#Schema Therapy
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Premium Tumblr themes are available from anywhere between $9 to $49.
Text
therapy resources / schema therapy / dbt/dialectical behaviour therapy / internal family systems / meditation / c-ptsd etc. resources
this is a link to my personal google drive, it has lots of dbt stuff, some random other resources that either i or my friends have found helpful incl. DID/OSDD/dissociation resources, & some handouts from a personality disorder program i did (was aimed at pplwbpd officially but the staff all refer to it as the "personality disorder clinic", fwiw)
bunch of other stuff under the cut including video content if that's more your thing
DBT stuff
this subreddit is a wonderful community, usually helpful with questions & has some resources linked also:
https://www.reddit.com/r/dbtselfhelp/ https://dbtselfhelp.com/
TIPP skills (from dbt/distress tolerance unit but deserves distinction. biochemical benefit > psychological benefit. at least for me)
https://manhattancbt.com/dbt-tipp-skills/ https://in.nau.edu/wp-content/uploads/sites/202/TIP-Skills.pdf
also emotional freedom tapping / eft (not a tipp skill iirc but it should be, one of the few things that kinda works for me)
https://www.health.com/emotional-freedom-technique-8399985
SCHEMA THERAPY
"client's guide to schema therapy"
https://disarmingthenarcissist.com/wp-content/uploads/2021/09/clientsguideSchemaTherapy.pdf
(the website name is very questionable but i can't find the pdf for free anywhere else orz. this is a good starting point for schema therapy tho. sorry y'all. i will steal it for my google drive when i have time)
https://www.psychologytools.com/professional/therapies/schema-therapy
^THAT LINK stuff is not free!!! BUT you can find a lot of them with this google search:
[title of worksheet/handout] -site:psychologytools.*
ex. i search the following: "unhelpful thinking styles" -site:positivepsychology.* ...and this pops up, tadaaaa:
https://talkheart2heart.org/resources/unhelpful-thinking-styles/
(i'm just linking the paid site because i cant find them gathered like that anywhere else… dont have time to search each one individually rn lol. maybe another day)
free stuff:
https://positive.b-cdn.net/wp-content/uploads/2021/01/Schemas-Needs-and-Modes-Reference-Sheet.pdf (overview) https://bmcpsychology.biomedcentral.com/articles/10.1186/s40359-020-0392-y/tables/1 (more detailed info on each schema) http://www.schematherapy.com/id72.htm (more info on modes) https://positivepsychology.com/schema-therapy-worksheets/ (a few worksheets linked on that page)
if video content is more your thing:
DBT UNITS:
interpersonal effectiveness extras: https://www.youtube.com/playlist?list=PLwPrhSDQ0V_tBg36U3wWZpLopxJBurSsq
"middle path" skills: https://www.youtube.com/playlist?list=PLwPrhSDQ0V_uB2e7Y570ihYBEYd7dK9Sv
"radically open" skills: https://www.youtube.com/playlist?list=PLwPrhSDQ0V_udTjVVHhz5e1wzOSDyVeN2
DBT expanded edition: https://www.youtube.com/playlist?list=PLwPrhSDQ0V_vjlYkkflUDRmfhw_hM13M-
more DBT, videos by Dr. Thomas R. Lynch: https://www.youtube.com/playlist?list=PLkKKzTWUSjRhnRr5Pe2GMA7VDg_E8wBcm
DBT skills animations:
https://www.youtube.com/playlist?list=PL4Qw4-tlRJe-T2l5MtFOsLkTIkfZqjobY
--
FAMILY SYSTEMS + ATTACHMENT
Patrick Teahan channel:
(great channel run by a mental health practitioner who has experienced childhood trauma, he gets it. check out the playlists tab. he also has some free resources/worksheets on his website which is linked on his channel iirc)
attachment styles playlist by Jennifer May, Ph.D: https://www.youtube.com/playlist?list=PLwPrhSDQ0V_smHuEjj2CxW4u7J_FozLlS
Crappy Childhood Fairy channel: https://www.youtube.com/@CrappyChildhoodFairy/playlists
(cptsd content mostly, haven't watched much of her stuff but i liked what i did see. she isn't certified but she is someone who experienced childhood trauma as well).
healing cptsd (small channel, few videos but good info iirc): https://www.youtube.com/@healingfromcomplexptsd2767
MEDITATION
(i cannot recommend her channel enough… i don't watch her longer videos/seminar(?) stuff but her meditation videos are like. actually helpful lol? i find a lot of that stuff not helpful at all but something about her is very calming and open and grounding. love her)
--
MISC
Rachel Richards massage channel:
https://www.youtube.com/@rachelrichardsmassage9660/playlists
(she has some great videos for somatic symptoms... some playlists focus on anxiety relief, breathing/relaxation, posture/mobility, sleep, etc.)
