#gender affirming health care
Photo








if you’re kaiser and you’re reading this, DON’T YOU DARE RESCHEDULE ME AGAIN my lungs can’t take it, thanks
#cw: anti-trans news#cw: transphobia#mental health#top surgery#trans rights#gender affirming health care#gender#transmasc#nonbinary#genderqueer#lgbtq#queer#trans#anxiety#journal comic#autobio comic#personal
1K notes
·
View notes
Text
HRT: hormone replacement therapy. Common forms include pills, injections, and gels.
–
We ask your questions so you don’t have to! Submit your questions to have them posted anonymously as polls.
#polls#incognito polls#anonymous#tumblr polls#tumblr users#questions#polls about lgbtq stuff#submitted dec 9#polls about health#hrt#trans#gender#transition#hormones#gender affirming care#transitioning#estrogen#testosterone
741 notes
·
View notes
Text
The Campaign for Southern Equality, in partnership with state and local organizations, is providing rapid response support to the families of youth who are impacted by anti-transgender healthcare bans that are passing across the South. We are providing grants, navigation support, and resources to impacted families as they ensure their children can access the care they need and deserve. We are currently providing support to impacted families in Mississippi, Tennessee and South Carolina, and we are preparing to work in other states.
Please join us by donating.
We are honored to work on this project in partnership with The TRANS Program, Mississippi Rising, Inclusion TN, and OUT Memphis.

(ID: text reads "Donate to support the Southern Trans Youth Emergency Fund. Fuel our work to provide direct support to trans youth and families impacted by anti-transgender healthcare bans across the south", below this the Campaign for Southern Equality logo and a link to the fund on their website.)
#trans#transgender#transgender health care#trans healthcare#trans healthcare bans#gender affirming care#trans healthcare fund#trans healthcare funds#queer#nonbinary#genderqueer#lgbtq#lgbtqia#lgbtqiap
2K notes
·
View notes
Text
Trans research and scientific consensus
(2020) - Study of 139,829 students finds that in comparison to other students, transgender identity, especially non-binary identity, is associated more with perpetrating bullying than being bullied. Non-binary identity was most strongly associated with involvement in bullying, followed by [transgender] opposite sex identity and cisgender identity.
(2023) 21 leading experts on pediatric gender medicine from 8 countries wrote a letter to Wall Street Journal expressing disagreement over how gender dysphoria in youth is treated, voicing concerns against things such as the affirmative model and research conducted outside of the US has found hormonal interventions for gender dysphoria to be without reliable evidence. Among these international experts is Dr. Rita Kaltiala, chief psychiatrist at Tampere university gender clinic and author of several peer-reviewed studies on trans medicine and Finland's top authority on pediatric gender care.
(2023) Landmark study from Denmark on 3,800 transgender patients pulled data from hospital records and applications from legal gender changes and discovered 43% of this group had a psychiatric illness compared with 7% of non-trans group, and despite "gender affirming care" and legal gender changes, still had 7.7 the rate of suicide attempts and 3.5 times the rate of suicide deaths. Researchers state this rate is likely even higher due to missing data.
(2016) Study finds association with increased risk of multiple sclerosis for trans women taking estrogen/reducing testosterone levels.
(2023) Metadata study shows, at best, no improvement for patients in gender-affirming care. "The conclusions of the systematic reviews of evidence for adolescents are consistent with long-term adult studies, which failed to show credible improvements in mental health and suggested a pattern of treatment-associated harms. Three recent papers examined the studies that underpin the practice of youth gender transition and found the research to be deeply flawed. Evidence does not support the notion that “affirmative care” of today’s adolescents is net beneficial."
(2011) Long term follow up of 324 transgender people having undergone sex reassignment surgery in Sweden, found that trans women retained male patterned incidents and rates of violence and had a greater significance and rate of rape and sexual violence than cisgender men. The study also found, "Persons with transsexualism, after sex reassignment, have considerably higher risks for mortality, suicidal behaviour, and psychiatric morbidity than the general population. Our findings suggest that sex reassignment, although alleviating gender dysphoria, may not suffice as treatment for transsexualism, and should inspire improved psychiatric and somatic care after sex reassignment for this patient group."
(2020) Largest study to date on 641,860 people finds association with autism and "gender diversity", "Gender-diverse people also report, on average, more traits associated with autism, such as sensory difficulties, pattern-recognition skills and lower rates of empathy — or accurately understanding and responding to another person’s emotional state".
(2022) US study examining 10 years of data on 952 people finds large percentages of young adults prescribed hormones for trans identity no longer getting the drugs 4 years later. Discontinuation rate for both sexes combined = 30%. Female discontinuation rate as high as 44%. The standard disinformation pushed is that only 1-2% of people who begin medical transition end up desisting. But these figures show that in this cohort of young adults, the overall rate of discontinuing hormone treatment ranged from a low of 10% to a high of 44% within a space of just 4 years.
