#Weight Loss Surgery Complications
Text

Gastric Sleeve Revision in USA
Introduction: Considering gastric sleeve revision in the USA? Look no further than Beliteweight Hospital, a renowned medical facility committed to helping individuals achieve their weight loss goals through safe and effective procedures. In this comprehensive guide, we'll explore the benefits of gastric sleeve revision and why Beliteweight Hospital is the ideal choice for your journey towards a healthier and happier life.
Why Choose Gastric Sleeve Revision? Gastric sleeve revision surgery becomes necessary in certain cases where individuals experience complications or inadequate weight loss following their initial gastric sleeve procedure. Whether you're dealing with issues like weight regain, stretching of the stomach, or other concerns, revision surgery can provide a solution to help you get back on track.
Benefits of Gastric Sleeve Revision at Beliteweight Hospital:
Expertise and Experience: Beliteweight Hospital boasts a team of experienced surgeons specializing in weight loss procedures, ensuring that you receive top-notch care from professionals who understand the complexities of gastric sleeve revision.
State-of-the-Art Facilities: Our hospital is equipped with state-of-the-art facilities, providing a comfortable and safe environment for your revision surgery. We prioritize patient safety and well-being throughout the entire process.
Customized Treatment Plans: At Beliteweight Hospital, we understand that each patient is unique. Our expert medical team will work with you to create a personalized treatment plan tailored to your specific needs, ensuring the best possible outcomes.
Comprehensive Aftercare: Post-surgery, our dedicated medical staff will provide comprehensive aftercare support to ensure a smooth recovery. We are committed to guiding you through every step of the process, from surgery to rehabilitation.
Proven Success: Beliteweight Hospital has a track record of success in helping individuals achieve their weight loss goals through gastric sleeve revision. Our satisfied patients stand as a testament to the effectiveness of our procedures and the quality of care we provide.
Conclusion: If you're considering gastric sleeve revision in the USA, choose Beliteweight Hospital for a transformative experience. Our commitment to excellence, experienced medical team, and state-of-the-art facilities make us the ideal partner on your journey to lasting weight loss success. Take the first step towards a healthier you by scheduling a consultation with our expert team at Beliteweight Hospital today.
#Best Gastric Sleeve Revision in USA#Gastric Sleeve Revision in USA#Gastric Sleeve Revision in California#Gastric Sleeve#Gastric Sleeve Revision#Weight Loss Surgery#Bariatric Surgery#Sleeve Gastrectomy#Revision Surgery#Gastric Sleeve Complications#Bariatric Revision Options#USA Bariatric Clinics#Obesity Treatment#Surgical Weight Loss#Sleeve Revision Specialists#Gastric Sleeve Redo#Weight Loss Surgery Complications#Bariatric Procedure Revision#Revisional Bariatric Surgery#Sleeve Gastrectomy Revision#USA Bariatric Centers#Weight Loss Surgery Aftercare#Bariatric Surgeons in the USA
1 note
·
View note
Text
Managing Obesity: Tips for a Healthier Lifestyle
Obesity is a major health problem affecting millions of people worldwide. This is a condition in which excess body fat builds up in the body, leading to a variety of health problems such as diabetes, heart disease, and certain types of cancer. It can be treated with medical intervention. This blog post will go into detail about different ways to treat obesity.
Diet
One of the most important factors in managing obesity is diet. A healthy and balanced diet is essential for maintaining a healthy weight. It is important to eat a variety of nutrient-dense foods such as fruits, vegetables, whole grains, lean proteins, and healthy fats. Avoid processed foods, sugary drinks, and foods high in saturated and trans fats.
Exercise
Physical activity is also important in managing obesity. Exercise helps burn calories, improve muscle mass, and boost metabolism. It is recommended to aim for at least 150 minutes of moderate-intensity exercise per week. This can be achieved through activities such as brisk walking, cycling, swimming, or strength training.
Behavioral changes
Making behavioral changes can also help manage obesity. This includes setting realistic goals, monitoring progress, and staying motivated. It is important to identify triggers for overeating and develop strategies to overcome them. Seeking support from friends and family, joining a support group, or consulting with a healthcare professional can also be helpful.
Medications
In some cases, medications may be prescribed to manage obesity. These medications work by reducing appetite, blocking the absorption of fat, or increasing feelings of fullness. However, medications should always be used in combination with diet and exercise.
Surgery
For those with severe obesity, surgery may be an option. Bariatric surgery is a type of surgery that can help reduce weight and improve overall health. This surgery involves reducing the size of the stomach or bypassing a portion of the small intestine to limit the amount of food that can be consumed.
Summary
obesity is a serious health condition that can be managed with the right lifestyle changes and medical interventions. A healthy diet, regular exercise, behavioral changes, and medical treatments can all help manage obesity and improve overall health. It is important to seek support from healthcare professionals and loved ones to ensure long-term success in managing obesity.
For More information Visit: www.hormoneclinic.in
#obesity#management#diet#exercise#behavioral changes#medication#surgery#health#Weight loss#Healthy lifestyle#Nutrition#Fitness#Obesity prevention#Body mass index (BMI)#Health complications#Metabolic disorders#Mental health#Self-care#Healthcare professionals#Support groups#Public health#Chronic disease management#Personalized medicine
4 notes
·
View notes
Text
I do have to impress on anyone who wasn't around for it how batshit the reality boom of the 2000s could be. Especially on Fox.
Here are some 100% real 2000s reality shows:
Who's Your Daddy? A woman has to guess which of eight men is her biological father. One of them really is, and if she guesses right she wins $100,000. If one of the seven fake dads convinces her to guess them, he wins $100,000.
