#misused mental health terminology
Text
🐈
#ooh I have a lot of thoughts about Six and Charley and her mysteriousness and how he responds to it#but they intersect with my Six's Mental Health Thoughts which are extremely headcanony#and I know a lot of the fandom would rather just kind of wall off Twin Dilemma and assume Six's proper characterization doesn't include it#and I don't know that I blame them for that#but I like trying to make things fit together#and also there's no way to do that without probably misusing real-world mental health terminology#because (watsonian) the doctor is an alien with an alien brain and (doylist) the writers do not know all that much about psychiatry#but. at least for a bit after his regeneration he deals with paranoia right?#like that's the term the narrative uses. (and it clearly explains his attack on peri - he's perceiving her as a threat due to delusion)#& she says 'I'm not letting a manic depressive paranoid personality like you shut me up' & he objects specifically to 'manic depressive'#later in uhhhh revelation of the daleks? he doesn't tell her about a real danger#and he says 'I didn't want to burden you with what might have been a piece of paranoid speculation on my part'#again I cannot emphasize enough how much I am talking about a fictional character with fictional problems. I do not know psychiatry either!#I do not want to mislead#but one of this character's problems is that he has a badly calibrated sense of danger. sometimes he sees things as threatening that aren't#and sometimes he overcompensates for that#and I think when he first meets Charley he is really not very sure whether he should trust the alarm bells he's hearing or not#she seems deeply suspicious! but also nice? he wants to like her? but deeply suspicious!#'or am I just being crazy?' he asks himself#and so he just kind of... keeps watching her#also unrelatedly to all that I think he kind of likes having the excuse of Mystery for doing what he does anyway which is orbiting her#just slightly obsessing over his companion at the time even if he also occasionally forgets they're there#(he's just very all or nothing in everything all the time)#but yeah. you know how 11 gets about Clara and her Mystery Plotline? 6 is like that about every companion in turn anyway#so he doesn't actually mind having the excuse of Mystery with Charley#this is also why 6 and Clara is so compelling#(this was a tag essay in response to lrb but I decided it was opening too many cans of worms and needed its own post)
19 notes
·
View notes
Text
been seeing these memes since like 2021 that are like "me when im delusional" and like "im such a delusionalgirl" and "me when i think the walls are talking to me" or whatever and at first i kinda assumed like Oh we're all in this together we're all experiencing things we fully believe against all evidence to the contrary huh. like we're all experiencing delusions right now. But its kind of occured to me that its probably just ableism actually . and people are probably referring to like... thinking their crush likes them back. and not that someone has transformed into a beetle and lives on their windowsill to watch them.
#text#ask to tag#i was like wow a lot of us were going thru this at the same time thats weird.. wait .#:/#so it's ableism again? it's misusing mental health terminology again to be 'funny'? saying this he picks up a large rock
16 notes
·
View notes
Text
Ok, so I have a question.
I was reading this post talking about TikTok and the misuse of the term "Intrusive Thoughts".
Now I have intrusive thoughts. I have one specifically that I call Dave that is so horrifying to me that I've had a meltdown over it at one point. I've dealt with them for a while, and I've figured out that my intrusive thoughts have a very distinct feel that other thoughts I actually think don't have.
They feel quicker
They're often in pictures despite me normally thinking in words
They have details that aren't technically in words, but that I still understand and can translate into words after the thought has already come
They're something I would never actually do
It's a far different feeling from the normal thoughts that I have.
I was once in a diner and just talking with the people I came with, and the waitress brought us a syrup dispenser. I glanced at it while I was talking and had the thought of guzzling it down and seeing the look on her face when she came back. I laughed at the objectively funny thought and joked about it with my friends before moving on.
It didn't disturb me, but it came quicker, was in a picture, had too much detail for how long it was in my head, and was something I would never actually do. It was clearly an intrusive thought, but it didn't disturb me in the slightest because it was funny.
Op said, among other things, “lol I had an intrusive thought to jump on the table” was not an intrusive thought. I haven't had that thought in particular, but I would say the story I told above compares.
So, my question is: if it looks like an intrusive thought, walks like an intrusive thought, and talks like an intrusive thought, why am I not allowed to call it one?
There was literally no difference between the thought about the syrup and one about my friend popping my eye out with an offset spatula except instead of cringing, I laughed, so it isn't real? I really looked at the dispenser and thought, "It would be a really good idea to drink all of that syrup!"? What they're saying here is that, deep down, despite the fact that it would make me sick, it's antisocial, it would make my friends worry, it would disturb the waitress, it would be deeply embarrassing and stupid, and I don't really have a sweet tooth, I actually wanted to drink the entire dispenser of syrup.
The thing I'm saying is that I disagree with op. The core of intrusive thoughts is not, thoughts/images/“urges”/ideas that are unwanted and distressing to the person having them. It's thoughts you wouldn't ever have otherwise. And I don't understand why I'm not allowed to call my intrusive thoughts, intrusive thoughts.
If anyone can explain why then do so! I would love to know! But I don't understand why we have to narrow this term down when it shouldn't be this narrow.
#intrusive thoughts#adhd#questions#mental health#terminology#silly internet discourse#<- my tag for things like this#misuse of terms
0 notes
Text
Oh my god, they’re…

Monsters: Mikey Sano x Reader x Izana Kurokawa

“They ate me alive and left me for dead”
series summary: your grievous sin was Emma standing up for you to her brothers. And now you’re going to pay the heavy price for destroying their perfect family dynamic.
updates: wednesdays and fridays
Series masterlist
mood boards
series content warnings (read carefully): 18+, DARK CONTENT, Tokyo revengers AU, female reader, virgin reader, heavy smut, polyamory, Dark Impulse Mikey, Manipulative Izana, inaccurate/inconsistent university terminology, heavy angst with little comfort, betrayal, misogyny and sexism, emotional, physical and mental abuse, virginity loss, purity culture allusion, mental break, manipulation, gaslighting, sexual harrassment, dubious consent, noncon, drug, alcohol and substance misuse/abuse, extreme violence, use of weapons, torture, criminal activities, PTSD, paranoia, emotional incest, power imbalance, character death(s) (not reader), anal penetration, mention of self-harm, religious guilt and trauma, religious themes, vouyeurism, gangbang, masochism, sadism, hard kinks, strangulation (non sexual), psychological horror (more warnings to be added soon)
Chapter 1: Warning Signals
summary: being friends with emma sano is nice, until you get on the wrong side of the Sano brothers.
word count: 9k
cw: misogyny, alcohol mention, sex mention, rape mention, brief religious mention, reader is called a whore/slut, slutshaming, sexual assault, noncon to dubcon, public initimacy, fingering (fem recieving), dacriphilia, gaslighting, manipulation, mention of vomitting, victim blaming, destructive thoughts, mention of violence (towards reader)
Chapter 2: Shots Fired
summary: izana kurokawa decides he has to teach you a bitter lesson that you wouldn't forget any time soon
word count: 7.5k
cw: smoking, mention of drugs, brief description of child abuse, childhood trauma and sex work, violence (against both character and reader), emotional incest, night terrors, allusions to sex, mention and brief description of rape, asphyxiation (non sexual), manipulation, slut shaming, near death experience, sexual assault, noncon, oral (m.recieving), face and throat fucking, attempted murder
Chapter 3: The Lesser of Two Devils
summary: the two brothers realize that peace with emma is within their grasp, they just need your cooperation
word count: 12.3k
cw: character x character smut - cunnilingus, struggling with sexual attraction, angst, mention of assault, physical violence, slut shaming, misogyny, intrusive/dark impulsive thoughts of murder and rape, manipulation, gaslighting, objectification of reader, mental health struggles, masking, breaking and entering, smut -character x reader, reader is threatened with r*pe, dubious consent, making out, dry humping, cunnilingus (reader receiving), pussy job, terrible aftercare, religious themes and guilt, panty stealing.
