#Chemical pathology
Text
#Anatomical Pathology#Automated Tissue Image Analysis#Cellular Pathology#Chemical pathology#Clinical biochemistry#Clinical forensic pathology#Clinical microbiology#Clinical Pathology#Cooperative Human Tissue Network#Cytogenetics
1 note
·
View note
Text
“She’s so sweet she’s always going out of her way to help others” quick someone give that girl all the love and safe space she deserves before being “sweet” (pathological people pleasing as a trauma response) destroys her and leaves behind a bitter empty shell of a person
#it will! learned that one the hard way! can’t believe I didn’t see that’s what I was doing for so long :)#always just thought “I’m so nice haha wish I wasn’t” turns out I wasn’t hahah just brain chemicals outta wack :)#not that I’m not actually nice but the people pleasing isn’t what makes me so :) (me @ myself)#post traumatic growth#pathological people pleaser#rants & reflections#csa survivor#cptsd healing#childhood emotional neglect#autistic trauma#autism in girls#late diagnosed autistic#cptsd recovery#bpd mood#undiagnosed neurodivergent#abuse survivor#people pleaser#inferiority complex#trauma response#trauma recovery#traumagenic#trauma disorders
71 notes
·
View notes
Text
...
#aye. in another life i would have loved to be an illustrator#i dont like to do digital tho and i dont wanna b a starving artist and i like science too much#but it would make me so hsppy if i was allowed to draw all day everyday#forever and ever drawing#but nooo i wanted to get a phd in microbial evolution. and im procrastinating working on my preproposal#literally doing anything to not work on it. i coulf have been a illustrator. an endocrinologist. a neurobiologist. a paleontologist. but i#chose microbial ecologist then thought no fuck ecology and went for photosynthetic mechanisms#bc i do love my lil cyanos and i do love Microbiology. i love those underapprecated lil guys#the world is so big and beautiful and all i wanna do is understand. but my stupid brain doesnt work right and ive burried my wonder for so#long i wonder if ill ever have it back. i was reading a bunch of lil notes i wrote this semester and i go from#everything is so beautiful i cant stand it. there are angels in the sunbeams and they feel like healing. to im the world around me is#warping beyond my control. i cant feel any joy. my head is sending me terrible ideas but im not even scared. it feels inevitable#but last week i was so full of energy i couldnt sleep. nothing changed but the chemicals in my head#hopefully next semester will b better and i can stop feeling like damaged goods and feel bad fro my advisor#for having to deal with me. hes v nice and has a bip0lar brother so he's sympathetic but i wish he didn't have to b#i want to stop fantasizing about being something else and just focus on being better at what i am#but im such a pathological perfectionist that its so difficult to make any progress. but whatever ive been feeling alright for the#past week or so. hopefully that carries through. and maybe somedsy i can illustrate something for my precious baby cyanobacteria#unrelated
16 notes
·
View notes
Text
HEY!!! THIS IS A PATHO CODED SONG!!!!!! I PROMISE!!
discuss or send me other patho coded songs so i can make a big playlist
#pathologic#daniil dankovsky#pathologic 2#artemy burakh#мор утопия#pathologic classic hd#my chemical romance#Spotify#playlist
23 notes
·
View notes
Text
every time i sit snug as a bug in my bed and think sagely about the things i like, i feel like this:

#i will literally just lay against my pillows and scroll through tumblr and think abt my favorite things.#tonight it's mcr and pathologic.#i fucking love brainrot <3#my chemical romance#mcr#did i mention i saw them live???#i made this#save
7 notes
·
View notes
Text
Has anyone done an animatic for our lovely healers to the song Blood by MCR? It fits a little too well
#my chemical romance#mcr blood#artemy pathologic#daniil pathologic#clara pathologic#these goobers would bleed themselves dry for a town that would rather see them six feet under
1 note
·
View note
Text
Faint of Heart
Author: piksafire
Pairing: Frank/Gerard
Rating: PG-13
Words: 14k
In autopsy, it is not a matter of life and death, it's a matter of DEATH AND LOVE! Frank Iero, the new registrar in the mortuary at Mercy hospital, was not expecting autopsy to be sexy, but he also wasn't expecting his hot new boss, Gerard Way. Featuring Cobra Funerals, sap, death by papercuts and LIFE THREATENING SITUATIONS (that don't necessarily involve corpses).
