#paranoid pd
Text
Non-cluster A people, y’all need to start recognizing that our PDs don’t make us “crazy”.
Schizoids? Their indifference and disinterest doesn’t make them crazy, nor does their flattened affect or lack of pleasure. Just because them not wanting to do something that doesn’t bring them joy for you doesn’t make them bad people or “weirdos”.
Schizotypals? Their unusual thoughts and mannerisms doesn’t make them crazy, nor does their lack of close confidants or general fear. Them doing what they feel is right is normal. Your beliefs are your realities, so don’t try and make schizotypals out to be the bad guys because theirs are odd compared to others.
Paranoids? Our mistrust doesn’t mean we’re crazy, nor does our self-preservation or self-defense. If the world was out to get you, you would be on edge too. Stop calling us burdensome because we have a normal human response to something thats abnormal to the average person.
Being schizoid doesn’t make you crazy. Being schizotypal doesn’t make you crazy. Being paranoid doesn’t make you crazy. Being cluster a doesn’t make you crazy. Being schizospec doesn’t make you crazy. We are not crazy.
#cluster a#personality disorder#ppd#szpd#stpd#actually ppd#schizoid#schizotypal#paranoid#paranoid personality disorder#schizoid personality disorder#schizotypal personality disorder#paranoid pd#schizoid pd#schizotypal pd#actually cluster a#cluster a awareness#schizo spectrum#actually schizospec
711 notes
·
View notes
Note
cluster a culture is never being taken seriously for fighting against and criticizing things like “if you don’t reblog this you’re part of the problem” “everybody has to reblog this” “_____ people will NEVER reblog this”. People act like it’s just some annoying thing, and not something that could be horribly debilitating to schizospec people
FOR REAL I hate reblog baits so much. people don't seem to get that it could trigger a psychotic episode in schizospecs, inducing delusions and derealisation is Not Cool.
160 notes
·
View notes
Text
I just realized that cats are the literal embodiment of all personality disorders (which is probably why they're so amazing!):
PPD: suspicious of change
SZPD: loners & content to just chill in the same room as you for "socializing"
STPD: odd behavior
ASPD: easily annoyed
BPD: mood swings
HPD: needs attention 24/7
NPD: obviously superior
AVPD: skittish & anxious
DPD: "don't ever go away overnight ever again!"
OCPD: rigidity & stubbornness
Feel free to add more ways in which cats embody PDs!
@pd-culture-is for when they come off hiatus :)
#just for fun#cats!#cats#kitties#positivity#positivity post#pd#personality disorder#pd positivity#cluster a#cluster a personality disorders#cluster a pd#cluster a positivity#ppd#paranoid#paranoid pd#paranoid personality disorder#szpd#schizoid#schizoid pd#schizoid personality disorder#stpd#schizotypal#schizotypal pd#schizotypal personality disorder#cluster b#cluster b personality disorders#cluster b pd#cluster b positivity#aspd
96 notes
·
View notes
Text

disabled adults who need one or more carers are not "adult children" we are adults. if you're determined to reduce us to our support needs, the legal term is 'dependant adult', you condescending pieces of shit.
#personcole#ppd#paranoid pd#actually ppd#actually paranoid#paranoid personality disorder#i feel like stealing kneecaps#dependent adults#actually disabled#disabled adults
131 notes
·
View notes
Text
I wish talking to people wasn’t so fucking terrifying lmfao
#selfposts#ppd#paranoid personality disorder#social anxiety#ptsd#paranoid pd#actually paranoid#paranoia#this post is about fear of conflict
327 notes
·
View notes
Text
Custer A Flags remade
[cluster a flags remade]

post one(link) - cluster b(link) - cluster c(link)



Paranoid personality disorder
moth/butterfly used: lackey moth


schizoid personality disorder
moth/butterfly used: arctic blue butterfly

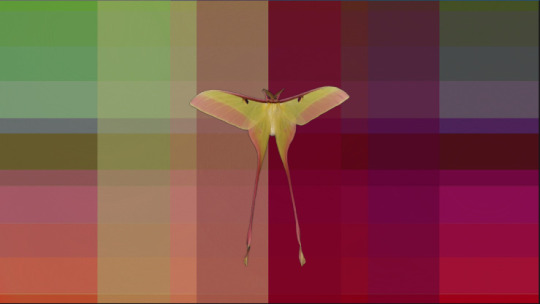
schizotypal personality disorder
moth/butterfly used: chinese luna moth
flags are exclusive to those with the disorders
apologies for the lack of ids due to a lack of spoons
radqueers, transx/id do not touch my flags thanks
tagging: @delightfulweepingwillows, @docsfallfromgrace, @acetrappolaswife, @clusterrune, @archival-arrival, @decayednightmaremogai