Chapter 4: The Calm
summary: emma decided you needed a break from all the stress of life and takes you to her home for a vacation and for a moment, you forget that reality is often disappointing .
word count: 12.5k
cw: male masturbation, academic fatigue, misogyny, objectification, one mention of unwanted pregnacy, implied drugging, age gap relationship, fluff to heavy angst, minor character death, murder, mental break down, panic attack, gang related violence, gun violence, metions of drug related business (c*caine), dubious consent, slight manipulation, mutual masturbation, fingering (fem. receiving), jerking off, nipple sucking, praise kink, squirting, proper aftercare.
Chapter 5: Act on Dark Impulses
summary: you knew better than to trust mikey and izana. yet you fall for their plan hook, line and sinker and live through the worst night of your life.
word count: 22.8k
cw: Dark CONTENT, 18+, NONCON, SMUT, threesome (mfm), implied character x character sex and relationships, violence, misogyny, tinsy but of fluff, heavy angst, dark impulse! Mikey, manipulator Izana, mention of sex work, illegal prostitution, allusions to sex, choking (not reader), bullying, gaslighting, guilt tripping, peer pressure, multiple betrayals, use of alcohol and drugs, drugging, r*pe fantasy, implied orgies, implied cheating, torture, dry humping, reader gets slapped in the face, light bondage, deepthroating/throatfucking, fingering (vaginal & anal) f. receiveing, spanking, virginity loss, double penetration, anal sex, unprotected sex, sadism, dacryphilia if you squint, slut shaming, degradation, dehumanisation, rough sex, overstimulation, mind break, mild breeding kink, facials, sexual torture.
Chapter 6: The Closest you’ll ever get to being in Love
summary: things get sicker and twisted with the two brothers and Emma is none the wiser.
word count:
cw: coming soon
Chapter 7: Trials and Tribulation
summary: You learn the hard way what happens when you refuse to be their stress relief because of your important exams.
word count:
cw: coming soon
Chapter 8: Divine Intervention
summary: You are called home to bury your mother and learn that nothing has changed since you left.
word count:
cw: coming soon
Chapter 9: Lead Me not into Temptation
summary: emma notices that something isn’t right with you when you come visit her in the sano residence.
word count:
cw: coming soon
Chapter 10: Deliver Me from All Evil
summary: you’ve finally broken the cycle, but at what cost?
word count:
cw: coming soon
notes from monica: I do not endorse any of these behaviors or any crime committed in this fic. This is purely for entertainment and introspection, please read the warnings for the series and each chapter and in case I missed anything, please dm me. If you are part of the taglist and you cannot read this fic because of your mental health, please, please and please alert me, I will take your name off. Your mental health first before my notes.
Thank you to my mutuals and all my followers who have supported me throughout and to those who will read this fic and support me. Since I began this account, I’ve made wonderful friends and I’ve been encouraged to write beyond my fears. Thank you, especially Zaya (@manjibunny) ! The mood boards turned out well because of you and all our discussions about the fic helped me a whole lot!
Anyways, enjoy. Asks, reblogs and comments are highly appreciated. PLEASE I LOVE TO HEAR YOUR THOUGHTS AND THEORIES. It goes a long way to know what people think about my fics.
This work belongs to monica. do not copy or steal my work, do not promote my work on tiktok or twitter and do not use my work in any AI or chatgpt program.
divider made by the lovely: @mikeykuns
banners, moodboards, gradient texts were all done by monica.
series taglist (special thanks to): @honeybleed @manjibunny @reiners-milkbiddies @izanaki707 @rukiaslvr @ilovetwodmen @bbykoo-7 @tenjikusstuff4 @cockonoi @koffeenoe2 @kodzukein @lostsomewhereinthegarden @cashout-princess @aliyxh-o @kay-bear200 @iluv-ace @vixensbrainrotts @missgab @urmomsksk @sweeytheart @charcoal-xl @uradveragewhore @wcayaw @blueberry3muffin @haikyuusboringassmanager @diana-005 @perilous-pasta @kokoscutie @kannaaa015 @abadonkori @datura-inoxia @dolledupformanjiro @sugacor3 @marcoswhore @mechamadelargatixa @luminouslaybyrinth @iadoremik3y @lillystar2007 @miinnttyy @naomithenerdgirl @officiallyjaehyuns @kakusimp
Bolded can't be tagged. You can comment or send me an ask if you want to join the taglist.
#tokyo revengers x reader#tokyo revengers#tokyo revengers smut#mikey x reader#izana x reader#tw. dark content#tw. dark themes#read the warnings#masterlist post#monsters ♡#updates: wednesdays and fridays#thank you to all my moots
875 notes
·
View notes
Text
i hate being involved in mental health group chats in which i’m the only person with ASPD+NPD, because people will misuse terminology and talk to each other about experiences with guilt, remorse, empathy etc.
i don’t experience guilt, empathy or remorse, and your misuse of mental health terms just makes you look idiotic.
#actually mentally ill#clusterb#actually npd#npd#actually aspd#aspd#cluster b#actuallynpd#actuallyaspd#actually antisocial#actually narcissistic#narcissistic personality disorder#actually cluster b#antisocial personality disorder#cluster b personality disorder#narcissistic sociopath#psychopathy#psychopath#narcissists#narcissism#narc abuse isnt real#narc abuse isn't real#sociopath#sociopathic#narc posting#i don’t experience guilt or remorse#empathy#no empathy#no guilt#no remorse
32 notes
·
View notes
Text
Busting some misconceptions about narcissistic abuse because I can.
"Narcissistic abuse is no different from any other type of abuse."
Wrong. Narcissistic abuse can take the form of any other type of abuse, but the purpose for it and therefore the way it is perpetrated is very different.
"Narcissistic abuse is abuse perpetrated by a person with Narcissistic personality disorder (NPD)"
Incorrect. Anybody can perpetrate narcissistic abuse and there is no evidence to suggest people with NPD are more likely to be abusers than any other.
"Narcissism and NPD are the same thing."
False. Narcissism is a personality type defined by being self centered or vain to a fault. NPD is a personality disorder diagnosed by medical professionals and can be expressed in over 100 different ways.
People who are narcissistic can recover and change the fact that they're narcissistic. People diagnosed with NPD can recover, but cannot change the fact that they have NPD.
"There is no definition of narcissistic abuse."
True and false. While every expert who discusses narcissistic abuse may use different terminology to define it, the common theme is that the person perpetrating feels joy or satisfaction in harming, scaring or controlling their victim.
On my blog I define narcissistic abuse as "abuse perpetrated for the purpose of satisfying narcissistic delusion.
"People with NPD are narcissists."
Maybe, but mostly no. Some people who are diagnosed with NPD like to self identify as "narcissists" as a shorthand for their disorder. This is not the name of the disorder and you shouldn't refer to people with NPD as "Narcissists" as it's not an accurate or particularly universal term.
Some people who are not diagnosed with NPD like to self identify as narcissists to describe their personality type. It's important to distinguish between "narcissists" and "narcissistic abusers." A narcissistic abuser is not the same thing as a narcissist.
"Narcissism is the mental illness that causes abuse."
Untrue. No accredited mental health body today recognises narcissism as a mental health disorder and no practising mental health professional in good standing will say that there is a psychological disorder that causes abuse.
Perpetrating narcissistic abuse is a choice made by abusers, completely seperate from trauma or mental illness or their lived experience.
"People with NPD are offended by the term 'narcissistic abuse' so we should stop using it."
Recently people who identify as narcissists have taken umbrage against the term 'narcissistic abuse.' The reasons varying from an argument that the term 'narcissist' can never be separated from the disorder NPD, to the argument that people using the term are armchair diagnosing their abusers with NPD and further stigmatising the disorder.
The truth is the term 'narcissist' has been seperate from the disorder NPD since the disorder was first recognised in the DSM in 1980, and the solution to people using the terms "narcissist" and NPD interchangeably is to educate them, not ban the use of terminology that might potentially be misused altogether.
"If you can spot a narcissist you can evade abuse."
This is unfortunately false. Lots of online articles can promise you "10 ways to spot a narcissist" but usually all they're teaching you to do is to be wary of neurodivergent people. The truth is the only real way to evade abuse is to spot red flags for future abusive behaviour and know to get out before the abuse starts.
"There is no evidence that narcissistic abuse is real."
