#interoception difficulties
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs




Fun Fact
The total number of visits Tumblr.com received during January 2021 is 327 million.
Text

#yeast infection#actually autistic#interoception difficulties#executive dysfunction#I’m struggling#i can’t feel my body#I can’t feel when I’m thirsty#I can’t feel yeast infection#to much information#meme
12 notes
·
View notes
Text
I've reached 35 responses! They're very interesting, but the sample size is still small, and I don't think it's at all representative of the Tumblr autism community. If I can't reach at least 100 responses, I don't think I'll be able to analyze Tumblr community views on support needs in depth. I'll still post descriptive statistics for the overall sample, but I won't have the statistical power to do anything else.
I'd really appreciate if everyone could help by taking the survey and reblogging this post to their followers!
As a reminder, the survey is meant to understand how people use support needs labels. For example, what makes someone low support needs and not moderate support needs? The survey also helps show what the community is like in general in terms of demographics and experiences!
A summary of the current survey results are under the Read More. Again, especially if a community that you're in is under-represented, please help by spreading the survey link! I'd especially love to hear from more people AMAB, racial/ethnic minorities, people who are not yet diagnosed or were diagnosed as adults, and higher support needs individuals!
Age: Most participants are young; 60% are under age 25%, and 20% are under 18.
Gender: Over half of the sample is AFAB nonbinary, almost 1/3 is trans men, and almost all of the remainder (14%) is cis women. Only 2 people who are AMAB have taken the survey.
Race/Ethnicity: Non-Hispanic White people are very over-represented, making up 82% of the sample.
Diagnosis: 57% are professionally diagnosed, 20% are informally or soft-diagnosed, and 14% are seeking a diagnosis. Only 9% are neither diagnosed nor seeking a diagnosis.
The most common diagnoses are ASD with no level (33%), level 1 ASD (25%), and "mild autism" (13%).
16% were diagnosed before age 8, 24% between ages 9 and 15, 32% between ages 16 and 18, 12% between ages 19 and 25, and 16% over age 25.
Autism Support Needs: The most common self-identified support needs label is "low-moderate" (43%), followed by low (23%) and moderate (14%). Most would benefit from but do not need weekly support (31%), only need accommodations and mental health support (17%), or rarely need any support (6%).
Autism Symptoms: On a severity scale of 0 (not applicable) to 3 (severe), the average is 1.7 overall, 1.8 socially, and 1.7 for restricted-repetitive behaviors. The most severe symptom is sensory issues (2.1), and the least severe are nonverbal communication and stimming (both 1.5).
83% are fully verbal, and 97% have no intellectual disability.
38% can mask well enough to seem "off" but not necessarily autistic. 21% can't mask well or for long.
Most experience shutdowns (94%), difficulties with interoception (80%), meltdowns (71%), alexithymia (71%), echolalia (69%), and autistic mutism (66%). Very few experience psychosis (14%) or catatonia (11%).
Self-Diagnosis: 20% think it's always fine to self-diagnose autism, 29% think it's almost always fine, 31% think it's only okay if an assessment is inaccessible, 71% think it needs to be done carefully, and 11% think it's okay to suspect but not self-diagnose.
15% think it's always fine to self-diagnose autism DSM-5 levels (including if the person has been told they don't have autism), 15% think it's fine as long as autism hasn't been ruled out, 21% think it's almost always fine, 18% think it's only okay if an assessment is inaccessible, 36% think it needs to be done carefully, and 36% think it's okay to suspect but not self-diagnose.
26% think it's always fine to self-diagnose autism support needs labels (including if the person has been told they don't have autism), 29% think it's fine as long as autism hasn't been ruled out, 37% think it's almost always fine, 29% think it's only okay if an assessment is inaccessible, 43% think it needs to be done carefully, and 6% think it's okay to suspect but not self-diagnose.
Disability: 71% feel disabled by autism, 17% feel disabled by another condition but not autism, and 11% are unsure.
Comorbidities: The most common mental health comorbidities are anxiety (68%), ADHD (62%), and depression (56%).
The least common mental health disorders are schizophrenia spectrum disorders (0%), bipolar disorders (3%), tic disorders (6%), substance use disorders (6%), personality disorder (9%), and OCD (9%).
The most common physical health comorbidities are gastrointestinal issues (29%), connective tissue disorders (29%), autoimmune disorders (24%), neurological disorders or injuries (24%), and hearing/vision loss (24%). All others are below 20%.
Overall Support Needs: When considering comorbidities, the most common self-identified support needs label is moderate (37%), followed by low-moderate (31%) and low (17%).
#autism#actually autistic#actuallyautistic#level 1 autism#level 2 autism#level 3 autism#low support needs#moderate support needs#medium support needs#high support needs
426 notes
·
View notes
Note
Hi!
I have reached out to more people, but I'm still having problems with this, and I wanted to hear another opinion.
As a writer, do you have problems continuing a story once you hit a difficult scene?
Because I do, and honestly it's getting me frustrated at this point.
I have a good idea and a plot already done, but every time I hit a difficult scene I just get stuck, and can't write for weeks, sometimes months. I hardly even open the documents when it happens, and sometimes it comes right when I'm on a writing spree and being happy with my writing.
Do you have any advice on how to deal with this? How can I get past this issue and just keep writing more frequently?
I'd really like to hear it!
What do you do when you hit a snag?
When approaching this topic, the frustrating thing is that age-old advice has a lot of truth to it. Sometimes it is true that the best thing you can do when you're stuck is to stop struggling against the resistance and take a meaningful, intentional break to rest your mind and reset your thought process. Sometimes the key to getting started again is shaking up the routine and the altering the process until you find a new combination of habits that meet you where you are.
However, for a lot of us, the turmoil reaches deeper than that. A lot of people who do creative things are neurodivergent, so that has a place in the conversation when discussing what's preventing us from realizing our vision. Even if you don't identify with specific neurodivergence, there are a lot of tools and techniques that have been tried and tested for coping with immense, intrinsic difficulty with things like productivity, mindfulness, interoception, focus, and consistency. Just because these techniques are not specifically designated for you doesn't mean they won't be effective for you.
