#"Bipolar disorder symptoms"
Text
10 Common Symptoms of a Mental Breakdown
10 Common Symptoms of a Mental Breakdown
Introduction
Feeling overwhelmed or having a tough time coping? You’re not alone. Many of us go through periods where it feels like the world is crashing down around us. This state often signals a mental breakdown, a term that describes a period of intense mental distress. During this time, managing day-to-day tasks can feel impossible. By understanding…

Vezi pe WordPress
#"Adult ADHD symptoms"#"Agoraphobia symptoms"#"Anxiety disorder signs".#"Anxiety symptoms"#"Bipolar disorder symptoms"#"Burnout symptoms"#"Depression symptoms"#"Emotional breakdown symptoms"#"Mental breakdown recovery"#"Mental breakdown symptoms"#"Mental health disorders symptoms"#"OCD symptoms"#"Panic attack symptoms"#"Post traumatic stress disorder symptoms"#"Psychological distress symptoms"#"PTSD triggers and symptoms"#"Schizophrenia symptoms"#"Signs of a nervous breakdown"#"Signs of mental illness"#"Stress symptoms"#"Types of mental disorders and their symptoms"#Anxiety#Depression#EmotionalHealth#MentalBreakdown#StressRelief#Symptoms
0 notes
Note
It's possible for alters to have their own mental health!!! Alters can have personality disorders that other alters don't have, I think what you're talking about is autism, ADHD and other disorders similar! (As those affect the brain and therefore affect the whole system, but personality disorders are a different sort of thing, so one alter can have a PD and the others might not!) We can provide links if you'd like ^^ /nm /info
Hey there Anon! Thank you for the offer. We also received the following anon from (probably) another user, which I'd like to address here as well:
Alters can have personality disorders: (link)
“✘ MYTH: ALTERS CAN’T HAVE THEIR OWN MENTAL HEALTH ISSUES IF THE MAIN SURVIVOR DOESN’T HAVE THEM.
They actually can, and many do. It’s extremely common for individual alters to battle depression, anxiety, OCD, bipolar, eating disorders, self harm, etc., while other members of the system experience no such thing. Some extremely differentiated systems may even need that system member to come forward and take medications that the rest of the system does not need and will not get. ..and their brain’s neurology responds accordingly.
But, make no mistake, most expressions of mental illness amongst alters are incredibly real and valid and should be treated as such.”
(cut up a little, the source is above, we're pretty sure the source is reliable, it seems so. We've also had other systems say this too, and to us that's how it works, as only one of us as far as we know are affected by NPD)
Firstly, I feel the paragraph that was cut out of the Beauty After Bruises section is very important for further context and explanation. It's quoted here below:
One note about some disorders, however. Non-verbal, poor eye contact, savant-like, or sensory-processing-disorder alters can be extremely common traits in DID systems. However, it’s important not to just jump to calling these parts “autistic” if the system as a whole is not autistic. It’s possible for alters to behave in ways that mimic their understanding of SYMPTOMS in other disorders they know about, while not actually possessing the neurology for them. This is a complicated subject we could try to elaborate more on at some point, but it’s just an encouragement to pause and not automatically label some parts as having certain conditions just because they show a few traits of them. It can cause a great deal of conflation and misrepresentation of those illnesses. It may also be purely based on discriminatory or uneducated stereotypes of those conditions that were adopted into a young child’s mind. So, it’s just helpful to check for that possibility first!
As Beauty After Bruises is saying here, neurology takes a place in this discussion. It seems as if this resource is mostly stating that alters can all struggle with mental illness, and can appear to struggle singularly with those illnesses symptoms -- in which case, the "This alter is a symptom holder" is exactly the language we feel comfortable with. Until we are able to research more, we're wary about spreading potential misinformation about how brains work.
As mods, we absolutely want to do our best to avoid spreading misinformation. From our understandings, NPD and similar personality disorders are caused by a structural shift in the brain -- something physical and concrete. Here's some of our resources we found on NPD.