Aside from the stories of survivors of abuse and their families, or the loved ones of those who sadly didn't survive their abuser, all sharing commonalities in what happened to them, narcissistic abuse is well documented.
Therapists specialising in abuse recovery recognise narcissistic abuse and treat survivors of narcissistic abuse every day. Mental health educators discuss the psychology of the narcissistic abuser and the narcissistic abuse survivor in their dissertations or thesis papers and professionals study those papers to write resources like books and guides for those recovering from narcissistic abuse.
Narcissistic abuse is well documented and the general consensus in the psychology world is that it is real.
Feel free to drop any questions into my asks and I'll be happy to answer.
#narcissistic abuse#narcissistic abuse awareness#narcissistic personality disorder#narcissism is not npd#narcissism awareness#narcissism positivity#narcissism#narcissistic abuse is real
38 notes
·
View notes
Text
No one is going to like this but the solution to people misusing mental health terminology like hyperfixation & special interest is to bring back the concept & framing of Nerd Culture. Also the term "squee".
#look we really threw out the baby with the bathwater in the process of distancing ourselves from 2010s nerd culture#and now there's a terminology vacuum#which is why people are like ''im hyperfixating'' when they're actually. ahem. ''fangirling''#i know a lot of people have convinced themselves that the level of investment in fiction that people#with tumblr accts have is actually 'normal' and therefore you don't need to call it anything. but that is simply not true.#fandom and 'nerdiness' is Considerably more mainstreamed than it used to be#but it is still not a thing that 'everyone does now'. and so people are going to want words#like to specify that they are an above average level of invested in something#so we might as well direct them away from the dsm even if the alternative is Cringe or w/e
21 notes
·
View notes
Text
Addressing the recent anti-endo stance of the "Alterhuman Things!!" Discord server and misinformation.
The events were covered in more detail by a member of the server here.
Discrimination against endogenic systems isn't new. Especially on Discord. And not just in system or even alterhuman spaces. I've seen people talk about endogenic systems being witch-hunted and banned across Discord servers that have nothing to with systemhood or alterhumanity. This is just the latest in a long line of discriminatory servers.
Although it's especially frustrating here given the close links between the alterhuman and plural communities, and how both groups are often fakeclaimed and have our identities dismissed and invalidated.
Even more so when it's from a server which touts morals of respecting the beliefs of others, and claims to be friendly to anyone exploring their identity.

I'm not going to go over the entire controversy. I wasn't a part of it and can't confirm the full context. But I do want to address the inaccurate and defamatory statements made against endogenic systems.
There are two main points I want to address here. One is the psychological basis for the experience of endogenic multiplicity, while the other is on the terminology.
Current Theories on Non-Disordered Plurality.
While the owner of the server says they don't think people are "inherently invalid" in their experiences, they also suggest at the same time that the only way to have headmates is to have trauma-formed dissociative disorders.
This is untrue.
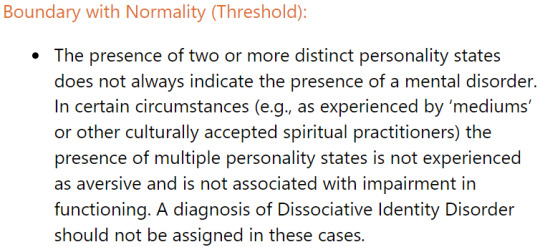
The ICD-11, which is the primary diagnostic manual around the globe and is created by the World Health Organization, describes alters as "personality states." It also makes it clear that having multiple "distinct personality states" is not inherently pathological.
In addition, the creators of the Theory of Structural Dissociation, the current lead theory in the origin of dissociative identity disorder, have also noted that being interpreted as spirits in mediumship may be "self-conscious dissociative parts of the personality."
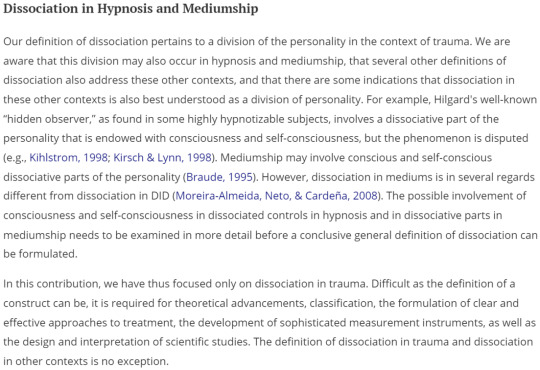
Both the creators of this theory and the World Health Organization acknowledge that other forms of multiplicity exist. Or at least could exist, in the latter case. Some forms of non-disordered psychological multiplicity is actively being studied, such as tulpamancy. This research is still ongoing but is believed by researchers to be a real psychological phenomenon.
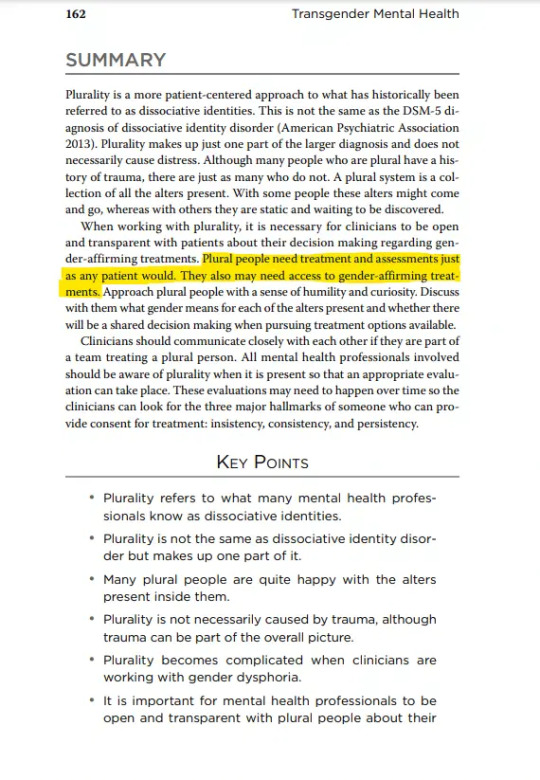
Non-disordered plurality has also been written about by psychiatrist Eric Yarbrough in his book Transgender Mental Health.
Who can call themselves plural?
The second big issue with the above post is claiming that calling ourselves plural is just a "misuse of vocabulary," which frankly, is even grosser to me than the pseudo-fakeclaiming.
So let's just set the record completely straight here: "Plural" is OUR word!
The first systems to refer to themselves as plural were doing so as a rejection of "multiple" and the medical model of multiplicity.
And there is a truth to that last line that holds true even today. That the power to name is the power to define and describe reality. It's why anti-endos try so hard to claim exclusive rights to terms they didn't create like "plural," "headmate," "fictive," "factive," and others that originated from non-disordered plurals.
These are attempts at stealing our power to name ourselves and define our experiences.
It's incredibly frustrating to me to be part of a community that coined terms to describe our experiences and then have people try to tell us that we're using the wrong vocabulary.
Additionally, Pluralkit, like Simply Plural and most other apps, spaces and organizations that use the term plural, is pro-endo and open to be used by any systems.
A Choice On Discrimination
We've established that experiences of non-disordered plurality is a real psychological phenomenon according to multiple psychiatrists and the World Health Organization. We've established that the term plural originated first with non-disordered plurals.
These facts are not in dispute.
What matters now is what you choose to do with this information. Not just the people who run this particular server, but those who run any servers with systems present.
There is an army of bigots out there who will demand that you discriminate and ban people for neurodivergences or their spirituality. If this were merely one server, I could have simply sent this in a DM and called it a day, but it's unfortunately an epidemic that constantly places people, often singlets, into these difficult positions where they feel they need to make these choices. Often with incomplete information if not just outright disinformation fed to them by anti-endos.
So this is it. You have the information necessary to make an informed decision. Your choice is that you can support a marginalized community that faces backlash often just for existing, a community with a strong overlap with the alterhuman community... you can uphold the values you claim to have of respecting people's beliefs and supporting those exploring their identities...
Or you can take the side of bigotry and discrimination. Join in those who want to discriminate against a marginalized community for our crime of existing.
In the end, the decision is yours to make.