It is always a helpful exercise to take a step back and examine how you're feeling, both when you are writing and when you aren't, and try to identify any areas where you might be able to improve by changing things within your control.
When it comes to a specific scene holding you back from carrying on, I usually find that it's the result of a decision I made earlier in the plot that isn't serving the story as it continues to develop. I would take a chunk of time to take an analytical look at the scene, where it's come from, what is and isn't sparking in it (is the stagnation mostly due to the characters, events, environment, or lack of information, and is it a scene that is imperative to the reader's understanding?). A lot of the time, it's a scene that can be cut, or it's a scene that can be made redundant by infusing the necessary information of the scene into another place within the story.
If you've identified a scene as "a difficult scene", ask yourself why. If it's daunting because it's too long, then it can probably be cut way down and then added to later if while editing it seems a little thin. If it's challenging because things aren't falling into place and you aren't getting into a flow, then the set-up for the scene probably hasn't been developed effectively and you need to decide whether you're gonna go back in the draft to investigate or move on and return to it while editing.
If the information in the scene needs to be communicated at this specific point in the story, the problem might be the way you've chosen to present it. Pay attention to what your instincts are telling you, because pushing through a scene for the sake of getting past it will not produce a compelling scene to read. If you need to move past it, you have permission to do that. You can always come back and completely dig it up later.
Overall, I think it's very important to write with acceptance that the plot may not turn out the way you planned it. The process is much more effective and much more enjoyable if you aren't trudging along on a predestined path. If the characters and story develop outside of the lines, see where they go. You'll always have the opportunity to return to the outline and tailor later.
Best of luck,
x Kate
158 notes
·
View notes
Note
Hey, I really appreciate your answering sex ed questions and was hoping you might be able to help me out. Sorry for the long tmi I'm about to give but I don't know how to ask this except by listing out everything relevant I can think of.
I'm afab (cis-ish in the sense I don't particularly see myself as a woman but don't bother trying to get other people not to, but that isn't really important here) in my mid 20s and a virgin, and I don't know much about sex drive but what I do makes me feel like maybe there's something off about mine? I used to consider myself bi ace until I realised I did feel some degree of physical attraction to women that I don't to men so now I call myself a lesbian but the attraction I feel is still very... vague? Like, I'll see a pretty woman and get some kind of rush of feeling, but it's not really a particularly physical feeling of arousal (though I am autistic so it could be I just don't recognise it as physical because of interoception difficulties), more like... sorry if this is an inappropriate metaphor but. More like the urge to pet a really cute cat. I've made out with women and it felt vaguely nice (certainly nicer than with men which I've also done but it was awkward and vaguely uncomfortable) but no more than that. I don't get anything from my physical partners biting down on my neck or nipples or other common erogenous zones though I feel like they expect me to, and kissing is kind of nice but kissing with tongue feels awful. I'm not sure if I'd ever actually want to have full on sex, the thought of letting someone near my sex organs sounds unpleasant. I sometimes masturbate by rubbing my clit and there's a moment that feels like a climax where it gets really hard and sensitive and I used to think that was an orgasm but reading your recent description of an orgasm I'm actually pretty sure I've never had one. I've never had the urge to stick anything in my vagina, only tried it because I heard if it causes pain it might be a cause for medical concern (it didn't cause pain - it felt kinda nice, not anything special though and certainly not something I'd do without prompting). When I masturbate there's only one specific non sexual scenario that gets me off (though maybe about once a year at most I can successfully get off to sexual scenarios with fictional characters but never with real people and it isn't as effective). I used to masturbate more than I do now (I know it dropping off suddenly can be a cause for medical concern but it wasn't sudden, just spikes of activity getting gradually shorter and rarer - I can think of months when I'd do it every night to fall asleep but those are very much outliers scattered across the years rather than my baseline, which is occasionally doing it absentmindedly while falling asleep but very rarely intensely and on purpose). I probably should have sought out more sex ed at some point but sex just never felt very important to me.
Anyway I guess my question is. Is all this normal? Am I actually ace after all? Do I just have a low sex drive? Is any of this cause for medical concern? Do you have any idea how I might be able to actually get an orgasm, if what I thought was that actually wasn't?
hi anon,
all of this is incredibly normal. what I'm hearing is that you kind of like kissing women and aren't particularly interested in sex? that's awesome. kissing women is great, strongly recommend, and if that's all you're interested in then that's just dandy. no need to pretend to enjoy anything just because a partner expect you to; a polite "no thanks" will suffice, followed by kicking your partner to the curb if they don't listen to the no.
whether or not you call yourself asexual is up to you, that's none of my business and I can't pick for you. there actually isn't a secret barcode hidden somewhere on your body that will reveal your Real True Sexuality, you can just pick whatever words you want that kind of get the gist at any given time. would calling yourself asexual feel nice or helpful to you in anyway? if so, awesome! does it not appeal to you at all? okie dokie! don't do that then.
literally nothing you have described sounds like something that would be cause for medical concern, unless I missed something that's regularly causing you any physical pain or discomfort.
I think focusing on orgasms isn't that important, actually, and you can actually just touch yourself in whatever way you want for as long as it feels good, and then stop when it doesn't!
68 notes
·
View notes
Text
i do think there are meaningful differences in subjective cognition and cogitation, but i also think the way these differences are pathologized and treated like astrology or pop taxonomy ("well i have aphantsia i cant imagine visual stuff at all" "well i cant think about smells" "well i cant conceptualize music" etc) is completely misguided and the differences that do exist are attributable almost entirely to interoception, individual experience, and especially training, and especially especially early childhood or even infantile training you probably were not even aware you were receiving. if anything, the most recent neurological research has shown the brain is more plastic than anyone could have imagined and you can teach anyone to do or think about anything you want if you invest in it sufficiently.