Black. White. A white family learns about racism by living a month in blackface, while a black family spends a month in whiteface. The black family was a real family, but the white family was just some actors hired to put on blackface to prove racism exists
Without Prejudice? Five strangers decide which of five strangers gets a cash prize based off clips and their answers to political questions. Cancelled when one of the choosers openly said he'd eliminate all black contestants
Welcome to the Neighborhood. Three conservative white families in a Austin subdivision decide which diverse family gets to move in. Unaired due to being literal housing discrimination
Seriously, Dude, I'm Gay. Two straight men try to pass themselves off as gay and whoever seems more gay gets $50,000. Unaired due to. Due to. Due to
Playing It Straight. A woman tries to find love among fourteen men, half of whom are straight and half of whom are gay, and she must eliminate two men she believes are gay each week. If she ended up picking a straight man in the end, they'd split a million dollars; if she picked a gay man, he'd win a million dollars
Boy Meets Boy. This was Playing It Straight but starring a gay man and he had to eliminate straight people
Who Wants to Marry a Multimillionaire? He wasn't a multimillionaire. He didn't even have a million dollars in liquid assets. He had a battery conviction Fox claims they didn't see. Because it was the 2000s, somehow this ended up with the woman he won being widely vilified and turned into a national punchline. How dare she complain about a massive corporation tricking her into marrying a lying abuser, good thing Matt Lauer's there to take her down a peg
The Swan. A "ugly" woman is given plastic surgery and wins a prize if she's the hottest at the end of the season. If she's not hot enough by the show's standards she's eliminated and called ugly on national TV
The Biggest Loser. Overweight people engage in competitive crash weight loss that often led to awful health complications. Studies showed basically everyone on the show regained any weight they lost once it was over and they didn't have abusive trainers demanding they take huge health risks to win a competitive weight loss competition. Like the others, this one was cancel-oh, it was a massive hit that ran for 18 seasons? Yikes!
Wife Swap and Trading Spouses. These were the same show and had a wife from one family go to another family that was different politically, racially, culturally, religiously etc. Most famous for the God Warrior
At the time people focused on the likes of Fear Factor but looking back it's wild how many of the worst shows toyed with politics. So many of these shows have a premise that's like "what if we exposed these conservatives to these people they hate?" or hyping themselves up as Important Experiments. Then they'd freak out when they got the kind of viral bigoted freakout they were trying to construct the whole time.
There were also a bunch of horrible reality shows, thankfully this time mostly unpopular, in the 2010s that based themselves around economic themes as a response to the market crash, but that's a story for another time
27K notes
·
View notes
Note
I saw a comment on your blog that says 'the way you eat does not cause diabetes'...are you able to expand on that or provide a source I could read? I've been told by doctors that my pre-diabetes was due to weight gain because I get more hungry on my anti psychotics and I'd like to fact check what they've told me! Thank you so much!
Pre-diabetes was rejected as a diagnosis by the World Health Organization (although it is used by the US and UK) - the correct term for the condition is impaired glucose tolerance. Approximately 2% of people with "pre-diabetes" go on to develop diabetes per year. You heard that right - TWO PERCENT. Most diabetics actually skip the pre-diabetic phase.
There are currently no treatments for pre-diabetes besides intentional weight loss. (Hmm, that's convenient, right?) There has yet to be evidence that losing weight prevents progression from pre-diabetes to T2DM beyond a year. Interestingly, drug companies are trying to persuade the medical world to start treating patients earlier and earlier. They are using the term “pre-diabetes” to sell their drugs (including Wegovy, a weight-loss drug). Surgeons are using it to sell weight loss surgery. Everyone’s a winner, right? Not patients. Especially fat patients.
Check out these articles:
Prediabetes: The epidemic that never was, and shouldn’t be
The war on ‘prediabetes' could be a boon for pharma—but is it good medicine?
Also - I love what Dr. Asher Larmie @fatdoctorUK has to say about T2DM and insulin resistance, so here's one of their threads I pulled from Twitter:
1️⃣ You can't prevent insulin resistance. It's coded in your DNA. It may be impacted by your environment. Studies have shown it has nothing to do with your BMI.
2️⃣ The term "pre-diabetes" is a PR stunt. The correct term is impaired glucose tolerance (or impaired fasting glucose) which is sometimes referred to as intermittent hyperglycemia. It does not predict T2DM. It is best ignored and tested for every 3-5yrs.
3️⃣ there is no evidence that losing weight prevents diabetes. That's because you can't reverse insulin resistance. You can possibly postpone it by 2yrs? Furthermore there is evidence that those who are fat at the time of diagnosis fair much better than those who are thin.
4️⃣ Weight loss does not reverse diabetes in the VAST majority of people. Those that do reverse it are usually thinner with recent onset T2DM and a low A1c. Only a tiny minority can sustain that over 2yrs. Weight loss does not improve A1c levels beyond 2 yrs either.
5️⃣ Weight loss in T2DM does not improve macrovascular or microvascular health outcomes beyond 2 years. In fact, weight loss in diabetics is associated with increased mortality and morbidity (although it is not clear why). Weight cycling is known to impacts A1c levels.
6️⃣ Weight GAIN does NOT increase the risk of cardiovascular OR all causes mortality in diabetics. In fact, one might even go so far as to say that it's better to be fat and diabetic than to be thin and diabetic.
Dr. Larmie cites 18 peer reviewed journal articles (most from the last decade) that are included in their webinar on the subject, linked below.
