#book: psychosis trauma and dissociation
Text
Chapters 1-4 of Psychosis, Trauma, and Dissociation: Historical conceptions of psychotic disorders and schizophrenia
The term 'psychosis' was first used as an alternative to terms like 'insanity' and 'lunacy.' It was coined by the Austrian physician Ernst von Feuchtersleben, taken from the Greek word 'psyche' (meaning mind or soul) and the Latin suffix '-osis' (meaning an abnormal condition). It referred to a sickness where both the body and the soul were sick, or a disease that affected 'the whole person.' The coining of this term was in response to a German psychiatry debate between mental disease located in the 'soul' and disease located in the 'body' - /Psychiker/ and /Somatiker./
Modernly, 'psychosis' is used to mean 'having psychotic symptoms.' However, psychosis is often used related to incomprehensibility. It's not new - Jaspers argued more than a century ago that 'genuine psychotic delusions' are 'not understandable.' Often, terms like "quasi-psychotic" and "psychotic-like" are used when the behavior can be made sense of in some way.
The book then argues that a useful conception of the word psychosis would be one where it means that a) an alteration in the 'hierarchy of reality' has occured, and b) the person as a whole has been changed in a fundamental way.
Thomas Sydenham (1624-1689) used the term 'hysteria' to denote any mental disorder short of 'frank alienation' (outright psychosis), while Thomas Willis (1621-1675) outlined a picture in 1672 of a condition what two centuries later would be called 'dementia praecox' by Emil Kraepelin.
In 1808, the term 'psychiatry' was first used by Johann Reil to refer to the treatment of the mind. Now, larger scale scientific observations could be brought to what used to be isolated accounts of individual observers.
John Haslam (1766-1844) provided cases that would be consistent with what would later be called 'schizophrenia', and his 1810 book /Illustrations of madness/ detailed a single case of insanity. It was of a paranoid psychotic man, James Tilly Matthews, who believed an 'infernal machine' was controlling his life and torturing him. Haslam also recognized that in some people there were states of excitement and depression that alternated - an early recognition of bipolar disorder.
In the mid-nineteenth century, the term 'psychosis' was first proposed by Ernst von Feuchtersleben to replace 'insanity' or 'lunacy.' Ironically though, he considered 'hysteria' to be a neurosis (a term proposed for any disease caused by the functioning of the nerves), and as such it was more 'biological' than psychosis…
Less than a generation later, Wilhelm Griesinger helped the somaticists win the soul versus soma dispute and 'psychosis' became a term for 'organically based mental disorders.' Under Griesinger's influence, psychosis came to mean organic (caused by organic processes) and neurosis came to mean non-organic (by-products of psychological development.)
Karl Ludwig Kahlbaum (1828 - 1899) labelled the disorders hebephrenia (with his student Ewald Hecker), to mean a psychosis of young adoloscents characterized by mental disorientation, and catatonia, a condition where the patient had no reactivity, was mute, and physically immobile.
Emil Kraepelin (1856 - 1926), while he wrote about every major psychiatric disorder, psychosis was a major interest of his. He built upon the ideas of Griesinger and Kahlbaum, observing many patients and outlined a classification of psychosis that is still very evident in the DSM-5.
Kraeplin grouped together disorders that had a poor outcome - 'catatonia', 'hebephrenia', and 'dementia paranoides.' On the sixth edition of his textbook, he outlined 'manic depressive psychosis' (bipolar disorder) and 'dementia praecox' (schizophrenic disorders.' Kraeplin claimed that on top of progressive and inevitable decline, essential features were a discrepany between thought and emotion, negativism, stereotypical behaviors, hallucinations, delusions, and disordered thought. His focus on 'inherent bodily defects' in psychiatric disorders and rapid decline led to a pessimisstic outlook on the treatment of dementia praecox.
Kraepelin also described 'paranoia,' a chronic illness characterized by delusional beliefs, in the absence of personality changes. He believed paranoia was less severe and associated with partial recovery.
The first use of the term 'schizophrenia' was by Eugen Bleuler (1908/1987). Over 10 years, Bleuler developed his ideas on schizophrenia in close cooperation with Carl Jung. Bleuler criticized Kraepelin's idea of dementia praecox, by saying that not all cases began early (praecox) and not all cases ended in full mental deterioration (dementia.) He proposed the term 'schizophrenia' in a Berlin psychiatry conference. The word literally means 'split mind' as he thought that /tearing apart/ ('Zerreissung') and /splitting/ ('Spaltung') were central to the disorder.
Schneider's first-rank symptoms of schizophrenia had a powerful influence on the diagnostic criteria for schizophrenia, from the 1970s onwards. They were considered sufficient but not necessary for a diagnosis of schizophrenia to be made. They were (In German, followed by their english translations): Gedankenlautwerden (audible thoughts), Stimmen in Form von Rede und Gegenrede (voices conversing or arguing), Begleitung des Tuns mit halluzinierten Bemerkungen (voices commenting on one’s behaviour), körperliche Beeinflussung (somatic influences), Gedankenentzug, Gedankeneingebung und ‐beeinflussung(thought insertion, thought withdrawal and thought influences/‘made’ thoughts), echter Wahn als Beziehungssetzung ohne Anlaß (delusional perception).