Thank you for your time.
#syscourse#alterhuman#otherkin#otherhearted#therian#therian community#discord#therianthropy#otherkin community#endogenic#pro endogenic#plural#plurality#system#multiplicity#systems#plural system#endogenic system#pro endo#actually plural
54 notes
·
View notes
Note
Hey so I've had a peak at the inside of your server and the discussion of psychological alterhumans. I see that you edited one of your posts to say you're specifically open to spiritual alterhumans, but all of your other posts and even your bio still say it's open to all alterhumans. It's strange when a lot of members within your server talk about psychological alterhumans as if they're somehow not as valid as spiritual alterhumans, going so far to call them "kinnies". I don't think that behavior should be perpetuated.
I also noticed that when you edited that post, you edited out the word "serious" and replaced it with "spiritual". Was just really interesting to me after hearing some of the experiences from inside the server and seeing how members and staff talk about psychological alterhumans, talking about therians on TikTok calling them "KFF" or calling them fake, or even eluding to the mindset that all psychological alterhumans are somehow delusional and painting actual delusional folks as if they're bad.
I might be wrong about some things here, but definitely not all of them. If your server is exclusive to spiritual alterhumans, make that more clear, but it doesn't give you the go ahead to talk about psychological and delusional alterhumans in a bad light.
Hello! We are currently in a transitional phase to move from a server for all alterhumans to a server based in spiritual alterhumanity. As most of the staff are adults with jobs or in college, we may not have had time to fully update our advertisements and rules everywhere. Thanks for the heads up - we will make sure our verbiage everywhere reflects this. As for old posts others have reblogged, we unfortunately cannot edit those.
We do believe psychological alterhumans are valid! The issue comes when people have conflated psychological kin with things like copinglinks, cameo shifts, or flickers. We believe that words have meaning, and being kin means to identify as something, not with. People have asked if they can join mem jams with no memories, just to discuss fandom, or cut off conversations about identity to say they only find their kins relatable and nothing else. As for the use of the term “kinnies,” we use this term to refer to anyone, including ourselves. We are aware of the terms origins but prefer to both reclaim it and use it as shorthand, and it has not been used derogatorily.
As far as tiktok therians go, the discussion in question was centered around people claiming therian identity while only identifying furries or quadrobics enthusiasts. We believe conflating a genuine community like therians with a hobby is wrong and waters down the whole community.
Lastly, our server is for alterhumanity, not mental health. We are not equipped to help someone through a delusion, nor do we plan to encourage them. The point of a delusion is that it’s an aspect of psychosis that actively causes harm to the person believing it. That’s the difference between delusion and a personal belief. Additionally, many of the members here have been called delusional for our spiritual beliefs in other places, and would rather have a space to discuss our beliefs freely without them being medicalized as such. The IRL community is notorious as a whole for taking historically kin terminology and saying kin aren’t allowed to use them. They have also claimed kin can’t have memories or are only relating to their kintypes. We prefer to distance ourselves from people like this that refuse to acknowledge the past significance of terms and experiences in a community.
In short, we found people decide to misuse and abuse our welcoming of “serious” alterhumans and have narrowed the scope of the server to reduce stress on both staff and members. We aren’t saying serious psychological kin don’t exist, but rather that we don’t have the bandwidth to question every new member on basic definitions that we’ve seen get misused frequently.
-warren
7 notes
·
View notes
Text
Things that can all be true at the same time:
1. The dsm is not an objective source of truth. It is a diagnostic tool in which disorders are classified based on how certain symptoms tend to cluster together.
2. Psychiatrists suck.
3. Psychiatry as an institution cares much more about preserving the status quo than it does helping people.
4. Psychiatry can, will, and has been used as a means of oppression. (It's default mode tbh)
5. Self diagnosis, especially in the face of an oppressive mental health care system, is valid.
6. What classifies a 'mental illness' is highly subjective.
7. Societal systems (ex: captialism) can create and exacerbate mental illness.
8. Even in a perfect society mental illness will always exist.
9. Activists focus too much on language and not enough on what will materially help those who need it the most.
10. Mental health terminology matters-- the misuse and redefinition of certain words can have serious consequences for the ppl who those words were originally made for (ex: ocd + intrusive thoughts).
20 notes
·
View notes
Text
i keep seeing posts about how the term "boundaries" is constantly misused to inflict rules on other people when boundaries "only relate to rules for yourself" which..... isnt true according to things ive discussed with my therapist? like yeah the overuse of medical terms as get out of jail free buzzwords is bad but also strict black or white rulings of a concept in a tweet or two is also bad, especially since i have not seen a damn one of these come from a credible source, either a mental health professional or like, clinical terminology sources
CONCRETE EXAMPLE where i set a boundary with roommates that required behavior changes on their part that my therapist named specifically as a boundary when i described it:
dishes are the biggest point of contention in basically any living situation with multiple people. my previous roommates were really bad at doing them, in a way that resulted the kitchen being really gross if i hadnt just cleaned it. even after many requests to do basic things of "empty the sink trap of soggy food so it doesn't rot" and "dont hoard dishes long enough to grow an ecosystem" over m o n t h s, i got nowhere with dishes being done regularly in a way that didnt bother me
in the end it was so continuously upsetting that i told them to not do the dishes at all ever whatsoever, i would take care it. mind, i was the only one who worked out of the house while commuting via bus as a chronically ill person with severe fatigue and i was putting in an average of 50 hrs a week every week for werks on end at the time. me deciding to take this on was not done lightly, this was me recognizing that it was better and healthier for all of us for me to take on this one task. it would result in me being much happier in that living situation at no real cost to the other party other than maybe the dishes would stack up a bit if i was particularly exhausted one day, but things would get caught up within the week
this did not go down well despite my best efforts, and i would not be surprised if this black and white portrayal of what boundaries are influenced that. this nonsense went down over like six solid months and every single session i had with my therapist had him absolutely baffled because he couldn't think of a single thing i could have done better
i am not a mh professional i do not know the specific difference between "dont do this thing it upsets me" and "dont do this thing that 'upsets' me because i am controlling you", but the blanket statement of calling something like this a boundary is misusing the term is black and white thinking. i have bpd, ive done some dbt about it and the first thing they teach you is how to spot black and white thinking because it us incredibly mal adaptive and *really fucking dangerous* and this specific trend is going to be taken advantage of by abusers just as much as coopting the use of "boundaries" to justify their behavior
tldr "boundaries are never about other people's behavior" and "you can't do xyz thing because it violates my boundaries" are two sides of the same abusive coin. people who have put in the work in a tangible and meaningful way, who are able to examine their motives and give grace to other people within their boundaries, can recognize that boundaries are a spectrum, like everything with social relationships and mental health in general
#mochi rambles#listen work has been absolute bullshit#like ungodly amounts of bullshit#i am so deep in bullshit i do not know how to deal with i have spent most of the eight days ive been back#absolutely screaming in a very literal sense#please note i returned last week after spending a week in the hospital because i almost died#it has not been a good month and i am fucking tired of these fucks who read one article about a thing#wnd feel confident making bullshit blanket statements#that then go viral#because people dont know the meaning of nuance#surprise!!!! turns out healthy approaches to interpersonal relationships have a lot of nuance#almost like people are individuals with individual needs qnd individual thoughts and individual histories#that impact how they interact with others and how they perceive others intents in their interactions#this is why black and white thinking is dangerous#more or less#im not a professional this is just what ive gathered from seeing mh pros pretty consistently for a decade#anyway im so fucking salty in general rn#but also specifically salty that i lost two friends i really cared about because their hang ups#resulted in my very genuine attempts to maintain a good relationship#being veiwed as abuse tactics#leading to them spreading slander to the same effect among other friends#who have subsequently dropped me#while me and my therapist over here in my standing bi werkly appointments are like wtf#and there has been so much of everything else that i have not had the brain to decide#if its worth the effort to try and convince people im not the bad guy#....... man i do not have enough time for all the therapy appointments i woukd really like to have#because fuck this year has been Something
5 notes
·
View notes
Text
May, Tom. “Why the Creative Industry Needs to Start Talking about Men’s Mental Health.” Creative Boom, 18 Nov. 2022, www.creativeboom.com/features/mens-mental-health-and-the-creative-industries/. [Accessed 5 Mar. 2024.]
