healing technology (which is really Ancient but without the ATA gene lock)
⟹ Radiology tech
⟹ MRI tech (which is radiology but a bit to the left)
⟹ Other adapted diagnostic equipment
Non-Surgical Medical Specialists
> Pathology
» 2x of these
» Coordinates with Life Science Department to develop diagnoses for novel diseases (in the Pegasus galaxy)
> Internal medicine | Internists
» 2x of these
> Anesthesiology
» For everything the OMS people don't do in terms of anesthesiology
» See also: Anesthesia (topic)
Remember how I said the qualifications were a doozy, and that nurses were a broad category? ... Yeah, this is why. The medical field is probably current in flux right now, given the shifting priorities of medical personnel and so much research that is still in the process of being applied, but I waved my magic plot-fixing wand and assumed the SGC figured this out for me.
All of these nurses are likely to be SGC imports, and thus unbelievably well-trained in everything that the SGC needs them to do. These are the personnel who know how all of the Goa'uld tech works on a functional level, have gotten the goodies first from engineering, and are waving their handheld MRI and other diagnostic equipment over their patients like a fairy godmother in scrubs. As with a real world hospital, these are the people actually running the show, and likely making the surgical team look like hypercompetent show poodles.
As for non-nurses who are also non-surgeons, pathologists are the ones who work up what people will actually be diagnosed with, figuring out all the newest and shiniest diseases and cataloguing them for reference. Doctor Biro is a pathologist, for example.
The thought occurred to me that we still need something resembling a general practitioner, but in light of fancy things like handheld MRIs and other scanners, this role is much reduced in favor of people who pack a greater intellectual punch.
However, I found that internists not only fill this gap, but are also hyper-specialized in their own way, in the respect of their knowledge base being internal diseases and multi-system diseases. Ergo, two of them, because they're just that useful. They'd probably coordinate quite a bit with cardiothoracic surgeons, as those are overlapping areas of study based on region of the body.
One (1) anesthesiologist, because the OMS cannot - nor should they - be the only person to perform anesthesia. This person functions as a sanity checker, and also the thin margin of the anesthesia that the surgeon doesn't cover.
We still need to round out this department, though. So far I've managed to cover in-patient, out-patient, and the various surgical stages. What else?
Well, recuperation - patients can't actually linger in the infirmary for the entirety of their healing process, for such practical reasons as beds available and boredom of patient, so the transitional phase needs to be covered.
Hence, the highly uncreative placeholder section name of Miscellaneous:
> Psychiatrist
» 1x of these, because canon says so?
> Physical therapist
» 1x of these, because canon says so?
Now while personnel such as nurses and internists are meant to convey educational material and instructions to patients about recuperation, it helps to actually have specialists on hand to make the patients commit to the bit.
Having only one psychiatrist on hand seems a bit of a Star Trek logical fallacy, but I'm once again waving my plot wand and assuming anyone that managed to get through the arduous employment process of 1) being told the Stargate exists (and coping with their world views being upended), 2) being employed by the SGC in general, and 3) passes their psychological assessment is probably mentally stable enough to only need one psychiatrist for the entire expedition.
(Yes, this does mean everyone on the expedition got their rubber stamp of sanity, and probably in grueling triplicate. Such as it can be defined a fanfiction-like world of scifi. I think they're coping pretty well with everything, no?)
With all the work that the surgical and non-surgical teams put into taking care of injured expedition members, a physical therapist is, as with everyone else here, very good at their job, but ultimately one of the last steps for patients that require longer term care. Think gaining back muscle after a broken leg, or more serious injuries that require months of guided exercise to be back to gate team-ready health (or general running for your life because Atlantis is just as dangerous).
Total Medical Department Personnel
Head of Department: 1
Surgical Team: 10
Non-Surgical Team: 10
Miscellaneous: 2
Total total: 23
I'll be going over headcanons on canonical personnel, such as Carson Beckett, Jennifer Keller, and Biro in their own posts, but for now this is a general accounting of the expedition's medical department.
