#mental health statistics
Text
Today I overheard a convo of people talking about ADHD saying everyone has it and it's just how the brain works...

Almost everyone has trouble concentrating. That's not ADHD.
"ADHD is a neurodevelopmental disorder that can cause attention difficulties, impulsivity, and hyperactivity. Research suggests that imbalances of neurotransmitters, such as dopamine".
Reducing ADHD to just trouble concentrating is inaccurate and quite ignorant. Some symptoms I have:
Hyperactivity and Impulsivity: Being unable to sit still, especially in calm or quiet surroundings, constantly fidgeting,
being unable to concentrate on tasks,
excessive physical movement, excessive talking, being unable to wait their turn,
acting without thinking, interrupting conversations, little or no sense of danger.
——————
Hyperfocus: Happens when a person becomes so absorbed in an activity that they tune out to everything around them. This usually occurs when the person is engaging in something they find fun, rewarding, and stimulating.
——————
Hyperfixation: Intense focus on a single subject may cause you to spend more time and energy on it than you intend to. If left unchecked, hyperfixation can lead to negative consequences and disrupt your day-to-day functioning.
——————
ADHD Paralysis: When a person with ADHD is overwhelmed by their environment or the amount of information given. As a result, they freeze and aren’t able to think or function effectively. This makes it challenging for the individual to focus and complete their tasks—including urgent ones.
——————
Emotional Dysregulation: Experiencing emotions so deeply that they become overwhelmed or “flooded.” One may feel joy, anger, pain, or confusion in a given situation—and the intensity may precede impulsive behaviors they regret later.
——————
Executive Dysfunction: A term used to describe faults or weaknesses in the cognitive process that organizes thoughts and activities, prioritizes tasks, manages time efficiently, and makes decisions. (I wouldn't say I experience this, but it's really common).
And if you know you don't have ADHD and think this is all relatable, remember the extent.
It's a disordser. I'm sure people without ADHD struggle a lot with some of these, but they do not have a biological difference that causes them. There's a difference between struggling with something and having a disorder.
——————
It has medical treatment, as s disorder. There are 3 different types of medicine that are prescribed by professional doctors. If you know you don't have ADHD, you cannot take it. Just like medicine for any other disorder.
A few not-so-fun statistics about people with ADHD:
Percent of children with ADHD who had at least one other disorder:

[The facts below are taken from Cross River Therapy]
About 10% of people with ADHD a substance use disorder regarding alcohol or drugs.
——————
Bipolar disorder is 6 times more common in adults with ADHD.
——————
About 33% of students with ADHD dropout of high school, more than twice as many as those without ADHD.
——————
Only 15% of people with ADHD complete a four-year degree at a university.
——————
Drivers with ADHD have a risk of accidents that is 47% higher than their non-ADHD peers.
Not everyone has ADHD.
And I kindly ask everyone to stop saying things like this. Because it's contributing to the myth that ADHD isn't a real disorder, just something people make up for attention, or isn't that serious.
#adhd things#adhd problems#adhd brain#adhd issues#actually adhd#mental heath#mental health awareness#mental health statistics#adhd awareness#adhd is wild#adhd culture#adhd diagnosis#mental disorders#depression#attention deficit hyperactivity disorder#attention defecit#adhd
26 notes
·
View notes
Text
#mentalhealthmatters#mental health#teenagers#mental health awareness#mental illness#mental health statistics
11 notes
·
View notes
Text

#stop stigma#mental health#mental illness#mental health stigma#mental health statistics#mental health awareness month#infographic
2 notes
·
View notes
Text

9K notes
·
View notes
Text
#future of mental health care#mental health technologies#Future trends in mental health care#mental health treatments#mental health statistics#mental health technology 2023
1 note
·
View note
Text
Mental Health Information