creative industry needs to start talking about mens mental health:
international mens day offers the opportunity to promote positive male role models, focus on male mental health and wellbeing, improve gender relations
what are agency leaders doing to challenge these issues:
feeling lost: most men no longer have jobs or are in roles where they have the need to be physical and strong and yet this expectation of them is still occuring. but there is an inyternal need to be the protector, breadwinner and alpha. because the expectation of men is shifting away from those stereotypes, some men are feeling lost. 3/4 of suicides a year are men, and suicide is the biggest cause of death for men under 50 and this feeling may be playing a part in that
internalising issues: men tend to bottle things up. one thing they have observed is thatmen dont tend to talk to one another about their issues or see each other 121, it tends to be more in groups because.
finding work life balance
being comfortable in your skin: be comfortable in yourself and your failings
finding focus: men tend to enjoy doing activities which create more pressure, danger and demands focus, which is why we see men doing more extreme sports like snowboarding. extreme sports can take up so much mental focus that you stop thinking about other things and this can be seen as a form of mindfulness because all other thoughts leave your head.
community efforts: this doesnt just have to be by the individual, we should be encouraging everyone to do this
this article has helped me understand both men in creative roles as well as the more broader experience of being a man. i think it has the potential to lend itself well to my project because i can understand other issues they might be facing and how to encourage a better dealing of those emotions and situations.
It has made me think about how i can look at the use or misuse of alcohol and how i can design to encourage change for good. this might be through partnership with a movement like dry january or international mens day.
Terminology used in this article also lends itself well to my project which unexpectedly sparked ideas. for example "bottle up emotions" lends itself well to the idea of alcohol and drinking which is something i want to come back to further down the line of this project.
0 notes
Note
Was with you until you started tossing around “ableist” completely inanely sigh gotta put that word on the shelf as well
do you think misusing mental health terminology to make jokes at our expense isn’t ableist?
28 notes
·
View notes
Text
bored. here are some opinions ppl on tumblr give a shit about
shipping: i'm not a cop but i will give you shit and not want to hang around you if you ship incest or adults with children. same with certain other ships like shipping a bigot with someone they're bigoted towards. ships where one of the characters turns 18 during the course of the story (i.e. light x l, narumayo) or the characters being related is a spoiler (i.e. cassandra x rapunzel, reylo) is fine but you're on thin ice.
literally any lgbt identity shit: i do wonder if we're falling back into microidentity shit from 2014 but just a bit more edgy about it especially considering society's gotten more anti-lgbt lately. it's a little individualist but western society is also individualist so i can't fully complain. i think solidarity is really important though so take some time to REALLY reflect upon that. not just "we're all lgbt we're a family" "let's stop fighting and start making out" like actually think about what you share with like. gay men, trans women, etc. <- examples for me
cringe culture: still alive to me if they're normie cringe. i watch baby shows i can call you cringe if you're obsessed with sonic. get into a more esoteric furry game like detective gallo (not the right genre i dont play video games).
sex/kink positivity: sex and kink are kind of inherently neutral. don't act like they're a unstoppable force of universal good don't act like they're pure evil. something to be said about getting off to something and being normal vs googling the bomb that kills all women.
mental health: psychiatry is fucking barbaric we're still in the dark ages. we have a very limited array of ways to actually deal with it and everything else is either a scam or too experimental and clinicians are unwilling to look further into it. mental health systems do serve those and power and can help you if you're a normie, but it's sort of becoming worshipped as the new family. you can't really question your therapist, which makes it easier to hurt you. that's also why i don't like seeing anything as a universal good.
misusing mental illness terminology: people act like this is an act of ableism instead of it being people not knowing shit fuck about psychology. XD idc if you do it.
punitive justice: world's most useless thing. you need to admit that you're a vengeful soul who simply doesn't want to see the people who hurt you again. idk how a restorative system would work in full, but starting from there i think is a good idea.
punitive justice but strictly stupid revenge schemes: funny. i'll allow them
callout posts: straight up ocd triggering and i could never make one. a lot of them are shit that shouldn't be public internet drama (stupid) or shit that shouldn't be public internet drama (actual fucking crimes). callouts are def a weird line when it comes to punitive justice because is it a punishment to tell everyone what you've done? it's like are rumors a punishment for being too close to someone in middle school? but at the same time it's undeniable there's a certain morality culture that causes people to leave you for dead about it.
1 note
·
View note
Text
Navigating the Complex Landscape of Billing for Behavioral Health Services
In the consistently developing field of healthcare, billing for behavioral health services and mental health services presents extraordinary difficulties that require a nuanced comprehension of both clinical practices and repayment structures. As experts endeavor to give fundamental mental health care, the complexities of billing can sometimes become an obstruction. This article means to reveal insight into the critical parts of billing for behavioral health and mental health services, offering bits of knowledge to specialists, heads, and healthcare experts.
Grasping the Scene: Behavioral Health Services
Billing for behavioral health services incorporates a wide range of care, going from treatment and directing to additional concentrated medications for people confronting mental health challenges. Behavioral health services frequently address conditions, for example, uneasiness, sadness, substance misuse, and other mental problems. While exploring the billing system, specialists should know about the particular codes and guidelines related to these services.
The Role of Legitimate Documentation in Billing for Mental Health Services
A basic part of fruitful billing for mental health services lies in exhaustive and exact documentation. Mental health experts should fastidiously record patient evaluations, treatment plans, and progress notes to legitimize the need for the offered types of assistance. Legitimate documentation guarantees adherence to moral norms as well as lays out a strong starting point for billing purposes.
Coding and Repayment
In the domain of billing for mental health services, exact coding is vital. Mental health experts utilize different Current Procedural Terminology (CPT) codes to address the particular services delivered during a meeting. It is urgent to keep up to date with updates to coding frameworks to try not to charge disparities. Furthermore, understanding the subtleties of repayment, including insurance contracts and charge plans, is fundamental for boosting income while giving quality consideration.
Exploring Insurance Challenges in Billing for Behavioral Health Services
Protection assumes a critical part in the repayment cycle for behavioral health services. Numerous mental health experts experience difficulties connected with pre-approvals, inclusion restrictions, and guarantee dissents. Effective billing for behavioral health services includes proactive correspondence with protection suppliers, confirmation of inclusion, and support for fundamental services to guarantee fair repayment.
Integrating Telehealth into Billing for Behavioral Health Services
The ascent of telehealth has transformed the conveyance of mental health services, giving more noteworthy openness to patients. Nonetheless, billing for telehealth services presents its arrangement of contemplations. Specialists should find out more about unambiguous telehealth CPT codes and comply with guidelines administering virtual help repayment. Exploring the crossing point of innovation and mental health billing is vital to adjusting to the developing scene of healthcare.
Difficulties and Opportunities in Billing for Mental Health Services
While presents difficulties, it likewise makes the way for open doors for development. Cooperative efforts inside the local healthcare area, continuous instruction on billing practices, and support for strategy changes are fundamental parts of tending to these difficulties. As the scene keeps on developing, experts should adjust and effectively take part in conversations that add to more straightforward and productive billing processes.
To Sum It Up
All in all, billing for behavioral health services and mental health services requires a diverse methodology that consolidates clinical skills with an exhaustive comprehension of billing guidelines. By focusing on legitimate documentation, remaining informed about coding and repayment changes, and embracing mechanical arrangements, mental health experts can explore the intricacies of billing while at the same time guaranteeing the conveyance of fundamental consideration to those out of luck.