#diabetes#t2dm#type 2 diabetes#prediabetes#weight science#weight stigma#fat liberation#fat acceptance#inbox
30K notes
·
View notes
Text
- ED trigger warning -
Being skinny ruined my life. If you’re thin and think to yourself, “why don’t fat people just lose weight?” Please read this
I was the “ideal fat” in the sense that I did everything skinny people wanted me to do. I tried every diet in the book. I exercised regularly. I worked with doctors and dietitians to figure out the best way to lose weight. But nothing worked. I did everything “right” to lose weight, and my weight stayed the same
But the thin people in my life kept telling me that I wouldn’t be happy, attractive, healthy, etc. until I lost weight. So, heartbroken, I came to the conclusion that anorexia was the only option left. It felt safer than bariatric surgery, and was obviously much more affordable
I became the perfect anorexic. 700 cal a day or less, except once a week I allowed myself 1400 cal. For reference, my body required at least 2800 to maintain weight, and at least 1800 to keep my organs and stuff fully functioning. Still, 700 a day, I persisted because everyone in my life told me weight loss was all that mattered. If dieting didn’t work, anorexia had to
And it did. My weight dropped all the way down to 110 pounds. I was skinny - underweight, even - in all sense of the word. The people in my life saw it as a miracle. The ultimate success story. My mother, my “friends,” my doctors, they all congratulated me on my accomplishment
When I confessed my eating disorder to my doctor, he told me, “that’s not the best way to go about it, but I’m glad you lost the weight.” My mother took pictures of me and sent them to relatives to brag
Okay, great. I was skinny. I did what I set out to do. But there were severe consequences
The most obvious was my joint pain doubled, maybe even tripled, to the point that I couldn’t leave the house without a wheelchair
I also developed several health complications, including fatty liver disease and extremely painful GERD. I had to see a handful of specialists and get an endoscopy because of severe stomach pain
My partner, who was the only person who saw my weight loss for what it was (a horrible thing that only happened because of an eating disorder), convinced me to enter a recovery program
For nearly a year, I relearned how to feed myself. I ate everything I was told to eat, nothing more and nothing less. My diet was 100% in the hands of somebody else
And I gained back every pound I has lost. All of the work to become thin went right out the window. It was proven to me that thinness and health were incompatible with my body. If I wanted to be thin, I had to forgo my physical and mental well-being. And vise-versa
Prior to the anorexia, I never once struggled with binge eating. I was naturally an intuitive eater, and I did a good job of having a well rounded diet. After the anorexia, after recovery, I developed a binge eating disorder. I had spent so long starving myself, that my brain and body got stuck in survival mode, desperate to consume any and all calories out of fear that I might starve again. To this day I struggle with binge eating
I did everything thin people wanted of me. I dieted. I exercised. And when all else failed, I starved myself. Now I have liver disease, stomach issues, and BED. Not to mention the loads of mental issues that accumulated as a result of my weight loss journey. During the throes of my anorexia, I had to be hospitalized for suicidal ideation
When you tell fat people to “just lose weight” you are suggesting they give themselves illnesses for which treatments are not always effective. You are asking fat people to destroy their stomachs and livers. When a fat person loses so much weight that they become skinny, they are likely giving up so much of their health in efforts to be treated like a human being
If you’re thin, do your part. Treat fat people like people before we tear our bodies apart
6K notes
·
View notes
Text
LAP Bands should be illegal
This post is going to deal with medical fatphobia, weight loss surgery, coercion, emetophobia, food issues, disordered eating, and just all around bad shit. But it’s important.
Shortly after I reached adulthood, I was coerced into weight loss surgery. I weighed about 250 pounds and was considered morbidly obese.
The Lap Band is a disgrace to the medical profession and is just another example of how the medical profession does not care about the lives of fat people.
To preface this: the surgery works. I lost 70 pounds and people treated me differently and I hated them all for it.
The Lap Band made my life miserable. When it was filled, I could not eat until noon without getting stuck. Even then, getting stuck was always a risk. There was a strict diet to follow and you were supposed to be safe from that if you followed it. On top of that, there were rules for how you ate. One standard I saw was not to eat in bites larger than your fingernail. Can you see yourself doing that for a week, let alone years and years?
Getting stuck is a horror you can't imagine. The food lodges in the top of your stomach, blocking off your system. You continue to produce saliva and swallow it down. Slowly, the mucous in your saliva builds up. It feels like you're drowning. Eventually, you have to essentially throw it all up. A disgusting experience (and a mortifying one if you're in public.) The saliva is thick and ropy. This experience is often called "sliming" on the forums.
I became frightened of eating in public. In a way, I became frightened of food altogether. I knew something had to give the day I reacted to someone biting a hamburger in a tv show the way a regular person would react to a killer jumping out in a horror movie. I developed the disgusting and unhealthy habit of chewing and spitting out food. I completely lost my enjoyment of many foods I had previously enjoyed because of how problematic they were (I can no longer enjoy a chicken thigh for example.) I stopped eating meals and began grazing. I developed eating habits worse than the ones that "made me fat"
After 3 years, I had the band emptied of fluid, which significantly decreased, but did not stop, these problems. I regained the weight, and found it didn't bother me. (Along the way I discovered that my discomfort with my body had never been weight related)
I had my band removed after 6.5 years earlier this year. I am in a support group on facebook for victims of this malpractice. There are 5.6 thousand members, each with their own horror stories. Some of them cannot get the band removed because insurance will not cover the procedure, though they happily covered the band's placement. Some have tried to go through with removal but have had surgeons try to coerce them into getting a different weight-loss surgery instead of just removing it. Many have long-term damage from the band eroding the walls of their stomach or esophagus, or from the band adhering to multiple organs. Many of them had the band for 12-14 years, before removal because none of our doctors told us it needs to be removed within 10.
Many practices no longer perform Lap Band surgery and now believe it is unethical. The surgeon who removed my band still performs this surgery regularly.
A study performed in 2011 with 151 lap band patients, found that 22% of patients experienced minor complications and 39% experienced major complications. The person who coerced me into surgery actually experienced major complications and needed an emergency removal.
I experienced no serious complications. Everything I described above is considered normal. And It still drastically lowered my quality of life.