View On WordPress
0 notes
Text
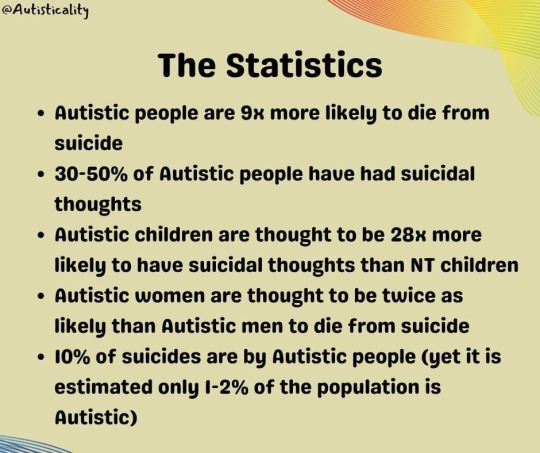
I would like to warn you that this post contains things like suicide and death. I believe this is a very important issue that needs to be addressed. If that makes you uncomfortable, you are free to click or scroll away. I understand.
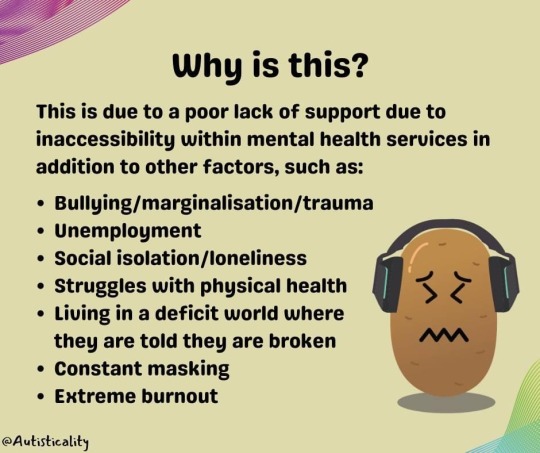
Autistic Suicide