1 note
·
View note
Text
if you need a sign to do that really important thing you keep putting off, this is it. just get it over and done with now and you'll never have to think about that thing ever again.
#this is entirely directed at myself#its 11pm and im only now studying for my exam in the morning#its okay biology is easier if you know how to use anki#oh how i wish i was an amoeba right now#oh you have an interest in epidemiology and pathology? name every disease ever#i may not know how to do taxes but i can tell you all about allopatric speciation and peppered moths#hey kids wanna learn about the use of chemical mutagens in modern warfare?
0 notes
Text
Cartoon depictions of the homeless increasingly reflect the hostility of today’s political leaders toward people on the streets. We’ve gone from images of charming hobos with bindles to zombies taking over cities.
If you consume any news at all, you’ve probably noticed that the United States is pathologically cruel to its homeless citizens. This May, the brutal killing of Jordan Neely—who was strangled to death, at the age of 30, simply because he was unhoused and shouting on the Manhattan subway—captured the national spotlight, but it was just one of many such cases of unprovoked violence. In January, two cops reportedly kidnapped a homeless man in Hialeah, Florida, drove him to an “isolated and dark location,” and beat him unconscious. That same month, art dealer Shannon Collier Gwin faced battery charges after he sprayed a homeless woman with a hose outside his San Francisco gallery, barking “Move! Move!” at her. (Predictably, Gwin got a lenient plea deal of just 35 hours of community service.) Elsewhere in the city, homeless San Franciscans have been attacked with chemical bear spray on at least eight occasions. Other assaults have been more impersonal but no less vicious. On July 14, the city of Houston abruptly closed its only public cooling center in the downtown area, potentially condemning anyone without shelter to suffer heatstroke in 90-degree weather. Among the property-owning class, the phenomenon of hostile architecture—sidewalks with spikes that stab anyone who tries to sleep, benches with iron bars, and the like—has become de rigueur. The widespread callousness and lack of compassion are both infuriating and hard to comprehend. How on Earth, we might ask, did things get this bad? [...]

Looking back at older cartoons, one of the things that stands out immediately is the absence of negative attitudes toward the homeless. In fact, during the Golden Age of animation, creators seemed to have had a real affinity for the poor and unhoused, often placing their most iconic characters in that role. There’s a wonderful 1948 Warner Bros. short called “Riff Raffy Daffy,” in which Daffy Duck is looking for a place to sleep—first on a park bench, then a trash can, and finally a furniture display in a shop window—and has to dodge the harassment of the police, as represented by Porky Pig in a little blue uniform. (Literally, the cop is a pig!) Or, in the 1950 cartoon “Homeless Hare,” Bugs Bunny’s rabbit hole is destroyed by a new construction project, leading him to unleash his usual slapstick mayhem against the developers until they put it back. In these cartoons, homelessness is something inflicted on people by outside forces—gentrification and the real estate business, in Bugs’ case—and something which can be successfully resisted.
Even Disney cast a homeless dog as a romantic lead in 1955’s Lady and the Tramp, contrasting Lady’s sheltered naivety with Tramp’s superior knowledge of the world. The title invokes the memory of Charlie Chaplin’s “Tramp” films, which similarly brought dignity and humanity to the role of a homeless man. (Bugs Bunny, too, takes inspiration from Chaplin, and multiple Warner animators have drawn him as the Tramp.) In 1961, Hanna-Barbera’s profoundly underrated Top Cat followed the adventures of a gang of wisecracking Manhattan alley cats, who, like Daffy, are always outwitting a meddling policeman. At worst, classic cartoons may trivialize the suffering and danger associated with homelessness—there’s a certain recurring image of the carefree hobo carrying a bindle, which paints the whole subject in a romanticized light—but the homeless themselves are rarely disparaged or made the butt of the joke. Quite the opposite.