#graypost#grayrambles#psychosis#schizophrenia#psychiatry#psychology#history#nerdpost#book: psychosis trauma and dissociation
35 notes
·
View notes
Text
"Even though certain events are more likely to be traumatizing, there is considerable variation in how individuals react to these events; if someone successfully deals with an event that others might see as extremely stressful, that event cannot be viewed as traumatizing for that person (Nijenhuis, 2015). Accordingly, one can conceptualize trauma as an individual’s ‘breaking‐point’ when faced with events that are, for him or her, personally overwhelming."
Moskowitz et al. on the definition of trauma, from "Defining Psychosis, Trauma, and Dissociation" in Psychosis, Dissociation, and Trauma: Evolving Perspectives on Severe Psychopathology (pp.17-18)
#trauma#ptsd#trauma informative#academic#psychosis dissociation and trauma: evolving perspectives on severe psychopathology#quotes#books
106 notes
·
View notes
Note
what do you think about systems or alters caused/made by psychosis? As in, someone whose delusion includes them believing they are one or more people
i support those people. it's not like they're doing it on purpose if it's a delusion. they deserve acceptance, resources, and access to help.
if you're asking for my opinions on whether psychosis-made systems are "real systems" or how similar it is to DID, i don’t have a fully formed opinion. i'm guessing that it's probably very different from DID, but how different? i have no idea.
it's actually something my professor and i have been discussing lately—the relationship between dissociation and psychosis, and the history behind them. it's pretty interesting. disorders like DID, PTSD, and schizophrenia were all birthed from the same idea of hysteria. historically there have been attempts to distinguish psychosis from dissociation, but looking back you'll find so many examples of psychosis being talked about way more like dissociation. there's always been tons of confusion and intermixing of these two concepts because people just don't know where the line in the sand is, even though there's clearly a line somewhere.
recently, i was reading a book on schizophrenia from the 60s. there was a lot of debate over schizophrenia back then....mostly debates over its cause. i was pretty surprised to see how often this book described schizophrenia almost exactly in the same way DID is described today. you could've showed me a page out of context and i would've thought the book was about DID! i wonder just how many old books and research on "psychosis" were actually just digging into dissociation, vice versa.
there’s a lot of overlap between schizophrenia and DID & PTSD, especially DID, but there's also a lot of differences between them. i find the professional debate over what to do fascinating. should schizophrenia be given a dissociative subtype? should it be reconceptualized as a trauma-related disorder? should PTSD and DID be given psychosis subtypes?
i really recommend reading this paper if you're interested in learning more.
45 notes
·
View notes
Note
since you typically recommend the EASE and the EAWE as resources, I'd like to also recommend the Perceptual Aberration Scale (PAS; Chapman, Chapman, & Raulin, 1978) and Magical Ideation Scale (MIS; Eckblad & Chapman, 1983) - they may be a tad old, but the book i'm reading (Psychosis, Trauma and Dissociation) mentions that they're widely used in measuring schizotypy and tend to be used in professional studies when assessing for schizotypy in a person! I'm not sure if they can be found online easy or not since I haven't looked yet, but I wanted to put the info out there anyways.
thank you for the info!
36 notes
·
View notes
Text
One thing I dont see talked about enough is dissociative psychosis, it occurs a lot in people w/ DID when they are on the cusp of remembering some major repressed trauma, or when alters are about to surface. These are hallucinations that represent the repressed trauma in some way, and can often be very extreme or horrifying. This is our mind trying to tell us about what happened in any way possible.
It doesnt mean youre insane though, it doesnt mean your trauma isnt valid, it really is a symptom of DID, and youll find a lot of literature mentioning this one. Its in nearly all books about DID.
Yet I see nearly no one in online spaces talk about it, in spite of it being really common.
#did#multiple#dissociative identity disorder#plural#protector alter#protector#plurality#persecutor alter#persecutor
16 notes
·
View notes
Text
Okay so— imma need some advice… ok xx
General mental health TW <<nothing major but pls take care of yourselves
Today I went to my GP. The reason is unrelated but I came out with another booking, next week and this time for all the psychological stuff that’s wrong with me
Btw I’m a minor with some trauma so there’s a lot of parental dependence here
Okay! So!! The main question>> Should I at all be open about my alterhuman identity? Has anyone had any experience with how the medical field handles this sort of thing? Have you been met with any… like, discrimination, shit i hope not
Like I think I have psychosis or some sort of dissociative disorder anyway but I want to feel safe and at least finish college “normally”
Not rlly sure how to finish this. Thxx for reading this far. ur a menace :]
#therian community#otherkin#nhs#mental health#therianthropy#alterhuman#feline theriotype#catkin#leopard therian#canine theriotype#therian#advice#pls help#i am silly
12 notes
·
View notes
Text
TLDR without a summary, so best to not click lol
DID is a diverse disorder. For some people, they watch Mr Robot and feel seen best. For some people, they watch Monsters(anime) and feel seen best. For some people, they watch Moon Knight and feel best seen. Some people relate to stories or tabloids about Britney. Some people don’t relate to any of them besides having DID, too.