I don't know why I'm sharing this or who I'm sharing it for, but here I am. If you know anyone considering the lap band surgery, don't let them go through with it without knowing the truth. And please be kinder to your body than the medical profession wants you to be.
3K notes
·
View notes
Note
Going off that post about nutrition and science, I'd love to hear what you think of the 5:2 diet/The Fast 800 and its creator, Dr. Michael Mosley. For context: in order to get an NHS-funded breast reduction (it's a gender thing, but also just a general quality-of-life thing), I need to be a certain BMI, so I've been referred to a weight management clinic. The lady I've been seeing initially just put me on a low-carb diet (130g or less of carbs per day, with an aside from her about how bullshit Keto and BMI limits for treatment are), but now she's said that, if I wanted to speed up the weight loss, I should include the 5:2 diet: 5 days in a week where I eat "normally", and 2 fast days in which I restrict myself to 800kcals.
I did a little looking into it myself, and found that 5:2 - which I HAD heard about before - is now being sold as part of "The Fast 800", with Dr. Mosley being the creator of it. I was shocked by that, because I was already a fan of Dr. Mosley's work (he has a podcast called "Just One Thing" that I really liked, and thought contained reasonable-sounding advice), and yet having a diet plan that he's clearly making money off of does immediately make me feel suspicious.
I've borrowed his "The Fast 800" book from the library, both to find out more about the diet I've been put on and to see if it's at all backed by evidence, and he does cite a bunch of scientific studies which seem to back up his ideas, but I don't know how valid they are, and I don't just want to accept them at face-value (especially since he's a "we got fat completely wrong in the 80s, therefore we should eat a Mediterranean diet!" types).
Obviously I'll go with what my weight management lady suggests, since she's obviously more qualified to talk about it than I am, but I am curious to know what you think, and whether I'm right to be distrustful of all of this.
I am, generally speaking, against any diet for rapid weight loss. They're not sustainable so people gain the weight back (often with more weight getting added on).
There have also recently been findings that suggest that BMI cutoffs for top surgery are detrimental to patients as patients in higher BMI categories are more likely to have minor complications like UTIs or to be readmitted, but are not likely to have major complications or be at risk of significant harm from having top surgery. I don't know if anybody will listen if you bring up that study, and I know that GCS is fraught in many places for many reasons.
I'm also just.
I'm so mad. I'm so fucking mad! I'm so mad about this!
One of my best friends is a guy who was pressured into a pattern of disordered eating and unhealthy exercise in order to qualify for top surgery; since then he has not been able to eat in a healthy way and has struggled with alternating between exercising to the point of harm and other destructive behaviors that make him unhappy and unsafe. And he didn't need that. He didn't need any of that! He needed a very safe surgery that had perhaps a slightly higher risk of minor complications at his size and instead he got top surgery and an eating disorder! I hate it! I'm so fucking mad about it!
Also as near as I can tell Michael Mosley qualified as a psychiatrist in the 90s, spent very little time working as a psychiatrist, and then became a media personality. From what is visible on his website and every biography I've found for him he apparently doesn't have any background in nutrition beyond whatever is standard for someone in medical school (which is NOT MUCH).
Hey I just looked at his website and this is straight-up fucked up.
Anybody recommending an 800 calorie a day diet for 2-12 weeks in a context that is not heavily medically supervised can fucking choke. That is *ridiculously* dangerous and the website says that this can improve insulin resistance but there are a shitload of studies about people on crash diets like this *developing* insulin resistance (oh hey like my friend who became prediabetic after his rapid significant weight loss).
Also in regard to the studies he cites on the website, the "two years later patients are still going strong in their diabetes improvements" it's really important to put shit like that in context

at 5 years 13% of the original intervention group were in remission from their type two diabetes; the average weight loss experienced by the intervention group as a whole was 6.1kg compared to 4.6kg in the control group. That's 1.5kg lower for the people who went through a twelve week medically supervised very low calorie diet compared. That's an average difference of 3.3 pounds between "starvation diet" and "no diet" for the Americans in the audience.
Yours is the second comment I've seen that has been leery of the Mediterranean diet, btw, and the Mediterranean diet is fine. It's very achievable and not super gimmicky and is based on very reasonable reassessments of fat, not the hardcore "you are fine to eat 100g of fat a day" kind of attitude that you get from the keto crew. There isn't really one Mediterranean diet and it certainly isn't low carb (which the bits from Mosely's website seem to indicate it is).
So, no, honestly I don't think much of Mosely and I'm very sorry you're in this situation, that sucks and I hate that they're refusing you treatment until you undergo an exceptionally difficult and potentially harmful weight loss excursion.
I know you're probably stuck with that and it's bullshit and I think it fucking sucks and unfortunately the medical advice you're likely to get is "eat in a significantly disordered manner at least until it is time for surgery" and it blows. That just fucking sucks.
If you're looking for rapid weight loss that you don't plan to sustain (and you shouldn't plan to sustain it, it won't stay off) you may want to look into body building forums for how they discuss cuts. It's still disordered eating and it's still not healthy, but at least they're effective and can tell you what supplements will keep you from becoming malnourished while you prepare for surgery. This is a terrible idea. I don't actually want to give this advice to anyone but bodybuilders are the exact kind of people who know how far and how fast they can push weight loss while having an awareness that it isn't really good for them and it won't stay off.
I cannot overstate enough how much I hate the thought that people are being encouraged to rapidly starve themselves in order to prepare to recover from surgery. I am so sorry and I'm so mad and
323 notes
·
View notes
Note
so i have a question, recently my doctor has recommended i lose weight for some health reasons, if i choose to go with that and lose weight willingly, does that make me fatphobic?
I can't tell you what to do with your body. Those decisions are yours. Life is complicated and nuanced, and so is oppression. If a trans person willingly loses weight because that's the only way the bigoted medical system will allow them to have top surgery, does that make them fatphobic?