-
Dr Daniel Fox channel:
https://www.youtube.com/@DrDanielFox/videos
(cw: ableism/ableist language toward cluster b's is present on this channel, he just has a LOT of videos so i include the link... like if youre looking for something specific to do with pd traits, there's a good chance you can find SOMETHING here. *i have mixed cluster b traits incl. the more demonized ones disclaimer*. but yeah steer clear if that bothers you)
-
Struthless channel:
(mostly adhd/exec dysfunction/motivational advice stuff but i find his videos like actually kinda inspiring/motivating so i'm including it here since not a lot of stuff... feels motivating to me at all ever. but i never regret clicking on his vids! good motivational speaker lol)
-
that's all i can think of rn please lmk if any of the links are broken or like... if you have a question u think i can help w ^-^
#ptsd resources#dbt skills#schema therapy#interpersonal effectiveness#trauma therapy#dialectical behavior therapy#actually cluster b#internal family systems#cptsd therapy#actually traumatized#ok i dont feel like putting more tags ... goodbye#x#btw the did resources don't include anything about integration... they're journal/symptom trackers#and stuff that helps with healthy multiplicity. total respect to both end goals but i do not have resources specific to integration#context this is a response to someone asking what to do when ur issues are too complex for therapists/no one will take you#i spent over 13 years in therapy and this is my 2 cents#because not a lot of stuff helps me lol#i have mixed cluster b traits and some other dxes#complex trauma#and therapy has been harmful for me many times. these things are ACTUALLY helpful to me. hopefully to anyone who sees this also
59 notes
·
View notes
Text
Entry #008
Flashcards
To deal with all the information that I find out on this journey of unmasking, I create flashcards. They help me remember what triggers I’ve got, how I get overwhelmed and what I can do to make it better. I have several structures.
Trigger flashcard
These flashcards are based on creating specific distressing behavioural plans (in advance) for certain situations, not as much for acknowledging and challenging the feelings and thoughts that accompany those triggers. Because sometimes it’s easier to acknowledge that you got triggered, than the emotions or thoughts that accompany these moments. The focus is therefore solely on calming your nervous system down. These trigger flashcards can change a bit per situation, they are really personally designed for each situation.
Right now I got triggered by (trigger / situation), which makes me feel (uncomfortable emotion).
It’s okay I got triggered by (trigger / situation) and feel (uncomfortable emotion). Because my ((list of) sensory system) gets also (overstimulated/understimulated) by the (trigger/situation).
To help me feel (comfortable emotion), I could ((list of) distressing behaviour). This has supported me in the past to feel (comfortable emotion).
Mode flashcard
They help identify the mode involved, how it was originated and how it distorted my experience or understanding of the world. When the schemata are too abstract for the moment I can use these. They test the reality and help follow the alternative behaviour through. I made two types, because sometimes I can recognise the mode more easier than the emotion that lead to the mode and one emotion is not exclusive to one mode.
Right now I feel (emotions / feelings), because (trigger / situation).
However, I know that this is my (mode). Which I learned through (origin). This leads me to exaggerate the degree to which (behaviour distortion).
So, even though I believe (negative core-believe). The reality is that (healthy view). This is supported by (life examples).
Therefore, even though I feel like (negative behaviour). Instead I could (alternative healthy behaviour).
Or
Right now I am in (mode), which makes me feel (emotion / feelings).
However, this (mode), which I learned through (origin). Got triggered by (trigger / situation) and leads me to exaggerate the degree to which (behaviour / cognitive distortion).
So, even though I believe (negative core-believe). The reality is that (healthy view). This is supported by (life examples).
Therefore, even though I feel like (negative behaviour). Instead I could (alternative healthy behaviour).
Schema Flashcards
They are based on validation and acknowledgement of the current feelings and trigger / situation, they help identify the main schema involved, how it was originated and how it distorted my experience or understanding of the world. They test the reality and help follow the alternative behaviour through.
Right now I feel (emotions / feelings), because (trigger / situation).
However, I know that this is my (early maladaptive schema). Which I learned through (origin). This leads me to exaggerate the degree to which (schema distortion).
So, even though I believe (negative core-believe). The reality is that (healthy view). This is supported by (life examples).
Therefore, even though I feel like (negative behaviour). Instead I could (alternative healthy behaviour).
Or
Right now my (early maladaptive schema) got triggered by (trigger / situation). This makes me feel (emotions / feelings).
However, I know that I learned this schema through (origin). This leads me to exaggerate the degree to which (schema distortion).
So, even though I believe (negative core-believe). The reality is that (healthy view). This is supported by (life examples).
Therefore, even though I feel like (negative behaviour). Instead I could (alternative healthy behaviour).
Integration
In another post I will create an example of how I use the trigger schema and the flashcards. I will also probably edit this post sometime later on, but for now it is just a start. Because I have also combined a few flashcards with a mode flashcard structure and a trigger flashcard structure, as well as a schema flashcard structure with trigger flashcard structure. It’s just not one clear structure for both combinations yet. So as soon as I’ve figured that out I’ll include it as well.