They may have different reasons behind their DID forming and different personalities they first projected on that specifically created DID that they needed to survive their specific stressful environments. DID is formed diversely to protect someone’s sanity and safety on the surface or to keep them alive past losing their sanity and sense of self.
Everyone with DID has at least 2 personalities, but that’s not always or mainly what makes DID difficult to survive through or what causes the distress with it. The personalities don’t have to be the cause of distress, and that’s why some people mourn after recovery or don’t want to integrate for recovery(take apart dissociative barriers and blend the personalities into each other as one personality). DID is a brain system to help us and keep something or almost anything hidden from others and the current self.
Those personalities may cause extreme distress or no distress depending on how the DID was formed and how the person grew to cope with DID. “No system is the same”. We say it all of the time. Doctors still don’t have actual proof about much of their theories besides that DID is a real disorder and commonly found in children or adults who have been through shit that humans in this century should not be going through or distressed by— or from multiple events over time that keep adding up until the person can’t take it anymore.
DID and Schizophrenia are what people think of when they hear, “insanity” or “gross/severe mental disorder”. High Schizotypy traits and psychosis isn’t rare in DID, either. It’s not a surprise when someone has both DID and Schizophrenia. Remember the, “DID is dissociative schizophrenia” theories? The answer isn’t relevant here, but the acknowledgment that people with DID are the pinnacle of gross insanity is there, everywhere.
There’s so many struggles that can come with having DID that it cannot be listed without taking up pages and becoming an essay, then a book. But something to note is that it’s usually created by trauma relating to people. It’s usually human-caused and related.
Then people tell us that we’re insane. That we can’t trust our intuitions or memory. That we can’t make decisions on our own. That we aren’t trustworthy or reliable— they use all of our symptoms against us and often in the same way that psychological abuse can create DID in someone by separating them from themselves and hammering out that we have to depend on them while taking the abuse, or else. Or else a lot. Or else anything that could harm or concern or distress the person with DID. Often threatening to take autonomy or something related to past trauma.
Idk what I was trying to think just now, but the thing is. I’m uncomfortable because I feel like the 2 most vulnerable presentations of madness that hurt the mad person are weaponized and used against us often with the same intentions or reasonings that create DID and Schizo/Psychotic Spectrum disorders from trauma. It’s hard for us to stand up for ourselves, to find safe support, to escape, to be free. When we try and if we succeed, some people meet heavy consequences from others that are traumatic, then they try to take advantage of the triggered DID to place the person back into the role that they want them in. It’s a cycle, and that’s why it’s so weird how DID is made fun of and not ever supported.
How do you think they created modern spies? I’m genuinely curious. How do you think big cults raise and keep their victims there, or have them go out into the huge and demonic world to try to recruit sick souls to save? Why do you think there’s child-stars in Hollywood and the music industry from parents obsessed with money either kill themselves or grow up into adults seeming “off” or outright insane? Or needing to be full of dangerous amounts of psychotropic meds? Have you never heard of brainwashing, and you don’t think that’s related to DID or shows an extreme example of what it could do to someone? That’s an extremely cruel and dangerous specified form of DID.
Are y’all without DID ever tired of pretending that we don’t exist, that we’re jokes, or that there’s a serious problem with how people react and keep cycles against people with DID? Ever tired of pretending that our QOL is low asf from people and how we tend to die younger and attempt suicide or show extreme self harmful behaviors at least once in our lives? You really think it’s a joke when you see someone showing symptoms of their mind breaking from stress you can’t imagine? Or something to dismiss? Are you sympathetic towards sick and disabled people or find mental illness and disability a joke? Which is it? Can you decide? Since our decisions and beliefs on that don’t matter to y’all. Because we’re the worst of the insane. But not insane enough to deserve sympathy and patience.
Monster is my favorite representation of DID. I am aware that the trauma causing their dissociative disorders was specifically government abuse related to create spies, and so it’s different from mine. But what caught my attention was the minimal focus on their personality changes compared to their other symptoms. And yes, to me, it seemed like all of the Kinderheim 511/Red Rose Mansion survivors had DID except maybe “the failure” son, who still was not sane. It could be said that he has a form of dissociative disorder, too. He wasn’t brainwashed because he escaped. He was a “failure” because they didn’t induce DID in him via cruelty and brainwashing.(& btw Monster isn’t unrealistic! Especially during the Cold War era, countries really did do this to orphaned, stolen, bought, POW, or their own related children for espionage or creating the perfect human race)
But Monster, compared to others I’ve accidentally seen or read haha, showed a lot of different sides to dissociative disorders and their consequences. It showed how people don’t believe the victims and have no support— they’re lucky if they have anyone yet don’t want others involved in what tore them apart. They show trances, fugues, unpredictable and scary breakdowns that others around them don’t understand, they show personality change in 2 characters that I can remember clearly that was triggered by memories they automatically forgot, and it was realistic.