Source 1: “They analyzed a total of 34 test subjects, of which 17 suffered from a narcissistic personality disorder… Using magnetic resonance imaging (MRI) methods, the scientists measured the thickness of the patients' cerebral cortex… The findings revealed that those subjects suffering from narcissistic personality disorder exhibited structural abnormalities in precisely that region of the brain, which is involved in the processing and generation of compassion.”
Source 2: “The decreased brain white matter microstructures among three clusters were found in the association, projection/thalamic and connection pathways of white matter in young adult males with NPD. The abnormal white matter brain regions may be one of the neuropathological basis of the pathogenesis of young males with NPD, and it may be related to white matter development in early adulthood."
Based on these sources, the moderators are most comfortable using the language of alters being symptom holders. Both sources indicate that NPD affects the structural nature of the brain, which would impact all of the members of the system. However, like Beauty After Bruises was suggesting, that doesn't mean that various alters don't reflect those symptoms in different ways. It's absolutely possible for alters to struggle more or less with disorders, or even seemingly not at all.
I hope this clarifies our perspectives. Thank you!
70 notes
·
View notes
Note
The tragedy of her fanbase being drawn to her and subsequently annihilated for the same reason- her disorder- is encapsulated well by the quote from Joker, “The worst part of having a mental illness is people expect you to behave as if you don't.”
People loved her for her raw and relatable expression of pain, trauma, and dysfunction, then crucified her for exhibiting the classic symptoms of her disorder. Missed deadlines, empty promises, emotional outbursts, delusions of grandeur, compulsive lying. At what point is someone mentally ill allowed to be mentally ill and live a semi public life? Should she have spent her entire career groveling and begging for mercy because she acted bipolar when she was bipolar and open about her struggle? The endless whining about accountability misses the point entirely. Her entire career exists because she was sick of having to live her life constantly asking for forgiveness for being visibly sick with something beyond her control. All of you ate it up with a spoon because you related, then managed your own symptoms well enough to feel superior to someone still struggling, likely with something more severe- or maybe you just stopped LARPing as mentally ill when you realized it was embarrassing and shameful. Either way, you’re hilariously blind to the hypocrisy. You claim you’re better because you weren’t taking money from fans who willingly spent it- and you also contributed absolutely nothing of value creatively to the world.
This fanbase is full of socially inept, chronically online, holier-than-thou cringe factories who laughably think they have some kind of moral high ground over Emilie or think they have the right to decide how much she was allowed to publicly struggle with bipolar based on how much her behavior annoyed them personally or offended them. No wonder emilie has ghosted this skidmark of a fanbase. I wouldn’t be caught dead seen in public with 95% of you.
.
20 notes
·
View notes
Text
This is kind of just an unhinged meta rant about Rymin so do with it what you will. It's about Ryan's parents and how, despite having very little screentime, they really play into the story and the disagreements that Ryan and Min-gi have.
Ryan's dad only has one line and it's to give exposition to the fact that he's from a large family. That's all any of the Akagis say about Ryan. They aren't paying any attention to him or what he's doing in the BBQ scene in the twin tapes. Ryan is the exact middle child, and I think that was chosen intentionally to drive this point home. Them overlooking him leads to a lot of his outbursts throughout the season (quotes may not be exact because im not going back to look) -- "Our parents are probably wondering where we are. Or, at least... yours are." (the old west car), "Why doesn't anyone care about how I feel?" (the art gallery car), "At least your parents actually care about you!" (the mega maze car), and "No one cares about me unless I'm doing... something." (honestly cannot remember which episode and I'm too lazy to look it up). Ryan's parents' absence from book four is purposeful -- their lack of presence says just as much about Ryan as Min-gi's parents presence says about Min-gi.
Ryan has a big personality. He's a performer. He loves dressing up in crazy outfits and he loves looking cool. I don't think these things necessarily stem from emotional neglect as a child, but they are affected by it. He craves attention and he hasn't been getting it, and that leaves him with severe issues when it comes to dealing with his feelings. All of those quotes I mentioned are him lashing out, seeking attention from Min-gi, hoping that Min-gi will notice how much he's hurting from being ignored -- but every time, Min-gi redirects back to his own family issues.