Abruzzese et al. 2023 'The Myth of “Reliable Research” in Pediatric Gender Medicine: A critical evaluation of the Dutch Studies—and research that has followed'
More to come.
#trans#transgender research#transgender health#trans health care#gender critical#detrans#desistance#detransition#FTM#MTF#non binary#gender studies#gender identity#LGBTQ#trans identity#gender diverse#autism#gender dysphoria#gender affirming care#gender affirmation#transitioning#protect trans kids#protect trans youth
453 notes
·
View notes
Text

The Tavistock performed gay conversion therapy in broad daylight, while undertaking medical experiments on kids with autism spectrum disorder (ASD).
https://www.thetimes.co.uk/article/it-feels-like-conversion-therapy-for-gay-children-say-clinicians-pvsckdvq2
So many potentially gay children were being sent down the pathway to change gender, two of the clinicians said there was a dark joke among staff that “there would be no gay people left”.
“It feels like conversion therapy for gay children,” one male clinician said. “I frequently had cases where people started identifying as trans after months of horrendous bullying for being gay,” he told The Times.
Transing the gay away is what Iran does.
#Wesley Yang#Tavistock#Time to Think#Hannah Barnes#gender affirming care#gay conversion therapy#conversion therapy#autism#autism spectrum#queer theory#gender ideology#mental health issues#mental health#medical malpractice#medical corruption#medical scandal#trans the gay away#trans away the gay#religion is a mental illness
269 notes
·
View notes
Text
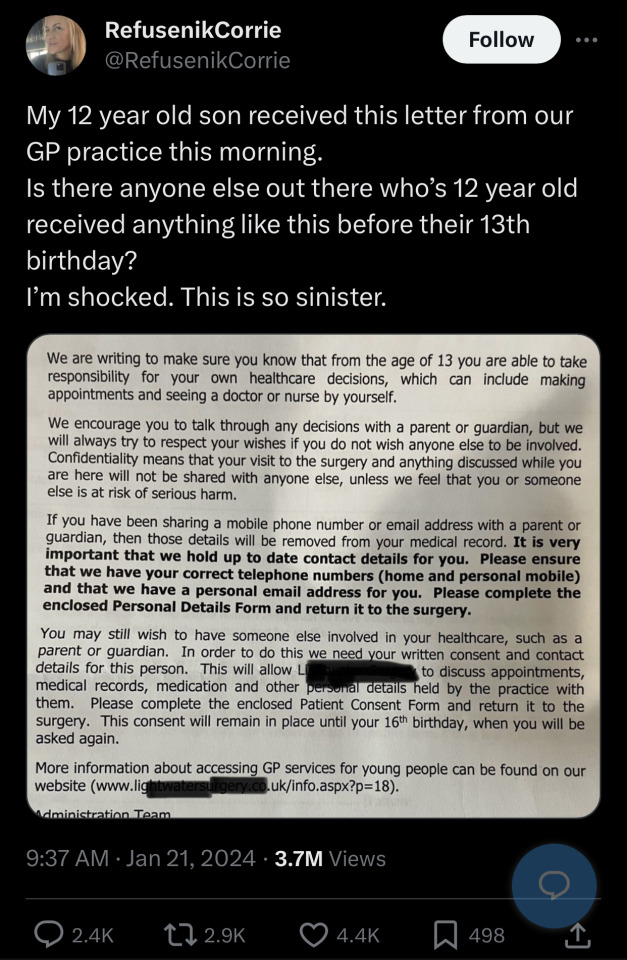
What’s so “sinister” about a child knowing their rights? Being freaked out by doctor-patient confidentiality is not showing concern, you just want to control your kid because you view children as not deserving of privacy and autonomy. There are plenty of reasons why a 12-13 year would want to speak to their doctor without their caregivers present:
They could have questions about their growing body that they’re too embarrassed/scared to ask their parents because FUN FACT! Not all parents are safe to people to talk to!
Someone in their life could be abusing in some way them and either their parents don’t believe them or they’re too scared/ashamed to talk to anyone else about it and the doctor-patient confidentiality could make them feel safe enough to speak up!
Their parents are sex negative/strict Christians and the child wants to expriment sexually but don’t want to get pregnant, get someone else pregnant or get STI/Ds, their doctor can provide ways to avoid just that, like contraceptives, because GUESS WHAT?? Teenagers are going to have sex with each other whether you approve of it or not!
Their parents could be an anti vaxxers and the child doesn’t want to get polio or some other illness that can be prevented!
Their parents could be controlling T3RF/GC cunts (just like the user who wrote the tweet above!) and wants to transition because FUCKING NEWS FLASH: Your children aren’t property and they’re autonomous beings, who deserve to make medical choices for themselves!
If your teenage child is desperate enough, they will try and go behind your back to transition or at the very least prevent going through a puberty that will make their dysphoria worse until they’re old enough to go on HRT.