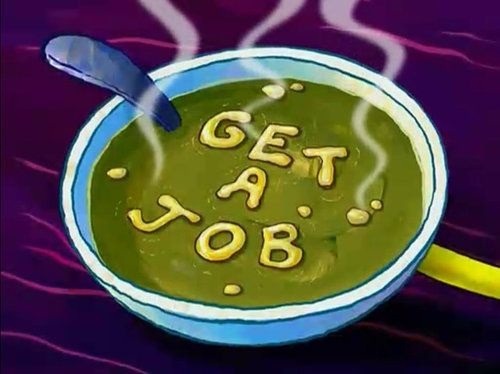
It took a few years, but cartoons caught up to the Reaganite turn. In episodes from the ’90s and early 2000s, there’s a palpable shift in the way homeless characters appear compared to earlier decades. The perspective is different: we’re now seeing them through the eyes of comfortably housed characters, rather than their own. Often they don’t even get proper names. [...] This trajectory leads us, perhaps inevitably, to SpongeBob SquarePants. [..] Squidward gets accused of stealing a dime by his comically greedy boss, Mr. Krabs, and quits his job in a fit of outrage. We then flash forward to see Squidward, now bedraggled and unshaven, living in a cardboard box on the street and begging for change. [...] Mercifully, the ever-cheerful SpongeBob gives Squidward a place to stay—but the moment he’s safely off the street, Squidward turns from a sympathetic victim of circumstance into a lazy, entitled freeloader, straight out of a Reagan speech. He makes no effort to find work and loafs around SpongeBob’s house for ages. [...] Eventually, an exasperated SpongeBob writes “GET A JOB” in his alphabet soup, before shoving him (bed and all) back to work at the Krusty Krab. [...]
Worst of all, though, the episode suggests that homelessness can be solved on an individual basis if the people in question simply stop being lazy and “GET A JOB.” This is the biggest myth of all. In 2021, a statistical analysis by the University of Chicago found that 53 percent of people in homeless shelters, and 40.4 percent of unsheltered people, do have jobs. The problem is that their wages are too low, and rents are too high. According to statistics from the same year, it’s impossible for someone working a full-time, minimum-wage job to afford a single-bedroom apartment in 93 percent of U.S. counties, and there are no states in which someone can rent a two-bedroom space on the current federal minimum wage of $7.25 per hour. In other words, homelessness has little or nothing to do with personal responsibility, or lack thereof. It’s a consequence of large-scale economic decisions made by landlords and bosses. [...]
— Alex Skopic
843 notes
·
View notes
Text
MY PATHOLOGIC ANIMATIC IS DONE!!!
Song: My Chemical Romance - Dead!
If you like it. Here's the YouTube version.
youtube
#pathologic#pathologic 2#мор утопия#мор#daniil dankovsky#artemy burakh#eva yan#даниил данковский#bachelor pathologic#pathologic art#art#Youtube
289 notes
·
View notes
Note
serious question but do you personally believe there is a way to approach psychiatry in a way that uplifts and upholds patient autonomy and wellness or is the entire trade essentially fucked haha. Btw this is an ask coming from a 3rd year med student—with a background of severe mental illness—who is considering a residency in psychiatry after receiving life-saving care in high school pertaining to said conditions. (I have peers who have been involuntarily hospitalized and treated horribly in psych wards, with approaches i patently disagree with, but was lucky not to experience. I don’t like modern american medicine’s approach to mental illness; “throw pills” at it to “make it go away” ie. a problem of overprescribing, inadequate and non-holistic approach to mental health, and i feel a lot of that can be attributed to the capitalistic framework. I also def agree with you that so much of what can be considered normal human responses to traumatic events/normal human suffering can be unnecessarily pathologized—a great example being the whole “chemical imbalances in the brain is the ONLY reason why im like this” argument that ive unfortunately fallen hard for when i was younger and am still currently dismantling within myself…and like dont even get me started on this field’s history of demonizing POC, women, LGBT, etc). Like i deeply love my psych rotations so far, and i utterly feel in my gut that this is the manner in which i would like to help people—a lot of whom are just like me—but im wondering if there is a way to reconcile these aspects in a way that one can feel morally okay participating within such an imperfect system, in ur opinion… ngghhhhhh i just want to be a good doctor to my patients…
(ps i love all ur writing and analysis on succession!! big fan mwah <333)
i don't mean to sound unduly pissy at you, specifically, but i do have to say: every single time i've talked about antipsych or broader criticism of medicine on this website, i immediately get a wave of responses like this, from doctors/nurses/psychs/students of the above, asking me to, like, reassure them that they're not doing something immoral or un-communist or whatever by having or pursuing these jobs. and it's honestly frustrating. why is it that these conversations get re-framed around this particular line of inquiry and medical ego-soothing? why is it that when i say "the medical encounter is not structured to protect patient autonomy or well-being," so many people hear something more along the lines of "doctors are mean and i wish they were nicer"? why is it that it's impossible to discuss the philosophical and structural violence of academic and clinical medicine without it becoming a referendum on the individual morality of doctors?