Ultimately, what matters to me most is ending fat people's systemic oppression. What an individual person decides to do with their body, I don't really have the energy to care about. All of my mental energy is going towards more important matters that I do have a say in, like ending the wage gap that fat people endure and supporting fat positive legislation.
So whether or not the decision you make is fatphobic, you have bodily autonomy. Now if you're doing this because you believe weight equals health, well, "weight equals health" is fatphobic rhetoric. If you decide to lose weight because you want to feel superior to fat people, yeah, I'd say that's probably fatphobic. But my lack of mental energy to dictate what someone should do with their body, plus how nuanced and unique every situation is, makes me want to answer this ask with a shrug ¯\_(  ̄o ̄ )_/¯
You do what you want to do. If someone had a terminal illness and was told they'd magically survive by losing weight, I don't think I could blame them for trying when they're in such a desperate situation. I think the more important question to ask yourself is "Will this actually improve my health? Or will this harm me?"
Some other good questions to ask yourself are:
"How permanent would this weight loss actually be?"
"Is my doctor telling me to lose weight as their only means of treatment for me? Did they even examine me? What quality of healthcare am I receiving?"
"Is it specifically weight loss that helps this condition? Or is it certain behaviors that help and happen to sometimes include weight loss as a side effect?"
"Is weight gain what caused this condition? Is the answer to the previous question scientifically proven, or is it correlation? Is weight gain actually a symptom?"
"What scientific research is my doctor using to justify their recommendation that I focus on weight loss? How long was the study conducted for? Are there conflicts of interest? Does this study contain validity errors?"
I hope these questions will help you with the decision-making process. Good luck
-Mod Worthy
#bodily autonomy#healthism#diet culture#fatphobia#medical fatphobia#Mod Worthy#ask#justaskingquestionstbh
217 notes
·
View notes
Text

Urgent Help Dalia's family Evacuate & Treat her parents
Plz Read Dr dalia Story:
Hello World , it's Dalia.
Please read this as if I'm a member of your family . maybe your sister, daughter or a friend and as if my family who's under death now is yours.
My name is Dalia and this is my story. I am 27 years old, a laboratory doctor, and a graphic and website designer, also a private lessons teacher. Before October 7th, I had a beautiful and peaceful life with my family. I had ambition and many dreams. I was working in Al Shifa Laboratory and had an office for my design work as well as private student groups. But now everything has changed. What happened to us is a nightmare. I lost everything at once, my home and my work in all its aspects. We are repeatedly displaced between danger and death.
I am the older sister and my family is a trust in my neck, and I work hard to ask for help in our survival.
since the beginning of the war, from October 7 until today. We spent the first week of the war in Gaza. During this short period, we were exposed to many bombings and damages, and we were hit by rocket fragments as a result of close-in shelling. After that, On October 13, they asked us to forcefully evacuate the area due to its danger and go to southern Gaza. We went to Al-Shifa Hospital while we were living in a nightmare, extreme danger, and a devastating war. We remained there for a week and were subjected to siege and bombing. We did not have mattresses or pillows for our heads, and we had no drinking water، no Food, and nothing. We were sleeping on the ground between the feet of passers-by and the blood of the wounded. We were suffering from the pollution of the place. This is my picture in Al-Shifa Hospital, sleeping on the floor.
Since the war on Gaza began, it has lost almost everything
In January, I lost 33 members of my family in one second to a single missile that ended their lives. I also lost my only uncle who died due to not receiving treatment and I do not want to lose anyone else.
As for me, I am a laboratory doctor, a graphic and website designer, and also a private lessons teacher. Before October 7th, I was living a beautiful and peaceful life with my family، I had ambition and many dreams. I was working in the Al-Shifa laboratory, which was bombed, and I lost my job there, also I had an office for private design work that was also bombed. What happened to us is a nightmare. I lost everything at once, my home and my work in all its aspects, my dreams and ambitions, and I became without a home, work, and clothes because we did not take anything from our house before it was bombed.
Before the war, my life was about successes and achievements. This picture is one of my design works that was displayed in one of the streets of Norway for a BBQ restaurant. I had a dream to reach the international level with my works and successes, but the occupation killed me and my dreams and everything before I arrived.
My work also designs perfume posters for a Saudi store, and I lost all of my work due to the war.
But my mother suffered the most, who had a hysterectomy 4 days before the war because of a tumor. She was sleeping on the floor and using a contaminated bathroom, which led to infection of the wound, bleeding, health complications, and a loss of 25 kilograms of weight. To this day, we have not been able to know the outcome of the tumor that was inside the uterus, and my mother also suffers from platinum in her spine due to the weakness of her vertebrae. She also suffers from a herniated disc in her neck, which poses a threat to her spine, She needs urgent surgery and is suffering from a lot of pain because she sleeps on the floor instead of a medical bed.
My mother also suffers from rheumatoid arthritis, asthma, and most importantly multiple sclerosis, in addition to being diagnosed with undifferentiated connective tissue disease and heart failure. She suffers from urinary excretion disorders, and needs urgent travel for treatment. Here is the medical report and diagnosis on her condition.
My father also suffers from heart disease, high blood pressure, and diabetes. Two months before the war, he underwent heart surgery due to 99% blockage of the arteries. His heart stopped twice during the operation. He stayed in intensive care for a month, and because of the war, he did not receive treatment for 8 months, which led to a severe deterioration in his health condition, and he suffered a severe heart attack that would have ended his life. He was unable to receive treatment due to the lack of medical equipment. My father took an echocardiogram on the floor without the patient’s bed.
My father also suffered a serious stroke a month ago due to his health condition deteriorating significantly. Please help me save their lives. I don't want to lose my father as I lost my only uncle who died in the war due to illness and not receiving treatment. I spend long hours with my father in his non-existent treatment. There is no medicine, no care, no treatment, no lunch, no meat, no protein. What we eat includes packaged foods, which cause many diseases.