If you think allowing a 13+ year old to have a say on who gets to be in the doctor’s office with them is “sinister” then maybe you need to ask yourself why you’re willing to deny your 13+ year old child privacy and bodily autonomy so you can ensure that only YOU get to decide what YOU want to happen to your teenager’s body!
#sage ponders#youth liberation#youth lib#child rights#youth rights#bodily autonomy#childrens rights#kids are people too#trans kids#trans youth#gender affirming care#anti terf#fuck terfs#dni terfs#anti gender critical#kids rights#children health#trans healthcare#child health#childism#adultism#body autonomy#anti ageism#adult supremacy
70 notes
·
View notes
Photo

y’all my top surgery consult HAPPENED! And it was GREAT!!! Now just waiting on the scheduler to get booked for a surgery date.
In the meantime here’s a doodle I forgot about in my drafts folder of me wearing this bangin hoodie I got from JustSaySK’s mutual aid fundraiser for community members’ top surgery costs. I’m extremely lucky to live in a place where gender affirming care is fully covered by my health insurance. This is how it should be everywhere!! But since it’s not, we gotta keep supporting each other financially when we can (and keep fighting like hell to change this gd system). Bonus when we also get to wear a soft and perfect hoodie that makes transphobes uncomfy when they figure out what it is 😎
#yes those are top surgery scars and a chest tattoo on the hoodie#transmasc#top surgery#gender euphoria#gender#gender affirming health care#lgbtq#queer#genderqueer#nonbinary#disasters and other genders
347 notes
·
View notes
Text
DIY HRT: purchasing and using hormone replacement therapy without a prescription.
–
We ask your questions so you don’t have to! Submit your questions to have them posted anonymously as polls.
#polls#incognito polls#anonymous#tumblr polls#tumblr users#questions#polls about health#submitted dec 19#polls about lgbtq stuff#gender#hrt#hormones#transitioning#gender affirming care#trans health#transition#diy hrt
344 notes
·
View notes
Text
Every time someone says we shouldn’t allow gender-affirming care for minors because evidence is low quality, you need to ask them if they’re suggesting banning abortion and birth control.
However they answer, they’ll be showing their whole ass.
I talk about their respective evidence bases here.
#transgender#trans#lgbtq#lgbtqia#queer#gay#lesbian#lgbt#gender affirming care#science#abortion#birth control#reproductive rights#reproductive health#reproductive justice
33 notes
·
View notes
Text
Sophie Perry at PinkNews:
The documents leaked by the Good Law Project and reported by QueerAF state that young people and their families who use “unregulated” and “overseas providers” for gender-affirming care should cease doing so, or they may face safeguarding referrals.
Speaking with QueerAF, Jo Maugham KC – executive director of the Good Law Project – said: “It’s reasonable to describe this as an attempt to force people to detransition.”
The document, which the Good Law Project states does not bear the name of any NHS professional, asks providers of mental health support to children and young people (CYP) to invite those on the national waiting list for gender services for a face-to-face appointment.
[...]
Furthermore, at the assessment stage, the providers have been asked to follow recommendations of the Cass Review and advise children not to take puberty blockers or gender-affirming hormones obtained via routes without “appropriate care”.
Whilst it is not stated what “appropriate care” refers to, the “overseas” routes being advised against.
If a trans young person disregards such advice and a provider considers that this “puts the child/young person at increased risk, then a safeguarding referral may also be appropriate in line with standard safeguarding approaches”.
In essence, if a trans young person seeks private gender-affirming care and their parents support them, they could be referred to local authorities.
[...\
In a statement provided to QueerAF following the publication of its report, a spokesperson for the NHS said that this process is about putting in place an “enhanced mental health support offer for all children and young people under 18 on the waiting list for specialist gender services, or who are awaiting their first appointment with the new services.”
England continues its not-so-sterling reputation as “TERF Island”, as trans kids in England could be forced to detransition following the Cass Review, per a leaked proposal from NHS England.
#NHS England#NHS#England#United Kingdom#Transgender Health#Forced Detransition#Detransition#Gender Affirming Care#Gender Affirming Healthcare#Good Law Project#QueerAF#Cass Review
20 notes
·
View notes
Video
Elevated Access
https://elevatedaccess.org/
#tiktok#Elevated Access#collective action#reproductive justice#reproductive freedom#reproductive rights#reproductive choice#reproductive health#lgbtq rights#LGBTQ#abortion is healthcare#abortion rights#gender affirming care#trans rights
118 notes
·
View notes
Text
By: Tamara Pietzke
Published: Feb 5, 2024
For six years I worked at a hospital that said all teenagers with gender dysphoria must be affirmed. I quit my job to blow the whistle.
I know from firsthand experience what hard times are. Though I had a happy childhood, raised as the middle child by working-class parents in Washington State, my mom died of ovarian cancer when I was 22.