i'm choosing to read you in good faith because i think it's possible to re-re-frame this line of questioning to demonstrate to you the sorts of critiques and inquiries i find more interesting and more conducive to patient autonomy and liberation. so, let me pick apart a few lines of this ask.
"is the entire trade essentially fucked?"
if you're thinking of trying to 'reform' the project of medical psychology within existing infrastructures and institutions, then yeah, it's fucked. if you're still assuming that affective distress can only be 'treated' within this medical apparatus (despite, again, no psychiatric dx satisfying any pathologist's understanding of a 'disease' ie an aberration from 'normal' physiological functioning) then you're not challenging the things that actually make psychiatry violent. you're simply fantasising about making the violence nicer.
"I don’t like modern american medicine’s approach to mental illness; “throw pills” at it to “make it go away” ie. a problem of overprescribing, inadequate and non-holistic approach to mental health, and i feel a lot of that can be attributed to the capitalistic framework."
i hate when i talk about psychotropic drugs being marketed to patients using lies like the chemical imbalance myth, and then pushed on patients—including through outright force—by psychiatrists, and the discussion gets re-framed as one about 'overprescribing'. my problem is not with people taking drugs. i am, in fact, so pro-drugs that i think even the ones administered in a clinical setting sometimes have value. my issue is with, again, the provision of misleading or outright false information, the use of force and coercion to put patients on such drugs in order to force social conformity and employability, and the general model of medicine and medical psychology that assumes patients ought to be passive recipients of medical enlightenment rather than active participants in their own treatment who are given the agency to decide when and how to engage with any form of curative or meliorative intervention.
'holistic' medicine and psychiatry do not solve this problem! they are not a paradigm shift because they continue to locate expertise and epistemological authority with the credentialed physician, and to position patients as too sick, stupid, or helpless to do anything but receive and comply with the medical interventions. there are certainly psychotropic drugs that are demonstrably more harmful than others (antipsychotics, for example), and some that are demonstrably prescribed to patients who do not benefit from them and are even harmed by them. conversely, there are certainly forms of intervention besides pharmaceuticals that people may find helpful. but my general critique here is aimed less at haggling over specific methods of intervention, and more at the ideological and philosophical tenets of medicine that cause any interventions to be imposed by force or coercion on patients, then framed as being 'for their own good'. were suffering people given the information and autonomy to actually choose whether and how to engage in any kind of intervention, some might still choose drugs! my position here is not one of moralising drugs, but making the act of taking them one that is freely chosen and available as an option without relying on physician determination of a patient's interests over their own assessment of their needs and wants.
"so much of what can be considered normal human responses to traumatic events/normal human suffering can be unnecessarily pathologized"
true, but don't misunderstand me as saying that drugs or any other form of intervention should be forcibly withheld from those who do want them and are made fully aware of what risks and harms seeking them could entail. again, this would still be an authoritarian model; my critique is aimed at increasing patient autonomy, not at creating equally authoritarian and empowered doctors who just have slightly different treatment philosophies.