Min-gi is from the opposite situation. I don't have as much to say here because the show is much more blatant about it, but his parents give him too much attention. They hover, they tell him what to do and how to do it. He is being slowly crushed by their expectations. He wants the same things as Ryan -- to make music, to perform, albeit for... lets say artsier reasons than Ryan does. But he's been taught those things are childish. He needs to be the responsible one, and clearly he's the only one with a good head on his shoulders, considering what Ryan is like. He lashes out at Ryan constantly, especially in the early part of the season, for continually dragging him into impulsive plans.
He wants Ryan to conform to societal norms, like he does, like his own parents taught him, so that Ryan will stop getting them into messes. However, Min-gi doesn't see that Ryan's personality and mental health issues don't give him the option to conform (creds to tumblr user vexahlla for that phrasing ... her tags on this post made my brain explode). He says "I couldn't get into uni if I tried" (the mega maze car). This is a whole other rant but Ryan also displays symptoms of bipolar disorder throughout the season which indicates to me that his brain chemistry would not physically allow him to slow down and follow a "typical" life path without genuine help (not the needling Min-gi was doing in the astro queue car). I think these problems that the show alludes to would have been alleviated a lot more if he'd had more help from his parents, but again, he's dealt with emotional neglect since he was tiny.
So Ryan and Min-gi end up as an unstoppable force and an unmovable object (which... now that i think about it... is a pretty accurate description of them as people, too). They both want to play music, but Ryan needs it immediately, because he needs the attention that he's not getting at home. He wants to get away, and fast. However he doesn’t realize that getting away without Min-gi is pointless, because Min-gi is who he actually wants attention from anyway. On the other hand, Min-gi can't leave immediately, especially when he thinks there's a particular life path he needs to follow. Both desperately want the other in their life, which keeps driving them back together, but they butt heads because their upbringings are so opposite.
This issue doesn't exactly get resolved in book four, but it doesn't need to, either. Book four ends with Ryan and Min-gi apologizing, and agreeing to stop sweeping things under the rug, actually try to look at each other fully, and see where the other person is coming from. So it's definitely a start to mending the gap between them and i think that's enough.
#rymin#infinity train#keeperofthebox talks#Theres so much more i want to say but its not really directly related to this point and i wouldnt know how to phrase it anyway#ryan akagi#min gi park#Im going to go listen to me and michael by mgmt and cry now
169 notes
·
View notes
Note
i disagree with a lot of your views on mental health just given my own research and knowledge of mental illness and the dsm-5.
i think the inherent issue with it is the categorization. organizing things by how they present behaviorally feels very unscientific. we need to do a lot more research to lean into like a sort of biological taxonomy. one big example is that schizophrenia and bipolar disorders have a LOT of overlap in brain areas, and while they are not identical areas, treating bipolar as something closer to anxiety and depression seems like a poor way to treat it, especially if you're looking from biological and medical perspectives.
i'm not as familiar on ptsd and personality disorders, but there's a lot of overlap there, and considering my own experience "developing a cluster b personality disorder" from trauma (i say this in quotations because i do not actually like the diagnostic system and would rather remain undiagnosed), i wouldn't be surprised if there was neural overlap in like, activity, connectivity. There's probably other stuff too we haven't really looked into. I feel like there's so much more we can do to look into the neurology of mental illness than we're doing as is. Focusing on symptoms too much, and even neurology wise plasticity can be a problem. Did you know bullying can change the way your brain works?! (Reductive way of saying it, but there's a bit of research on bullying +plasticity, also i'm off track.)
i also feel as though the clinical/general applied psych community could do a lot more pulling from basic research. we only get the moolah if we work through their lens (i'm a cognitive neuroscientist), so like. i wish therapists and psychiatrists would look a little more into our readings sometimes...