#cluster a#mod cass#flag design#flag blog#my flags#flag coining#flag making#flag designs#flag redesign#ppd flag#ppd#paranoid pd flag#paranoid pd#paranoid personality disorder flag#paranoid personality disorder#spd#stpd#stpd flag#szpd#szpd flag#schizoid personality disorder#schizoid#schizoid pd#cluster a pd#schizotypal#schizotypal pd#schizotypal personality disorder#flags#disorders#personality disorder
43 notes
·
View notes
Text
Pertaining to the self ship community I keep seeing posts about this so, yeah it's a community, but no one is obliged to like or interact with your posts, it doesn't matter if you don't get a single interaction, no one is obliged to interact with you just so you don't feel left out. People are allowed to stay in their bubble and in their comfort zone because guess what! they self ship for their enjoyment, not yours!
Not even need to mention how some neurodivergencies make you want to stay by yourself and how disrespectful trying to force those people to interact is!
Pro/com-shitters fuck off!
#endos fuck off#self ship#self ship community#self insert community#self shipping#selfship community#actually szpd#cluster a#cluster b#actually npd#actually aspd#actually schizoid#f/o community#fictional other#si x fo#f/o imagines#f/o x s/i#f/o stuff#self insert#safeshipping#oc x canon#f/o tag#imagine your f/o#selfshipper#self ship positivity#selfship#schizoid#schizotypal#avoidant pd#paranoid pd
31 notes
·
View notes
Note
When I was a kid and somebody wasn’t bowing down to me I thought that meant they were going to attack me. So, I would attack them. Hit, punch, strangle, tie up with a jump rope, etc…
I quickly realized I couldn’t do that and get away with it. Nowadays I just gaslight them into thinking they hurt me to guilt trip them. In my mind they’ve hurt me but not in a way that’s socially understandable, so I have to break it down for the fools. I sometimes trigger them on purpose and then act as though I didn’t know. Then I tell them that I’m sorry but I was “just feeling trapped/stuck because you (insert blame)”. I mean it in the moment but I also don’t? Anyways, then we make up and they apologize and don’t do it again.
I feel guilty in theory about this but I also don’t because they hurt me and I believe they deserve it. Again, it’s just not in the way I say it was because nobody understands it.
-A disingenuous histrionic and paranoid
.
#actually histrionic#cluster b#histrionic pd#histrionic personality disorder#honestly histrionic#hpd#actually mentally ill#paranoia#actually paranoid#paranoid pd#paranoid personality disorder#cluster a#dark and depraved confessions
7 notes
·
View notes
Text
Flag for Paranoid Personality Disorder (PPD)