That’s almost too realistic, and that never really happens in media. They did mess up on one point of the story. They were saved by multiple believing and trusting in them or working together with them. The doctors and children were patient even through their uncertainty and fear. They were gentle with the survivors and kind. They weren’t curious from morbid interest. They wanted Justice, safety, anddddddddd freedom. That’s why I’d say the main 3 were all saved although the ending for 2 of them was tragic. They all 3, from human kindness and grace, found what they needed inside of them.
It’s unrealistic only because I don’t see or hear of anything that could suggest people like that exist. The closest is psychologists, and I don’t think I need to explain why that could stop being an option for people with DID and related disorders. I’m being bitter. I know that. To others, they may think “you’re insane and paranoid and this isn’t true” or “you’re probably not accepting help” or “you have a bad personality probably so people don’t want to care”.
But you know, through all of my personalities and years of being alive and adapting to the people around me, my focus only about others for survival, I don’t ask for help anymore because I was punished for being insane. Every time. I can’t reach my hand out anymore because it’s been ripped apart by too many fucked up dogs. It’s that problem, and if I step closer or start to raise my arm hesitantly, dipping my feet into the waters because I’m still searching despite of it, they react to my hesitation with rage, with taking offense, with no patience or consideration of why.
I have a scar running down a bit above the inside of my elbow to where my inner forearm and wrist meet. I don’t think it’s too bad. I used a scalpel, so it was a clean cut and healed well. But it’s apparently enough for people to ask me if I’ve had surgery. To say I’m both sane and insane and haven’t been through anything but have been through a lot and don’t feel anything but have to walk on eggshells with and obnoxiously weird but it’s on purpose and that scar was made to manipulate others and—
Hey, mom and dad. I’m sorry, but I don’t have the energy or reason inside of me to pretend from 3 years old onward that I’m struggling just to fuck with your life. Why the fuck would I commit to something like that, and how does it make sense? It doesn’t.
Why are the effects left from me being broken apart still about others? It’s all about y’all, huh? The DID y’all hate is for y’all in y’all’s minds and in reality is used for y’all’s benefits at our cost.
And honestly I’m so tired of people who don’t have a form of DID or Schizo- disorders rn frrr. I’m tired. You’re cruel. You’re so cruel and think it’s natural and normal to be to us. Then you blame and hate us for being on guard or eccentric/deviant to societal norms or not fitting anywhere. No matter what we do, because of a disorder we didn’t want or understand was forming, we are used as tools or people to project anger onto. Because no one is rlly standing up for us. There’s no consequences to bullying someone Schizo or with DID. It’s cowardly.
It’s cowardly to choose to worry more for your reputation being harmed by standing up for and helping vulnerable people with fucked up heads who everyone uses as tools or to join them in that than stand by the values you claim to have and reach out your hand calmly.
Yes, some people are so hurt that you “have to walk on eggshells”. Is being considerate of others that hard for you? That you’d say that about people with DID?
#…#(If someone does read this there’s a lot to be misconstrued/misunderstandings could form from language so just ask tho)
8 notes
·
View notes
Text
Bsd characters as a mental disease/congenital disease
I don't own any of these characters. They all belong to Asagiri Kafka
Characters: Dazai Osamu, Atsushi Nakajima, Chuuya Nakahara, Akutagawa Ryunosuke, Edogawa Ranpo, Edgar Allan Poe, Fyodor Dostoevsky, Nikolai Gogol, Jouno Saigiku, Tetcho Suehiro
𝙰𝚝𝚝𝚎𝚗𝚝𝚒𝚘𝚗: i took all the information from Vikipedia( in russian) and translated it. This text is for the entertainment purposes only.

☠︎︎𝘋𝘢𝘻𝘢𝘪 𝘖𝘴𝘢𝘮𝘶☠︎︎
Cotard's syndrome
This syndrome occurs with a persistent desire to commit suicide and constant depression. People who have such a diagnosis complain about the loss everything that connects them with the world of the living: interests, tastes and even their own body, or any part of it. The sick have a belief that they are not longer people, but hte walking dead
☦︎𝘈𝘵𝘴𝘶𝘴𝘩𝘪 𝘕𝘢𝘬𝘢𝘫𝘪𝘮𝘢☦︎
Impostor syndrome
A psychological phenomenon in which a person is not able to attribute their achievements to their own quality, abilities, and efforts. Despite the external evidence of their co-activity, people affected by the syndrome continue to be convinced that they're cheaters and don't deserve the success they've achieved. They usually attribute their success to luck, getting to the right place and time, or misleading others into thinking they're smarter and more completent than they really are.