my big "what do you mean my experiences arent universal" thing as an adult has been finding out most people's parents largely did not teach them how to notice and experience sensory information, think about stuff, or how to remember things (i dont mean in an executive function/recall sense, i mean in a "remembering a life event or experience in a narrative way that provides fodder for contemplation, i guess, at the risk of sounding like a complete prat), and especially not how to think about media, and by this i mean metacognition skills. thinking about thinking about. synthesizing information. and that stuff is where most of the abstract thought skills come from. its also where you get your ability to be aware you are even (for example) thinking about a smell in the first place. of course you can think about smells. if you can walk past a cinnabon and have some sort of reaction, even if its just "thats familiar to me", the pattern of the cinnabon smell exists in your brain in a way you can access. maybe you cant access it on purpose very well, but it exists and you were able to form the memory, which is what "imagining" things is. its a type of memory, not an eidetic type usually but a synthesized type from many different discrete experiences.
there are people who cant do that. they usually have brain damage to specific areas. if you really couldnt imagine what a crosswalk looks like, as many people who believe they are aphantasic believe about themselves, they would hit people with their cars constantly and wouldnt be able to identify their friends and family in photographs. people with that type of brain damage do have that latter problem, although the "face blindness" issue is complicated by, for example, the tendency of a lot of people not to look at faces in the first place, which is the current strongest theory about why autistics are seemingly "faceblind" despite having uncanny pattern recognition and visual acuity in all other areas--it's theorized by some researches that its the acuity thats making autistic kids avoid looking at faces in the first place, because its too much information literally, and it "hurts".
i cant recognize visual influences in art and think about them while im on the toilet because i was synthesized in a vat in the lourve, i can do it because a series of adults painstakingly and boringly taught me how to do it over the course of decades. and more importantly they taught me that i was already doing it and wasnt aware of it. now im too aware of it and all it got me is being annoyed that other people arent aware of doing it. so it goes. the other half of it is the difficulty in using spoken language to describe sensory experiences, im pretty sure most of you can imagine food just fine but are significantly less skilled at explaining what that food is like or what the process of imagining the food or smell or image is like, even to yourself, so you assume you arent doing it at all.
125 notes
·
View notes
Text
I find it really interesting how the way I explain my thinking often sounds so much like a plural system that I often get responses from members of plural systems either assuming that I mean it literally and relating to it, or just saying certain things I posted remind them of things that happen between them and their headmates.
I’ve realized that the reason I think like this is largely because of AuDHD. ADHD working memory challenges and difficulties with interoception (from both ADHD and Autism) mean I end up noticing many fleeting thoughts and feelings without fully connecting with them.
I end up observing these thoughts and feelings from an outside perspective, knowing they are mine, but not feeling the source of them, if that makes sense, so I see these thoughts not as another person in my head but just like things in my head, and that’s where autistic object personification comes in.
So I personify these thoughts and feelings in my head to some degree, and that means when I go to explain them, I describe them in a personified way. And when I describe the sensation to others, I often put even the nonverbal thoughts into words, with a tone of voice and things like that, in an attempt to convey the vibe that thought had.
And the end result is that it sounds like I’m talking about headmates when I’m not. And like sometimes I do actually “hear” the thoughts as voices in my head, but they feel like me subvocalizing, just different disconnected parts of me subvocalizing many very different things in quick succession, especially when I’m quickly trying to think of a response to something.
And it helps that on top of that, transitioning threw me into a state of wondering what my identity really is, and challenging prior assumptions about how things made me feel that might have actually been fear of being “found out”. So there has been the occasional discussion of identity, and it’s hard not to, to some degree, personify these versions of myself when there’s literally a name (deadname) for the pre-transition me, and a name (first new name I tried) for the version of me during my first realization I was trans, and a name (first new name I tried while transitioning) for my extremely baby trans phase, and a name (Sabrina) for me now.
And I do things like have multiple side blogs that blur the line between RP and being some filtered version of myself, where I do really “try on” different personalities.
And I often personify ADHD and Autism, and talk about them like they are distinct entities in my head even when they are clearly intertwined and all-encompassing. And I separate things like my role self vs my true self, my brain vs me (whatever that means), the versions of myself I am around different people, taking off one “hat” and putting on another, and I’m sure many other things.
And sometimes it does feel like “Who made that decision? I wouldn’t do that.” But it’s always like “Wow I know that’s how I felt and was thinking at the time but why would i do that, I’m not like that usually and I wouldn’t do that now,” and not, like, a headmate did that.
But I definitely see it not like I’m in a plural system, and not like I’m externally/logically applying a model of multiple people to explain something, but more like that is the model under which I naturally understand my brain, if that makes sense.
But yeah, plural folks feel free to relate to things I say if you relate to things, and feel free to share your similar experiences, I love hearing them. And if anyone knows more about this sort of stuff and wants to armchair psychoanalyze this post, feel free, I’m always open to looking into new things about myself and exploring them in therapy if needed. ☺️
#audhd#autism#adhd#neurodivergent#transgender#trans#plurality#sabrina is working on herself#sabrina says
12 notes
·
View notes
Text
Text:
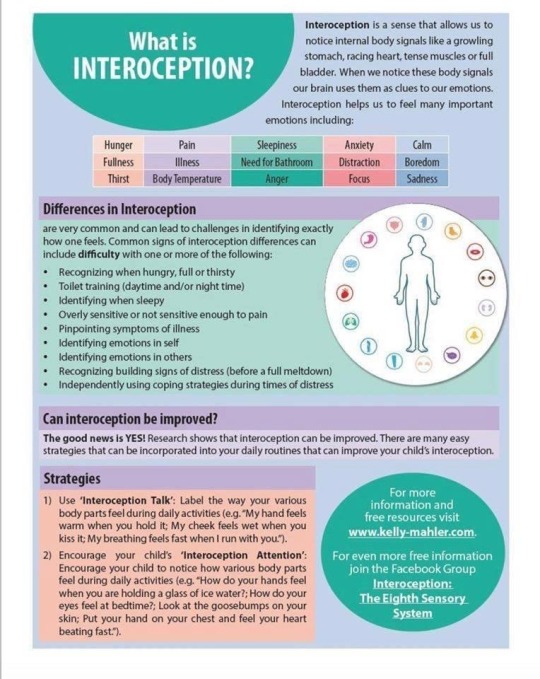
What is interoception?