i've been doing a lot more reading on dimensional models, and i kind of like what it's putting down. part of me worries that having neurological profiles of mental illnesses might end up sort of labelling neurotypical people in the same sort of essentialist way a lot of diagnostic labels do with mentally ill people (reason i would like to remain undiagnosed). But I think the idea of quote unquote "neurotypicals" with tendencies (something discussed both in literature and in clinical settings where mental illness is defined as symptoms + distress) and similar brain patterns to those with adhd, autism, ocd, depression, psychosis etc sort of forming community with those who have those disorders proper. i think we could learn a lot from one another! coping mechanisms, how to deal with big stressors, learning what sets us off in situations with better coordination and less yappy narcs than group therapy. perhaps it's idealist, but i'm a bit of a dreamer.
i hope you read this and consider my point of view, even if it did meander a bit XD
It took me awhile to be able to sit and take this in, and even still I'm having a hard time comprehending chunks of it so if my response ends up misinterpreting anything feel free to send another anon to clarify.
I do agree that we're still not at a perfect stage of "all of these things are 100% properly understood", and by no means do I feel psychiatry has managed to hit a perfect stride when it comes to diagnostics either. Things can and do still get misdiagnosed for various reasons, and there's definitely disorders that get seen as "similar" because of behavior that brain-structure wise may be worlds apart.
I also agree that in concept, having spaces that allow currently undiagnosed/traits of/self-suspected people, or those who just have a few similar symptoms that find themselves relating to, is certainly not a horrible idea. Having peer-to-peer support spaces shouldn't necessarily depend on whether or not a doctor has given you the "stamp of approval," and in some cases I've even seen well-vetted, non-specific spaces that foster this in a very positive manner.
But in the spaces dedicated for a specific disorder, the language used in them is.... not that. It isn't someone who suspects they have it asking for advice on how to see a doctor, or another saying "I relate to x symptom, what do the people here with y disorder find helpful for mitigating this?"
It's often rife with people who, whether due to comorbid disorders, malingering, or active faking, are spreading vast and wild misinformation that causes harm to both those already diagnosed (possible to adapt false behaviors and receive improper care if doctors assume misdiagnosis), and those actively seeking one (may exaggerate/lie about symptoms or use key words found online that lead a doctor to assume malingering, even during real cases).
There's so many takes that disregard the medical misinfo to fixate on validating "all" experiences, regardless of when those experiences indicate a different disorder. And if that gets called out, then you're fakeclaiming every single person there somehow. And if the space is actively pro-self dx, then they're often prone to telling people that no psychiatrist should be trusted (ESPECIALLY if they tell you your self dx is wrong) and that a diagnosis doesn't matter anyway because it's all some grand conspiracy to further oppress you.
And outside of that, even when someone has similarities, traits, or specific relatable symptoms, there's times where those of us experiencing a specific disorder want to feel a sense of community with those who have the same type of experience, and not just someone who understands "by proxy" or as an outsider.
I have plenty of people who don't have a dissociative disorder in my life who can relate to certain symptoms I have, or can understand in a sympathetic manner when I talk about my experiences and frustrations. But I don't know anyone else with DID, let alone that I know is being honest about it. I don't have a sense of community or belonging-- I feel isolated. And the internet hasn't made me feel more of a sense of community in having DID, but instead it's managed to make me feel more shut-out due to how wide-spread the horribly reductive rhetoric around it is.
I don't have this in regards to having autism or adhd. Hell, I'm even less strict about my views around posts and self-recognition of those because 1. they're often found due to social irregularities that a person experiencing them may be able to pick up on, and 2. people are much more receptive to when misinformation, infantilization and ableism in regards to them is called out.
This has turned into a bit of my own meandering but basically, a lot of my frustration at the moment is stemming from the internet's treatment of DID (and dissociation in general), and there's definitely things I've said about disorders in general that I think there are exceptions to, but it can be hard for me to sit down and think about/talk about those things while I'm wrapped up in my frustrations about this thing specifically.