☯︎𝘊𝘩𝘶𝘶𝘺𝘢 𝘕𝘢𝘬𝘢𝘩𝘢𝘳𝘢☯︎
Dissociative identity split
Also used is the diognasis of Multiple Personality Disorder, or split personality- a rare mental disorder in which person's personality is divided, and it seems that there are several different personalities in the body of one person. At the same time, at certain moments, a person "switches"- one person replace another.
☹︎𝘈𝘬𝘶𝘵𝘢𝘨𝘢𝘸𝘢 𝘙𝘺𝘶𝘯𝘰𝘴𝘶𝘬𝘦☹︎
Mobius syndrome
This anomaly is congenital. Symptoms: the absence of any facial expressions as a result of impaired developement of some cranial nerves, as well as paralysis of the facial nerve. Patients can not smile at all, and their face resembles a mask.
✵𝘙𝘢𝘯𝘱𝘰 𝘌𝘥𝘰𝘨𝘢𝘸𝘢✵
Peter Pan syndrome
In modern psychology, there is such a thing like "Peter Pan syndrome". It affects people who don't want to grow up and take responsibility, infantile boys in their thirties who live exclusively for themselves, do not think about tomorrow and are afraid of serious relationships.
❦︎𝘌𝘥𝘨𝘢𝘳 𝘈𝘭𝘭𝘢𝘯 𝘗𝘰𝘦❦︎
Bibliomania
Bibliomania is an unhealthy collection, a patgological passion for collecting books. Like any hoarding mania, it's a desire for possession. Moreover, the obsession to acquire books is not necessarliy connected with desire to read them. This behaviour may be conscequance of a neurotic defence mechanism associated with some past trauma or other disorders.
✞︎𝘍𝘺𝘰𝘥𝘰𝘳 𝘋𝘰𝘴𝘵𝘰𝘦𝘷𝘴𝘬𝘺✞︎
The "Jerusalem" syndrome
This is very rare disease, which is kind of religious psychosis and is provoked by visiting Jerusalem. The syndrome can be acquired by followers of any religion. The disease is provoked in this way: after travelling to Jerusalem, people with unstable minds begin to think they've become prophets(gods), can establish their own religions and even demand repetance from sinners.
☻︎𝘕𝘪𝘬𝘰𝘭𝘢𝘪 𝘎𝘰𝘨𝘰𝘭☺︎︎
Angelman syndrom
Angelman syndrome is a pathology caused by genetic anomaly, characterized by such sighs as delayed mental developement, sleep disorders, seuzures, chaotic movements(especially of the hands), frequent laugher or smiles. This syndrom is also called "Parsley syndrom" or "Happy doll syndrom".
❤︎𝘑𝘰𝘶𝘯𝘰 𝘚𝘢𝘪𝘨𝘪𝘬𝘶❤︎
Anosognosia of blindness(Anton-Babinsky syndrom)- lack of awareness and denial of the presence of blindness. At the same time, confabulatory visual images are perceived as real. Anasognosia of blindness is a rare symptom of brain damage in the occipital lobe.
ꕥ𝘛𝘦𝘵𝘤𝘩𝘰 𝘚𝘢𝘪𝘨𝘪𝘬𝘶ꕥ
Allotryophagy
It's a mental illness. Symptoms: the desire to eat inedible objects: paper, dirt, clay, coal, glue and more. This syndrom is often found in people with mental retardation. Of course, there are also accidents with this disease: patients can swallow dangerous and sharp objects, for example, glass, nails, needles, etc. Allotryophagia can manifest itself in a midler form, for example, with nervous disorders or during pregnancy.
#osamu dazai#bsd akutagawa#bsd tetchou#bsd jouno#bsd dazai#bsd atsushi#ranpo edogawa#tetchou suehiro#saigiku jouno#jouno saigiku#dazai osamu#fyodor dostoevsky#nikolai gogol#chuuya nakahara#akutagawa ryuunosuke
86 notes
·
View notes
Text
cats who i think should be canonically disabled Or that should have been handled better:
- bluestar (her whole mental health thing nearish the end of her life?? ABSOLUTELY psychosis please give her kitty antipsychotics)
- cloudtail (he shoulda been deaf pleaseplease)
- snowkit (PLEASE let him live)
- longtail (longtail coming out of retirement to train jayfeather!! longtail learning how to be a blind warrior alongside jaypaw!!!)
- hollyleaf (her vision getting fucked up bc of how long she spent in the tunnels....her working w jayfeather to adapt to being blind)
- dovewing (when her powers left they should've taken a lot of her senses with them!! hard of hearing dovewing!! partially blind dovewing!!!)
- berrynose (the man's missing half his tail!! cats need those!!)