Interoception is the sense that allows us to notice internal body signals like a growling stomach, racing heart, tense muscles or full bladder. When we notice these body signals our brain uses them as clues to our emotions. Interoception helps us feel many important emotions including: hunger, fullness, thirst, pain, illness, body temperature, sleepiness, need for bathroom, anger, anxiety, distraction, focus, calm, boredom, sadness.
Differences in interoception are very common and can lead to challenges in identifying exactly how one feels. Common signs of interoception differences can include difficulty with one or more of the following: recognizing when hungry, full or thirsty; toilet training (daytime and/or night time); identifying when sleepy; overly sensitive or not sensitive enough to pain; pinpointing symptoms of illness; identifying emotions in self; identifying emotions in others; recognizing building signs of distress (before a meltdown); independently using coping strategies during times of distress.
Can interoception be improved?
The good news is YES! Research shows that interoception can be improved. There are many easy strategies that can be incorporated into your daily routines that can improve your child's interoception.
Strategies:
(1) Use 'Interoception talk': Label the way your various body parts feel during daily activities (e.g. 'My hand feels warm when you hold it. My cheek feels wet when you kiss it. My breathing feels fast when I run with you.')
(2) Encourage your child's 'Interoception Attention': Encourage your child to notice how various body parts feel during daily activities (e.g. 'How do your hands feel when you are holding a glass of ice water? How do your eyes feel at bedtime? Look at the goosebumps on your skin. Put your hand on your chest and feel your heart beating fast.')
A free, downloadable version of this infographic and other resources can be found here: www.kelly-mahler.com/printable-resources/
Source will be below
I CAN Network Ltd
#interoception#interception explained#physical health#feel free to reblog/share#source: i can network ltd (facebook)
106 notes
·
View notes
Text
Mentioned this to a friend the other day but in the landscape of "your godly parent makes you more susceptible to developing X disorder, or, at the very least, significant traits of it", I was looking at OCPD and the Zeus/Jupiter kids.
"Obsessive-Compulsive Personality Disorder is characterised by a pervasive preoccupation with orderliness, perfectionism, and control (with no room for flexibility) that ultimately slows or interferes with completing a task. Patients with OCPD need to be in control, this, they tend to be solitary in their endeavours and to mistrust the help of others."
This fits the aspect of Zeus/Jupiter being the god of law and order. According to the DSM-5, OCPD is determined through a persistent pattern of preoccupation with order, perfectionism, and control of self, others and situations. This pattern is show by at least 4 or more of the following:
Preoccupation with details rules, schedules, organization, and lists
A striving to do something perfectly that interfere with completion of the task
Excessive devotion to work and productivity (not due to financial necessity), resulting in neglect of leisure activities and relationships
Excessive conscientiousness, fastidiousness, and inflexibility regarding ethical and moral issues and values
Unwillingness to throw out worn-out or worthless objects, even those with little to no sentimental value
Reluctance to delegate or work with other people unless those people agree to do things exactly as the patient wants
A miserly approach to spending for themselves and others because they see money as something to be he saved for future disasters
Rigidity and stubbornness
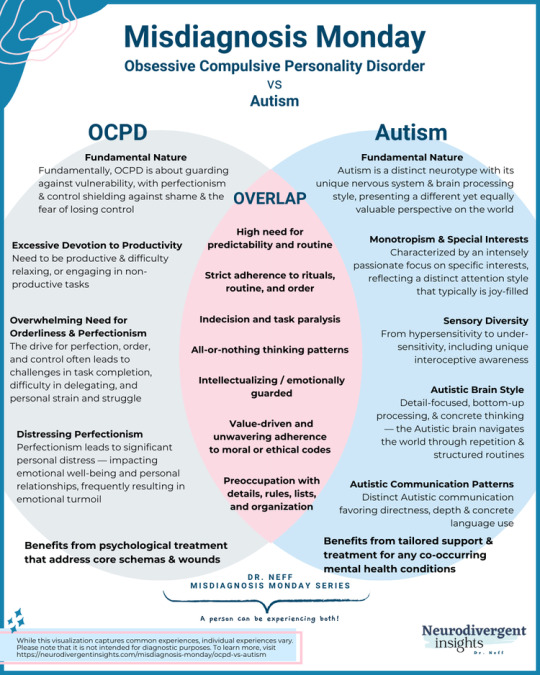
There's also a good deal of traits that overlap with Autism as well - which I HC Jason to have. See the Venn diagram below:
Read the full article here.
[ID: A Venn diagram showing the differences and overlap between Obsessive-Compulsive Personality Disorder and Autism. It is titled Misdiagnosis Monday.
The section relating only to the symptoms of OCPD lists:
Fundamental Nature: Fundamentally, OCPD is about guarding against vulnerability, with perfectionism and control shielding against shame and the fear of losing control
Excessive Devotion to Productivity: Need to be productive and difficulty relaxing or engaging in unproductive tasks
Overwhelming Need for Orderliness and Perfectionism: The drive for perfection, order, and control often leads to challenges in task completion, difficulty in delegating, and personal strain and struggle
Distressing Perfectionism: Perfectionism leads to significant personal distress - impacting emotional well-being and personal relationships, frequently resulting in emotional turmoil
Benefits from psychological treatment that address core schemas and wounds
The section relating to symptoms that overlap between OCPD and Autism lists:
High need for predictability and routine
Strict adherence to rituals, routine, and order
Indecision and task paralysis
All-or-nothing thinking patterns
Intellectualizing/emotionally guarded
Value-driven and unwavering adherence to moral or ethical codes
Preoccupation with details, rules, lists, and organization
The section relating only to the symptoms of Autism lists:
Fundamental Nature: Autism is a distinct neurotype with its unique nervous serious and brain processing style, presenting a different yet equally valuable perspective on the world
Monotropism and Special Interests: Characterized by an intensely passionate focus on specific interests, reflecting a distinct attention style that typically is joy-filled
Sensory Diversity: From hypersensitivity to under-sensitivity, including unique interoceptive awareness
Autistic Brain Style: Detail-focused, bottom-up processing, and concrete thinking - the autistic Brain navigates the world throw the repetition and structured routines
Autistic Communication Patterns: Distinct Autistic communication favouring directness, depth, and concrete language use
Benefits from tailored support and treatment for any co-occurring mental health conditions
/end ID]
The fear of losing control is something I relate to with Zeus/Jupiter. I imagine he's very paranoid about being overthrown, and gets easily stressed out when other people try to take over a situation. It might be weird to consider him as an anxious person, but, you know, what other kind of person would eat a woman because a prophecy said she would give birth to a son that would overthrow him. 🤷♂️
Also, personally when I think of the Big Six's childhood and the Titan war, I imagine him as having very specific ideas of his siblings before they were thrown up. The fact that they ended up being very little like his imagination and don't respect him as their future king furthers this stress and anxiety, since, as the older siblings, they do have more of a claim to the throne he was promised in return for defeating their father.