"dont even get me started on this field’s history of demonizing POC, women, LGBT, etc"
ok, framing this as "demonisation" tells me that you're not understanding that, again, this is a systemic and structural critique. it is certainly true that a great many doctors currently are, and have historically have been, outright racist, trans/misogynist, ableist, and so on. framing this as a problem of a well-intentioned discipline being corrupted by some assholes is getting it backwards. medicine attracts prejudiced people, not to mention strengthens and promotes these prejudices in its entire training and practice infrastructures, because of its underlying philosophical orientation toward enforcing 'normality' as defined by 18th-century statistics and 19th-century human sciences that explicitly place white, cis, able-bodied european men as the normal ideal that everyone else is inferior to or failing to live up to. doctors who really nicely tell you that you're too fat are still using bmi charts that come from the statistical anthropometry of adolphe quételet and the flawed actuarial calculations of metlife insurance. doctors who really nicely deny you access to transition surgery are still operating under a paradigm that gives the practitioner authority over expressions and embodiments of gender. the issue isn't 'demonisation', it's that medicine and psychiatry explicitly attempt to render judgments about who and what is 'normal' and therefore socially 'healthy', and enforce those standards on patients. this is not a promotion of patient well-being, but of social conformity.
"i deeply love my psych rotations so far, and i utterly feel in my gut that this is the manner in which i would like to help people"
let me ask you a few questions. you say that you like your psych rotations... but how do your patients feel about them? is their autonomy protected? are they in treatment by free choice, and free to leave any time they wish? are they treated as human beings with full self-determination? if you witnessed a situation in which a patient was coerced or forced into a certain treatment, or in which you were not sure whether they were consenting with full knowledge or freedom, would you feel empowered to intervene? or would doing so threaten your career by exposing you to anger and retaliation from your higher-ups? what higher-ups will you be exposed to as a resident, and then as a practicing physician? could you practice in a way that committed fully, 100%, to patient autonomy if you were working at someone else's practice, or in a hospital or clinic? could you, according to current medical guidelines, even if you had your own practice?
when you say "this is the manner in which i would like to help people", what do you mean by "this"? can you define your philosophy of treatment, and the relationship and power dynamic you want to have with any future patients? is it one in which you hold authority over them and see yourself as determining what's in their 'best interests', even over their own expressed wishes? have you connected with patient advocates, psych survivors (other than your friends), and radical psychiatrists and anti-psychiatrists who may espouse heterodox treatment philosophies that you could consider? do you think such philosophies are sufficient for protecting patient autonomy and well-being, or are they still models that position the physician's judgment and authority over that of the patient?
"im wondering if there is a way to reconcile these aspects in a way that one can feel morally okay participating within such an imperfect system"
and here is the crux of the problem with this entire ask. you are wondering how to sleep at night, if you are participating in a career you find morally distasteful. where, though, do your patients enter into that equation? do you worry about how they sleep at night, after having interacted with a system of social violence that may very well have traumatised them under the guise of providing help? why does your own guilty conscience worry you more than violations of your patients' bodies, minds, and basic self-determination?
i can't tell you whether your career path is morally acceptable to you. i don't think this type of guilt or self-flagellation is fruitful and i don't think it helps protect patients. i don't, frankly, have a handy roadmap sitting around for creating a new system of medicine and health care that rests on patient autonomy. affective distress is real, and is not something we should have to bear alone or with the risk of having violence inflicted upon us. what you need to ask yourself is: how does the medical model and establishment serve people experiencing such distress? how does it perpetuate violence against them? and how do you see yourself countering, or perpetuating, such violence as someone operating within this discipline? what would it mean to be a 'good' actor within a violent system, if you do indeed believe that such a thing is ontologically possible?