[ID: A rectangle flag with seven stripes, the third and fifth being much thinner than the rest. The stripes go in the order of purple, blue, yellow, orange, yellow, blue, and purple. All colors are muted. End ID.]
-
This is just a flag for PPD, because all of the ones we saw were very heavily eyestrain, so we wanted to make one that wasn't as bad.
-
Yellow + Orange: paranoia symptoms
Blue: acceptance and awareness
Purple: the concept of having a trusted person/trusted people
#paranoid personality disorder flag#ppd#paranoid personality disorder#flag#mad pride#pd pride#Perseonality disorder pride#paranoid pd#blurred-pride coining
81 notes
·
View notes
Text
✨✨✨✨✨✨✨✨✨✨✨✨✨✨✨✨✨✨
22. He/Him & She/Her.
STPD. BPD. PPD. ASPD Traits.
Side blog. Main is @huecollective.
✨✨✨✨✨✨✨✨✨✨✨✨✨✨✨✨✨✨
#psychotic#psychosis#schizophrenia#schizospec#actually schizotypal#schizotypal personality disorder#schizotypal#actually bpd#bpd#ppd#ASPD#Stpd#actually borderline#borderline pd#schizotypal pd#actually paranoid#paranoid pd
2 notes
·
View notes
Text
IF YOU AREN’T PARANOID AND/OR CLUSTER A LISTEN TO THIS: STOP USING PARANOID AS AN INSULT/IN A NEGATIVE WAY!!!
I recently made a repost about this but as somebody with paranoid pd I find it highly stigmatizing and dehumanizing how others treat paranoid people.
I often seen “paranoid” as a means to describe a toxic person or somebody who’s “weird” and/or bad. A good chunk of the time they just straight up list PPD symptoms without saying paranoid either.
An example I saw one time was “POV: you have a paranoid mother”. It was just a video of a mother character displaying PPD symptoms, particularly the symptoms of believing close confidants are out to harm you, believing benign things to be threatening, and counterattacking these threats.
The video, instead of focusing on the behaviors of shaming a daughter for going to college and hitting the daughter, focused more on the paranoid symptoms.
This is so telling of how paranoid people are treated, yet many leave us and other cluster As out of pd stigma discussions. It’s honestly insulting how we are treated outside of and by our own community.
But yeah, that’s all I have to say for now. Thank you for reading, goodbye.
#paranoia#paranoid#ppd#paranoid pd#paranoid personality disorder#cluster a#personality disorder#actually paranoid#actually ppd#schizo spectrum#schizotypal#actually schizospec#schizoid#schizophrenic spectrum#schizoaffective
126 notes
·
View notes
Text
some comparisons between disorders and symptoms
we've been meaning to write this for a while now, because we often receive asks that are like "how do I know if I have a schizospec disorder or (another disorder)?"
so, here are breakdowns of symptoms that affect thoughts, some things we'll take from the EASE for more officiality and clarity
intrusive and impulsive thoughts
intrusive thoughts are by nature aggressive, horrid, macabre, and/or sexual.
they're different from impulsive thoughts. impulsive thoughts are silly, usually fun, are things that wouldn't bring too much harm on yourself or others if acted upon. things you would realistically do in the spur of the moment. they are purely caused by impulsivity.
examples of impulsive thoughts:
thoughts/imagery of breaking some object
thoughts/imagery of sneaking up on a person to give them a scare
thoughts/imagery of impulsive buying, spending, etc
examples of intrusive thoughts:
thoughts/imagery of blood, catastrophes, death, etc
thoughts/imagery of harming yourself/others
thoughts/imagery of sexual harassment, violence, etc
intrusive thoughts are unwanted, cause distress, are met with resistance, and often with attempts to push them away
impulsive thoughts aren't necessarily unwanted, cause minor distress or no distress at all, aren't met with much resistance
intrusive thoughts are a symptom of many, many, many mental health issues and illnesses. though, they also happen in healthy people, occasionally.
the keyword is: occasionally.
when intrusive thoughts become frequent and constant, they become obsessions.
obsessions
obsessions are, simply put, ongoing intrusive thoughts.
they are repetitive, they won't stop showing up no matter how much resistance or attempts to ignore them is shown, and are cause of great distress.
they are often met with attempts to push them away, which can too become frequent and become compulsions.
compulsions are often present with obsessions, but not always, and the reverse is also true. obsessions are often present with compulsions, but not always.
obsessions are the defining feature of OCspec disorders such as obsessive-compulsive disorder (both obsessive and obsessive-compulsive types, but not compulsive type) and body dysmorphic disorder.
ruminations
thoughts/imagery of any past event.
ruminations are frequent and ongoing as obsessions, but they're a bit different depending on the subtype of ruminations.
subtype 1:
the person is unable to find any reason for their tendency to obsessive-like states; they simply rethink and relive what happened during the day/past days – not motivated by perplexity, paranoid attitude, or sense of vulnerability or inferiority.
subtype 2
the obsessive-like states appear as a consequence of a loss of natural evidence, disturbed basic sense of the self, or hyperreflectivity, or they appear to be caused by more primary paranoid phenomena (suspiciousness, self-reference, etc) or a depressive state.
subtype 3
ego-dystonic, as in obsessive-compulsive disorders, with ongoing internal resistance, but a content that is not aggressive, horrid, macabre, or sexual. they're also categorised as true obsessions, but can have a different content.
subtype 4
obsession-like phenomena, which appear more as ego-syntonic (not met with resistance, or only occasionally), and with a content that is directly aggressive, sexually perverse, or otherwise bizarre. they often feature an imaginative character doing the actions, instead of the person who's experiencing the ruminations.
to make it clearer:
intrusive thoughts are unwanted, cause distress, are met with resistance, and often with attempts to push them away. they do not happen regularly, and often aren't a cause of concern, though they are distressing. everyone can experience intrusive thoughts, regardless of if they have a disorder or not.
obsessions are unwanted, cause distress, are met with resistance, and often with attempts to push them away. they happen regularly, often on a daily basis, and often are cause of concern. since they cause distress regularly, they're often basis for a diagnosis of obsessive-compulsive disorders. again, if they don't cause distress, they're not obsessions, they might be ruminations or impulsive thoughts, or something else entirely. they are often, but not always, met with compulsions, rituals, or attempts to ignore them to neutralise the obsession.
ruminations are varied. they all have in common that they happen regularly, often on a daily basis, and they're thoughts/imagery of past events. they can just be (subtype 1); they can be in response to depression, hyperreflectivity such as anxiety, paranoia, suspiciousness, etc (subtype 2); they can be bizarre, met with resistance and distressing as obsessions, but of a different content (subtype 3); they can be of the same content as obsessions, but without the same resistance and without being distressing (subtype 4). though, they can also be met with compulsions, rituals, or attempts to ignore them. they can happen in any disorder, but especially subtype 1 can... just happen, even in healthy people. subtypes 2-4 are frequent in schizospec disorders. subtype 2 is also frequent in other non-schizospec disorders such as anxiety, depression, etc.
#cluster a#stpd#schizotypal pd#szpd#schizoid pd#ppd#paranoid pd#schizospec#schizophrenia spectrum#ocd#obsessive compulsive disorder#body dysmorphic disorder#intrusive thoughts#obsessions#ruminations#long post
404 notes
·
View notes
Text
here's some positivity for paranoid people who actively struggle with not being "controlling" towards friends, partners and/or family out of a misplaced desire to protect them or yourself from harm.
you are not a bad person
you are not abusive for having these feelings and urges
you are not a bad friend/partner/family member for having these feelings and urges
it's not wrong to want to keep people safe from harm
knowing that you are prone to being over-protective due to your paranoia and working on combating those impulses, so you don't inadvertently hurt people you care about, is enough
you are enough
90 notes
·
View notes
Text
Guys, please answer if you can!
Yo, guys, I’m doing a school project to develop accomodations for other students like me who have some disorder from the Schizo-Spectrum or/and Cluster A PDs. If anyone reading this happens to struggle with some Schizo-Spectrum disorder, Cluster A PD, or “just” psychosis in general, and feel comfortable enough, please answer my form! Thank y’all so much for the attention!
https://forms.gle/93wPof5EsKXEiswM9
#cluster a#personality disorder#mental health#mental illness#schizoid stuff#schizoid#psychosis#schizo things#schizofrenia#schizotypal#SzPD#schizoaffective#paranoid personality disorder#paranoid pd#forms#research#project#school#accomodations#pls answer#l'il academic needs data#:3
15 notes
·
View notes
Text
Cluster A Disorder flags
Flags to represent cluster a personality disorders. do not use unless you have these.
transx/transid stay the fuck away from my posts none of this is for you.
--
cluster b, cluster c
--