(I've written about this a bit before, check out the "happy talks greek mythos" tag if you wanna look)
OCPD is a cluster C diagnosis. Cluster C personality disorders are labelled as anxious and fearful. Similarly OCD a specific type of anxiety disorder. I think a lot of people conflate the two by accident. A lot of depictions or jokes about OCD relate to the perfectionism and needing things to be orderly which is more of an OCPD thing.
The IOCDF has a fact sheet on OCPD you can review for further information on the differences between the two. Click the related disorders tab to locate the pdf.
OCPD also differs from OCD in that people with OCD have a self-awareness. They know their thoughts are unreasonable, irrational, and/or unwanted, where people with OCPD typically believe their way is the right (and only) way, and do not respond well when people don't adhere to their self-imposed system of rules. Which, again, befits my headcanon that children of Zeus/Jupiter develop various rules and/or routines for how the world (should) work and struggle with not inflicting "justice" on people who break those rules, no matter how minor.
For example, I headcanon Zeus to have a thing about cups. Different types have different purposes. Don't use a wine glass for water, etc, etc. To any other person, it would be a "kinda weird but whatever" if you passed them a wine glass filled with ice tea, but he'd freak the fuck out because that's not what it's for! And then, depending on his mood, either lecture you about it or kill you.
(Fun fact: In the early stages of the whole Titan War, let's try to kill our dad and other relatives thing, Hestia tried pottery during some rare downtime and made everyone a cup! They had no handles and were improperly made because she spent most of her life in a stomach. Zeus gritted his teeth and said, "Thank you, I love it" while internally his brain was on fire, and he wanted to strangle her and break everyone's cups, because it's not a fucking cup. He loves her so much, everyone's favourite sister and all, but dear stars above, he wanted to kill her so bad for this major infraction)
So, lol, yeah. I think Zeus has a lot of neurotic tendencies that he passes down to his kids. There's also the whole "you're a child of Zeus/Jupiter, you're the leader now" thing that demands them to be perfect beyond reason, which could propel the development of OCPD, or some of its traits.
I also HC that one of the powers the kids may have is the ability to force people to follow/believe in the same system of rules that they do. Helpful in battle when you're faced against more enemies than you can handle. Less helpful when it's just you and your buddies and you think them drinking iced tea out of wine glass is incorrect and despicable.
Anyway, these days I'm kicking my legs up over personality disorders, lol, but hey, if anyone has any disorders, personality or not, they think may fit a specific set of demigods, hit me up! I'd love to look into it. So far I have:
Neptune = Schizoid Personality Disorder (based on the idea that PJO's Neptune represents the emotionless and uncaring sea);
Poseidon = Borderline Personality Disorder (based on the idea that PJO's Poseidon represents the emotional and volatile sea);
Ares = Intermittent Explosive Disorder (haven't discussed it before but if you look into it, it's fairly self-explanatory - does not necessarily apply to children of Mars as Mars is more disciplined than Ares, though I think both sets of kids likely have a high propensity for anger issues);
Zeus/Jupiter = OCPD (as discussed above) and Autism (mostly because of my Jason is autistic HC, which I'm sure I've discussed it in some detail before as well)
#happy talks pjo#obsessive compulsive personality disorder#ocpd#jason grace#zeus (pjo)#also if you have ocpd and like pjo feel free to hmu if you have thoughts on what ive written 👍 would be happy to hear your ideas#happy rambles about mental health
31 notes
·
View notes
Text
Regulating Emotions with Hypnosis
I've finished up the section on emotions. This was much more work than I expected, because I wanted to talk about regulation.
Emotional regulation is one of those concepts that therapists and psychologists are very familiar with, but which means very little to the general public. Regulation is the balancing of emotions that virtually all adults do.
It's the emotional work that you do to not yell at someone when you're angry, not cry when you're sad, and support your friend when they're down. It's support, it's distraction, it's suppression, it's reappraisal, it's playing computer games, or even going out and drinking. There are many emotional regulation strategies, and none of them are objectively good or bad, but usually we do need to pick something. Otherwise we just have emotions turning into unproductive actions, and that's no good for anyone.
There is a taboo in recreational/erotic hypnosis that you aren't suppose to use hypnosis as therapy, and should leave that up to the professionals. I think that's fair.
I also think that hypnosis is one regulation strategy out of many, and regulation is a human activity. Regulation is comforting. If your partner trusts you and wants to be comforted with hypnosis, then you should comfort them with hypnosis.
I will also admit there are parts that I just couldn't bring myself to write. Discussing sadness or horror is one thing, but discussing how you can regulate it through hypnosis is beyond me. I'm not saying you should leave it for therapists, or you shouldn't do it. But I don't know of a way that I can talk about it. So I'm just going to not.
There are more bits about emotions that I find really interesting but don't really work in the guide. The chain of connection between interoception and emotion is fascinating, as is the concept of emotions as a "perception of self" and how it plays into decision making. Did you know that people who have brain damage which reduces their ability to feel emotions have difficulty making decisions? And how much of our decision making ability is purely unconscious? Emotions are really the original thoughts and sentience of the brain, and what we think of as "thoughts" are just a thin editorial layer pasted on top of that.
Anyway. Next section is on mental perceptions, aka beliefs. That's going to be a fun one.
8 notes
·
View notes
Text
Acknowledging my daily pain is not taking anything away from people whose chronic pain is worse than mine. I'm allowed to be distressed by my body hurting every single day for as long as I can remember.