The Autistic Teacher
#autism#actually autistic#autism awareness month#autism acceptence month#TW suicide#TW death#autism and suicide statistics#mental health#neurodivergence#neurodiversity#actually neurodivergent#feel free to reblog/share#The Autistic Teacher (Facebook)
152 notes
·
View notes
Text
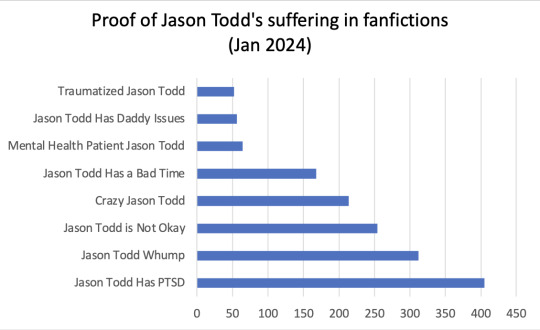
Here you go! The charts resulting from the poll!
Date of creation: 05.01.2024
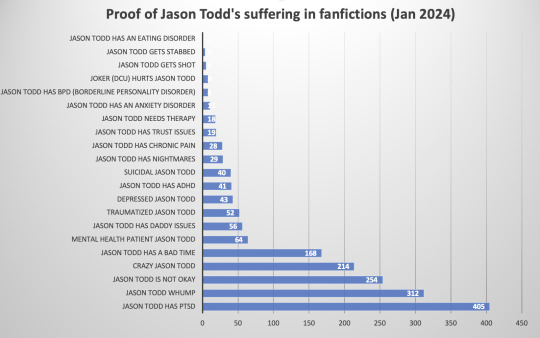
The second chart is the more detailed version including more tags.
I excluded the meta tag "Hurt Jason Todd" (more than 2000 tags) because its subtags are already on the chart.
I assume no guarantee or liability for the completeness, correctness and accuracy of this chart despite my best efforts.
Includes fanfictions in all languages available on Ao3, NOT English only.
More charts will follow. :)
Want to have a chart for different pairings, headcanons etc. in your favourite fandom? Send me an ask!
#ao3#ao3statistics#batfam#dc comics#batfamily#ao3 fanfic#statistics#batman#jason todd#bruce wayne#jason todd suffers#jason Todds suffering in fanfiction#mental health#hurt jason todd#jason todd has ptsd#jason todd whump#jason todd is not okay#crazy Jason todd#jason todd has a bad time#mental health patient jason todd#jason todd has daddy issues
112 notes
·
View notes
Text
Pride is infested by big banks, cops, and puritanical anti kink rhetoric all while the rising tide of fascism want us dead but this is what's "gentrifying" the community, allegedly (also why the automatic assumption that these men aren't also bisexual? 🤨)
#maybe if people didnt act like this and there was community support for bisexuals we'd have our own designated bars#dont make me tap the sign of bisexual mental health statistics#op is bi? embarrassing!#imagine being a pick-me bisexual to the biphobes they're not gonna fuck you
121 notes
·
View notes
Text
anyway it always kind of baffles me when i see takes saying that deaf people aren't disabled or don't face ableism when we have been historically subjected to eugenics, can face neurodevelopmental difficulties due to language deprivation, have been called 'dumb' in the ableist slur sense, don't have access to a lot of spaces that don't have sign language or cued speech interpreters and that just. in general. hearing loss even when you're only partially hard of hearing can be so fucking isolating
#can't remember the exact statistics but we are a demographic extremely vulnerable to depression & other mental health issues#as a consequence so yea :)#and that's not even mentioning deaf people whose deafness intersects with other disabilities#also.... deaf/neurodivergent solidarity WHEN. there is a lot of overlap between our communities can we talk about itttt#entries#deaf tag#deaf#ableism#audism#disability
396 notes
·
View notes
Note
Genuine question, what’s wrong with the DSM?
[OP refers to the Diagnostic and Statistical Manual of Mental Disorders, which I mentioned being unpopular among mental health professionals.] Disclaimer: I'm not a psychiatrist, I'm not a therapist, and I'm not trained in counseling. I'm a social psychology researcher. If a therapist contradicts me, listen to the therapist.
The problem with the DSM as I understand it: a lot of counselors/ psychiatrists/ etc. want to move away from a category- and source-based diagnostic system, toward a symptom-based treatment system. For example, think about Pepto Bismol: you feel nauseous, you chew pink tablets, it ends your nausea. It doesn't matter if your nausea is indigestion or seasickness or lactose intolerance. You match a treatment (pink bismuth) to a symptom (nausea) and don't waste time or money on diagnosis unless that treatment proves ineffective.
A large percent of counselors etc. would like to take the same approach to mental health. So we'd be researching treatments for nightmares (neurofeedback? MDMA?) in the long-term, and giving clients treatments for nightmares (meditation! Ambien!) in the short-term. All without worrying too much about whether the nightmares are caused by General Anxiety Disorder or a phobia or Seasonal Affective Disorder. There are many strengths to that approach.
Only, see, there's this big purple dinosaur holding us back.
[Image ID: Hardcover copy of the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, DSM-5, American Psychiatric Association; the title is white text on a purple background.]
So if everyone who uses the DSM also hates the DSM, why does it still exist and why do we keep buying it every time a $100 text revision gets published? Two reasons, in order of importance:
Insurance
Communication
Insurance is, I kid you not, the DSM's #1 reason for existence. American insurance companies won't cover treatment unless it's for a diagnosed illness, and so therapists put diagnosed illnesses on what they'd often be more comfortable describing as "bro, this dude is hella distressed and I'm trying to help undistress him." Note the word American on the cover; other countries have other manuals, and no other country's counselors are as chained to theirs as we are to ours. This means that the DSM helps — yay, affordable therapy! It means the DSM hurts — sets of symptoms get grouped artificially, spectra get split into categories, and diagnosis happens way too early in the therapeutic process.
Another comparison to unmental health: I don't have carpal tunnel syndrome, but my insurance provider thinks I do. I only announce that I don't because I haven't told you who I am or where I live. (If the insurance companies find us... Well, we just won't let them find us. The thing you should know is everyone is getting screwed by health insurance. Yeah, even you.) I have wrist pain and tingling. It has the wrong antecedents for carpal tunnel, and it has weird manifestations — pressure on the base of my thumb causes pain in my pinky — but my OT wrote down "Carpal Tunnel" on the forms because the alternative was a $500+ round of diagnostic scans. No one cares whether my median nerve is inflamed or not; occupational therapy still looks like "try this stretch, that stretch, this brace, that brace, and these activity changes; keep whichever combination makes the pain and tingling go away."
This kind of thing also happens in mental health all the time. Many therapists don't care — and neither should you — if your serotonin levels are low; if you're miserable and an SSRI prevents the misery, take the dang SSRI. If your mother was harshly critical and now you feel panic at any hint of criticism, it doesn't matter whether that better fits C-PTSD or NPD; it matters whether you cope with soothing self-talk or if you cope with alcohol. Put something from the DSM on the forms, and focus on finding which stretches (breathing exercises) make the tingling (panic) go away.
Communication is the biggest strength of the DSM. It means that clients can benefit from labels ("I'm not lazy, I'm ADHD") and consistent standards of treatment can be applied across different clients in different states. The DSM has huge lists of things like "if your client shows memory problems, be sure to check for alcohol abuse" or "if they have self-harm, make sure it's non-suicidal before you do anything else" that are tremendously helpful. It can help therapists who encounter a set of behaviors they've never seen before to go "client is rigid, rule-bound, and lacks insight... huh, looks like I'd better refer them to an OCPD specialist." (It's also the source of a lot of toxic misinformation on social media when symptom lists get taken out of context without that all-important differential diagnosis information, but I digress.)
However, diagnosis should never be the beginning point for therapy — it's impossible to know your client's mind without first building trust and transference — but reliance on the DSM for insurance often forces it to be. Diagnosis should never be the end point for therapy — knowing your perceptions don't match others' because of Bipolar I won't stop you hearing the dang hallucinations — but home use of the DSM often acts that way. Categorical diagnosis is limiting if your therapist is primarily interested in how depressed you are but the Beck Depression Inventory uses an absolute cutoff point for "depressed" or "non-depressed." Categorical diagnosis is useless if over 50% of people diagnosed with a depression are later diagnosed with an anxiety disorder, and vice versa. So it's an imperfect book that does a lot of things well and a few things badly, and many of its heaviest users would argue that it shouldn't exist at all.
For further reading, I recommend The Body Keeps the Score by Bessel van der Kolk. I don't agree with all the axes he grinds or all the ways he grinds them, but he's got decades of psychiatry experience and is (I hope) predicting the next paradigm shift in mental health.
For instance, van der Kolk argues that it doesn't matter if at intake your client has long blond hair and is named Linda, only to show up the next time with no hair and the name Gerald, only to come next time with short red hair and the name Taylor. The therapist should only be asking "how does the client feel about these changes?" and "what are these changes doing for the client?" If Linda can't remember what Gerald did, then focus on the terrible memory gaps that alter identities create. If Taylor became Gerald to try and please you, then focus on teaching mindfulness and self-compassion. If this is a happily genderqueer person, then figure out why they're seeking help and don't worry about the appearance changes. If this is someone who thinks in absolutes and regards their personality as constantly changing, then work on teaching them to see the world and themself with moral complexity. It doesn't matter whether Dissociative Identity Disorder exists or not; just ask your client what they need and how you can help, then go from there.
Anyway, the DSM is an imperfect solution to a complex problem, and a lot of mental health practitioners view it as a relic of a more paternalizing era. No one has come up with a really good solution for how to remove and replace it, so for now it's the least-bad option.
#dsm#dsm 5#psychology#psychological research#therapy#counseling#mental health#diagnostic and statistical manual of mental disorders#psychiatry#diagnosis#long post#(almost) nothing to do with animorphs#depression mention#ptsd mention#suicide mention#american politics#to be 100% clear: I *do not know enough* to have an opinion about whether or not Dissociative Identity Disorder exists#i only know that some very expert people have argued for it *and* that some very expert people have argued against it#and that all these very expert people absolutely agree on listening to the client howsoever the client chooses to identify#more research is needed#I reiterate: I AM NOT A THERAPIST AND NONE OF THIS IS MEANT AS MENTAL HEALTH ADVICE
587 notes
·
View notes
Text
What triggered your mental illness?
What contributed to the trauma underlying it?
What caused the circumstances such that you couldn’t get better?
It’s capitalism, baby.
#anti capitalism#capitalism#mental illness#leftist#anarchist#anti psychiatry#statist education system#capitalist education system#education system#neoliberalism#anti neoliberalism#politicize mental illness#mental health#anarchism#anti statism#capitalist realism
40 notes
·
View notes
Text