Shout-out to @savestave and @stinalotte for the discussion and feedback on the original post!
21 notes
·
View notes
Text
mmm thinking about this because one of the vampire rules in the anne rice books is "do not turn the crippled/maimed," and, like obviously, well, it's anne rice, but... you see artists who do fun*, well-meaning things with vampirism and physically disabled people--what would a vampire with xyz mobility aid like? how would they hunt? sure, ok. *not personally particularly interesting to me for a variety of reasons that mostly have to do with The Vampire As A Symbol, but!!!
i have been thinking about vampiric transformation which effects physical "perfection" as a site of horror. if one turned me, and I "lost" the musculoskeletal disability I have had since birth, what would that do to how i recognize my body as mine, yknow? there's already this emphasis in lots of modern vamp media about fledglings having to adjust to their new, heightened senses and physical prowess: what about further disruptions to the body map--senses of balance, baseline mobility, silhouette and posture, sensorium. what are the standards of ability for vampires, and if all vampires meet that standard (in this hypothetical), what further degrees of trauma are visited upon those who fell far short of human standards in life?
#like sure there's plenty of turning sick or gravely injured ppl but i am tempted to write some kind of dissociative body horror shit about#suddenly being 'cured' of a lifelong 'impairment.' for fun.#txt#just waffling don't worry#vampires
15 notes
·
View notes
Note
I guess count another person on the list of “today I may have discovered a possible diagnosis for myself on TUMBLR of all freaking places.”
Does MCAS have common comorbidity with anything else? I see that is can cause all sorts of issues from pulmonary to gastrointestinal to musculoskeletal to neurological. Well guess who has various issues in all four of those categories! (Un)Lucky me.
I'd apologize, but it's kind of my schtick talking about it ^^;
And MCAS is often comorbid with conditions like Ehlers Danlos Syndrome or POTS, which is a type of dysautonomia.
For some of us, it seems to be present from birth, while others seem to develop it later in life, usually in response to a viral or bacterial infection or some other sort of stress or trauma. (Rates of patients with MCAS and c-PTSD are very high due to how stress hormones affect mast cells.) Covid has been causing people to develop mast cell instability. This is why so many more doctors are learning about it in quick time, though whether these people will develop long-term MCAS is unknown.
There's also some ongoing research that hypothesizes that Fibromylagia might be linked to it as well due to neuroinflammation MCAS can cause.
Basically, there's a chance it's linked to a lot of things, but research and medical acceptance have been so piss-poor until recently when covid caused a bunch of skeptical doctors to go "oh shit" and start throwing money at the research they've been neglecting for decades. Fingers crossed we see improvements in diagnosis and testing because right now, all of the lab testing is better suited for mastocytosis, which is somewhat better established.
469 notes
·
View notes
Text
Beyond Bones: Healix Trauma Care Revolutionizes Treatment For Orthopedic And Abdominal Injuries

In the realm of medical emergencies, trauma care stands as a beacon of hope for those facing life-altering injuries. Healix Hospitals, with its unwavering commitment to excellence, has pioneered Trauma Care that extends beyond traditional approaches, offering comprehensive solutions for orthopedic and abdominal injuries.
Let's delve into the innovative methods and specialized expertise that Healix brings to the forefront of trauma care.
What are some common orthopedic and abdominal injuries?
Certainly! Here's a more detailed rewrite of the content:
Orthopedic injuries encompass a wide array of conditions that affect the musculoskeletal system. These injuries commonly include:
Dislocations: Occur when the ends of bones are forced out of their normal positions within a joint. This can result from trauma or sudden impact, leading to pain, swelling, and limited range of motion.
Fractures and Breaks: Refers to the partial or complete breakage of bones due to trauma, overuse, or weakened bone structure. Fractures can vary in severity from hairline cracks to compound fractures where the bone pierces the skin.
Impingement Syndromes: Involve the compression of soft tissues between bones in a joint, often seen in conditions like shoulder impingement or hip impingement. This can lead to inflammation, pain, and restricted movement.