- ptsd twigbranch (did you SEE how she reacted to bramblestar in...asc book 1 i think? girl's traumatized to high hell)
- bramblestar (some sort of dissociative disorder the guy canNOT be present in his own body. like he's a shithead but he's also NOT a mentally healthy cat)
- any of the arc 1 elders. WHY r they called things like "one-eye" (and why the dash?? that is never ever used ever again) and "halftail" like i could see halftail being a natural name (we've got onekit/whisker after all) but ONE EYE???? BRO.
- alderheart (autistic anxiety kitty :] )
- shadowsight (idk Why but he gives me Such plural vibes. shadowsight w an ashfur introject fuckin things up in his head. shadowsight w some random-ass loner named twig in his head. shadowsight thinking this is an offshoot of the ashfur thing)
- shadowsight, again (HE SHOULDA KEPT THE SEIZURES.)
- fallen leaves (that cat has Something going on in his head. depressive disorder maybe?? agoraphobia?? plain old trauma from dying in the tunnels and still living there for generations afterward??)
- crookedstar (the guy would have had to relearn how to eat. i feel like his jaw would have played a much more disabling role than it seemed to)
#sundrops#warrior cats#< - less for maintagging and more for categorization. however feel free to add on
9 notes
·
View notes
Text
Table of overlapping symptoms and unique features of schizophrenia and DID, from chapter 21 of Psychosis, Trauma and Dissociation.

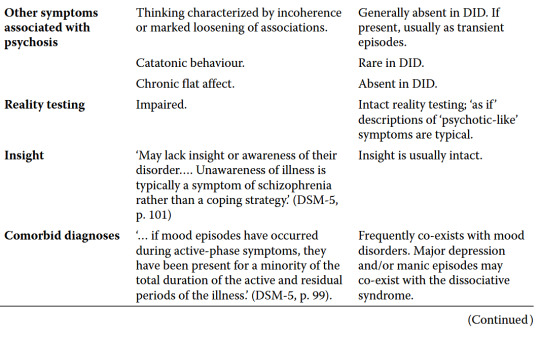

Comparison of dissociative disorder (DD) and psychotic disorder (PD) patients on personality and cognitive testing, from chapter 22 of the same book.


#graypost#nerdpost#did#schizophrenia#comorbidity#psychology#psychosis#psychotic disorders#dissociative disorders#book: psychosis trauma and dissociation
30 notes
·
View notes
Note
I need some help...
I have periods of time (could be from 1 minute to over a day) where I either feel like I'm not real, everything else isn't real, or both. At first it was every once in a while, but now it's gotten a lot more frequent, to the point where it makes it difficult for me to do anything. It's really bad, and I can't even look at the sky anymore without feeling like I'm going to throw up. For a while, it was manageable, but now whenever I look at an object I feel like something's off; it's either too detailed or not detailed enough, a slight shade different than it "should" be, doesn't look like how I remember it to be, etc. I think it's going to keep on getting worse, because earlier today I couldn't even look at my reflection. There's just a voice in my head now that tells me that nothing is real. I don't even feel like I am actually in my body, I have a constant headache all the time, and I can barely remember my name. I think this started happening because I've consumed so much media (for example, books, webtoons, TV series, movies, sometimes even daydreaming), but now the only way for me to get my mind off of feeling like nothing exists is to consume more media, which then furthers the problem. I really don't want to be alive anymore because my brain just hurts all the time. Any suggestions on how I could try to fix this?
That sounds A LOT like disassociation/dissociation or even psychosis. Both are obviously serious and scary, and I would definitely recommend seeing a psychiatrist as it can be related to trauma, PTSD, mental/personality disorders, etc.
I’m not an expert by any means in mental health, but that’s what I’d recommend.
#Lizzie speaks#lizzie answers#op#advice#mental health#mental health support#positivity#love#self love#self care#take care of yourself#recovery
5 notes
·
View notes
Note
I'm a DID system with MADD, but lately I've been catching on to other symptoms that don't really fit into these categories as far as I can tell. It took me a long time to catch on due to dissociative amnesia. The biggest thing is visual hallucinations, usually in the form of fluttering shadows, but I've had times where my brain convinces me that it's something there that's dangerous, and even if I know it can't possibly be real, the fear is still real. I occasionally get auditory hallucinations too I think, I have a hard time telling with those though. I don't have paranoia as far as I can tell, anxiety, but that's as far as I've ever seen it go.
I read through some things on your blog, and some things click together in ways I never even thought about before, which just serves to confirm suspicions I've had for a while about being psychotic on some level.
All of that being said, I have a few questions.
How does psychotic and schizo spec disorders work with DID and MADD? Can those things cause/effect delusions (such as the content of them, things like that)?
What's the difference between psychosis and schizo spec? (If there is any, or is one more like a sub-category?)
Hi there! Welcome on the blog :) I'm glad it was helpful in terms of clicking some things for you!