#actually autistic#aspergers#aspergers syndrome#autism#autism spectrum disorder#autistic#autistic adult#autistic community#autistic spectrum#being autistic#high functioning autism#unmasking autism#high masking autism#autistic things#autistic stimming#autistic experiences#early maladaptive schemas#schema therapy#schema modes
20 notes
·
View notes
Text

60 notes
·
View notes
Text
Initial ask | @chaos-in-one
A Schema Therapy Approach to CDD in a Cross-Cultural Setting: A Single Case Study
Alberto Barbieri [1], Federica Visco-Comandini [2], Alessandra Trianni [3], Angelo Maria Saliani [4]
Published: June 13, 2022
Claims
Complex Dissociative Disorders (CDDs) include Dissociative Identity Disorder (DID) and Otherwise Specified Dissociative Disorder - Type 1 (OSDD-1).
CDD patients are highly impaired and need a lot of (expensive) treatment that may not be accessible to the target demographic.
Migrants/refugees are at high risk of developing trauma and trauma-based/dissociative disorders. They would benefit from therapy that balances their cultural needs with productive treatment.
Point of study
Schema Therapy (ST) is being proposed as a solution to effectively treating CDDs and trauma patients of every culture (not just Westerners). ST is an integrative psychotherapy: a type of therapy that mixes and matches different practices and teachings. It's made to be flexible so the therapist can adapt to the patients needs in therapy.
This study looks at one patients experience with ST to evaluate how effective it really is at treating patients with CDDs.
Participant Demographic
Patient - male; 38 years old; Yemeni refugee; is said to have OSDD-1, PTSD, and BPD
2 Italian therapists in a co-therapy environment; one male, one female.
Arabic interpreter and cultural mediator
Treatment was provided in Italy.
Procedure
Examine the process of individual therapy (meaning the focus is on one patient, not a group) using ST practices.
Specifies a three phase-based approach: a way of going about therapy in 3 "phases": stabilizing the patient by introducing coping mechanisms, building trust, and helping them feel safe in therapy; trauma memory recall and processing; and integrating what was learned to the patients life outside of therapy while encouraging re-socialization.
Assess for change in the patient. They had the patient assess himself for dissociative symptoms, PTSD symptoms, and how well he felt he was willing to cooperate with his therapists. He also had to self-report his cognitive schemas; basically how he interprets things and how he feels/reacts as a result.
The study took place over the course of 2 years and 4 months of treatment on top of an additional 6 months for follow-up.
Results
Reminder that the term "significant" does not mean the same thing in research as it does in everyday/social contexts! "Significance" in research is determined by the "p-value". So if the calculated results are lower than the set "p-value", that means that they are psychologically significant.
In this particular study, they used patient self-assessments to determine improvement.
Comparing self-assessments from early in the patients therapy to the follow-up assessments showed significant improvement in dissociative and PTSD symptoms. Also showed significant improvement in some cognitive schemas.
Despite limitations, results suggest that 3-phase ST may be an effective way of treating CDDs.
Limitations/implications
Case study - case studies are good for close examination but aren't very good for application outside of the study (referred to as generalization and ecological validity). That is, to say, the procedure had positive results for this specific case study, but it may not be the same for other people of a similar demographic/in other countries.
Language barrier - since there was an interpreter needed, some of the patients feelings or expressions may have been "lost in translation", so to speak. However, the patient provided his own art regarding his trauma and disorder which aided mutual understanding.
Cultural differences between therapists and patient - could have been another source of misunderstanding but didn't seem to keep the patient from connecting with his therapists (he scored his feelings of cooperation and understanding with them very highly by the second and third years of treatment).
Presence of a CDD - results for patients with CDDs can be inconsistent. It's difficult to tell which "self-state" did the assessment and whether or not that "self-state" was being honest (direct quote says "self-states may inhibit truthful responses"). It is recommended that future studies use the "integration measure" to test how integrated the patients "self-states" and sense of self is over the course of therapy.
Issues with assessment material - the researchers state that there are very few studies with very small samples that check the validity and reliability of the Arabic dissociation/schema assessments. They also had to use an Italian version of the self-reported patient-therapist alliance (cooperation) assessment, since there wasn't a version of it available in Arabic.
Timing of follow up assessment - 6 months after therapy is not enough time to accurately check the patients stability. The results would benefit from a longer term follow-up.

Other
NOTE: THIS SECTION IS A WIP SO THE OUTLINE (above divider) GOES PUBLIC UPON COMPLETION
Anything else from the study that we think will supplement the above outline, think is cool, or just feel is worth reiterating will go here!
[TBA]
We welcome all comments, questions, and concerns - there is no such thing as a stupid question and critique of our summary is always accepted. We are not perfect, please correct us when needed. Thank you for reading!