Sports Hernia: Also known as athletic pubalgia, it's a strain or tear in the soft tissue of the groin area. It commonly affects athletes involved in sports that require sudden changes in direction or intense twisting movements.
Overuse Injuries: Result from repetitive stress on muscles, tendons, ligaments, or bones without adequate rest and recovery. Examples include tendonitis, stress fractures, and muscle strains.
Sprains: Occur when ligaments, the tough bands of tissue that connect bones to each other, are stretched or torn. This often happens during sudden twisting or stretching movements, causing pain, swelling, and instability in the affected joint.
Abdominal injuries involve trauma to the area between the chest and pelvis and can vary greatly in severity and complexity. Common abdominal injuries include:
Contusions: Bruising of the abdominal wall due to blunt force trauma. While contusions may seem minor, they can sometimes indicate underlying internal injuries.
Lacerations: Refers to cuts or tears in the abdominal organs or tissues, often caused by sharp objects or severe blunt force trauma. Lacerations can lead to internal bleeding and require prompt medical attention.
Puncture Wounds: Penetrating injuries that breach the abdominal wall, potentially causing damage to internal organs such as the liver, spleen, or intestines. These injuries pose a risk of infection and internal bleeding if not treated promptly.
Herniations: Involve the protrusion of abdominal organs through weak spots in the abdominal wall muscles. Hernias can be congenital or develop over time due to factors like obesity, heavy lifting, or abdominal surgery.
Abdominal injuries can affect various vital structures, including the liver, spleen, pancreas, kidneys, stomach, small intestine, colon, ureters, bladder, and vasculature.
Blows to the solar plexus, a complex network of nerves located in the upper abdomen, are particularly common and can cause momentary paralysis of the diaphragm, leading to significant pain and respiratory distress.
Recognizing and promptly managing orthopedic and abdominal injuries are crucial to prevent serious complications such as chronic pain, loss of function, organ damage, and even life-threatening conditions like internal bleeding or sepsis. Seeking immediate medical attention and appropriate trauma care can significantly improve outcomes and facilitate recovery.
Read More: https://www.healixhospitals.com/blogs/beyond-bones:-healix-trauma-care-revolutionizes-treatment-for-orthopedic-and-abdominal-injuries
#Orthopedic and Abdominal Injuries#Trauma Care#Orthopedic Injuries#Abdominal Injuries#Emergency Medicine#Injury Treatment#Trauma Center#Fracture Management#Soft Tissue Injuries#Internal Injuries#Emergency Room#Trauma Surgery#Sports Injuries#Musculoskeletal Trauma#Critical Care#Surgical Treatment#Rehabilitation Services#Advanced Care#Injury Rehabilitation#Medical Emergency#Abdominal Trauma
1 note
·
View note
Text
My first attempt at Fanfic for the Fallen Hero universe. I am a science nerd in healthcare, so I'd like to try the first Dr. Halabi note as a SOAP (physician) note at Dr. Mortum's facility for my Sidestep (Arya).
Arya, as Retribution, is an anarchist set on justice and has been revealed to the Rangers, but Sky-Raider got her out before any of the Rangers could make a move.
__________________________
Note: These records are for internal use ONLY. Disclosure of these forms will be met with swift recourse.
Date: 5-10-21
Facility: Mortum Site 01
Patient #: 2344
Patient Name: Arya Skovsgaard
Gender: Female (She/Her)
Attending: Dr. Halabi, MD
CC: Traumatic MVA
HPI:
Arya Skovsgaard is a 30 y.o. AFAB transferred to Site 01 two days following a motor vehicle accident. Per LDPD reports, the patient was restrained, and airbags were deployed. The patient appeared to be driving down the opposite lane on a two-lane highway and struck an oncoming truck. The larger truck was undamaged, but the vehicle the patient was driving was no longer operable. The patient is a known telepath (T12345678), Alpha level. She is known to be capable of operating other individuals through telepathy. The patient was transferred from the care of the Los Diabolos’ Rangers prior to arrival at Site 01. Previous to this, they were at Memorial Hospital under the care of another, unknown physician, wherein lower extremity injuries were treated. The patient chart was consulted prior to transfer. During their stay at this facility, the patient was discharged to inpatient care with a bilateral tibial fracture along the mid-diaphyseal line and a right femoral fracture at the mid-epiphyseal line. Lastly, physicians at the Ranger facility note left SI joint disjunction. It is not known if the accident was intentional, but the Ranger discharge notes allude to this as a possibility. For this reason, the patient will be under constant security detail.