Paranoid Personality Disorder

Schizoid Personality Disorder

Schizotypal Personality Disorder

General Cluster A flag
#cluster a#personality disorders#cluster a positivity#cluster a flags#stpd#schizoid personality disorder#cluster a personality disorders#admin kazuha/link#flag design#flag coining#pd flags#cluster a pd#cluster a flag#ppd#paranoid personality disorder#paranoid pd#ppd flag#paranoid pd flag#paranoid personality disorder flag#schizoid#schizoid pd#schizoid pd flag#spd#schizoid personality disorder flag#schizotypal#schizotypal personality disorder#schizotypal pd#schizotypal flag#schizotypal pd flag#schizotypal personality disorder flag
102 notes
·
View notes
Text
We made a personality disorder sideblog called @histrionicparanoidhell !!! Go check it out it if you want stuff on paranoid personality and histrionic personality.
There aren’t any posts yet but we’ll make some LMAO
#histrionic personality disorder#histrionic pd#hpd#actually hpd#paranoid personality disorder#paranoid pd#ppd#actually ppd#did alter#did osdd#osddid#hc did#polyfrag system#polyfragmented#polyfrag#actually mentally ill#endos dni#did introject
4 notes
·
View notes
Last Seen Blogs

marcusdjamison
Untitled

kadart-h
Kadart_h

ambereyedsnek
ambereyedsnek

kakarinlin
daydreaming

atelierarenas
Atelier Arenas