#syscourse#case study#complex dissociative disorder#co-therapy#cross-cultural psychotherapy#schema therapy#otherwise specified dissociative disorder type 1#osdd 1#borderline personality disorder#bpd
5 notes
·
View notes
Text
my life rn
6 notes
·
View notes
Text
trying to dismantle my social isolation/alienation schema feels like walking around a huge block of ice trying to melt it with a kitchen blowtorch
but! I noticed the vulnerability schema has reduced a lot and it’s something I’d like to stick to
2 notes
·
View notes
Text
*receives text from my mother* *sighs* *opens google* *searches ”18 maladaptive schemas”*
3 notes
·
View notes
Text
Friday, March 22nd
After the breathwork session, while I was taking a shower, tears mingled with the water as I begged God for forgiveness. Memories of the abuse at home flooded back, overwhelming me with guilt once again. It felt like I deserved it somehow, like I was just a disobedient kid who deserved punishment. That’s what they always told me, and too often, I believed them. I endured being hit, yelled at, threatened, and punished for things they thought I did wrong. And it always came with shame. They made me feel like I was a disgrace, like I should be ashamed.
In the days following the breathwork session, I was once again confronted with the realization of how strange it is to feel safe in unsafe environments. The very place and people that were supposed to be my refuge turned out to be both safe and unsafe. Several years ago, Schema therapy helped me come to this realization, but it’s a contradiction that still baffles me.
The contradiction not only affected my sense of safety but also influenced the relationships I attracted. It led me to form unhealthy relationships and prevented me from establishing healthy boundaries. While I’ve seen some improvement in recent years, it remains a work in progress. I continue to work on setting boundaries and cultivating healthier relationships, and though there have been improvements, I acknowledge that there’s still work to be done.
Despite the progress, the journey can feel lonely at times. There’s a longing to be understood, held, and comforted when things get dark and heavy. But it is what it is, and I’ve made a promise to myself not to be driven into the wrong arms again.
In the days after the session, I also found that I had more space within myself, allowing room for compassion. I realized that I didn’t deserve what my parents put me through. So my prayers have changed, and I now ask for more courage, strength, and self-compassion as I continue on this journey.
#personal#healing#breath work#emotions#inner child#schema therapy#God#guilt#shame#grief#unhealthy relationships#emotional intimacy#healthy relationships#boundaries#self care#self reflection#self love#220324#0324
6 notes
·
View notes
Text
Entry #004
Schema therapy
I love schematics. I love making and filling out schemata. I therefore use the theory of schema therapy a lot, and integrated dialectical behavioral and acceptance-commitment therapy as well.
It really helped me to figure out how much masking I was actually doing and creates some backbone to create alternative ways to healthy unmask and get support. So to help you understand what I’m talking about, I’m writing out the theory down below.
If you want to figure out what maladaptive schemata you have, you can fill out the Young Schema Questionnaire (YSQ-L3 or YSQ-S3 – long or short form)
Schemata
There are 18 early maladaptive schemata that people can have developed during their childhood and adolescence. They get developed by basic emotional needs that did not get met. It’s also really based on personality and temperament if and how a schema gets developed and coped with.
Abandonment
Mistrust and Abuse
Emotional Deprivation
Defectiveness and Shame
Social Isolation
Dependence and Incompetence
Vulnerability to Harm and Illness
Enmeshment and Undeveloped Self
Failure
Entitlement and Grandiosity
Insufficient Self-Control and Self-Discipline
Subjugation
Self-Sacrifice
Approval and Recognition Seeking
Negativity and Pessimism
Emotional Inhibition (Emotional Constriction and Fear of Losing Control)
Unrelenting Standards and Hypercriticalness
Punitiveness (Punitiveness to Others and Punitiveness to Self)
The schema “Emotional Inhibition” can be split up into “Emotional Constriction” and “Fear of Losing Control”, just like schema “Punitiveness” can be split up into “Punitiveness to Others” and “Punitiveness to Self”. This got proposed by Yalcin in 2021 in his paper (Yalcin, O., Marais, I., Lee, C., & Correia, H. (2021). Revisions to the Young Schema Questionnaire using Rasch analysis: the YSQ-R. Australian Psychologist, 57(1), 8–20. https://doi.org/10.1080/00050067.2021.1979885). You can fill out their revised schema questionnaire to make the distinction between those with the YSQ-R.
And now..
You can create a model of your schemas in how much they affect you. This is my model:
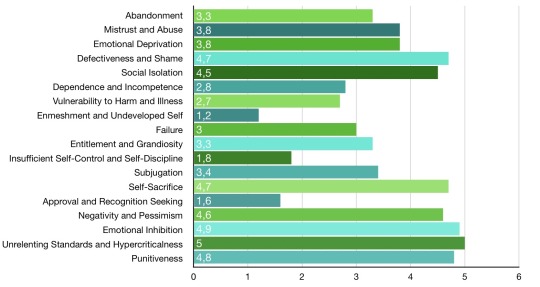
I use this model in my trigger schema to identify unhealthy or unhelpful behaviour. Because most of the time when I get triggered, one of my schemas gets triggered as well. This has led me into masking my autistic symptoms or tendencies, but isn’t necessarily helping me to have a balanced lifestyle. I will explain the trigger schema another time.
There are three coping styles or strategies to each schema, surrendering, overcompensation and/or avoidance. For these coping styles we have modi, which helps us give insight into what we feel and think and how we behave. But more on that another time.