After that, my family fell apart. I felt lost and alone.
I decided to become a therapist because I didn’t want anyone to go through what I had, feeling like no one on this planet cares about them. At least they can say their therapist does.
I earned my master’s in social work from the University of Washington in 2012, and I have worked as a therapist for over a decade in the Puget Sound area. Most recently, I was employed by MultiCare, one of the largest hospital systems in the state.
For the six years I was there, I worked with hundreds of clients. But in mid-January, I left my job because of what I will go on to describe.
The therapeutic relationship is a special one. We are the original “safe space,” where people are able to explore their darker feelings and painful experiences. The job of the therapist is to guide a patient to self-understanding and sound mental health. This is a process that requires careful assessment and time, not snap judgments and confirmation of a patient’s worldview.
But in the past year I noticed a concerning new trend in my field. I was getting the message from my supervisors that when a young person I was seeing expressed discomfort with their gender—the diagnostic term is gender dysphoria—I should throw out all my training. No matter the patient’s history or other mental health conditions that could be complicating the situation, I was simply to affirm that the patient was transgender, and even approve the start of a medical transition.
I believe this rise of “affirmative care” for young people with gender dysphoria challenges the very fundamentals of what therapy is supposed to provide.
I am a 36-year-old single mother of three young kids all under the age of six. I am terrified of speaking out, but that fear pales in comparison to my strong belief that we can no longer medicalize youth and cause them potentially irreversible harm. The three patients I describe below explain why I am taking the risk of coming forward.
* * *
Last spring, I started seeing a new client, who at 13 years old had one of the most extreme and heartbreaking life stories I’ve ever heard. (For the sake of clarity, I am referring to all patients by their biological sex.)
My patient’s mother has bipolar disorder and was so abusive to my patient that the mother was given a restraining order. My patient was sexually assaulted by an older cousin, by one of her mother’s boyfriends, and also once at school by a classmate. Her diagnoses include depression, PTSD, anxiety, intermittent explosive disorder, and autism. She is being raised by her mother’s ex-boyfriend (not the one who assaulted her).
The year before I started seeing her, when she was 11, she was hospitalized for talking about committing suicide. Later that year, a pediatrician diagnosed her with gender dysphoria after she started to question her gender. The pediatrician referred her to Mary Bridge Children’s Gender Health Clinic, whose clinicians recommended she take medicine to suppress her periods and that she think about starting testosterone.
Mary Bridge, MultiCare’s pediatric hospital, runs the gender clinic for minors and employs nurses, social workers, dietitians, and endocrinologists, who provide gender-affirming care, which includes prescribing hormones to young patients who question their gender. In order to get that prescription, patients first need a recommendation letter from a therapist. Because Mary Bridge is a part of MultiCare, their patients were often referred to therapists like me who were in their system.
In an April 2022 blog post, a Mary Bridge social worker wrote that the gender clinic’s referrals increased from less than five a month in 2019 to more than 35 a month in 2022. In May 2022, the clinic received a $100,000 donation from Patient-Centered Outcomes Research Institute “to study health care disparities” in transgender youth.
The clinic operates in Washington, one of the states with some of the most lenient legislation on gender transition for youth. In May 2023, the state legislature passed a law guaranteeing that youth seeking a medical gender transition can stay at Washington shelters—and the shelters are not required to notify their parents.
Because of my patient’s autism, it was difficult for us to engage in introspective conversations. During our first visit, she came over to my desk to show me extremely sadistic and graphic pornographic videos on her phone. She stood next to me, hunched over, hyper-fixated on the videos as she rocked back and forth. She told me during one session that she watched horror and porn movies growing up because they were the only ones available in her house.
She showed up to our therapy sessions in disheveled, loose-fitting clothes, her hair greasy, her eyes staring down at the ground, her face covered by a Covid mask almost like a protective layer. She went by a boy’s name, but she never raised gender dysphoria with me directly—though one time she told me she would get mad at the sound of her own voice because “it sounds too girly.” When I asked her how she felt about an upcoming appointment at the gender clinic, she told me she didn’t know she had one.
In between scrolling through videos on her phone, she told me how she cried every night in bed and felt “insane.” She described a time when she was eight years old and her mother nearly killed her sister. She remembered her mother being taken away. At times, she would “age-regress,” she told me, by watching Teletubbies and sucking on pacifiers.
When she started seeing me, she had recently threatened to “blow up the school,” which resulted in her expulsion.
I knew I couldn’t solve all of her problems, or make her feel better in just a few therapy sessions. My initial goal was to make her feel comfortable opening up to me, to make the therapy room a place where she was heard and felt safe. I also wanted to try to protect her from falling prey to outside influences from social media, her peers, or even the adults in her life.