I could ramble a lot, but I'm gonna try to stick to answering your questions to the best of my understanding (feel free to ask follow up questions, i may also be able to do a bit more research for you later).
First off, how psychosis and schizo spec disorders interact with maladaptive daydreaming and DID is a very big question. There's been some interest in the intersection between trauma, dissociation and psychosis for sure.
One of my former professors recently was an editor and contributor in a selection of articles collected in the book 'Psychosis, Trauma and Dissociation : Evolving Perspectives on Severe Psychopathology'.
I'm very interested in reading some of those articles, and I recently found a pdf version, so once I push through the inertia I hope to have gained a better understanding of new and different perspectives on the matter. It's safe to say that the sharp distinction between psychosis and dissociation often seen in popular psychology is actually a lot more complicated, messy and unclear in reality. MADD, as well as DID, as well as psychosis, reflects something about yourself, your life and your culture. The brain can't come up with anything that you couldn't come up with, so to say. And beyond any diagnostic categories, these are all your experiences. They cannot be separated into neat boxes, and as such they can and do interact. How so is individual, of course. And I would need a bit more info to say something more personal about the matter.
The difference between psychosis and schizo spec.. keep in mind that there's different ways to understand schizo spec, but this is how I use these terms:
Experiencing psychosis for any reason makes you psychosis spec. Psychosis spec people may not have anything other than psychosis in common with many schizo spec people. Non-shizo disorders that can cause psychosis are plentyful. Classics include depression and bipolar, but depending on who you ask it also can be a part of ptsd, ocd and more.
The schizospec disorders, at the most basic, are the disorders that are called schizo-something. Schizophrenic, schizoaffective, schizotypal, schizophreniform, schizoid..
The schizo spec disorders, while different, usually involve some level of psychosis, but they also come with other stuff that sets them apart. Ofc everyone is an individual, but common things include: strong negative symptoms (lack of motivation, energy, etc), cognitive difficulties (ala adhd or a learning disorder), social cognitive impairment and sensory difficulties (could look like asd), and a bunch of hard to explain, diffuse 'ways of relating to yourself and the world', such as overreflecting and questioning everything and feeling distanced to the world or like there is no difference between you and the world..
Interestingly, many of these can feature during/just around psychosis in non schizo people, but for schizo spec people it's often just how we are.
While some things like negative symtoms and cognitive symtoms often get worse after a big psychotic break, most schizo spec people have been more or less visible neurodivergent always, in a 'schizospec flavour' that is easier to notice in retrospect. Many get diagnosed with autism or adhd.
I don't have much data on this, but anecdotally it's quite rare for me to run into a schizo spec person who hasn't always -even before noticeable psychosis- struggled with reality on some level.
Out of the schizo spec disorders I mentioned, schizophrenia and schizoaffective are always included. I include schizotypal as well bc while it usually doesn't involve full blown psychosis, the patterns of experience and thinking are often quintessentially schizo spec in nature. Schizoid pd I also include, but I think it's quite individual whether a schizoid person feels kinship with the schizospec community. That said, many do, given that the symptoms of schizoid pd can be much like negative symptoms of other schizospec disorders, and there are often many other shared attributes.
So you can be schizo spec without having psychosis (fairly rare), and can be psychosis spec without being schizo spec.
There's obviously a huuge overlap in experience. And one of the reasons I am very careful to include both most of the time in my writing, is because I don't want anyone to feel excluded based on the categorization of their experience. The differences outlined above are statistical in nature, and cannot be used to predict any one singular person's experience.
7 notes
·
View notes
Text
Seventeen years ago the American Psychological Association launched a mapping project in the exciting book, Varieties of Anomalous Experience (E. Cardeña, S.J. Lynn and S. Krippner, eds.). Here a number of psychologists write about quirky themes such as lucid dreams, out-of-body experiences, telepathy, precognition, healing and other strange experiences that are not in harmony with our usual perception of reality. However, it becomes evident from the case studies in the book that such experiences do not have to be confusing or intimidating, but in fact can also be deeply meaningful. For example, many people experience a new and more serene relationship with both life and death after so-called near-death experiences, where one typically has a feeling of leaving the body, being enclosed by a great light, meeting deceased family members, angels or other spiritual beings, and the like.
The authors of Varieties of Anomalous Experience emphasize the experience, and especially the aspects connected with personal meaning, and largely refrain from telling us how these phenomena are to be objectively understood. Psychologists and psychiatrists will typically explain (or explain away) such experiences, resorting to pathological descriptions: hallucination, psychosis, dissociation, trauma, etc. But, interestingly enough, two of the three editors of Varieties of Anomalous Experience (Krippner and Cardeña) have said elsewhere that they think at least some of these strange phenomena are likely to be objectively real—i.e. that beyond people’s feelings of having telepathic contact there may also occur genuine telepathy (a direct transfer of thoughts, feelings and sensations from one person to another).