710 notes
·
View notes
Text
"what is your purpose in life?" to live. to continue living. i was put on this world continue the chemical dance that is our collective life that started when the first cell membranes inexplicably formed around amino acids and will continue until our inevitable extinction wether through the sun or our own pathology. and endless cycle of creating consuming and decomposing that i have been granted the delighting privilege of partaking in.
i pluck out the cherries turned from sunlight into sweetness, as the tree they hang from roots into the soil fertilized by mulch, the flowers fertilized by bees in turn, as the birds on the branches, and the microorganisms living in my body feast along with me.
and one day, either sooner or later, i will die, and the worms and bacteria and mycelium will feast on me as they do on every browning leaf and rotten fruit and fallen tree and and any other corpse big or small and the dance of life will continue. and i will rest easy knowing i had a body that ate and moved and lived and that there was nothing more precious for me to do. what greater purpose could there be?
#MISS ME with that productivity and sentience shit idgaf about any of that i'm just here for the ride man#death cw
118 notes
·
View notes
Note
I do not mean to sound stupid, but I read your post "dissociation is not solely trauma-based", and I was wondering if you knew of any sources or books about it?
I think I don't fully understand what dissociation is.
For exemple, no matter how I look at it, I don't understand how meditation could be considered like anything close to dissociation, simply because it's also used as a grounding technique.
I'm combining two asks here, because I'm going to cover both in one go :) you don't sound stupid.
You've got to start with the understanding that dissociation is a continuum from normal (aka nonpathological) to "abnormal" (I hate that word, but aka pathological). I finally dropped the wild existence of Dr Jamie Marich, clinical trauma specialist and a pro endo, CDD system, who wrote Dissociation Made Simple. Let me quote because the book is actually good.
Yes, dissociation is so hard to understand that she wrote an entire book about the concept.
"The English word dissociation comes from the Latin root dissociātiō, meaning “to sever” or “to separate.” At this point when lecturing, I usually ask my students: What are we severing or separating from when we dissociate? You may take a moment, before reading on, to ask this question of yourself. Try not to think on it too rationally. Listen to your gut-level response...
For the purposes of this opening chapter, let’s focus on the form of separation that every human being can likely relate to —severing or separating from the present moment—especially when the present moment becomes unpleasant, overwhelming, or otherwise painful."
Dissociation is a disconnect from something-- this can be memories, thoughts, emotions, or, in worst cases, reality. The present moment.
Not all meditation is dissociative, but most is. For example, emptiness meditation is about disconnecting from everything in the moment. You are literally fine-tuning your dissociative techniques. This is also true when you're using grounding meditation to disconnect from overwhelming emotions or thoughts to get back into the moment.
There are a variety of tasks that we either develop naturally or learn as a way to achieve some degree of separation (e.g., enough to stay somewhat present but still get some relief, or going further into totally cutting oneself off from in-the-moment presence). Dissociation of this nature is not all or nothing—it generally happens in degrees and can depend upon how much distress you feel in any given context. We can do this by daydreaming, drifting off, zoning out, zoning inward, disengaging eye contact with people, losing focus (especially when driving), or getting a little floaty in many other life circumstances. Some people frame this “floatiness” as similar to hypnotic trance and others feel it is quite distinct. We may even take deliberate steps to enhance the experience of separation. How often have you escaped into a book or a movie, into your phone or computer, or into some activity, because it makes the harshness of dealing with the present moment and the emotions it can elicit somewhat more bearable?
Let me be very clear, if you said yes to this question, this answer does not mean that there is anything wrong with you! All of these can be quite ordinary forms of dissociation that every human being is capable of experiencing.
A really, really good way to understand this concept is actually through maladaptive daydreaming (MADD), a highly addictive form of dissociation.
Indeed for many of us, substances or other behaviors that cause major surges of dopamine (e.g., spending, computer games, sexually acting out) can become the accelerant of dissociation...
Whenever we become accustomed to dissociating, especially as children growing up in complex trauma, our brain becomes bonded or some would even say addicted to that state of escape. Once chemical or other reinforcing behaviors are introduced to us, they can accelerate that already familiar experience and we become further bonded to that behavior.
Daydreaming itself is dissociative. Point blank. It is both the most normal kind of dissociation, and yet the most common maladaptive dissociation.