4 notes
·
View notes
Note
Any tips/advice for peeps who just got diagnosed? Searching for information in the void is …. 😵💫
Heyhey, let me just say, welcome :) it means a lot that you turned to me. I'll give my best, but keep in mind I'm not an expert (and this could be ten times as long).
Okay, first of all...know that what you're doing (seeking info) is amazing, sadly sometimes rare, so I commend you for that.
I'd go through some legit sources first. I highly reccomend dr. Kay Redfield Jamison's works (especially her autobiography An Unquiet mind, that helped me accept bipolar). And one that really is just a comfort ("comic")book for me is Marbles: Mania, Depression, Michelangelo and Me by Ellen Forney. Another badass woman with bipolar was Carrie Fisher. You can look up her quotes and talks regarding the illness (truly amazing, 100% reccomend).
A good way to track everything (especially at the beginning) is a mood app. There are some designed for bipolar, but I used Daylio (simple and easy).
Then try to identify triggers (this comes gradually). Usually sleep changes are the first indication of an episode (often mania if sleep is reduced). Any sort of change is a potential trigger. Now you have to carefully watch yourself until you find yours (consult with a professional about them, if you can). The thing about bipolar episodes is that they tend to sneak up on you, and unfortunately not recognizing the obvious is in fact a symptom in itself.
Remember: prevention is your best asset. A full blown episode is always harder to treat, leaves more damage and lasts longer.
Find a routine that works best and try to stick to it. And seriously, stay on meds (if you have them prescribed).
...things that possibly await you are: love/hate relationship with medication, idealizing and longing for an episode (commonly euphoric mania), explaining things to people (realizing some are jerks, finding better ones), a vicious cycle of romanticising and cursing this illness, more medication and doctor problems, acceptance, stability, different views of the world, loving communities, awesome memes etc...
And lastly, patience. Honestly, it's hard and chasing stability can seem Sisyphus' work. But it's really just an illness, one part of you that might seem as big as an ocean (but that's a lie). You'll find there's lots of hope out there, wonderful medication and support. You are most certainly not alone, even when it seems so. 46 million people around the world are affected by bipolar disorder, we're all in this together and trust me on this, you'll never fight alone.
If you have any questions about something specific (therapy, "coming out" about it to others, more sources, just conversation...whatever really) don't hesitate to DM me.
Lots of love,
<3
#ask#answered#bipolar disorder#advice#mental disorders#actuallybipolar#manic depression#actually mentally ill#actually bipolar#manic depressive
78 notes
·
View notes
Text
PART 2
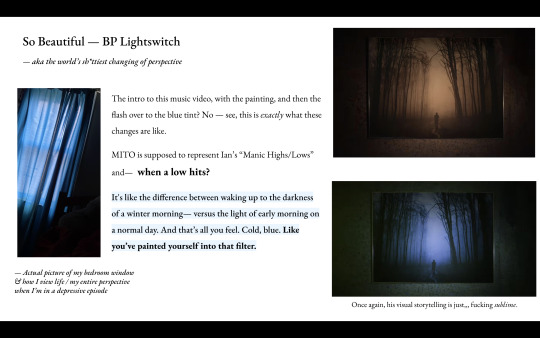
Out of all of Ian's songs, "So Beautiful" is one of my absolute favorites, especially the MV because of [again] the visuals and how accurately they convey what being Bipolar is like or what going through an episode is like.
Often I have the hardest times knowing I'm in an episode (until it's escalated significantly) because I go from being "unable" or "meh" to being able, and --like the quote above;
I can't tell if I've entered into a mood episode, or if I'm generally just having a good day.

You'll see this in a lot of my journal entries, but lack of control is major when (in my experience) it comes to being Bipolar.
Having no control over your own mental stability is "maddening"...for lack of a better term.
Around three years ago, I watched SKAM France and began to wonder if I was Bipolar.
Seeing Eliot, all I could think was: "Yeah that's me."
But since I didn’t know if I actually had it — I started mood journaling — and eventually I went to a psychiatrist (don’t get it twisted, I went for depression LOL — and because I was seeking to find an ADHD evaluation), and yeah. I was diagnosed with both ADHD and Bipolar.