A similar stance has been taken by a number of talented physicists, including Nobel Prize winners, who have argued that these kinds of phenomena, rightly understood, need not be contrary to the Laws of Nature. For example, Cambridge Professor Brian Josephson, who won the Nobel Prize in Physics in 1973, claims that both telepathy and psychokinesis (direct impact on the physical world by the power of mind) are ‘objectively occurring phenomena’ (not just hallucinations, etc.).
-- Terje G. Simonsen, A Short History of (Nearly) Everything Paranormal
10 notes
·
View notes
Note
Hey Elliott! Could I ask you for the pdf of that psychosis, dissociation, and trauma book you mention in your tags on a recent reblog?
Here's a link to the book that should work!
10 notes
·
View notes
Text
1/31/2023: Me
I keep thinking about that scene in adolescence where I was in a dark bookstore and found a book about vampires in a cardboard box. The darkness started settling over me again. This was important partially because it's tied to past trauma but also because I feel like I was really "me," maybe for one of the last times.
I was still that self-serious girl who did well in school, loved reading and drawing and had some degree of a relationship with her relatives. I still had a little hope for the future. I dreamed about being an artist. I could be solemn but a little funny and creative. Teachers and classmates liked me.
I wasn't happy--in fact, I was miserable during this time--but I was still ME. My personality was intact. I feel connected to this version of myself because she's one of the last remnants of the person that I was until high school.
Everyone changes, but this is different. I didn't change naturally as I grew older. The delusions, dissociation and eventual psychosis that started in high school disintegrated my personality. Even I don't recognize the person that I became, especially in my early twenties.
I'm doing better than I was then, but I'm still not "me." "Me" is gone. My personality is shattered. The girl in that adolescent memory was whole despite her issues, and now I'm a pile of broken glass.
At the risk of sounding defeatist, I don't think that I can go back. All I can do is try to move forward with this new personality.
I don't have dissociative identity disorder, but I've heard people with DID talk about feeling depleted, like each split took part of their personality. That's how I feel, too. But I don't have personalities to integrate into my consciousness and restore the old "me." It's just...gone.
There's an adult version of me who grew up without all this bullshit running around. I don't hear much from her, though. I don't think she's an alter because she never controls me or takes over or anything like that. She just hangs out in the background. Strange person. I can tell that she has an odd sense of humor but in a good way. Her parents didn't make her feel bad about herself--at least not to excessive levels.
And "child me" is still in here, but I avoid her because 1. I don't like her and 2. trying to interact with her has often made my problems worse. Gonna set that aside for another time.
Maybe reaching out to them would help, but again--I don't think it would work right now. I'm focused on other things.
Thanks for reading,
📔
#actually psychotic#actual ptsd#actually ptsd#ptsd#ptsd recovery#living with ptsd#complex ptsd#depersonalisation disorder#dissociative#dissociation#depersonalization#disassociation#actually dissociative#dpdr#actually dpdr#entry#regression#age regression#child regression#repression
4 notes
·
View notes
Text
I've actually found there's a LOT of decent science out there that's vaguely relevant to plurality and dissociation that doesn't fall into the pitfalls of The Tiny DID Research Community and all its... let's just say *problematic* researchers.
Most of my favorite researchers (bar Bethany Brand) who delve into plurality aren't DID researchers at all, but instead psychosis researchers, especially in the field of voice-hearing. I recently acquired a copy of Dr. Eleanor Longden's new book (at her recommendation to me!) and it discusses concepts such as integration (not final fusion, integration as in more cohesive and fluid communication between parts), multiplicity of selves, trauma, dissociation, and compassion for parts, without ever talking about DID itself (at least from what I've seen so far).
And I think... maybe this is the way forward for research? Psychology's treatment of DID is fraught with unethical therapy, bad science, and morally corrupt researchers, and this has brought about an unfortunate but understandable mistrust of DID research as a whole. Going into DID research can be a fatal blow to a psychologist's academic career sometimes. Which sucks, because like, what's the alternative? People on the plural spectrum are disregarded as crazy or exaggerating or plain old making shit up?
Not necessarily. You can look at all the core concepts of plurality - dissociation, integration, compassion for parts, etc etc from a novel psychosis treatment framework. Traditional treatment for voice hearers has been mostly "ignore and suppress the voices", but research is showing that this is unhelpful at best and harmful at worst, in most cases. Understanding and compassion for voices/self states/etc as part of a greater system looks like the way forward, and seeing multiplicity as a spectrum that we all are on is very helpful.
Plus it turns the stupid idea that "DID alters are real and should be communicated with and psychosis voices are fake and crazy and should be ignored" that I would often see tauted around in Tumblr DID circles, on its head.
It's basically just different manifestations or flavors of the same thing.
4 notes
·
View notes
Last Seen Blogs

masachairs13-blog
Masachairs

bluebayard
THE TIME'S ALWAYS RIGHT TO FIX WHAT'S WRONG

cinema-corner
Cinema-Corner

theellipelli
ROSE ROSE