Daydreaming and journeying into my head’s imaginative scenarios is another series of behaviors that can have both adaptive and maladaptive qualities. As a kid, they kept me safe. As an adult, they are the source of so much of my creative power—yet if I engage them too long, too hard, or too much, I run the risk of getting lost and not being able to attend to what helping professionals might call my activities of daily living (e.g., eating properly, sleeping, taking good care of myself, getting to work, attending to loved ones appropriately and with good boundaries).
Let's cut away from the book really quickly to look at Eli Somer, the guy who came up with MADD.
Maladaptive daydreaming is a dissociative disorder: Supporting evidence and theory.
The only real thing I want to quote is:
Although trauma may be one causal factor, we indicate several other etiological pathways to the development of MD. We discuss associations with related concepts and suggest directions for future research.
And
MD is strongly related to dissociation and seems to rely on an innate tendency for absorptive and imaginative fantasy. Through its rewarding properties, this form of immersive daydreaming becomes abnormal. MD may thus be viewed as a disordered form of dissociative absorption.
While Somer talks about how it can be a behavioral addiction in that paper, I find this is a more succinct description.
Maladaptive Daydreaming: Epidemiological Data on a Newly Identified Syndrome
Maladaptive Daydreaming (MD) is a proposed mental disorder characterized by excessive, compulsive immersion in vivid and complex fantastical daydreamed plots, generating intense emotional involvement, often accompanied by stereotypical movements. This addictive absorption in daydreaming becomes maladaptive as it consumes many hours a day, generates shame or guilt, hinders achievement of short- and long-term goals or tasks, and overall causes clinically significant distress and/or interferes with functioning in social or occupational realms. Maladaptive Daydreamers (MDers) report a strong urge to daydream whenever they can and annoyance whenever they cannot, and, repeated unsuccessful efforts to control, cut back, or stop daydreaming, like other behavioral addictions.
And that's the best way to look at DID and other maladaptive, pathological forms of dissociation. It's a behavioral addiction, an escape that we not only crave, but can no longer live without. Just like you can get addicted to working out and gambling, you can become addicted to severing ties with reality through pleasurable (and in some cases, necessary) forms of escape.
I don't know if this is going to make sense, but I've found looking at dissociation like an upside-down iceberg helps me.
At the top, the widest part, is everyone on the planet, and the basic, general concept of dissociation. Severing from the present moment, be it through your phone, book, daydreaming, meditation, zoning out.
As you go down, and it gets narrower, it becomes more important to put names to specific types and forms of dissociation, and fewer people struggle with these forms. In the middle is a confusing mix of seemingly normal and pathological dissociation. You have mediumship, authors with living characters, OCD (yup), ADHD (shocking, I know), MADD, DPDR, (C)PTSD, people on the edge of forming behavioral addictions.
At the bottom, the smallest point, only pathological dissociation, with a much smaller population experiencing it. DID, OSDD, severe and chronic DPDR, DA.
For people that struggle with dissociation... they fell down a hole and travelled all the way to the bottom of the iceberg. What was once a general, normal, human experience became a very specific problem. Over the years, as they travelled deeper, they used and developed a complex mix of various normal dissociative reactions until it eventually became a named, pathological experience.
I sincerely hope that this helps explain and answers both questions ):
Here's another really interesting paper (from none other than, DUNDUNDUN, Colin Ross).
Maladaptive Daydreaming, Dissociation, and the Dissociative Disorders
#syscourse#pro syscourse conversation#CDDs first#cdd system#actually cdd#did#osdd#actuallydid#actuallyosdd#actuallytraumagenic#plural#actuallyplural#pro endogenic#endogenic safe#system safe#pro system#dissociation#actually dissociative#anti endo#pro endo#resources
75 notes
·
View notes
Text
why is it so weird to be a human being. ive got pathologies ive got blood in me ive got a brain full of chemicals ive got layers of skin ive got a tumblr blog
275 notes
·
View notes
Text

[ID: a page with text on the top saying "When your brain is the one breaking down, the idea of mental illness seems excruciatingly real" on the right is a line drawing of a person talking to a therapist. to the left is a block of text "When you start to ask the authorities questions like What are Mental Illnesses? you tend to get answers like:" a block of text with an image of a brain answers the question with "In general they're disorders of the brain, your body's most important organ. A mental illness is:
a health condition, much like heart disease or diabetes
no one's fault-- not the person's, nor the family's"
To the left the text continues "These answers reassure a lot of people. They make it clear mental illness isn't a result of weakness. They take away a lot of the shame. And they offer a hope that mental illness can be treated with drugs and standard medical procedure, like any other disease."