0 notes
Text
Understanding The Stages Of Substance Use Disorders
Table of Contents
Key Takeaway:
Defining Substance Use Disorders: Understanding the Terminology
Types of Substances: Common Categories and Their Effects
The Stages of Substance Use Disorders: Progression and Warning Signs
Experimentation: Trying Drugs and Alcohol for the First Time
Regular Use: Frequent Consumption of Substances
Risky Use: Engaging in Dangerous Behavior while Under the Influence
Harmful Use: Damage to Physical, Mental, and Social Health
Dependence: Physiological and Psychological Dependence on Substances
Addiction: Loss of Control and Compulsive Use of Substances
Treating Substance Use Disorders: Options for Recovery
Detoxification: Withdrawal Management in a Safe Environment
Behavioral Therapy: Changing Thoughts, Emotions, and Behaviors
Medication: Reducing Cravings and Withdrawal Symptoms
Support Groups: Peer Support and Accountability
Preventing Substance Use Disorders: Strategies for a Healthy Lifestyle
Education and Awareness: Understanding the Risks and Consequences
Early Intervention: Addressing Substance Use Issues at an Early Stage
Access to Treatment: Overcoming Barriers to Recovery
Social Support: Building Positive Relationships and Community Support.
Take the Leap Towards a Renewed Tomorrow
5 Well-Known Facts About Understanding the Stages of Substance Use Disorders: From Experimentation to Addiction:
FAQs about Understanding The Stages Of Substance Use Disorders: From Experimentation To Addiction
What are the different stages of substance use disorders?
How do I know if I am in the experimentation stage?
What is regular use?
What is risky use?
What is dependence?
What is addiction?
Key Takeaway:
Understanding the stages of substance use disorders can help individuals and their loved ones identify warning signs and take action before addiction takes hold.
The stages of substance use disorders progress from experimentation to addiction, with each stage characterized by specific warning signs and behaviors.
Treating substance use disorders often requires a combination of detoxification, behavioral therapy, medication, and support groups, and prevention strategies should focus on education, early intervention, access to treatment, and social support.

Defining Substance Use Disorders: Understanding the Terminology
Defining Substance Use Disorders: Understanding the Terminology is crucial to recognize the stages of addiction. It is essential to understand that substance use disorders are a condition where an individual continues using drugs or alcohol despite experiencing negative consequences in their personal, social, and professional life. The most common forms of substance use disorders include alcohol use disorder, nicotine addiction, and drug abuse.
It works by identifying the patterns of behavior that indicate a person is suffering from substance use disorder. Generally, these patterns emerge when individuals begin using substances in ways that are detrimental to their health or well-being. They continue using despite social or interpersonal problems, developing physical tolerance and experiencing withdrawal symptoms.
The terminology can be broken down into valuable information obtained about each type of substance misuse disorder, including its causes and symptoms. People who suffer from substance abuse usually have difficulty controlling their impulses to seek pleasure from drugs or psychoactive agents. Such issues often result in changes in brain circuits related to judgment, decision-making capabilities, and motivation.
Historically speaking, Defining Substance Use Disorders: Understanding the Terminology has been a contentious topic due to inconsistencies in language and terminology around addiction. Previously referred to as ‘substance abuse’ or ‘harmful habits,’ people now recognize it as a chronic illness requiring medical treatment across different jurisdictions worldwide.
Types of Substances: Common Categories and Their Effects
Types of substances refer to different categories of drugs that people use. Substance abuse is a significant public health problem in the world today, and it affects people from all walks of life. Understanding the types of substances and their effects is key to preventing substance use disorders and seeking treatment when necessary.
Types of Substances: Common Categories and Their EffectsSubstance CategoryExamplesEffectsStimulantsCocaine, Methamphetamine, Nicotine, Ecstasy, ADHD medications (Ritalin, Adderall)Increased energy and alertness, decreased appetite, elevated mood, increased heart rate and blood pressureDepressants or SedativesAlcohol, Barbiturates (phenobarbital), Benzodiazepines (Xanax, Valium), Opioids (Heroin, Fentanyl)Euphoria or relaxation, slowed respiration and heart rateHallucinogensLSD (Acid), Psilocybin mushrooms (“Shrooms”), Mescaline; Designer cannabinoids (“Spice”, “K2”) , KetamineAltered reality perception or senses (sight, smell etc.)Cannabis/MarijuanaCannabis sativa plant being smoked or consumed through ediblesEuphoria followed by slow thinking speed;InhalantsAerosol sprays or volatile liquids such as paint thinners, cleaning fluids etcA sense of “drunkenness” with drowsiness
Stimulants are drugs that increase energy levels and alertness in users. They can cause rapid heartbeat rates and high blood pressure levels in some people. Depressants or sedatives slow down brain activity which can lead to feelings of drowsiness or euphoria in users. Hallucinogens alter perceptions like sensory experiences making users feel separated from reality.
A true fact is that drug addiction has increased globally by 30 percent in the past decade, and opioids are the most commonly abused substances worldwide. (source: World Health Organization)
Now that we have discussed types of substances let’s dive into the progression of substance use disorders from experimentation to addiction. As humans, we all crave something, and many times, it can be the illusion of being in control that turns a curious individual experimenting into a chronic addict with enormous physical and mental health challenges.
The Stages of Substance Use Disorders: Progression and Warning Signs
Substance use disorders develop over time, with each stage featuring its own unique warning signs and risks. In this section, we’ll dive into the stages of substance use disorders and explore the progression from experimentation to addiction. We’ll examine the different stages of substance use, including:
Experimentation
Regular use
Risky use
Harmful use
Dependence
Addiction
and discuss the warning signs for each stage. It is essential to recognize the early stages of substance use disorders to prevent further development and seek help before it’s too late.
Experimentation: Trying Drugs and Alcohol for the First Time
Experimentation: Trying Drugs and Alcohol for the First Time is a stage in the progression of substance use disorders that involves the initial introduction to drug and alcohol consumption. Many young people, sometimes pressured by peers, experiment with drugs and alcohol as they seek new experiences or try to fit in. Others may be curious or have heard positive things about using these substances. Regardless of the reason, Experimentation is often the first step towards addiction.
During Experimentation, individuals may try drugs or alcohol once or twice out of curiosity but then return to their normal lives without any significant consequences. In some cases, however, Experimentation may lead to more frequent use and eventual addiction. Individuals who continue to use drugs or alcohol beyond Experimentation often experience a sense of exhilaration and relaxation that can lead them to crave more.
While trying drugs or alcohol may seem like an exciting adventure at first, it’s essential to understand that experimentation does carry some real risks. For example, there is always the possibility of overdose or negative side effects from mixing different substances. Moreover, engaging in risky behavior while under the influence can lead to serious accidents or legal problems.
If you are considering experimentation with drugs or alcohol, think carefully before taking action. Instead of giving in to peer pressure, consider alternative ways to socialize and have fun that don’t involve substance use. Remember that your health and safety are paramount considerations when trying new things – don’t risk them just for a momentary thrill.
Regular Use: Frequent Consumption of Substances
Regular use refers to the frequent consumption of substances, either drugs or alcohol, in which an individual starts to develop a pattern of regular and repeated usage. Initially, the substance may be used occasionally, but with time it becomes a regular part of daily life. The individual may start consuming the substance for various reasons like anxiety, depression, boredom or simply to experience pleasurable feelings.
The frequent consumption of substances leads to chemical changes in the brain and the body develops a tolerance to the substance. As a result, users need more of the substance to feel its effects – this leads to drug dependence or addiction. Regular users will often begin seeking out these substances more frequently or in larger amounts than before.
Regular use also affects individuals differently; some people can control their consumption while others cannot. This is because genetics plays an essential role in determining whether an individual is prone to addiction or not. Additionally, environmental factors such as home environment and peer influence can also contribute to regular use.
There are different stages in substance use disorders that are characterized by progressive changes in behavior and physical health. One such stage is Regular Use and if left untreated progress into riskier behaviors with greater consequences.
Risky Use: Engaging in Dangerous Behavior while Under the Influence
A dangerous outcome of substance use disorders is the engagement in risky behavior while under the influence. This can include activities such as driving under the influence, unprotected sex, or even criminal behavior.
When a person uses drugs or alcohol, their judgment and decision-making abilities are significantly impaired. They may feel invincible and be more likely to take risks they wouldn’t otherwise. Additionally, some substances can increase aggression or decrease inhibition, making it easier to engage in dangerous behavior.
Risky use can have severe consequences for both the individual and those around them. In addition to legal repercussions, individuals may suffer from injuries, sexually transmitted infections, or other health problems. It can also strain relationships with loved ones or lead to social isolation.