With a patient like this, with so many intersecting and overwhelming problems, and with such a tragic history of abuse, it took our first three sessions to get her feeling more comfortable to even talk to me, and to understand the dimensions of her problems. But when I called her guardian last fall to schedule a fourth appointment, he asked me to write her a letter of recommendation for cross-sex hormone treatment. That is, at age 13, she was to start taking testosterone. Such a letter from me begins the process of medical transition for a patient.
In Washington State, that’s all it takes—a few visits with a therapist and a letter, often written using a template provided by one’s superiors—for minors to undergo the irreversible treatments that patients must take for a lifetime.
I was scared for this patient. She had so many overlapping problems that needed addressing it seemed like malpractice to abruptly begin her on a medical gender transition that could quickly produce permanent changes.
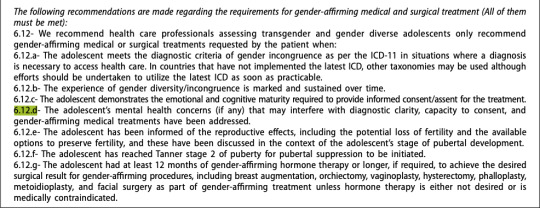
The MultiCare recommendation letter Tamara was given for approving the medical treatment of minors with gender dysphoria. I emailed a program manager in my department at MultiCare and outlined my concerns. She wrote back that my client’s trauma history has no bearing on whether or not she should receive hormone treatment.
“There is not valid, evidenced-based, peer-reviewed research that would indicate that gender dysphoria arises from anything other than gender (including trauma, autism, other mental health conditions, etc.),” she wrote.
She also warned that “there is the potential in causing harm to a client’s mental health when restricting access to gender-affirming care” and suggested I “examine [my] personal beliefs and biases about trans kids.”
When Tamara outlined her concerns about giving a patient testosterone to her manager at MultiCare, she was told to “examine your personal beliefs and biases about trans kids.” She then reported me to MultiCare’s risk management team, who removed my client from my care and placed her with a new therapist.
A risk manager’s job is to minimize the hospital’s liability, but in my case, they deemed that my concerns posed a greater risk to my client than giving her a life-altering procedure with no proven long-term benefit.
I shouldn’t have been surprised by this. Just a few months earlier, in September of last year, I was one of over 100 therapists and behavioral specialists at the MultiCare hospital system required to attend mandatory training on “gender-affirming care.”
As hard as it is to believe given my work, I hadn’t heard about gender-affirming care before that moment. I needed to know more. So each night in the week leading up to the training, I searched online for information about gender-affirming care. After putting my kids to bed, I sat glued to my computer screen, losing sleep, horrified at what I found.
I discovered that neither puberty blockers nor cross-sex hormones (testosterone or estrogen) were approved by the Food and Drug Administration as a treatment for gender dysphoria. In fact, prescribing these treatments to kids can have drastic side effects, including infertility, loss of sexual function, increased risk of heart attack, stroke, cardiovascular disease, cancer, bone density problems, blood clots, liver toxicity, cataracts, brain swelling, and even death.
While gender clinicians claim hormonal treatment improved their patients’ psychological health, the studies on this are few and highly disputed.
I found that those experiencing gender dysphoria are up to six times more likely to also be autistic, and they are also more likely to suffer from schizophrenia, trauma, and abuse.
The research also implies that the dramatic rise in these diagnoses across the West likely have a strong element of social contagion. In children ages 6 to 17, there was a 70 percent increase in diagnoses of gender dysphoria in the U.S. from 2020 to 2021. In Sweden there was a 1,500 percent increase in these diagnoses among girls 13–17 from 2008 to 2018.
Yet, countries that were once the pioneers of gender transition medicine are now starting to backtrack. In 2022, England announced it will close its only gender clinic after an investigation uncovered subpar medical care, including findings that some patients were rushed toward gender transitions. Sweden and Finland undertook comprehensive analyses of the state of gender medicine and recommended restrictions on transition of minors.
I decided—though it was potentially dangerous to my career and to me—to ask questions about the findings I discovered.
The training I attended laid out an affirming model of gender care—from pronouns and “social transition” to hormone treatments and surgical intervention. In order for children to be diagnosed with gender dysphoria, the training stated, patients must meet six of eight characteristics, ranging from “a strong desire/insistence of being another gender” to “strong preference for cross-gender toys and games.”
Tamara and her MultiCare colleagues were trained to diagnose gender dysphoria among their young patients when they met six of the eight above characteristics. It was made abundantly clear to all in attendance that these recommendations were “best practice” at MultiCare, and that the hospital would not tolerate anything less.
When the leader of the training brought up hormone treatments, I shakily tapped the unmute button on Zoom and asked why 70 to 80 percent of female adolescents diagnosed with gender dysphoria have prior mental health diagnoses.
She flashed a look of disgust as she warned me against spreading “misinformation on trans kids.” Soon the chat box started blowing up with comments directed at me. One colleague stated it was not “appropriate to bring politics into this” and another wrote that I was “demonstrating a hostility toward trans folks which is [a] direct violation of the Hippocratic Oath,” and recommended I “seek additional support and information so as not to harm trans clients.”