HPI is incomplete due to the current AMS.
ROS:
Patient arrived to facility in a state of alterted mental status leading to an incomplete ROS
Head: Positive for trauma
ENT: Negative for dental trauma
MSK: Grossly apparent damage to bilateral lower extremities
Integumentary: Positive for abrasions, lacerations, ecchymosis
Psych: Altered mental status
Neuro: Loss of consciousness
Physical Exam:
Physical exam from Dr. Petroza at time of surgery and reconstruction is included as a separate document. Below is Dr. Halabi’s secondary PE upon admission to Site 01.
Head: Trauma noted to bilateral orbitals. Ecchymosis around orbitals with classic appearance of trauma.
Neck: No trauma noted
Lymph: No abormalities noted.
Musculoskeletal: See diagram. Dr. Petroza and team applied bilateral leg casting to patient from femural head distally to ankle. Difficult to assess. Otherwise noted
CV: No murmurs, rubs, gallops. Normal rate, rhythm.
Respiratory: Some wheezing. Imaging from Ranger HQ shows no pneumothorax. Brusing to ribs, possibly due to CPR on scene.
GU: No abnormalities noted
Integumentary: Diffuse ecchymosis and bruising to regions visible, patient has [REDACTED] on skin noting them to be [REDACTED].
Psych: Unable to assess
Neuro: Unable to assess. Known telepath.
Assessment:
Agreement with prior disagnosis of bilateral tibial fracture along the mid-diaphsyeal line and right femoral fracture at the mid-epiphyseal line with protrusion from the medial right femur and bilateral media tibia.
Dipostion:
Inpatient discharge.
Progress notes:
5-20-21
2320: Call recieved that patient is en route.
5-21-21
0023: Patient arrives to Site 01.
0024: Dr. Halabi, attending, in room and performing phyical exam.
0100: Patient woke briefly and [REDACTED] attacked them - they were removed from the premises. Security was tightened on the room.
0300: Patient awakens and requests food. Dr. Mortum in room and discussion plan with patient.
0800: Phone call received on patients cell phone from number listed “Julia.” Voicemail left.
TRANSCRIPTION: “Arya, I know you’re out there. I… I’m glad. We’ll talk when you’re ready. I know you don’t want me to be around for this - but we need to talk. I want to help. I had some time to think… you might not have gone about this in the way I would have expected, but I think you have the right idea. Please call me. I love you.”
0830: Patient requesting discharge to their home. The Site will send her with an escort.
Electronic Signature:
Dr. Halabi, MD
This report is to remain within Site 01. If it is found outside of these servers, it should be destroyed, and the aforementioned party should be warned.
25 notes
·
View notes
Text
König HCs
Because why not lads. These are some of my personal ones regarding the lore I’ve put together for him. TW: untreated mental illness, childhood neglect, burn injuries, surgical trauma. Uh, some other shit, too, probably. Idfk reader beweader you’re in for a sceader.
Bro has BPD. It covers a lot of the beloved fanon interpretation of him being clingy and hot/cold and scared of being left. He’s got Fear Of Abandonment Syndrome, and he’s like 10% more likely to make a fucky wucky on himself and end up sleeping in the forever box.
Source: I have it and my baby girl only gets the best of the worst from me.
H a t e s d o c t o r s. And hospitals, and surgical procedures, and anything of the like. He’s probably already got more health issues than a blue blood racehorse just from his sheer size alone - prone to heart issues and musculoskeletal strain - but there’s no way on god’s green earth that he hasn’t been through a handful of major procedures because he’s diagnosed with human knife block and bullet sponge disorders respectively.