Harmful Use: Damage to Physical, Mental, and Social Health
Harmful use of substances can lead to damage in various areas of our health, including physical, mental, and social aspects. It’s important to understand that harmful use doesn’t just refer to addiction or dependence on substances, but also includes any usage patterns that adversely impact our well-being.
This kind of harm can occur due to the direct effects of substances on our bodies or from the secondary effects such as impaired decision-making abilities or negative consequences related to substance use. Harmful use can cause physical harm such as liver damage, infections, injuries, and a weakened immune system. It can also lead to mental issues like depression, anxiety, psychosis, and memory impairment.
Harmful use also affects our social health since it can cause difficulties in maintaining relationships with family and friends. The impact of harmful substance use is not limited only to the user but extends widely to those around them too. Apart from that, it can result in financial problems that may strain relationships among people.
Pro Tip: If you find yourself struggling with harmful use or know someone who does, seek professional help immediately. There’s no shame in asking for assistance when dealing with substance-related concerns no matter how minor they might seem at first glance.
Despite initially providing a sense of fun and relief for users sometimes browsing to explore new things leads towards dependence on Substances; which prompts us towards the next heading ‘Dependence: Physiological and Psychological Dependence on Substances‘.
Dependence: Physiological and Psychological Dependence on Substances
Dependence: Physiological and Psychological Dependence on Substances is a commonly heard term when it comes to substance use disorders. The dependence that individuals develop on these substances is of two types- physiological and psychological.
Physiological dependence occurs when the body becomes accustomed to the presence of a particular substance in the system. As a result, when this substance is withdrawn abruptly, the body experiences physical symptoms like nausea, tremors, seizures or sweating. On the other hand, psychological dependence occurs due to a shift in an individual’s thought process whereby they feel like they cannot function properly without consuming their substance of choice.
Several factors play into how both physiological and psychological dependence on substances work. For instance – the person’s age, gender, weight or genetic disposition can impact their likelihood of developing an addiction. Additionally, using drugs to alleviate mental health conditions like anxiety or depression can also increase one’s risk for dependency as well.

Addiction: Loss of Control and Compulsive Use of Substances
Addiction: Loss of Control and Compulsive Use of Substances is a state where an individual’s dependency on certain substances has reached the point where they feel powerless to control it. It is characterized by a constant urge to use drugs or alcohol despite adverse consequences.
In exploring Addiction: Loss of Control and Compulsive Use of Substances, let us examine its five significant components:
Habitual or repeated drug use can lead to addiction so that there is a need for greater amounts over time to produce the same effect, known as tolerance.
Despite recognizing negative consequences, such as health hazards or relationship problems or job loss due to substance abuse, one continues using the substance.
Behavioral changes due to drug intake affect relationships with friends and family; for instance, being secretive about one’s habit or having an agitation when there is no access to the drug.
Individuals with addiction usually become preoccupied with acquiring their substance of choice when it is not available.
Stopping substance use may cause withdrawal symptoms like anxiety, insomnia, depression and in severe cases seizures.
The complexity of Addiction: Loss of Control and Compulsive Use of Substances lies beyond reinforcing effects but also relies on psychological elements such as emotion regulation deficits and compulsivity features. It includes various genetic and environmental factors like trauma at early life stages contributing to developing addiction.
Treating Substance Use Disorders: Options for Recovery
In this section, we’ll explore different options for recovery that can help individuals break the cycle of addiction. We’ll start by discussing detoxification, which provides a safe environment for managing withdrawal symptoms. Next, we’ll delve into behavioral therapy, which seeks to change the underlying thoughts, emotions, and behaviors that contribute to addiction. We’ll also look at medication-assisted treatment, which can help to reduce cravings and ameliorate withdrawal symptoms. Finally, we’ll discuss the benefits of support groups, which offer peer support and accountability through the recovery process.
These options, when used alone or in combination with each other, can greatly increase the chances of success in recovery.
Detoxification: Withdrawal Management in a Safe Environment
Detoxification or “detox” refers to the process of removing toxic substances from the body. In the context of substance use disorders, detoxification specifically means managing withdrawal symptoms in a safe and controlled environment. This is an important first step in treating addiction because withdrawing from certain drugs can be dangerous or even life-threatening.
Detoxification works by gradually reducing the amount of drugs or alcohol in a person’s system while managing withdrawal symptoms. This process may involve medication-assisted treatment (MAT) to ease symptoms like nausea, tremors, or seizures. MAT can also help prevent relapse by reducing cravings and other psychological symptoms.
The goal of detoxification is to help individuals safely manage withdrawal and stabilize their physical health so they can move on to further treatment options. But it’s important to note that detox alone doesn’t address the underlying issues that contribute to addiction, such as trauma or mental health problems.
In some cases, people may attempt to detox on their own at home, but this can be dangerous – especially when withdrawing from certain drugs like benzodiazepines or opioids. Withdrawal from these substances can cause severe physical symptoms and might require medical attention. That’s why professional medical supervision is crucial for safe and effective detoxification.
Behavioral Therapy: Changing Thoughts, Emotions, and Behaviors
Behavioral Therapy: Changing Thoughts, Emotions, and Behaviors is an essential part of treating substance use disorders. It focuses on changing negative thoughts and emotions surrounding addiction to promote positive behaviors that lead to recovery.
This type of therapy works by identifying and addressing the root causes of addictive behaviors, such as stress, trauma, or mental health issues. A therapist will work with a patient to develop coping mechanisms and alternative solutions to combat triggers and cravings.
Research has shown that Behavioral Therapy is incredibly effective in reducing drug use, improving mental health outcomes, and enhancing overall quality of life for those struggling with addiction. By addressing negative thought patterns and emotional distress head-on, individuals can build a stronger foundation for long-term sobriety.
Did you know that Cognitive Behavioral Therapy (CBT) is often used in conjunction with other forms of therapy for optimal results? This combination approach has been proven in studies to be more effective than singular approaches.
Medication: Reducing Cravings and Withdrawal Symptoms
Medication: Reducing Cravings and Withdrawal Symptoms is a crucial aspect of treating substance use disorders. Medications can be useful in different stages of addiction, ranging from reducing cravings to helping with withdrawal symptoms during detoxification.
In the first point, Medication-Assisted Treatment (MAT) can help reduce drug or alcohol cravings by blocking certain receptors in the brain that trigger these urges. It can also alleviate anxiety and depression associated with addiction. Second, medications like methadone or buprenorphine can manage opioid withdrawal symptoms effectively for individuals recovering from opioid use disorders. Third, Antabuse is a medication used to treat alcoholism by making patients ill if they drink while taking the medication.
In addition to traditional medications, emerging treatments such as Deep Transcranial Magnetic Stimulation (dTMS), which uses magnetic pulses to stimulate nerve cells in the brain, shows promise in treating substance use disorders.
Interestingly, some medications previously used for other illnesses have been found to be useful in treating substance use disorders. For example, Naltrexone was initially used to treat opioid addiction but has been found effective in treating alcohol dependence as well.
With so many options available to combat substance abuse and addiction, it’s important to seek the advice of professionals regarding treatment options that are suitable for individual needs.
Support Groups: Peer Support and Accountability
Support groups are vital when it comes to substance use disorder recovery because they provide both peer support and accountability. The power of having a support system made up of people facing similar struggles is invaluable, and the accountability factor keeps individuals on track towards their goals.
Here are six important points to consider regarding Support Groups: Peer Support and Accountability:
Peer support means receiving encouragement, guidance, and advice from individuals who understand the challenges you’re facing.
Being accountable to oneself can be difficult; being accountable to a group means stronger motivation to follow through.
Many support groups use a 12-step program that creates an environment of camaraderie and shared experiences among its members.
Research shows that people who participate in support groups have better substance use treatment outcomes than those who don’t.
There are countless types of support groups available, including faith-based programs, wellness-focused meetings, and gender-specific groups.
Many rehabilitation centers offer access to support groups for ongoing care after treatment.