Explanation per schema
Down here I’ve put the explanations per schema. The explanations are mainly taken directly from the book Schema Therapy: A Practioner’s Guide, and I slightly modified it in some parts, which is written in italics (Young, J. E., Klosko, J. S., & Weishaar, M. E. (2003). Schema therapy: A Practitioner’s Guide. Guilford Press. p. 14 - 17.).
Abandonment and Instability
The perceived instability or unreliability of those available for support and connection. Involves the sense that significant others will not be able to continue providing emotional support, connection, strength, or practical protection because they are emotionally unstable and unpredictable (e.g., have angry outbursts), unreliable, or present only erratically; because they will die imminently; or because they will abandon the individual in favor of someone better.
Mistrust and Abuse
The expectation that others will hurt, abuse, humiliate, cheat, lie, manipulate, or take advantage. Usually involves the perception that the harm is intentional or the result of unjustified and extreme negligence. May include the sense that one always ends up being cheated relative to others or “getting the short end of the stick.”
Emotional Deprivation
The expectation that one’s desire for a normal degree of emotional support will not be adequately met by others. The three major forms of deprivation are:
Deprivation of Nurturance: Absence of attention, affection, warmth, or companionship.
Deprivation of Empathy: Absence of understanding, listening, self-disclosure, or mutual sharing of feelings from others.
Deprivation of Protection: Absence of strength, direction, or guidance from others.
Defectiveness and Shame
The feeling that one is defective, bad, unwanted, inferior, or invalid in important respects or that one would be unlovable to significant others if exposed. May involve hypersensitivity to criticism, rejection, and blame; self-consciousness, comparisons, and insecurity around others; or a sense of shame regarding one’s perceived flaws. These flaws may be private (e.g., selfishness, angry impulses, unacceptable sexual desires) or public (e.g., undesirable physical appearance, social awkwardness).
Social Isolation and Alienation
The feeling that one is isolated from the rest of the world, different from other people, and/or not part of any group or community.
Dependence and Incompetence
Belief that one is unable to handle one’s everyday responsibilities in a competent manner, without considerable help from others (e.g., take care of oneself, solve daily problems, exercise good judgment, tackle new tasks, make good decisions). Often presents as helplessness.
Vulnerability to Harm or Illness
Exaggerated fear that imminent catastrophe will strike at any time and that one will be unable to prevent it. Fears focus on one or more of the following:
Medical catastrophes (e.g., heart attacks, AIDS)
Emotional catastrophes (e.g., going crazy)
External catastrophes (e.g., elevators collapsing, victimization by criminals, airplane crashes, earthquakes).
Enmeshment and Undeveloped Self
Excessive emotional involvement and closeness with one or more significant others (often parents) at the expense of full individuation or normal social development. Often involves the belief that at least one of the enmeshed individuals cannot survive or be happy without the constant support of the other. May also include feelings of being smothered by or fused with others or insufficient individual identity. Often experienced as a feeling of emptiness and foundering, having no direction, or in extreme cases questioning one’s existence. Also includes parentification to siblings.
Failure
The belief that one has failed, will inevitably fail, or is fundamentally inadequate relative to one’s peers in areas of achievement (school, career, sports, etc.). Often involves beliefs that one is stupid, inept, untalented, lower in status, less successful than others, and so forth.
Entitlement and Grandiosity
The belief that one is superior to other people; entitled to special rights and privileges; or not bound by the rules of reciprocity that guide normal social interaction. Often involves insistence that one should be able to do or have whatever one wants, regardless of what is realistic, what others consider reasonable, or the cost to others; or an exaggerated focus on superiority (e.g., being among the most successful, famous, wealthy) in order to achieve power or control (not primarily for attention or approval). Sometimes includes excessive competitiveness toward or domination of others: asserting one’s power, forcing one’s point of view, or controlling the behavior of others in line with one’s own desires without empathy or concern for others’ needs or feelings.
Also includes the feeling that one is responsible for things one is actually not really responsible for or can be held accountable to. The feeling that one should always be the one to help, e.g., because of the assumption that others will not step up to it.
Insufficient Self-Control and Self-Discipline
Pervasive difficulty or refusal to exercise sufficient self-control and frustration tolerance to achieve one’s personal goals or to restrain the excessive expression of one’s emotions and impulses. In its milder form, the patient presents with an exaggerated emphasis on discomfort avoidance: avoiding pain, conflict, confrontation, responsibility, or overexertion at the expense of personal fulfillment, commitment, or integrity.
When people are very punitive and have unrealistic standards, they often think they have this schema as well. Except they actually are having such high expectations of themselves that it is practically impossible to meet them (all). Then, they don’t actually have this schema, but rather only have hypercriticalness and punitiveness as schemata.
Subjugation
Excessive surrendering of control to others because one feels coerced — submitting in order to avoid anger, retaliation, or abandonment. The two major forms of subjugation are:
Subjugation of needs: Suppression of one’s preferences, decisions, and desires.