Sub-point A: born with a cleft palette and lip. Palette was corrected, has a turned second incisor as a result. Lip was botched. Pulled a pot of boiling sugar off a stove and burnt a big-ass portion of his face, neck, chest, and stomach. Multiple painful reconstructive and corrective surgeries to deal with keloid scarring.
Sub-point B: psychology might help OTHER people, but HE is built DIFFERENT. He’s not crazy, you see, and if you suggest otherwise you’ll suddenly develop a case of Backpfeifengesicht and he’ll provide the violence. DBT? That’s Dick and Ball Torture, babey.
Despite this, he lies through his teeth at psych evals. He knows the “right” answers, and he is not going to get his livelihood taken away from him, even if it’s not exactly what he wanted. If he’s answering for his own actions, he can swerve and intuit what thing will calm things down the most and get him the smallest punishment.
Developed most of his wheedling skills as a kid, parents were neglectful as shit. Mostly disregarded him during his upbringing. Youngest of three, an eldest sister and a brother. Not in contact with any of them.
He’s 34. I don’t know if I’ve accepted him being a Colonel into my heart as my lord and savior, I’m still figuring that one out until there’s more concrete canon material besides a loading screen.
Grew up in a hoarder house of apathy, alcoholism, and depression and it was DISGUSTING. Black mold, water damage, trash everywhere, travel lanes carved through the most useless fucking junk. His parents bred Doberman dogs to sell as guard/security dogs, and some lived in the house, adding to the filth and destruction. He can’t stand a dirty house, and as an adult has an insane cleaning routine. Often stress cleans. You could eat off his bathroom floors.
He Does Not Like Dogs. Period. He especially hates Dobermans. He doesn’t like dog breeders worth a fuck either, good or bad.
Did not have any sort of media or anything as a kid. Parents didn’t spend money on tech or pop culture stuff, they were kind of stuck 30 years behind everyone else. His parents were older when he was born, he was very unplanned and not particularly warmly welcomed. Kept himself entertained out in the boonies, did a lot of reading, learned to juggle, learned to juggle knives. Had a big brokedown half-draft horse to take the kennel dogs on longer walks in the country, horsebacked a lot.
Soon as he was in the army, away from his family home, and living on his own, he got his first cell phone and computer and pretty much started living on the internet. He’s self taught in a couple of programming languages, very tech literate, halfway kind of lives on Reddit (narrowly swerved getting redpilled, thank fuck) on his personal time, and built his own PC set up. Built one for Horangi, too, and gives Stiletto advice on her own build when she asks for it.
H E H A T E S K L A U S
Bc I said so, everyone I love hates Klaus. All my homies fuckin hate Klaus.
König was raised secular Jewish, really doesn’t know all that much about it and didn’t get a bris or bar mitzvah, it’s just like Yeah That’s What I Put On Papers to him. Klaus is always getting in his shit about Austria and WW2. König’s grandparents made it out of the camps and went on to become: a microbiologist, a professor at the Austrian University of Veterinary Medicine, a multi term mayor of a small village/candy maker, and a beloved homemaker. The brilliance of the family seemed to leech out with each passing generation, and König sees himself as the dead end of it all.
König has rocked Klaus’s shit about the shitty jokes before and will do it again.
Favorite rugby club is South Africa, and he has an intense crush on Faf de Klerk even though he’s been traded to Japan. He’s kind of hot for all scrum halves tho lbr here.
Lunch break is over and this is ridiculous, will probably do more later.
#könig#konig#konig call of duty#könig mw2#call of duty#mw2#konig cod#idk I just slap tags around and go hehe#my head canons
72 notes
·
View notes
Text
Bessel van der Kolk is a psychiatrist who wrote the best selling book “The body keeps the score”. There are 5 points to be made after reading his book.
Lesson 1: The Brain-Body Connection Is Real
When we experience a real or perceived threat, our brain's alarm system gets triggered. This alarm system involves a region of the brain called the amygdala, which Dr. Van der Kolk refers to as the brain's smoke detector.