In the training, gender-affirming treatment is presented as “suicide prevention.” As soon as I closed my laptop, I burst into tears. I care so deeply about my clients that even thinking about this now makes me cry. I couldn’t understand how my colleagues, who are supposed to be my teammates, could be so quick to villainize me. I also wondered if maybe my colleagues were right, and if I had gone insane.
Later, my boss reached out to me and told me it was “inappropriate” of me to raise these questions, telling me that a training session was not the proper forum. When I tried to present the evidence that caused me concern—the lack of long-term studies, the devastating side effects—she told me she didn’t have time to read it.
“I am speaking out because nothing will change unless people like me blow the whistle,” Tamara writes. “I am desperate to help my patients.” In retrospect, this ideology had been growing in power for a long time.
I remember in 2019 seeing signs of how gender dysphoria arose among many of my most vulnerable female clients, all of whom struggled with previous psychological problems.
In 2019, I started seeing a 16-year-old client after her pediatrician referred her to me for anxiety, depression, and ADHD. When I first met her, she had long blonde hair covering her eyes, to the point you could barely see her face. It was like she was going through the world trying to be invisible.
In 2020, during the pandemic, she told me she had started reading online a lot about gender, and said she started feeling like she wasn’t a girl anymore.
Around this time, her anxiety became so debilitating she couldn’t leave her house—not even to go to school. After taking a year off school during the pandemic, she enrolled in an alternative school for kids struggling with mental health. I was relieved that she was making friends for the first time, and seemed to be feeling a lot better.
Then she started using they/he pronouns, identified as pansexual, and replaced the skirts and fishnet stockings she often wore with disheveled and baggy clothes. Her long hair became shorter and shorter. She started wearing a binder to flatten her breasts. She tried out a few different names before settling on one that’s gender neutral.
The official diagnosis I gave her was “adjustment disorder”—an umbrella term often applied to young people who are having a hard time coping with difficult and stressful circumstances. It’s the type of diagnosis that doesn’t follow a child forever—it implies that mental distress among kids is often transient.
She came out as transgender to her family in 2021. Her mother was supportive, but her dad wasn’t. Regardless, she went to her pediatrician seeking a referral to a gender clinic.
In 2022, she went to Mary Bridge Children’s Gender Health Clinic for the first time, where the clinicians informed her and her parents that if she didn’t receive hormone replacement therapy, she could be “at increased risk for anxiety, depression, and worsening of mental health/psychological trauma,” according to her patient records. Her dad refused to start his daughter on testosterone, and so all the clinic could do was prescribe birth control to stop her period due to her “menstrual dysphoria,” or distress over getting her period. Which is something I thought all teenage girls experienced.
Five months later, she swallowed a bottle of pills and her mother had to rush her to the emergency room.
By early 2023, my client logged on to our weekly session, which we started doing by Zoom, and she told me she identified as a “wounded male dog.” She explained to me that this was her “xenogender,” a concept she had discovered online, which references gender identities that go “beyond the human understanding of gender.” She said she felt she didn’t have all of the right appendages, and that she wanted to start wearing ears and a tail to truly feel like herself.
I was stunned. All I could do was silently nod along.
After the session, I emailed my colleagues looking for advice. “I want to be accepting and inclusive and all of that,” I wrote, but “I guess I just don’t understand at what point, if ever, a person’s gender identity is indicative of a bigger issue.”
I asked them: “Is there ever a time where acceptance of a person’s identity isn’t freely given?”
The consensus from my colleagues was that it wasn’t a big deal.
“It sounds like this isn’t something that’s ‘broken,’ ” one colleague wrote me back, “so let’s not try to ‘fix’ it.”
“If someone told me they use a litterbox instead of a toilet and they were happy with it and it’s part of their life that brings them fulfillment, then great!” she continued. “I might think it’s weird, but then again, not my life.”
After learning that one of Tamara’s patients identified as “a wounded male dog,” a colleague replied: “If someone told me they use a litterbox instead of a toilet and they were happy with it and it’s part of their life that brings them fulfillment, then great!” I was baffled and alarmed by her unquestioning affirmation. At what point does a change in identity represent a mental health concern, and not something to be celebrated and affirmed? Fortunately, my client never brought up her “xenogender” again. She also isn’t on testosterone due to her father’s disapproval. So I kept these thoughts to myself, and ultimately, in order to keep my job, I let it go.
Another female patient, who transitioned as a teen, serves as a warning of what happens when we passively accept the idea that gender transition will entirely resolve a patient’s mental health issues.