Subjugation of emotions: Suppression of emotions, especially anger.
Usually involves the perception that one’s own desires, opinions, and feelings are not valid or important to others. Frequently presents as excessive compliance, combined with hypersensitivity to feeling trapped. Generally leads to a buildup of anger, manifested in maladaptive symptoms (e.g., passive–aggressive behavior, uncontrolled outbursts of temper, psychosomatic symptoms, withdrawal of affection, “acting out,” substance abuse).
Self-Sacrifice
Excessive focus on voluntarily meeting the needs of others in daily situations at the expense of one’s own gratification. The most common reasons are: to prevent causing pain to others; to avoid guilt from feeling selfish; or to maintain the connection with others perceived as needy. Often results from an acute sensitivity to the pain of others. Sometimes leads to a sense that one’s own needs are not being adequately met and to resentment of those who are taken care of. (Overlaps with concept of codependency.)
Approval-Seeking and Recognition-Seeking
Excessive emphasis on gaining approval, recognition, or attention from other people or on fitting in at the expense of developing a secure and true sense of self. One’s sense of esteem is dependent primarily on the reactions of others rather than on one’s own natural inclinations. Sometimes includes an overemphasis on status, appearance, social acceptance, money, or achievement as means of gaining approval, admiration, or attention (not primarily for power or control). Frequently results in major life decisions that are inauthentic or unsatisfying or in hypersensitivity to rejection.
Negativity and Pessimism
A pervasive, lifelong focus on the negative aspects of life (pain, death, loss, disappointment, conflict, guilt, resentment, unsolved problems, potential mistakes, betrayal, things that could go wrong, etc.) while minimizing or neglecting the positive or optimistic aspects. Usually includes an exaggerated expectation — in a wide range of work, financial, or interpersonal situations — that things will eventually go seriously wrong or that aspects of one’s life that seem to be going well will ultimately fall apart. Usually involves an inordinate fear of making mistakes that might lead to financial collapse, loss, humiliation, or being trapped in a bad situation. Because they exaggerate potential negative outcomes, these individuals are frequently characterized by chronic worry, vigilance, complaining, or indecision.
Emotional Inhibition (“Emotional Constriction” and “Fear of Losing Control”)
The excessive inhibition of spontaneous action, feeling, or communication, usually to avoid disapproval by others, feelings of shame, or losing control of one’s impulses. The most common areas of inhibition involve:
Inhibition of anger and aggression
Inhibition of positive impulses (e.g., joy, affection, sexual excitement, play)
Difficulty expressing vulnerability or communicating freely about one’s feelings, needs, and so forth
Excessive emphasis on rationality while disregarding emotions.
“Emotional Constriction” and “Fear of Losing Control” as two different schemata can be explained as an over-control to shame or embarrassment to show emotions and as an anxiety to not being able to control or contain the emotions or consequences and/or impulses following the emotions.
Unrelenting Standards and Hypercriticalness
The underlying belief that one must strive to meet very high internalized standards of behavior and performance, usually to avoid criticism. Typically results in feelings of pressure or difficulty slowing down and in hypercriticalness toward oneself and others. Must involve significant impairment in pleasure, relaxation, health, self-esteem, sense of accomplishment, or satisfying relationships.
Unrelenting standards typically present as
Perfectionism, inordinate attention to detail, or an underestimate of how good one’s own performance is relative to the norm
Rigid rules and “shoulds” in many areas of life, including unrealistically high moral, ethical, cultural, or religious precepts
Preoccupation with time and efficiency, the need to accomplish more.
Punitiveness (“Punitiveness to Others” and “Punitiveness to Self”)
The belief that people should be harshly punished for making mistakes. Involves the tendency to be angry, intolerant, punitive, and impatient with those people (including oneself) who do not meet one’s expectations or standards. Usually includes difficulty forgiving mistakes in oneself or others because of a reluctance to consider extenuating circumstances, allow for human imperfection, or empathize with feelings.
#actually autistic#aspergers#aspergers syndrome#autism#autism spectrum disorder#autistic#autistic adult#autistic community#autistic spectrum#being autistic#early maladaptive schemas#schema therapy
18 notes
·
View notes
Text

17 notes
·
View notes
Text
Overcoming Early Maladaptive Schemas Through Stoicism
xr:d:DAGCFTzNeaw:2,j:2585490690809663052,t:24041105 Attachment theory has recently gained significant attention, shedding light on how our early relationships shape our interactions and emotional bonds. Similarly, Early Maladaptive schemes (EMS), a concept that may be unfamiliar to many, offer profound insights into our psychological makeup. EMS are not just abstract ideas; they are deeply…
View On WordPress
#Acceptance#Blogging#Cognitive Behavioral Therapy#Coping Mechanisms#Coping Strategies#Early Maladaptive Schemas#Emotional Control#Emotional Well-being#EMS#gratitude#Jeffrey Young#mental health#Mindfulness#Personal Growth#philosophy#Psychology#Relationships#Resilience#Schema Therapy#self-awareness#Self-Improvement#Stoic Practices#Stoicism#Therapy#virtue
2 notes
·
View notes
Text
This can change with the right type of therapy and the right therapist. Something that focuses on healing interpersonal and complex trauma. One of these:
- Internal Family Systems therapy (IFS)
- Eye Movement Desensitization and Reprocessing (EMDR)
- Deep Brain Reorienting (DBR)
- Schema-Focused Cognitive Therapy with a healthy dose of imagery rescripting
Don't try to heal this with Cognitive Behavioural Therapy or Acceptance Commitment Therapy unless you like being gaslighted.