My heart is torn apart in pain. My parents are the most precious things in my life and they are my whole life, I am the eldest daughter of my family and I have all the responsibility on my shoulders. I can no longer bear all this oppression and pain. Please help me, I need you, You are my only hope to save me and my family.
You can donate to DR Dalia and Her Family in GoFundme: click here
#free palestine#save palestine#palestinian genocide#i stand with palestine#all eyes on palestine#palestine#gaza#free gaza#gaza strip#gazaunderattack#gaza genocide#donations#donate#gofundme#gaza donation
45 notes
·
View notes
Text
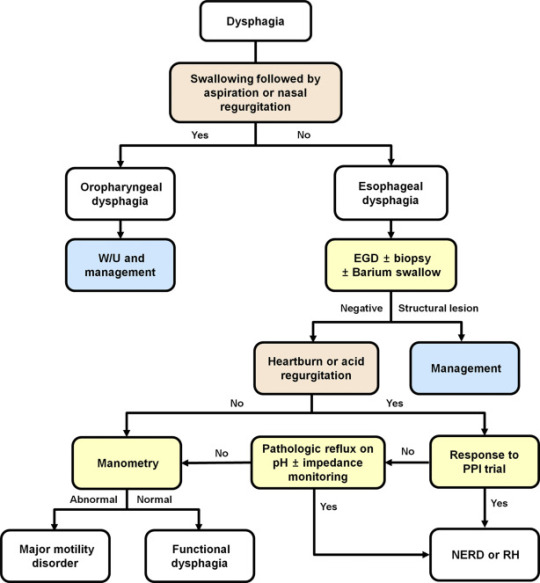
Explaining dysphagia
Dysphagia is simultaneously a symptom and a diagnosable condition. Most people think of it (if they think of it at all) as the choking on food disease but in reality it's much more complicated than that.
There are four categories of dysphagia: oropharyngeal, esophageal, esophagogastric, and paraesophageal
only two of those categories (oropharyngeal and esophageal) are commonly used and diagnosed so those are the main two I'll be talking about.
The diagnosis of dysphagia is a fairly complicated process involving a lot of radiological testing and things stuck up your nose and down your throat.
lost the source :(
source
the ICD 10 further divides dysphagia into unspecified, oral phase, oropharyngeal phase, pharyngeal phase, pharyngoesophageal phase, and other dysphagia which includes cervical dysphagia and neurogenic dysphagia
Oropharyngeal dysphagia
Oropharyngeal dysphagia occurs when someone has difficulty initiating a swallow. It's often accompanied by coughing, choking, feeling food stick in the throat, and nasal regurgitation. Other symptoms include frequent repetitive swallows, frequent throat clearing, a gargly voice after meals, hoarse voice, nasal speech and dysarthria, drooling, and recurrent pneumonia.
Oropharyngeal dysphagia is diagnosed with a modified barium swallow and/or a transnasal video endoscopy.
Some of the consequences of oropharyngeal dysphagia include aspiration pneumonia, upper respiratory infections, and weight loss. Common treatment includes rehabilitative swallowing exercises, botox, surgery, and/or a feeding tube.
Esophageal Dysphagia
Esophageal dysphagia is dysphagia where there is a problem with the passage of food or liquids through the esophagus between the upper and lower esophageal sphincter. Esophageal dysphagia is usually a result of abnormal motility in the esophagus or a physical obstruction to the esophagus. Symptoms of esophageal dysphagia vary depending on cause.
Motility: People with esophageal motility disorders will experience problems with swallowing both liquids and solids. Motility disorders consist of abnormal numbers of contractions in the esophagus, abnormal velocity of contractions, abnormal force of contractions, abnormal coordinated timing of contractions, or several of these simultaneously. People with esophageal motility disorders may also experience spasms or chest pain.
Obstruction: People with an esophageal obstruction will have more difficulty swallowing solids than liquids.
Some symptoms of both include pain when swallowing, the inability to swallow, sensation of food being stuck in your throat or chest, drooling, and regurgitation.
Esophageal dysphagia can be diagnosed with a barium swallow, upper endoscopy, esophageal manometry, and an endoFLIP.
Some common treatments for esophageal dysphagia include medication, esophageal dilation, surgery, stent placement, and/or a feeding tube.
Esophagogastric Dysphagia
Esophagogastric dysphagia occurs when there is a problem with material passing from the lower esophageal sphincter into the gastric fundus.
Paraesophageal Dysphagia
Paraesophageal dysphagia occurs when the esophagus is narrowed due to extrinsic compression.
The ICD 10 Classifications
Oral phase - difficulty moving food or liquid to the back of the throat
Oropharyngeal phase - difficulty initiating swallowing
Pharyngeal phase - difficulty swallowing when food or liquid is at the top of the throat
Pharyngoesophageal phase - unable to find information
Other dysphagia- cervical dysphagia (caused by problems with the cervical spine) or neurogenic dysphagia (caused by problems with the central or peripheral nervous system)
Sources
x x x
+ some others I definitely (/sarcasm) didn't lose the link to
92 notes
·
View notes
Text
Re: a certain post going around, please don’t refer to elective weight loss surgeries as “mutilations”. Yes, they can cause very serious complications; yes, a lot of people are pressured into them due to fatphobia; yes, sometimes people regret them. But these are still procedures that hundreds of thousands of real people have already had. People who are reading your posts. Those people are welcome to call themselves mutilated if they feel that way, but it’s pretty damn rude to call them that yourself. You can speak convincingly about medical bigotry and the inherent risks of elective procedures that alter the function of the digestive system without using the same weird, stigmatizing language about “mutilating healthy organs” that transphobes use. I actually think it detracts from the message.