This client, who I started seeing in 2022, is now 23 and rarely leaves the house, spends most of the day in bed playing video games, and envisions no path to working or functioning in the outside world due to a variety of mental health problems. In 2016, this patient was diagnosed with autism, anxiety, and gender dysphoria. Later the diagnoses grew to include depression, Tourette syndrome, and a conversion disorder. In 2018, at age 17, the Mary Bridge Gender Health Clinic prescribed testosterone, despite the fact that this patient is diabetic and one of the hormone’s side effects is that it might increase insulin resistance. The patient’s mother, who has another transgender child, strongly encouraged it.
This patient now has a wispy mustache and a deepened voice, but does not pass as male. It turns out that testosterone, which will be prescribed for life, did not relieve the patient’s other mental illnesses.
My biggest fear about the gender-affirming practices my industry has blindly adopted is that they are causing irreversible damage to our clients. Especially as they are vulnerable people who come to us at their lowest moments in life, and who entrust us with their health and safety. And yet, instead of treating them as we would patients with any other mental health condition, we have been instructed—and even bullied—to abandon our professional judgment and training in favor of unquestioning affirmation.
I am speaking out because nothing will change unless people like me—who know the risks of medicalizing troubled young people—blow the whistle. I am desperate to help my patients.
And I believe, if I don’t speak out, I will have betrayed them.
--

https://www.tandfonline.com/doi/pdf/10.1080/26895269.2022.2100644
--

Amidst the scandal, Mary Bridge Children's has deleted the above blog post by self-professed "they/them," Aytch Denaro. However, the internet doesn't forget.
#Tamara Pietzke#Jamie Reed#whistleblower#medical malpractice#medical transition#medical corruption#gender dysphoria#gender ideology#queer theory#gender affirming care#gender affirming healthcare#gender affirmation#mental health#mental health issues#mental illness#gender cult#genderwang#religion is a mental illness
37 notes
·
View notes
Text
Sometimes it feels like because I'm a "successfully (medically) transitioning" ftm guy, I'm not allowed to experience mental health issues. Like I should be happy and confident.
Testosterone is not an antidepressant. I've been depressed since I was 8. Anxious for even longer. On and off psychosis since I was 14. I have BPD.
I started hormones. I like hormones. Hormones make my body change in ways I want it to. Hormones also make me emotionally volatile because it's fucking p u b e r t y. Puberty is not easy, and it's not my fault.
The fact that I still experience rather severe mental illness while on T doesn't make me any less trans. I feel pressured to be mentally healthy, otherwise I get intense imposter syndrome. I'm at the mercy of my own biochemistry.
Cis men are allowed to be mentally ill, why can't i? I'm sick of having to prove everything.
#ftm#ftm hrt#testosterone#gender affirming care#hormone therapy#transgender#trans man#mental health#mental illness
31 notes
·
View notes
Text
A Nebraska Republican state senator who voted for a combined anti-trans and anti-abortion bill that passed by one vote in the legislature has admitted that she didn’t pay attention to the issue.
State Senator Christy Armendariz represents the 18th District in the state.
Writing for New York magazine, journalist Lila Shapiro said that the Senator “led me to a bench in an empty hallway” to say that she “found it puzzling that a reporter from New York would come all the way to Nebraska to cover this affair.”
“I don’t watch the news or get the newspaper,” she told the magazine. “Is there anything going on I should be aware of?”
The writer told Ms. Armendariz that other states have passed other similar bills restricting trans and women’s reproductive rights and that an appeals court on the federal level in the Nebraska circuit had ruled that one of them was unconstitutional.
“So is it a big widespread thing?” she asked the writer, adding that regular Nebraska residents were unaware of the issue.
“I knocked doors for a year, and nobody brought this up,” the Senator said, adding that she wished that the legislation had never been brought to the floor.
For three months, a group of lawmakers in the state ground nearly all legislative business in the state to a halt, grabbing the nation’s attention with a remarkable filibuster to stifle a bill that would end gender-affirming care for young transgender people.
Late Tuesday 16 May, Republican lawmakers broke through, advancing a bill that not only bans gender-affirming care for trans people under 19 years old but also tacks on an amendment to outlaw abortion after roughly 10 weeks of pregnancy and hands the state’s GOP-appointed medical officer the authority to set the rules for affirming care for trans youth.
Hundreds of protesters filled the capital in Lincoln, standing outside the doors and in the gallery above lawmakers while chanting “one more vote to save our lives”; only one Senator would have had to defect from supporters of the bill to kill the legislation.
The vote – on the 78th day of a 90-day session – followed a series of manoeuvres that opponents argued were bending and breaking the rules of the state legislature to hammer through the legislation and avert the filibuster, which would allow opponents to occupy their allotted time to speak the bill to death.
“What you are attempting to do today is the lowest of the absolute lows,” state Senator Machaela Cavanaugh, who spearheaded the filibuster, told Republican lawmakers.
“You literally have to cheat at every moment of this debate in every possible way … You are allowing it to happen,” she added. “You do literally have blood on your hands, and if you vote for it, you will have buckets.”