I don't have to be a "warrior". That should not be expected of me.
I am allowed to be tired out and overwhelmed by pain that I could tolerate the day before.
My understanding of my pain is influenced by my difficulties with interoception. It is okay that I can't always define the pain itself, only how it affects me.
Not knowing the cause of my pain is valid, and it is reasonable for me to be concerned about it.
I may never make peace with my chronic pain, there are always new ways it can manifest that frighten me and interfere with my functioning. It's not going to ever stop, and I'm allowed to be upset by that.
#affirmations#moss-opossum#disability#disabled#chronically ill#chronic illness#physically disabled#chronic pain i guess?#chronic health issues#chronic pain#multiply disabled
28 notes
·
View notes
Note
But for us, growing up in the 90s, unless you had severe deficits or learning disabilities, you were seen as "odd" , "quirky" or "naughty" and so go undiagnosed.
How do we know that you not just „odd“ but that you are neurodivergent? Like how can you distinguish this? Can you be misdiagnosed and would that be harmful because of no treatment? If so many people are undiagnosed could that be the reason why we have so many arseholes running around? Bad joke here, obviously I‘m not saying you’re an asshole when you have an undiagnosed or diagnosed illness. Also if these questions are in anyway hurtful please tell me. I‘m sorry but I find this incredibly interesting.
I don't take offence as I can tell you genuinely want to understand
"Treatment" is a misnomer, particularly with autism. Autism is a neurological disability z a neurological difference. You don't have medication for it (melatonin for sleep maybe but that's not really medication). Autism is something you support - allow stimming, adapt preferences of food and textures of clothes, provide sensory aids (ear defenders, sensory objects, things to stim with)
Don't get me wrong, there are various degrees to how severely autism affects a person, it is a wiiiiiiiide spectrum. My sons, 7, has selective mutism and food aversions whereas my son, 5, is hyperverbal and has no aversions whatsoever and in fact seeks out lots of flavours and textures for oral stimulation.
Autism isn't an illness. You don't "suffer" with it, especially if you're not severely affected by what comes along with autism. There are those who have severe behavioural challenges, may not be verbal, may never learn interoceptive skills and so remain incontinent, or never be able to understand if they're unwell, or hurt, or in pain.
There is a lot of factors, and a lot to learn and understand.
Each autistic person is very different and all experience autism differently. Many, many people with autism lead a typical life but perhaps may experience more deep emotions, or meltdowns, or social communication difficulties but appear otherwise very typical. Other individuals need support for their whole lives.
Forgive typos, I don't have my glasses on.
2 notes
·
View notes
Text
CH! Frida Kahlo Headcanon(s)
As much as I love Frida, I feel like she deserves to have some personality, character, and other stuff about her other than being “the laidback voice of reason”. So here we are:
Frida has confrontational issues. Because of how chilled and laidback she is, she would rather leave or wait things out rather than be direct and confront the problem(s)/conflict(s). She doesn’t take fighting nor arguing very well—thus becoming more passive and dismissive.
They struggle with chronic pain in their legs, mainly in their right leg. Due to their clone mother getting polio at a young age and suffering chronic pain in their leg as a result, Frida ends up inheriting that chronic pain (maybe also suffering from polio at the same age as well?) and thus struggles with it. Winters and cold weather is the worst.
On those occasions where Frida’s leg is in extreme amount of pain, he uses a cane.
Has Alexithymia. Pups cool and laidback attitude is partially due to pups difficulty identifying pups emotions and issues related to interoception. Sometimes either forgets of doesn’t realize pup’s hungry, tired, dehydrated, stressed, etc—hence pup carefreeness. This is a more personal HC as I have this as well, and so I feel she has it too.
While we’re at it, Frida also has ADHD and even experiences autistic traits. They tends to hyper focus HARD on painting murals and getting certain art pieces done. Simultaneously, they also had alot of unfinished works that are lying around their room. Even murals. They also tends to listen more than speak, preferring to be able to consider what they has to say. Uses advice they had learned from others and giving it on. Yet, there are times where they acts out impulsive whenever nervous or excited (i.e. when they crushed on Cleo).
Has sleeping issues related to her ADHD and is the type to sleep at 4 am. Tends to either pace around, paint, or rant to herself or Harriet early in the morning.
Has been masking for all his life and hasn’t realized this until he and Topher became friends. Topher pointed out that his disconnect to his identity and personality is most likely his masking.
OH and I decided—Frida has ✨identity issues✨ and internally struggles to see if pup really is the cool and go-with-the-flow type of person.
Is nonbinary, they/she & occasionally uses he/pup.
Is bisexual—has a preference for woman but occasionally had dated and crushes on men.
Has dated Diego Rivera’s clone son. Didn’t go so well…
Becomes friends with Topher & besties too with Gandhi (ADHD solidarity)
Wears a binder <33
Had a crush on Abe but never said anything about it—only reason they remained cool is because it wasn’t as big of a crush compared to Cleo.
And that’s about it for now!
#ch#clone high#clone high season two#clone high season 2#clone high reboot#clone high frida#frida clone high#frida kahlo#frida#clone high headcanons
33 notes
·
View notes
Text
Level 1 RRBs can look like (for me)-
Eating the same foods every day and been doing so for years.
Certain foods can only be eaten at certain times.
Having rituals for eating in which certain foods NEED to be eaten the same way EVERYTIME. Certain foods NEED to be placed a certain way.
Severe sensory issues with foods that largely restrict your diet.
Rituals/rules that restrict how foods are prepared or whether they can be consumed.
Having a consistant daily routine. In which doing the same things on a daily basis at roughly the same times everyday. Been doing so for years.
Adverse reactions to routines being changed.
Having meltdowns/shutdowns when plans are cancelled and not being able to recover in a decent timeframe.
Not understanding and reacting poorly to a new plan being made.
A need to take the same route to places even if only around your home.
Difficulties in transitioning between tasks.
Negative reactions and distress at needing to do multiple things at a time.
Big distress at items/objects being moved that hadn't been moved previously.