when you grew up as a lonely uncool girl it will never stop haunting you by the way. you will meet a cool person at a bar or the train station or at a friend's party and you can wear your most stylish outfit and striking eye makeup and you will swear that they can see through all of the facade and see the lonely terribly insecure teenage girl you used to be who desperately wanted to connect and you will swear that they know that there is like an insurmountable gap between you. this will happen forever
107K notes
·
View notes
Text
Schema therapy for borderline personality disorder: A qualitative study of patients’ perceptions
Open Access Peer-reviewed Research Article Yeow May Tan , Christopher W. Lee , Lynn E. Averbeck , Odette Brand-de Wilde , Joan Farrell , Eva Fassbinder , Gitta A. Jacob , Desiree Martius , Sophie Wastiaux , Gerhard Zarbock , Arnoud Arntz Published: November 21, 2018 https://doi.org/10.1371/journal.pone.0206039 Abstract Schema therapy (ST) has been found to be effective in the treatment of…
0 notes
Text
After a weekend heavy with emotions, I stepped out onto my balcony this evening to admire the enchanting beauty of the full moon. She’s always captivatingly beautiful. I cherish her in all her phases. Much like the moon, I too go through my own phases, and through my love for her, I’ve discovered a deeper love and understanding for myself amidst these changes.
As I gazed at the night sky, I envisioned various versions of myself standing beside me. I cradled my toddler self in my arms, while my childhood self stood to my left and my 16-year-old self to my right. Slightly behind me stood a version of myself from my early twenties. Together, we stood there, bathing in the moonlight, embracing each other, in a moment both comforting and emotionally charged. It felt as though all versions of myself were offering solace, much like I comfort and reassure them in my thoughts, a coping mechanism I learned through schema therapy. It was truly a magical moment.
Besides the fact that it’s a full moon, eclipse season has also commenced. It’s an interesting time astrologically, and I find myself immensely curious about what lies ahead. Emotionally, I’m navigating through a challenging period, yet I hold faith that the paths in this phase of my life will be illuminated, guiding me towards the right direction on this journey of life. I trust that what is meant for me will find its way to me, while what isn’t meant for me will fade into the vastness of the universe’s light.
Aligned with the full moon’s grace, happy full moon! ✨🌕✨
#personal#full moon#night sky#lunar eclipse#moon#self love#self care#breath work#healing#grief#reflection#schema therapy#inner child#emotions#astrology#spirituality#230424#240324#250324#0324
5 notes
·
View notes
Text
Entry #009
Trigger Schema and Flashcard Examples
Today I had the trigger of coming too late, so I created a Trigger Schema (entry #005) for this with some flashcard examples down below.
Trigger Schema
"Coming too late"
Situation
I overslept, because I was so tired from working a double shift yesterday. My partner was at his parents house for repairs on the car so he called me 10 minutes before I had to catch the bus to see why I hadn’t texted him yet.
Emotion
Happiness: 0/100; Sadness: 20/100; Fear / Anxiety: 80/100; Angriness: 60/100; Shame: 75/100; Disgust: 40/100
Feelings
Sensory System
Vestibular: overstimulated by having to rush, which makes me feel unstable on my feet
Proprioceptive: overstimulated by having tension in muscles and having tendon pains in my hips and legs
Interoceptive: nauseous, tired, stomach ache, heart rate increase, itchy eyes, toilet urge, throat ache
Auditory: understimulated by quietness in the house, which gives me a ringing sound in my ears (tinnitus) and makes me hypersensitive for the littlest of noises
Visual: understimulated, which gives me object permanence blindness and makes me trip over my cat
Tactile: overstimulated by dry skin
Olfactory: overstimulated by congestion
Gustatory: overstimulated by taking medication and forgetting to brush teeth
Thoughts
Shit, I’m not going to make it in time. I’m forgetting everything. I can’t take the time to do my things I need to do. I totally messed up. I'm so tired. Why am I so tired? I’m not able to function today. Everybody is going to be so angry and disappointed with me. I'm letting everybody down.
Behaviour
I immediately panicked and haste everything I think of that is necessary to do. I feed my cat and pack my back. I get on the bus just in time.
Effect – Outcome
I sit in the bus and train anxious about all the things I might have forgotten to do and didn’t do. I am extremely self-conscious and have the feeling everyone can see how much I failed this morning and that I forgot crucial things.