Lesson 2: Trauma Causes Physical Symptoms
Being trapped in a prolonged state of emotional reactivity might change the way our body functions. According to The Body Keeps the Score, when we are chronically angry or scared, constant muscle tension might lead to spasms, back pain, migraine headaches, fibromyalgia (widespread musculoskeletal pain), and other forms of chronic pain.
Lesson 3: The Mind Is Not Tending To The Present Moment
Being traumatized is not simply a problem of being stuck in the past; it is also a problem of not being fully present in the here and now.
Lesson 4: We Have the Power to Regulate Our Physiology
If our brain activity has been impacted by trauma, our brainwaves are likely less coordinated than they should be. However, dysregulated brainwave patterns are not irreparable: they can be rewired and transformed thanks to a process called neuroplasticity.
Lesson 5: Positive Relationships Are Fundamental To Our Well-Being
As Dr. Van der Kolk states in The Body Keeps the Score, our attachment bonds are our greatest protection against threats. Nothing soothes our fear like a soothing voice or a solid hug from a trusted person.
.Information source: Written by: Dubravka Rebic ✓ Fact-checked by: Dr. Nathan Brown, Ph.D.
#the body keeps the score#bessel van der kolk#body and mind connection#trauma#cptsd#healing takes time#soulinkpoetry#poetry#she writes#thoughts#feelings#poets on tumblr#recovery
48 notes
·
View notes
Text
A collection of my Jason Todd headcanons/AUs
if you're here from a fic, all headcanons/aus/special power shit is in here.
if youre here for any other reason, you know what you're getting into.
That being said, warning for death and rape mentions
Here is a reminder that i have not touched canon, just been told that characterisation is bullshit, and i have attached myself via hyperfixation to jason todd.
When a headcanon is referred to being in all AUs, it means it fits in all of them. Not that they’ll be relevant, or that they have even happened yet.
This is present in all AUs. Jason was trafficked and raped when he was younger. This ties into the Siren AU, and Jason is really good at comforting victims. Mainly through music or song.
This can be adapted into any AU: for the genderbent version of Jason, her name could be Medea or Medéa. From the Greek Μήδεια Mēdeia, possibly meaning someone who is pondering or cunning. It is also the name of a sorceress in Greek mythology that took nobody’s shit.
This is present in all AUs. Fibromyalgia is a disorder characterized by widespread musculoskeletal pain accompanied by fatigue, sleep, memory and mood issues. Jason has chronic pain because he died, or if in Titans, because Trauma™. Sometimes it’s manageable, sometimes its crippling.
This is present in all AUs. When Jason was dead, he was in limbo. With him, was Death the Endless. She was actually very nice, and gave him the ankh, which shrinks down into a small but intricate tattoo on his left forearm, which allows him to shape his soul into anything, and when he does, the tattoo grows, spiralling out. Similar to the all-blades but far more versatile. He has hours until he needs to stop using it to stay alive. Death also talked with him and became an almost aunt or grandmother-like figure, which is true, considering her child is Gotham, and Gotham’s child is Jason.
There was a lady. With wild black hair, reaching her hand out, smiling at him. And a lot of red. And it was so quiet , oppressively quiet, the kind that traps you and drowns you and eats you from the inside out. Moonlight shines through the warehouse window. It reflects off the container, and his eyes glow green. (link)
This is present in all AUs. Gotham is sentient, and is the daughter of Death the Endless, and is Jason’s mother (technically). Jason is intertwined with Gotham, and the shadows show that. Jason has claimed the people of Crime Alley as his, so Gotham helps hide them: they can manipulate the shadows, disappear, and resist death, though not to the extent Jason can.
In any AU marked at the bottom with ‘Eldritch Gotham Shadow AU’, Jason is more eldritch than others. He manipulates the shadows and has a much larger well of power. He is the grandchild of Death the Endless, and here, both Gotham and him actually show the fact that they are eldritch cosmic entities, bound by breaking string into the husk of a city and a man respectively. However, the power is hard to control and is inaccessible most of the time. Major impacts are weird shapes in peripheral vision etc.