Distress and sometimes meltdowns/shutdowns at being made to participate in new systems/ways of doing things.
Difficulties transitioning and using new items.
Sometimes taking weeks or months to use a new item even if excited for it.
Rituals in bedtime/morning routine, getting dressed, doing certain chores, that result in distress if even the slightest part of it is done differently.
Having a specifc spot that you sit whether in the car, dining table, loungeroom, that causes distress if you can not sit there.
Needing to use specific tools/items and not being able to use anything else.
Stimming in some form or another for hours+ in your day.
Maladaptive daydreaming as a form of stimming which has become an addiction and I can not go a day without doing it. Can last hours when started.
Strong attachment to certain items that cause extreme distress if item is messed with.
Tensing muscles in and around ears to cope with noises.
Struggles with temperature regulation.
Poor interoception when it comes to eating, temperature and drinking.
Tuning out noises, sights, people, when focused on tasks even if task is small.
There's probably a lot more I'm missing. But hey, I can look after my personal hygiene, I can get myself meals even if simple and eat by myself and for myself. I can do basic tasks to a degree.
I wanted to post this just to show what Level 1 RRBs can look like.
I still need support.
15 notes
·
View notes
Text
The dilemma is that I do need to exercise sometimes in order to not feel like shit. But I'm also bad at feeding myself under the best of circumstances (various reasons incl interoception issues/prep + planning difficulties/getting bored when the eating takes too long or becomes Too Texture/etc). So any rare Real Exercise session I manage is a recipe for debilitating hunger afterwards
#tbt when i took a weightlifting class for a semester (out of pre t cope)#and we did an assignment where we were supposed to track our calorie intake for a week (to make sure we were getting enough#to support the weightlifting)#and i stared at the results like 'hm. perhaps this explains the public crying breakdowns of late.'
8 notes
·
View notes
Text

Katy Higgins Lee, MFT tending paths
(Overlapping areas are shared traits)
Autism: Needing routine, order, and/or clear expectations (especially when under stress). Tendency to hyperfocus on a few interests for an extended period of time. Differences in verbal and non-verbal communication and interactions. Alexithymia (difficulty identifying and naming feelings). Hyper and/or hypo-awareness of sensory information. Tendency toward concrete thinking/difficulty with abstract thinking. Preference for direct communication. Pattern recognition. Soothed/stimulated through repetitive behaviors, movements, sounds, and thoughts ("Stims"). Motor skills impacted. Preference for interpersonal connection through interests.
Giftedness: Tendency toward abstract thinking. Rapid comprehension and/or "skip" thinking. Wide range of interests. Early emotional awareness. Fascination with theory. Awareness of and need for complexity. Needing interpersonal connection through shared interest in complexity. Needing intellectual stimulation/mental challenges. Tendency to predict consequences and foresee problems. Tendency to make connections across domains. Early concern for (and ongoing need to explore) existential issues.
ADHD: Difficulty with transitions due to challenges with switching focus. Social interactions affected by impulse control and focus differences. Working memory impacted. Tendency to hyper-focus on a wide range of interests. Needing movement or fidgeting/stimming to aid in focus. Ability to respond quickly in crisis situations/emergencies. Differences in regulating attention (hyper-focus when interested and difficulty focusing when not interested). Craving novelty.
Autism/Giftedness: Ability to notice details. Preference for logic and fairness. Thinking in systems. Highly developed morals. Preference for precision in expression. Needing time spent in solitude/contemplation.
Giftedness/ADHD: Easily bored. Thinking in metaphor and symbol. Learning in a non-linear manner.
Autism/ADHD: Stimming. Differences in impulse control. Different perception of time. Atypical social interactions. Hyperactivity (physical and/or mental). Processing speed impacted. Interoception differences.
Autism/Giftedness/ADHD: Emotional sensitivity. Interest-driven. Asynchronous development. Divergent/creative thinking. Executive function difficulties. Intense curiosity. Unique ways of learning. Sensory differences.
5 notes
·
View notes
Text
YOUR JOURNEY WITH AUTISM
(Learning about yourself to get the support that you need)
- Diagnosis
- Searching what your sensory issues are and taking action to get accomodations your sensory needs (note : sensory can also be about differences such as synaesthesia)
(a list of senses (hypersensitivity/hyposensitivity) :
auditory (noises are overwhelming, you have trouble talking to other people because background noises distract and overwhelm you (you need things to be repeated because you got distracted by background noises), loud, repetitive and sudden noises overwhelm you, you hate eating certain foods and doing certain things because they make a lot of noise, focusing is hard because background noises overwhelm and distract you, you can’t go outside because noise is overwhelming, you place your hands over your ears when noises are overwhelming, you set your phone at a very low volume/you seek loud noises, you set your phone at a high volume, you often don’t respond to your name being called because you don’t hear it, you often need things to be repeated, you’re unable to locate where sounds come from),
smell (smells are overwhelming, you can’t eat certain foods because their scent is overwhelming, you’re super hygienic because you’re worried about smelling bad and you smell strongly your bodily smell, others don’t smell as much your bodily smell as you, you hate the smell of laundry detergent on your clothes/you seek smells, you like eating foods with strong scents, you’re unaware of smells other smell, you may not have a strong preference for foods other commonly enjoy (smell affects taste)),
gustative and texture (you are a very picky eater and rely on eating the same meal a lot of the time, you refuse to eat new food/you eat things with a strong taste, you explored objects with your mouth a lot as a child (even after being a toddler), you aren’t aware of food quantity and temperature, you bite your tongue and your lips more frequently than other people)
touch (your wardrobe is very limited, you wear a lot of the time the same thing, you avoid touching a lot of things and hate physical touch, you have a low pain tolerance/you tend to get injured without noticing, you didn’t noticed when you were covered in mud when you were playing as a child, you’re unaware of your own strength, you seek touch, you have a hard time telling someone where you feel pain and where you got injured, you have a high pain tolerance )),
vision (lights, the sun are overwhelming, you avoid eye contact (eye contact issues isn’t specific to visual hypersensitivity, lots of autistic have issues with eye contact regardless of if they have this), you squint, you often close your curtains and dim the light, you can’t go outside because you get sensory overload from the light/you get accidentally injured easily because you didn’t see something, you often bump into other people and objects, you can’t find or see things that are seen by other people, you stare at lights, you like colorful and high contrast things, you often watch others)