Early Maladaptive Schema
Defectiveness and shame. Dependence and incompetence. Failure. Negativity and pessimism. Unrelenting standards and hypercriticalness. Punitiveness.
Modi
Vulnerable mode. Angry mode. Demanding mode. Punitive mode. Guilt-inducing mode. Worrying overcontroller mode. Surrenderer mode. Avoidant protecter mode.
Healthy View
My parents were very punitive and unforgiving about oversleeping and making mistakes because of it, it is therefore understandable where my anxiety comes from. However, everybody oversleeps sometimes and nobody likes to do it. Oversleeping doesn’t make me a lesser person. It’s okay I wasn’t able to do everything I usually do in the mornings, because I still managed to get on the bus on time and I did the most necessary things. I went over my window of tolerance the day before and strained my energy levels, so my body needed it.
External Factors
My partner called 10 minutes beforehand, which helped me to get on the bus on time, but didn’t leave me much time to prepare.
Overreaction
I don’t have to be so punitive to myself, because in the end I managed to make it. So even the doom thinking wasn’t entirely justified. I don’t want to be worrying the entire trip that I might’ve done something wrong or forgot something crucial.
Involved schema to overreaction
Punitiveness
Wanted behaviour / reaction
I want to be able to calm down and not keep on worrying after I managed to get on the bus. I don’t want to forget everything in the moment I’m hastening.
Helpful thoughts
Everybody oversleeps sometimes. Oversleeping doesn’t make me a lesser person. It’s okay I won’t be able to do everything I usually do in the mornings. It will turn out alright. I don’t have to be afraid.
Helpful behaviour
Doing relaxation breathing exercises. Taking eye drops. Taking a mint to suck on. Putting on music. Following a list of what I need to do in the morning to get ready. Putting on moisturising cream. Taking my nose salts. Drinking water. Saying affirmations.
Flashcards
After creating a trigger schema I create one or more flashcards, depending on the situation and what I need. I will try to give you some examples of the flashcard structures (entry #008) based on this trigger schema.
Schema Flashcards
Right now I feel anxious, because I overslept and had to haste.
However, I know that this is my punitiveness schema. Which I learned through my youth, because my parents were very punitive and unforgiving about oversleeping, coming too late and making mistakes in general. This lead me to exaggerate the degree to which I'm worrying I did something wrong.
So, even though I believe that because I overslept I can't make it right, I did everything wrong to a degree it's unfixable and it makes me a bad person. The reality is that everybody oversleeps sometimes and it doesn't make a lesser person. This is supported by the way other people reacted in the past to when I overslept and I wasn’t able to follow through with my routine in the morning.
Therefore, even though I feel like I can’t stop worrying and ruminating about what I did wrong and what I didn't do. Instead I could do relaxation breathing exercises, ask for help or support, take a mint to suck on, put on music, use essential oils, follow a list of what I need to do to get ready, put on moisturising hand cream, or say affirmations.
Mode flashcard
Right now I am in worrying overcontroller mode, which makes me feel anxious.
However, this worrying overcontroller mode, which I learned through my youth, because my parents were very punitive and unforgiving about oversleeping, coming too late and making mistakes in general. Got triggered by oversleeping and having to haste and leads me to exaggerate the degree to which I'm worrying I did something wrong.
So, even though I believe that because I overslept I can't make it right, I did everything wrong to a degree it's unfixable and it makes me a bad person. The reality is that everybody oversleeps sometimes and it doesn't make a lesser person. This is supported by the way other people reacted in the past to when I overslept and I wasn’t able to follow through with my routine in the morning.
Therefore, even though I feel like I can’t stop worrying and ruminating about what I did wrong and what I didn't do. Instead I could do relaxation breathing exercises, ask for help or support, take a mint to suck on, put on music, use essential oils, follow a list of what I need to do to get ready, put on moisturising hand cream, or say affirmations.
Trigger flashcard
Right now I got triggered by oversleeping and having to haste, which makes me feel anxious.
It’s okay I got triggered by oversleeping and having to haste and that it makes me feel anxious. Because my vestibular system, proprioceptive system and interoceptive system gets overstimulated and my visual system gets understimulated by the situation.
To help me feel relaxed, I could do relaxation breathing exercises, take a mint to suck on, put on music, use essential oils, follow a list of what I need to do to get ready, put on moisturising hand cream, or say affirmations. This has supported me in the past to feel more at ease and comfortable.
#actually autistic#aspergers#aspergers syndrome#autism#autism spectrum disorder#autistic#autistic adult#autistic community#autistic spectrum#being autistic#autistic things#autistic experiences#autistic stimming#high functioning autism#high masking autism#unmasking autism#schema modes#early maladaptive schemas#schema therapy
11 notes
·
View notes
Text
One thing about getting a Clinical Psychology degree is that some lectures will genuinely change your brain chemistry and make you look like this

"Did anyone take notes?"
"Sorry I was busy bawling my eyes out"
#been thinking about schema therapy for three days now#im so normal about it#hannibal#hannigram#hannibal lecter#will graham#hannibal nbc
123 notes
·
View notes