31 notes
·
View notes
Text
#Best Gastric Sleeve Revision in USA#Gastric Sleeve Revision in USA#Gastric Sleeve Revision in California#Gastric Sleeve#Gastric Sleeve Revision#Weight Loss Surgery#Bariatric Surgery#Sleeve Gastrectomy#Revision Surgery#Gastric Sleeve Complications
0 notes
Text
bariatric surgery is a barbaric surgery. filling you with foreign objects to reduce stomach space, banding your esophagus or fundus such that your body interprets its internal pain signals as fullness. cutting your stomach to a tiny size or evn removing it altogether. it leads to vitamin deficiencies and has a high rate of complications including bile leakage, dumping syndrome, osteopenia, abscesses, pancreatitis, and more. the way people are taught to hate their size so much that they would undergo dangerous surgery, and that the medical industry happily tells people where to sign without telling them the full extent of bodily disfigurement, is tragic. while people may have a valid reason to pursue weight loss, we need to look critically at the way bariatric surgery is marketed and performed and explore more holistic options.
215 notes
·
View notes
Note
I totally understand and can empathize with fat activists when it comes to medical fatphobia. But I do think its important to provide nuance to this topic.
A lot of doctors mention weight loss, particularly for elective surgeries, because it makes the recovery process easier (Particularly with keeping sutures in place) and anesthetic safer.
I feel like its still important to mention those things when advocating for fat folks. Safety is important.
What you're talking about is actually a different topic altogether - the previous ask was not about preparing for surgery, it was about dieting being the only treatment option for anon's chronic pain, which was exacerbating their ed symptoms. Diets have been proven over and over again to be unsustainable (and are the leading predictor of eating disorders). So yeah, I felt that it was an inappropriate prescription informed more by bias than actual data.
(And side note: This study on chronic pain and obesity concluded that weight change was not associated with changes of pain intensity.)
If you want to discuss the risk factor for surgery, sure, I think that's an important thing to know - however, most fat people already know this and are informed by their doctors and surgeons of what the risks are beforehand, so I'm not really concerned about people being uninformed about it.
I'm a fat liberation activist, and what I'm concerned about is bias. I'm concerned that there are so many BMI cutoffs in essential surgeries for fat patients, when weight loss is hardly feasible, that creates a barrier to care that disproportionately affects marginalized people with intersecting identities.
It's also important to know that we have very little data around the outcomes of surgery for fat folks that isn't bariatric weight loss surgery.
A new systematic review by researchers in Sydney, Australia, published in the journal Clinical Obesity, suggests that weight loss diets before elective surgery are ineffective in reducing postoperative complications.
CADTH Health Technology Review Body Mass Index as a Measure of Obesity and Cut-Off for Surgical Eligibility made a similar conclusion:
Most studies either found discrepancies between BMI and other measurements or concluded that there was insufficient evidence to support BMI cut-offs for surgical eligibility. The sources explicitly reporting ethical issues related to the use of BMI as a measure of obesity or cut-off for surgical eligibility described concerns around stigma, bias (particularly for racialized peoples), and the potential to create or exacerbate disparities in health care access.
Nicholas Giori MD, PhD Professor of Orthopedic Surgery at Stanford University, a respected leader in TKA and THA shared his thoughts in Elective Surgery in Adult Patients with Excess Weight: Can Preoperative Dietary Interventions Improve Surgical Outcomes? A Systematic Review:
“Obesity is not reversible for most patients. Outpatient weight reduction programs average only 8% body weight loss [1, 10, 29]. Eight percent of patients denied surgery for high BMI eventually reach the BMI cutoff and have total joint arthroplasty [28]. Without a reliable pathway for weight loss, we shouldn’t categorically withhold an operation that improves pain and function for patients in all BMI classes [3, 14, 16] to avoid a risk that is comparable to other risks we routinely accept.
It is not clear that weight reduction prior to surgery reduces risk. Most studies on this topic involve dramatic weight loss from bariatric surgery and have had mixed results [13, 19, 21, 22, 24, 27]. Moderate non-surgical weight loss has thus-far not been shown to affect risk [12].
Though hard BMI cutoffs are well-intended, currently-used BMI cutoffs nearly have the effect of arbitrarily rationing care without medical justification. This is because BMI does not strongly predict complications. It is troubling that the effects are actually not arbitrary, but disproportionately affect minorities, women and patients in low socioeconomic classes.
I believe that the decision to proceed with surgery should be based on traditional shared-decision making between the patient and surgeon. Different patients and different surgeons have different tolerances to risk and reward. Giving patients and surgeons freedom to determine the balance that is right for them is, in my opinion, the right way to proceed.”
I agree with Dr. Giori on this. And I absolutely do not judge anyone who chooses to lose weight prior to a surgery. It's upsetting that it is the only option right now for things like safe anesthesia. Unfortunately, patients with a history of disordered eating (which is a significant percentage of fat people!) are left out of the conversation. There is certainly risk involved in either option and it sucks. I am always open to nuanced discussion, and the one thing I remain firm in is that weight loss is not the answer long-term. We should be looking for other solutions in treating fat patients and studying how to make surgery safer. A lot of this could be solved with more comprehensive training and new medical developments instead of continuously trying to make fat people less fat.
656 notes
·
View notes
Text
Susan Rinkunas at Jezebel:
Today the Supreme Court held a brutal two hours of arguments in a case about whether women and pregnant people deserve life-saving medical care if that care happens to be abortion. (Yes, this is the second abortion case this term.) Several justices, and the lawyer for the plaintiff, trotted out wild hypotheticals and invoked the dangerous concept of fetal personhood in a disturbing preview of the future that awaits every state if Donald Trump wins the presidency. It could mean that people face horrible medical mistreatment simply because they’re pregnant and, at the most extreme end, could lead to a federal abortion ban.