#mental health#mental illness#mental illness statistics#mental health awareness month#mental health awareness#mental health statistics#infographic
0 notes
Text
oh did I ever update anyone on the internet trauma survey? No? okay here!
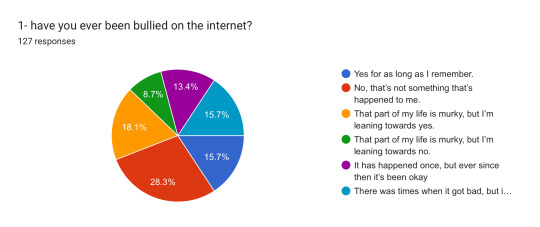
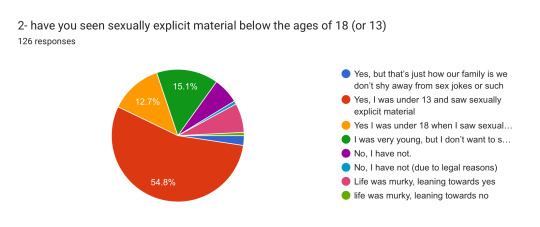
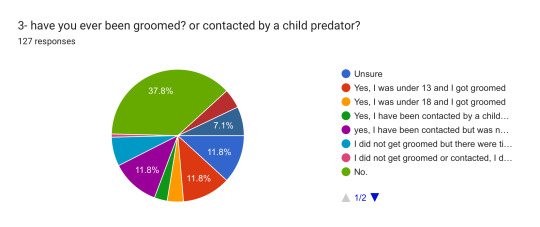