proprioception (sitting in a non-conventional way, fine motor skills issues, uncoordinated, hypersensitive to pain, appearing stiff, holding your body in positions that are considered odd, appearing lethargic, becoming tired after standing for a long time, hating and avoiding being touched, avoiding wearing tight clothing, avoiding activities that require physical effort/ bumping and stumbing a lot upon things, difficulty doing things that involve balance such as riding a bike, often leaning against a wall or furniture, holding objects with a weak grasp and letting them go, sitting on the floor in a W stance, difficulty navigating a room and avoiding objects, you can’t grasp what personal space is, tip toe walking, pressing too hard on furniture, pushing or playing roughly, walking very loudly, constantly being in movement)
interoception (feeling overwhelmed by physical sensations, thirst, hunger, exhaustion, need to go to the bathroom and by your feelings/having trouble feeling your physical sensations, forgetting your physical needs and having trouble knowing what you’re feeling)),
vestibular (easily motion-sick, fear of heights, dislike many sports/easily lose balance, accidentally injure themself often, able to spin for a long time without getting dizzy, risk taker)
This list isn’t exhaustive
- Looking at, understanding your communication differences and the neurotypical social cues
- Searching what your special interests are
- Observing yourself a lot to learn what your stims are and how to replace your harmful ones
- understanding your hatred of change (might be/not be/both be the case if you have ADHD diagnosed or not as well)
- realizing you experienced meltdowns and shutdowns (you can be autistic and not have meltdowns and shutdowns, if you wondered)
- learning, reading about autism, autistic experiences and the autistic community
This list doesn’t have a particular order
I’m myself on this journey currently (I honestly do not know if I’m autistic even if I got diagnosed ten years ago when I was a child), currently it’s the stimming part for me, turns out stim toys might actually be helpful for me !
This journey is about discovering, accomodating and enjoying yourself. You can experience every feeling through this journey :
anger, sadness, fear, joy, confusion, surprise, joy.
I personnally experienced confusion and anger a lot because I didn’t understood my diagnosis as I didn’t related to most autistic experiences, I now go through surprise a lot when I realize that I actually experience some autistic traits that fall under the spectrum umbrella.
I don’t want this post to give an impression that autistic people don’t really have autism, my case is very rare and specific among the spectrum : I didn’t got socially ostracized and knew a lot of social cues (yet I also had issues with some), I also don’t have sensory issues or a need for routine.
Yet, to neurotypical people I have a few differences :
communication and social cues ones, stimming a lot, special interests, a bit impaired fine motor skills (nothing too serious).
If I’m truly autistic, this is a prime example on how the autism spectrum is very wide :
If you’ve met an autistic person, you’ve met one type of autism, there are infinite types of autism.
A few more important things :
- some common disabilities that comes with autism :
ADHD (about 50 percent or so of us also have it),
learning disabilities (dyspraxia might be the most common one),
insomnia (sensory issues),
depression,
anxiety,
social anxiety,
personality disorders,
PTSD,
CPTSD (trauma and living in a society that doesn’t accomodate to our needs and where you get ostracized (be careful borderline personality disorder is a common misdiagnosis, though you can also get both BPD and autism),
SPD/allodynia,
OCD,
Ehler Danlos Syndrome (a skin collagene muscle issue, don’t ask me about this I don’t know a lot about it),
ID (though not all of us, treat autistic people kindly without expecting them to have ID if you meet them the first time please),
hypersomnia,
epilepsy (epileptic people should be treated normally, yes epilepsy can cause you other issues by brain damages but lots of epileptic people still don’t have ID, though ID and other disabilities shouldn’t be an excuse for you to treat anyone badly),
speech issues (what I said about ID still stands here, we can get them temporarily through shutdowns and meltdowns),
migraines (sensory issues)
- motor issues even small ones are common within the spectrum
- face blindness is also common
- milestones delays are common
- executive dysfunction is common
- autistic catatonia is rare but is a thing
- we can get any physical or mental disability through our life just like anybody else
- some accomodations you can look/ask for :
noise-cancelling headphones/earplugs,
wearing specific types of clothes,
eating food that doesn’t cause you sensory overload,
sunglasses,
non slip shoes,
white noises,
having someone check on you to make sure you don’t get injured without noticing or simply to take care of yourself,
asking to not be touch (you will have to learn especially how to enforce your boundaries as a disabled person),
visual accomodations (some of us are very visual and might appreciate having schemes to understand things),
AAC,
sign language,
someone that lives with you and do things for you,
weightened blanket (some of us like and need deep pressure),
hammock swing/trampoline,
stim toys (hyposensitivity makes you stim a lot but hypersensitive autistics also stim a lot since stimming help them to cope with their sensory issues),
sunflower landyards,
your own communication means,
medication (autism can’t be treated, unlike ADHD but it can reduces your anxiety, your agressivity if you get meltdowns and treat mental issues if you have some, it can help you if you struggle with regulating your emotions I think but I’m not sure though, you should reach your psychiatrist before considering taking it),
therapies (occupational therapy might be a good one, idk a lot about it though, ABA should be avoided)
reminders for physical needs, school and work accomodations
A thing everyone should know :
for every autistic trait experienced by an autistic person, there is another autistic person that don’t experience it. My point still stands for other disabilities. Everyone should listen to autistic persons first. I made this post on a consequent amount of knowledge through months of research on autism on the internet, since autism was my special interest.
Edit :
you should also go out of your way to research autism by listening to the autistic community, there are many many traits that I didn’t listed on this list that we experience and that autistics can relate to.
You can have hyposensitivity and not be sensory seeking. You can have hypersensitivity and not try to avoid sensory input (I’m not saying this is something you should do, I’m saying some autistic person are like that).
Added vestibular and vision senses because I forgot and it is important.
Also added more accomodations, same motive as before.
Added more precision to senses and a few disabilities autistic people often experience, for the same reason as above.
12 notes
·
View notes