Peer support involves not just emotional help but practical assistance with issues like transportation or childcare needs so that addicts aren’t derailed from attending meetings or therapy sessions. It also helps break down the feeling of isolation many experience when dealing with substance abuse disorders on their own. During group meetings, participants learn about new strategies for coping mechanisms and develop new tools for handling triggers that contribute to substance use.
Now that we know what ‘Support Groups: Peer Support and Accountability’ entails, let’s explore how to prevent substance use disorders with strategies for a healthy lifestyle. So, You think you know all there is to know about addiction? Think again.
Preventing Substance Use Disorders: Strategies for a Healthy Lifestyle
In this part of the article, we focus on strategies for living a healthy lifestyle and preventing substance use disorders. Here, we’ll discuss various sub-sections that provide a comprehensive understanding of preventing substance use disorders, such as the importance of:
education
early intervention
access to treatment
social support
By implementing these strategies, we can create a culture that prioritizes prevention and positive support, and ultimately, reduce the prevalence of substance use disorders in our communities.
Education and Awareness: Understanding the Risks and Consequences
Understanding the risks and consequences of substance use is essential for preventing substance use disorders. Education and awareness can be an effective strategy to create a healthy lifestyle and prevent addiction.
Education and awareness work by providing knowledge about the effects of substance use on physical and mental health, relationships, work-life, and society. When people understand the risks, the reasons to avoid or stop using substances become more apparent. They are more likely to make informed decisions about their behaviors.
Additionally, education and awareness can reduce stigma around substance use disorders. It can encourage people to seek help if needed without feeling ashamed or embarrassed. Furthermore, it can facilitate communication between parents, teachers, healthcare providers, peers, and individuals struggling with addiction.
According to a study published in the Journal of Substance Abuse Treatment, school-based interventions that focused on educating students about alcohol and drug abuse had a significant impact on reducing substance use among adolescents.
Did you know that only 24% of people who need treatment for substance use disorders receive specialized care? It highlights the need for education and awareness at all levels of society.
“Prevention is better than cure,” but addressing substance use issues at an early stage can save lives. In my next section segment ‘Are you or someone you know struggling with Addiction? Early Intervention Can Save Lives.’ let’s learn how early intervention strategies like screening, brief intervention, referrals to treatment (SBIRT), mindfulness techniques, cognitive-behavioral therapies (CBT), motivational interviewing(MI), contingency management(CM) can benefit individuals dealing with addiction.
Early Intervention: Addressing Substance Use Issues at an Early Stage
Intervening early in addressing substance use issues has proven to have a positive impact on reducing the risk of individuals developing substance use disorders. It involves identifying the signs and risk factors of drug or alcohol use at an early stage, and implementing measures to prevent them from becoming habitual.
Early intervention works by providing education and support to individuals before they develop an addiction. It raises awareness about the harms of substance abuse and helps individuals make informed decisions about their choice of using drugs or alcohol. By intervening early, it becomes easier for individuals to overcome peer pressure and withdrawal symptoms. When family members or healthcare providers intervene, they can help create a supportive environment that empowers the individual to seek treatment if needed.
One valuable aspect of early intervention is its ability to recognize risky behavior patterns that may not be immediately visible to others. Often, young adults experiment with drugs or alcohol as a coping mechanism during stressful life circumstances, which can escalate into addiction. Early intervention provides an opportunity to address these underlying issues and offer alternative coping mechanisms.
Access to Treatment: Overcoming Barriers to Recovery
Access to Treatment: Overcoming Barriers to Recovery is a crucial component of preventing substance use disorders. It refers to the accessibility and availability of evidence-based treatments for individuals struggling with addiction. This includes both behavioral therapies and medication-assisted treatment options.
Access to treatment is important because it can help individuals overcome the barriers that prevent them from seeking help. These barriers can include stigma, lack of insurance coverage, limited resources in rural or underserved areas, and personal beliefs about addiction and recovery.
One of the ways access to treatment works is by providing education and awareness about addiction and recovery. When individuals understand that substance use disorders are a chronic condition that require long-term management, they are more likely to seek out professional help. Additionally, connecting individuals with support groups or counseling services can play an important role in overcoming stigma and creating a sense of community.
Research has also shown that medication-assisted treatment (MAT) for opioid addiction is highly effective at reducing substance use and improving outcomes like employment and social functioning. Access to MAT can be limited by regulations, healthcare provider bias, or insufficient funding for comprehensive care programs.
Social Support: Building Positive Relationships and Community Support.
The role of social support in preventing substance use disorders is a topic that needs to be discussed at length. Building positive relationships with individuals who provide emotional, informational, and instrumental assistance can play a significant role in reducing the risk of addiction. It not only provides one with reassurance but also creates a sense of community support.
Social Support: Building Positive Relationships and Community Support works by providing individuals with meaningful relationships that promote healthy behaviors. People who are isolated or lack social support are more likely to experiment with drugs as it can ease their anxiety and provide comfort. In contrast, people with strong social networks have better coping mechanisms to deal with stressors in life; thereby dependence on substances decreases. Thus, building positive relationships is essential for preventing substance abuse.
It would interest you to know that social support has been found to be effective in reducing nicotine cravings amongst teens who were trying to quit smoking (Pediatrics, 2008). This study tells us the importance of the role of social support in overcoming addiction.
Research shows that social support networks come from various sources such as family members, friends, religious groups, workplaces, volunteering organizations or clubs. These individuals have a powerful influence on our decision making towards drug use. Family environment plays an important role too — families who create an open and supportive space for communication are less likely to see their children suffer from addiction problems.
Take the Leap Towards a Renewed Tomorrow
In understanding the intricate stages of substance use disorders, one gains not only awareness but the power to seek timely intervention. The journey to recovery begins with knowledge and an empowering community by your side. If you or a loved one is navigating this challenging path, remember: The Nestled in Las Vegas is here to guide, support, and facilitate transformative healing. Don’t wait; reach out today and take the first step towards a brighter, substance-free future.
5 Well-Known Facts About Understanding the Stages of Substance Use Disorders: From Experimentation to Addiction:
✅ Substance use disorder is a complex condition that can be influenced by genetic, environmental, and psychological factors. (Source: National Institute on Drug Abuse)
✅ Substance use disorder develops over time, often starting with experimentation and occasional use of drugs or alcohol. (Source: Mayo Clinic)
✅ Continual use of drugs or alcohol can lead to physical dependence and tolerance, which can make it difficult to quit without professional help. (Source: American Addiction Centers)
✅ Substance use disorder can have severe consequences on an individual’s health, relationships, and ability to function in day-to-day life. (Source: Substance Abuse and Mental Health Services Administration)
✅ Effective treatment for substance use disorder often involves a combination of medication, therapy, and support groups. (Source: National Institute on Drug Abuse)
FAQs about Understanding The Stages Of Substance Use Disorders: From Experimentation To Addiction
What are the different stages of substance use disorders?
The stages of substance use disorders are: experimentation, regular use, risky use, dependence, and addiction. Each stage is characterized by different levels of use and patterns of behavior.
How do I know if I am in the experimentation stage?
If you are in the experimentation stage, you may be trying a substance for the first time or trying a new substance. Your use is limited and sporadic, and you are not experiencing any negative consequences from your use.
What is regular use?
Regular use occurs when a person begins to use a substance more frequently, often on a daily or weekly basis. This stage is characterized by the need to use the substance to feel normal or to cope with daily life.
What is risky use?
Risky use is when a person begins to use a substance in a way that increases their risk for negative consequences, such as using more than they intended or combining substances. This stage often leads to problems in various areas of a person’s life, such as work, relationships, and health.
What is dependence?
Dependence occurs when a person develops a physical and/or psychological dependence on a substance. They may experience withdrawal symptoms when they try to stop using the substance and require more of the substance to achieve the same effects.
What is addiction?
Addiction is the most severe stage of substance use disorders, characterized by compulsive drug seeking and use despite negative consequences. People in this stage may lose control over their use and experience significant impairments in various areas of their life.
0 notes
Last Seen Blogs

jamesrodrigeuz
James Rodriguez


ella-se-vuelve-loca
Which Lane Am I Feeling Today?

ivelllll
i v e l (COMMS UP)

dakhoday
Dakho's day