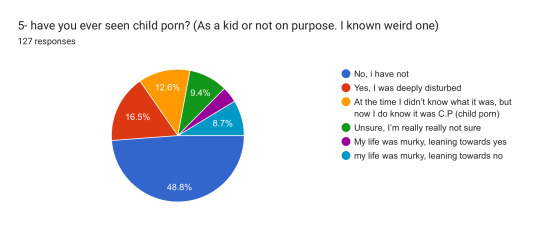
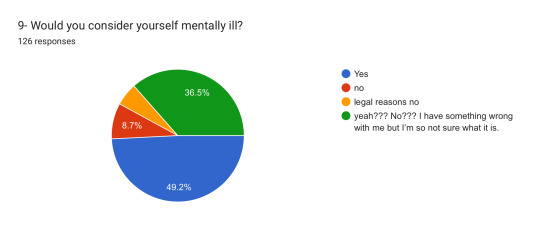

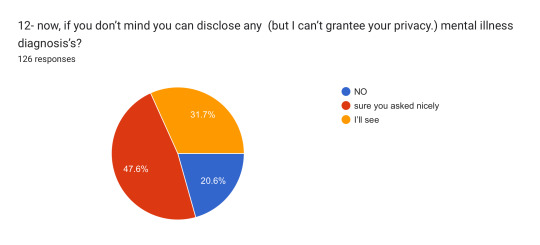



Here’s all the charts!
I am too tired and don’t have enough people to fully start putting together stats yet, but this is some of the stuff that wasn’t individual responses I have to sort through.
here’s the form https://docs.google.com/forms/d/13FLWcID1Wd3tPUY9NPzah8KL9U6YVXQ8EZcKbK8feCE/viewform?edit_requested=true#responses
and I hope this is interesting!
#-pop#internet trauma#the internet#internet#websites#mental health#mental illness#trauma#google forms#survey#online survey#research#statistics#discussion
27 notes
·
View notes
Text
Random Fact #6,427
Only about 3% to 5% of violent acts can be attributed to individuals living with a serious mental illness, according to the US Department of Health and Human Services.

#gun violence#gun control#misconceptions#ableism#united states#statistics#did you know#little known fact#stigma#mental health#random facts#random fact
67 notes
·
View notes
Text
'It's alarming': More than half of LGBTQ young people unable to get mental health care, study finds - ABC11 Raleigh-Durham
As North Carolina legislators debate Senate Bills 636 and 579, young people in the LGBTQ community reported in a new survey that their mental health is being harmed.
Senate Bill 636 would prohibit transgender girls from joining female sports teams in middle and high school. Senate Bill 579, referred to by supporters as "Prevent Harm to Children," would increase the punishment for disseminating obscene materials when a minor is present.
"They're being told by their leaders that they don't matter, that they don't have value, that they are villains," said Candis Cox with the LGBTQ Center of Durham.
The Trevor Project just released results of a nationwide survey that involved more than 28,000 LGBTQ young people between the ages of 13-24.
The results found
41% of LGBTQ young people seriously considered attempting suicide in the past year
56% of LGBTQ young people who wanted mental health care were not able to get it
A majority of those surveyed reported being bullied or harassed at school by people who thought they were LGBTQ
Nearly 1 in 3 said their mental health was poor most of the time or all the time due to anti-LGBTQ legislation and policies
Nearly 2 in 3 said hearing of the potential of new laws and the prohibition of discussion of LGBTQ issues in the classroom made their mental health a lot worse
"41% is an alarmingly high rate. For anyone I mean, 1% is a terrible thing, but 41% LGBTQIA+ people to be considering suicide is terrifying," said Cox. "Because that means that nearly half of LGBTQIA+ people surveyed don't feel as though they actually have a right and an ability to live and to exist and to be in this country and in this world."
#Lgbtqia#Mental health#lgbtq youth#protect trans lives#protect trans youth#Trans#Statistics#Tw suicide mentioned
27 notes
·
View notes
Last Seen Blogs

the-plague-beast-blog
Welcome to the Hollow

kana-muchi-midori
MESSAGING SYSTEM IS BROKEN PLZ USE INBOX

obscenebulges
Obscene Bulges

didoff
Artismod