Now — you might ask: “How can you NOT know or realize you have bipolar disorder?” And ohooooo my friend, let me TELL you.
— Depressive Episodes—
In Bipolar (though no one experiences it the same way — it’s a spectrum, but there are some general commonalities), there tend to be more depressive episodes than manic or hypomanic episodes.
“Although mania and hypomania specifically identify bipolar illness, depression is of major concern in patients with bipolar disorder, because depressive symptoms are far more frequent than manic symptoms and most suicides occur during the depressive phase.” (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1324957/)
In this academic article about the burden of bipolar depression within bipolar disorder, it shares studies particularly on how Bipolar
Depression significantly impacts Bipolar patients.
People with Bipolar usually seek help when they’re in a depressive phase; and are therefore often misdiagnosed as MDD — Major Depressive Disorder. The problem with this is that MDD treatment, usually going onto antidepressants, can send the Bipolar patient into acute mania, mixed states, and/or rapid cycling states. (I will define these in a second.)
...
“Bipolar disorder has a negative impact on virtually every facet of a patient's life, with depressive symptoms having a particularly strong effect on patient well-being. Depressive symptoms predominate over hypomanic/manic symptoms in the courses of both bipolar I and bipolar II disorders. In prospective studies of the natural history of bipolar disorder, bipolar I patients reported experiencing depression for 31.9% of weeks and hypomanic/manic symptoms for only 8.9%, whereas bipolar II patients reported depression for 50.3% of weeks and hypomanic/ manic symptoms for only 1.3%.”
“Similar findings on the prevalence of depressive symptoms were reported in a study of 258 outpatients admitted to the Stanley Foundation Bipolar Network. Approximately 25% of these patients reported being ill for more than three quarters of the year, with a mean of 214 days depressed, and 40% were intermittently ill, with a mean of 120 days depressed. An overview of findings from the Stanley Foundation Bipolar Network concluded that, despite treatment, bipolar outpatients remain significantly affected by their illness, with depressive symptoms posing a greater problem for effective treatment than mania.”
“Over 60% of patients in the Stanley Center Bipolar Disorder Registry were unemployed, despite the fact that 30% had completed college.”
“Termination of mood stabilizers may also have negative effects in patients with bipolar disorder. In published studies of patients with bipolar disorder who discontinued lithium treatment, suicide rates rose 20-fold and affective illness recurred in 67% of patients during the first year after discontinuation of lithium. Termination of treatment with other mood stabilizers, including the atypical antipsychotics, may be associated with negative outcomes.”
These are quotes taken from the same source quoted above in red.
[Right.]
So — for me, since my onset of Bipolar was around puberty (late middle school; early high school), added in with the emotional dysregulation of ADHD, my mood episodes were something I had gotten used to, and that I thought were normal. (LOL.)
Plus, I didn’t realize or know what hypomania and mania was; ergo—I only really recognized the major depressive episodes. “Ah, everyone gets depressed <33.” ←My bonkers thought process.
I didn’t realize my intensity of depression was something that people didn’t normally experience — in fact, I remember talking to my little sister, and she told me she barely ever got depressed, and when she did it was just for a short period of time. The ‘surprised pikachu’ meme would be apt here, LOL!
My wake-up call that it wasn’t normal was a tv show (SKAM — the french one; though I have watched the OG one.) that had an accurate portrayal of Bipolar Disorder in one of the main characters. The way they went from happy elation; that flirty feeling of being on-top of the world, to the fall into a major depressive episode.
That depression was all too familiar to me. Literally looked the EXACT fvcking same.
...