In any AU marked at the bottom with ‘Reflection AU’, the damage done to Gotham is reflected onto Jason. If there is a bomb, Jason will have a burn the same percentage of his body that the bomb destroyed of Gotham. When Gotham is heavily damaged, Jason is also extremely injured, but he can delay injuries reflecting onto him with the use of some runes. In some AUs, the reflection isn’t 1:1, and it doesn’t hurt Jason as much, but he is still injured. Being a mirror also grants him the ability to know almost everything happening in Gotham always.
In any AU marked at the bottom with ‘Shifting Inks AU’, Jason, when he was with the All-Caste or when he was dimension walking with magicks, he was tattooed with magic ink. The ink can change forms, but no matter what form the ink takes, it is vibrant and strong. Sometimes the ink takes the form of runes hidden inside art, or hints from Destiny and/or Dream the Endless.
This is present in all AUs. The people of Crime Alley call Jason’s gang the ‘Merry Men,’ after the group that Robin Hood led. This catches on, and now they’re unofficially called the Merry Men. To refer to multiple of them, they’re called Merries, and to refer to one, they’re called a Merry. They are all very close, and mostly consider each other family.
In any AU marked at the bottom with ‘Lazarus Pit Regeneration AU’, coming out of the Lazarus Pit would only heal injuries that are open(not scars, nor malnutrition)/ incapacitates them (makes movement impossible or extremely hard) so Jason is shorter, (maybe 5’5” maybe 5’6”, 5’7” at most - to the 5’4” he was at 15 and the 6’0” he was at 21), and has the build of a gymnast: compact muscle and packs a punch.
This build was inspired by my sister, who is only 5’4” but is an international medalist and can deadlift about three me’s at once. Also, I hate the fact that DC didn’t really have major diversity early, because, come on, be a little creative. Canon Jason is just Bruce but shorter and a little wider.
In any AU marked at the bottom with ‘Soul and Ghosts Sight AU’, Jason can always see ghosts and help them find peace and move on if they want to. He can also see people’s souls, and when he was young, he judged on instinct how safe they were. When he’s young, he’s brutally honest about what he sees and knows, which surprises a lot of people, but he can also get high off of positive emotions because he wasn’t exposed to them often when he was young. The soul reading (as he gets older) changes into seeing the presence of Death the Endless around someone, which – based on the shade - tells him how many people they’ve killed, how many people they know have died, how many people have died as a result of something they’ve done (not purposefully trying to kill), what deaths they blame themselves for, how close they are to dying, and their magic if they have any.
In any AU marked at the bottom with ‘Fire in His Veins AU’, Jason has fire in his veins. It makes him a heat pack. The Bats don’t know this, and when he gets really pissed off, it leaks out of his skin. Jason is involved in the magical community of Gotham. His ‘base power’ is the fire-lava veins thing, but it can be adapted into runes and constructs and shit. Anyways, he helps the magical community, and they all love him.
In any AU marked at the bottom with ‘Nonna Force AU’, the grandmothers, the aunties, the mothers, band together to make Crime Alley healthy. Heavily ties in with the Merry Men being family. All Nonnas are magical, all-powerful, omnipotent beings, and they are never called by their names, only variations of their title.
In any AU marked at the bottom with ‘Siren AU’, Jason has magic channelled through his voice, and he doesn’t sing a lot at all because of it. When he’s comfortable, he will, and some songs with memories attached/plot devices use golden magic to make constructs. He can also hear the songs of people’s souls, as well as those associated with memories. The Siren’s Blessing is something that was passed through Catherine’s maternal line, and when extremely desperate, those with the Blessing can call upon the Oceans, and this summons a few very pissed off Sirens. Because of the connection, Jason is friends with some Atlanteans, and he can also swim fast, breathe underwater, and heal quicker.