State Senator Megan Hunt, the first openly LGBT+ member of the state legislature and the mother of a trans child, lambasted lawmakers for their “escape routes” from the capitol to avoid facing protesters.
“If you can’t go out and face them, you are not worthy,” she said. “Your legacy is filth.”
Protesters surrounded the state capitol chambers in Lincoln again on 19 May, chanting “keep your bans off our bodies” and “save our lives” as lawmakers made their final round of votes on the bill, which passed 33-15. The bill reached the exact number of votes needed to pass.
Republican Governor Jim Pillen signed it into law on Monday.
“We are working to inspire Nebraskans to get in the game so that abortion is simply unthinkable in the state of Nebraska,” Mr. Pillen said, according to WOWT.
He called the legislation “the most significant win for [the] social conservative agenda that over a generation has seen in Nebraska. I think that’s something we need to clap and shout about.”
At a show in Nebraska hours after the vote on Friday night, the artist Lizzo lambasted the legislation from the stage. “It really breaks my heart that there are young people growing up in a world that doesn’t protect them,” she said.
“Don’t let anyone tell you who you are. ... These laws are not real. You are what’s real, and you deserve to be protected,” she said.
“Hat tip to Senator Armendariz, who says she doesn’t know anything about the issue, doesn’t pay attention to current events, and wishes the bill she voted for hadn’t been introduced. It passed by 1 vote,” wrote Ari Kohen, a political science professor at the University of Nebraska–Lincoln.
“These are the people who devoted an entire legislative session to taking away people’s rights in the face of massive opposition from experts and ordinary citizens. They openly admit that none of their constituents mentioned this issue to them and they don’t know much about it,” he added. “We have a handful of legislators who care enough to listen and learn. And then we have the majority, who seem not to know or care what they’re doing as long as it feels right to them and they have the votes to do it. Awful.”
The Independent has requested comment from Ms. Armendariz.
#us politics#news#the independent#Nebraska#republicans#conservatives#Christy Armendariz#new york magazine#Lila Shapiro#gender-affirming care#gender-affirming care bans#trans healthcare#trans healthcare ban#abortions#abortion bans#reproductive rights#reproductive health#Machaela Cavanaugh#Megan Hunt#gov. Jim Pillen#WOWT#Lizzo#celebs#celebrities#music#Ari Kohen#tweet#twitter#2023#lgbtqia+ rights
72 notes
·
View notes
Text
Not asking about medical complications since that's sort of a different question; this poll is asking about the aesthetic and/or functional results. Obviously a person can have multiple different procedures done with different levels of satisfaction; select any one that applies.
Gender-affirming surgery includes but is not limited to procedures like breast removal, reduction, or augmentation; facial feminization or masculinization; the construction of different genitals; liposuction/body sculpting, etc.
–
We ask your questions so you don’t have to! Submit your questions to have them posted anonymously as polls.
#polls#incognito polls#anonymous#tumblr polls#tumblr users#questions#polls about health#submitted nov 17#polls about the body#polls about lgbtq stuff#lgbtq#trans#transgender#gender affirming care#gender affirming healthcare#gender affirming surgery#trans healthcare#surgery#medical
305 notes
·
View notes
Text
Dr. Riittakerttu Kaltiala, 58, is a Finnish-born and trained adolescent psychiatrist, the chief psychiatrist in the department of adolescent psychiatry at Finland’s Tampere University Hospital. She treats patients, teaches medical students, and conducts research in her field—publishing more than 230 scientific articles.
In 2011, Dr. Kaltiala was assigned a new responsibility. She was to oversee the establishment of a gender identity service for minors, making her among the first physicians in the world to head a clinic devoted to the treatment of gender-distressed young people. Since then, she has personally participated in the assessments of more than 500 such adolescents.
Earlier this year, The Free Press ran a whistleblower account by Jamie Reed, a former case manager at The Washington University Transgender Center at St. Louis Children’s Hospital. She recounted her growing alarm at the effects of treatments that sought to transition minors to the opposite sex, and her escalating conviction that patients were being harmed by their treatment.
Although a recent New York Times investigation largely corroborated Reed’s account, many activists and members of the media continue to dismiss Reed’s claims because she is not a physician.
Dr. Kaltiala is. And her concerns are likely to get more attention in the U.S. now that a young woman who medically transitioned as a teenager has just sued the doctors who supervised her treatment, along with the American Academy of Pediatrics. According to the suit, the AAP, in advocating for youth transition, has made “outright fraudulent statements” about evidence for “the radical new treatment model, and the known dangers and potential side effects of the medical interventions it advocates.”
Here, Dr. Kaltiala tells her own story, describing her increasing worries about the treatment she approved for vulnerable patients, and her decision to speak out.
20 notes
·
View notes
Last Seen Blogs


thejanicewong
Janice

sotlen-blog
It's story about my fall... in love.

transjimlakejunior
Protag Energy

hard-as-iron
In the Bleak Midwinter