The case, Moyle v. United States, is about whether state abortion bans like Idaho’s can override a longstanding federal law that requires emergency rooms to stabilize patients, including by offering abortion if necessary. That law, the Emergency Medical Treatment and Active Labor Act (EMTALA) says hospitals that accept Medicare funding have to stabilize patients in medical crises and deliver babies when women are in labor. But given that some states passed abortion bans that only have exceptions to prevent death, not to treat threats to health, the Biden administration reiterated hospitals’ obligations after the Dobbs decision, and later sued the state of Idaho.
Idaho strongly disagrees that its hospitals should have to provide abortions for threats to health—like when a woman’s water breaks in the second trimester, far too early for a baby to survive but, when left untreated, could result in a life-threatening infection called sepsis or extensive blood loss known as hemorrhaging. The state worked with the right-wing Christian legal firm Alliance Defending Freedom to craft its legal arguments and one such argument raised in briefs and in the courtroom is the claim that a fetus is a patient under federal law.
Justice Elena Kagan asked Josh Turner, the lawyer representing Idaho, how the state ban functions when doctors believe a woman’s pregnancy complication might cause her to lose her uterus, and thereby her ability to have children in the future, but not cause her to die. Turner’s response was chilling: “Congress under EMTALA recognizes that there are two patients to consider in those circumstances. And the two-patient scenario is tough when you have these competing interests.” This logic is terrifying, mostly because a fetus is only a patient under EMTALA when there aren’t health threats to the pregnant person. The woman is the patient first and foremost. Idaho is trying to claim that because the words “unborn child” are used in the law, it means that the interests of the woman and the fetus have equal weight, when they do not.
This is fetal personhood and it’s scary not least because the people being denied ER treatment in Idaho and other states are often in their first and second trimester and there’s no way the embryo or fetus will survive. The fetus is a lost cause at that stage, yet states like Idaho say that women themselves need to be facing death before they can have an abortion. (People coming to ERs later in pregnancy with complications would typically have labor induced and then doctors would try to keep the fetus alive.)
[...]
If by some miracle the court rules against Idaho, that doesn’t mean abortion access is safe by any means. Barrett and Gorsuch both asked if a future Congress could ban hospitals from performing any abortions or gender-affirming surgeries as a condition of accepting Medicare funds. Prelogar said yes, Congress does have the power to pass laws like that. And of course, there is the lurking threat of the 19th-century Comstock Act which a Republican president could enforce to ban abortion nationwide, even at clinics in states with abortion protections.
SCOTUS heard oral arguments on a pair of cases pertaining to EMTALA on Wednesday, and the radical right-wing black robed theocrat-majority are likely to rule in favor of Idaho's cruel anti-abortion law to weaken EMTALA.
See Also:
HuffPost: Conservative SCOTUS Almost Entirely Ignores Pregnant Patients In Emergency Abortion Arguments
Vox: The Supreme Court’s likely to make it more dangerous to be pregnant in a red state
#EMTALA#Abortion#Abortion Bans#Moyle v. United States#Idaho v. United States#Fetal Personhood#Idaho#Idaho SB1309#Alliance Defending Freedom#Elizabeth Prelogar#SCOTUS
19 notes
·
View notes
Text
Phallojourney Part 3
Hi everyone! I had my consult with the plastic surgeon, my urologist, and a licensed social worker yesterday. We went over some of the next steps, they took some measurements of my forearm, and talked about what I need to do to prepare.
One of the unfortunate things is that they’re going to have to use my left arm for the skin graft, which means I’ll be losing the tattoos on that arm. They’ll be internal so the phallus won’t be tattooed. They want me to do electrolysis and check back in 3 months to see if the skin is ready. I’ve heard that it’s not comfortable, but about on par with pinching or getting a tattoo.
Another step for me is losing weight. I don’t appear to be very overweight, but because I’m short my BMI is more heavily affected. I’m currently 214 lbs and will be aiming for around 190 lbs before the surgery. I don’t want to take weight loss drugs, so I’m going to be increasing my normal activity and working on eating out less. Depending on your BMI, this may be a requirement for surgery if you go through the same process. People with a higher BMI are more at risk for complications or problems healing, so someone surgeons have restrictions in place.
Another thing I’ll need to do is getting my letters for insurance. I’m currently seeing a psychiatrist, so I’ll be asking her for a letter. The social worker at my appointment will also set up an appointment with me and will write me a second letter. Some insurance companies are more strict about how many letters are needed, so definitely talk with your insurance to see what is required. The surgeon is also asking that I get established with a new therapist since I’m currently not seeing one.
They also gave me some information about what I can expect from the surgery and recovery. The actual procedure will take all day and then I’ll spend around 5-7 days in the hospital. I’m also being advised to take around a month off work, even though I work from home at a computer. If you’re in a more active job, you’ll likely need to take longer. I’ll have 2 catheters alongside drains, so they recommend having someone at home to help you with taking care of it.
Last for this update, we also discussed the additional features of the surgery. I decided that I did not want to do the scrotoplasty and I want the vaginectomy. This means that they will remove any vaginal tissue and sew it closed. They will not be creating a scrotum. I also made the decision that, in terms of appearance, I would prefer a circumcised look. I am also not pursuing an erectile implant, but I will be doing urethral lengthening to be able to urinate through the new phallus. All of these are options that you can choose to customize your new phallus, but are not required. Any additional surgery, such as creating the circumcised appearance, will take place a few months after the creation of the phallus after it has healed enough.
Thank you for joining me on this journey and I’ll see you all with the next update!
9 notes
·
View notes
Last Seen Blogs

haiiiheee
Untitled
cosplayerintraining
cosplayerintraining

lharvey250
BlueStockingReviews

ragedagainst
RAGE AGAINST.

housecaelin
I Await You At The Dread Isle.