He loved singing as a kid, and Crime Alley knew Jason and Jeslyn as the Songbirds- not vigilantes, but if you get a good song, you get lucky. He learnt that singing could also get him in trouble and found out, so he only ever did it with Jeslyn or in private. They can also hear each other sing whenever they are singing, and when they sing the same song and aren’t near each other, golden constructs of them appear with each other, and when another person is sung to that also was Blessed/had a magical anchor, they could also project to them (as well as the Blessed who died, like Catherine), and any person who they have sung to. The Blessing is not designed to be hostile, but, because they have magic, they can cast spells and draw runes, even though it is hard to wield as an offensive power. However, when saying a vow (threatening, promising, being intimidating) their voice layers with others that stand by the vow as well.
In all AUs, Jason also has siblings, the oldest being Antonio, who was 10 years older than him and very dead, having been pulled into gangs by Willis. His closer siblings consist of Jasmine, a sister 4 years older, and then Jeslyn, his fraternal twin who is older than him by a few minutes. Jason is the tiny one of the family, as Jasmine is built a little like Willis and Jes is tall and willowy. Jes also has the Siren’s gift. But when they first got it, they were stuck in amber for like 2 years, and so Jes and Jay are 2 years younger than their birth certificates. In some AUs, Jay’s siblings are dead.
---
ok
if i use these to write oneshots, the AU/s in them will be mentioned at the bottom!
if you wanna use one of my headcanons, please credit me and tell me bc i wanna read it.
#jason todd#jason todd angst#jason todd headcanons#jason todd headcanon#jason todd fic#maybe?#yeah#there will be#jason todd is the youngest child here#and mostly#robin!jason#i also managed to hyperfixate on the titans show version of jason within the last 48 hours#so#eeeeeeeeeee#many fics planned#so many#question is: motivation?
8 notes
·
View notes
Note
As a continuation of my previous Ask, the life of Canon Sunny and Omari AU Mari are really sad if you think about it, not only were they suffering mentally because of the Trauma of the incident but also physically because of the stress cause by their trauma and mental problems
made worse with the fact that they probably never went to see a therapist or a doctor during those 4 years they shut away as stress can actually damage various system of the body if left untreated (Nervous Sytem, Musculoskeletal System, Cardiovascular System, ect)
Oh definitely. But it's hard to think about who would be in the worse conditon because they're both just plain frail phycially, but for different reasons.
Sunny is phycially frail because the accident happened when he was 12 so the stress and trauma took a toll on his body and stunted his body growth by not being in a healthy enviorment to properly advocate for puberty. Hence why when he's 16, he's only JUST as tall as Mari was at 15- even though he should be taller since boys tend to have more frequent or more drastic growth spurts.
While Mari is physically frail as well but this being further progressed due to her fractured knee. Due to her sleeping for most hours of the day, she's barely getting any exercise to help keep her bad leg in a good condition at best. So because of that, I can actually see Omari Mari having either her leg brace and a cane OR due to her numb and tuned out state, she more than likely just limps around the house. not really bothering to take care of her leg due to her thinking she more than likely deserves it.
And in terms of outside infulences, we can't say for sure who's worse off here because people can write OMARI's story however they want. In Canon, the Dad disowns his son and divorces his wife, that ending with him leaving. But with OMARI, it can either be the Mom leaving or Both parents stay for their daughter's sake (since it's pretty well implied that Mari was their favourite out of their kids)
But yeah... Canon Sunny and OMARI Mari are just heartbreaking and need to comfort each other. Despite them being alternate versions of their dead sibling, they're still brother and sister and this is the closest sibling relationship I've ever seen in media.
#omori#omori game#omori spoilers#ask response#text post#text response#omori: omari#omari au#omori mari#omori sunny#mod mack#mod ask
14 notes
·
View notes
Last Seen Blogs

cheesehambu
CheeseBurger🧀
jinjjae
derp.

rajeshwaridatta
@RajeshwariDatta

bigmoneyy1-blog
Untitled

king-pootis
King Pootis of Pootopia