"But it's not that simple. There's no blood test for mental illness. Diagnosis relies entirely on the subjective opinion of the psychiatrist. And the American Psychiatric Association has recently added new "disorders" like Compulsive Shopping Disorder and Oppositional Defiant Disorder to its list of illnesses. Are these really chemical conditions like diabetes that should be treated with drugs, or are they outgrowth of a sick culture seeking quick fixes for unhappy housewives and easy ways to control kids who question authority?"
"When you ask some people What are Mental illnesses? you get answers like "Mental illness" is a convenient label for behavior that disrupts social order." to the right is a line drawing of a person performing chemistry.
A text box with small print takes up the bottom of the page.
"You get answers like: people who notice how screwed up our world is, or who perceive reality in radically different ways than "normal" folks, and then display "extreme" reactions, get labeled with a disease. Which could render dumpster diving and Christian fundamentalism a form of pathology, depending on who's making the diagnosis. Consider: a kid can't sit still in class and wants to talk when he has an idea, instead of when he gets called on. Is the kid out of control and in need of Ritalin, or is it possible that school is actually incredibly regimented, unimaginative, and mind-numbing to the point that a child with an active, inquisitive brain might find it very difficult to pay attention? According to the DSM-IV, the official diagnostic manual of the American Psychiatric Association, a behavior "clinically significant" enough to be labeled a disorder must not be an "expectable and culturally sanctioned response to a particular event." So if an average American responds to any given atrocity-- like the fact that people are starving in cultures all over the world where farmers are being forced to grow coffee for America instead of food for their people--with an expectable and culturally sanctioned response, like turning on the television to avoid thinking about it, they are healthy. Whereas if I sob hysterically and talk to strangers about it and stay up all night trying to think of ways to change it, I might be the one who gets labeled with a disorder."]
-Navigating The Space Between Brilliance And Madness: A Reader & Roadmap Of Bipolar Worlds
#antipsychiatry#anti psychiatry#anti psych#antipsych#mad pride#mad liberation#madpunk#neurodivergent
20 notes
·
View notes
Text
look. im not saying that adhd doesn't cause very real struggles, because it does, and im not saying that adhd is made up to pathologize fairly normal human behaviors. but there are certain things that we sometimes recognize as symptoms of adhd that are actually just part of human nature and are brought out by circumstances that we were not created or evolved to handle on a regular basis.
don't get me wrong, I hate the notion "adhd only exists under capitalism" because adhd is a brain chemical deficit that exists even outside the stressful demands of consumerism and profitability of productivity. this can be evidenced in long states of depression and inactivity when it comes to things we even want to do but can't force ourselves to. but that doesn't negate that the symptoms of adhd can be greatly exacerbated and even feigned from the pressures and anxiety that "grind culture" generates. so when you see someone say "im really stressed out by my 9-5 job and don't want to/can't sit at my desk staring at a screen completely silent and still for 8 hours," your immediate thought probably shouldn't be "that's adhd," it should be that we as humans are just not built to do that. framing these emotions and behaviors as "abnormal" from the ideologically perfect human that doesn’t exist doesn't help anyone except to oil that capitalist machine. these conditions are inherently inhumane and not structured with humans in mind.
270 notes
·
View notes
Last Seen Blogs

coffeebooksrain18
Team Green Defender

mollyponkevitch
The Ecliptic

ossielv
Ossiel V

alicampping
alicamping.com

polish-art-tournament
orki z majorki (i z ukrainy)