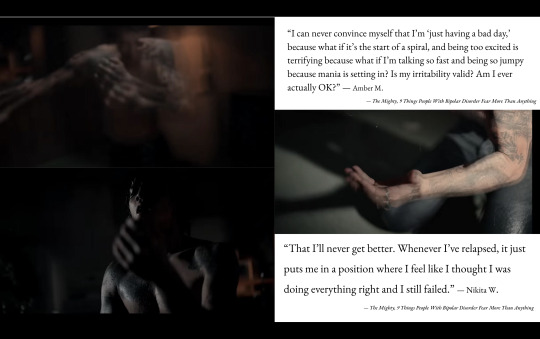
Three best portrayals of what my sudden depressive episodes look like:
[1] Mr. Robot — Eliot bawling his eyes out in episode 1. (20:00 Minutes in Timestamp)
(Link clip example here)
[2] Eliot Demury — Skam France (And Even — OG SKAM)
[3] Ian Gallagher, Shameless (U.S)
— (Linked clip example here)
...
I don’t know how to exactly describe it. Sometimes there’s just this overflow of emotion that makes me either cry or laugh or both. But mostly….it’s the apathy. Nothing matters. Nothing. The reason I don’t really care anymore about others’ opinions is because once I felt that apathy — that feeling of emptiness; of not caring — because life was nothing; I was nothing. So anyone’s negative opinions of me didn’t matter, I didn’t care about myself, so whatever they said ‘was probably right’ ←in my head; but it was as good as dust to me because nothing and no one could beat the hate I had for myself, OR the sh*t I was telling myself.
It’s fvcked up, I know. Even more fvcked up — is that there would be days I couldn’t get out of bed for a week. I would lay in bed. I wouldn't eat, it would be rare if I got up to use the bathroom— and any responsibility I had, I would not attend to — and you couldn’t make me. I would sleep 17-18 hours a day. Tired of everything, I would have no energy.
I ended up losing a lot of weight in college because of this LOL. I also fainted because of this (rip). When I could function enough to eat, go to class, I would still be empty and fatigued. I would go to class, eat, and then spend the rest of my time sleeping.
Even in high school, I would have an exorbitant amount of “sick days.” And when I did go to school, when I got home I would do my (1) chore and then sleep. School, chore, sleep. School, chore, sleep. It was to the point that my parents thought I was on drugs because all I would do was sleep. LOL.
And that depression would last for months. If it lasted two weeks or less that would be lucky. Anyways, there was a period of time (a few months after I graduated college) that I was normal. I felt normal, I acted normal, I had normal amounts of energy.
I remember telling my friends that (because I made a psychiatrist appointment) I wouldn’t tell them (the psychiatrist) about my depression because “Bah, it’s not that bad. I can sleep it off 🤪.” Anyways — I suddenly (and for no reason) fell into a depressive episode, and when that hit I was like, “Yeah I need to go tell the psychiatrist and get this figured out.”
I actually started treatment for depression before ADHD. And my depression was so bad, the antidepressants just barely made me functionable. Literally could not tell if they were working and my depression was that bad, or if they genuinely didn’t work. Anyways; yes they WERE working, my depression was just that bad. LOL.
(TW: Suicidal Ideation)
When I get low like this, if I start spiraling (which often happens) I get to the point where I think, constantly: “I don’t want to wake up anymore.” Sometimes I would even pray not to wake up anymore. I had crippling fatigue — so there was no energy to hurt myself. Which is why most of my mixed episodes are so dangerous.
Mostly though, when I’m down / dipping, I sleep. I just let myself do nothing, and sleep. Until it leaves, however long that may take.
I've talked about my experience being manic a few times.
Here I talked about being euphoric
Mania Episodes
I have had both euphoric AND irritated mania. And I have got to say — I liked the euphoric one; but FVCK the other one.
Mixed Episodes
Ok. Mixed episodes — where one has energy (manic symptoms) but irritation or depression / fatigue (depressive symptoms); basically it's a mix of both mania and depression.
For me — this is when I get into the most dangerous states.
Most of the time I’m so tired it actually hurts. It feels like the fatigue is killing me; like I’ve sunken into the dark circles under my eyes. Except the moment I lay down? BOOM! Wide fvcking awake.
The fatigue doesn’t leave, nor does the pain, but there’s this energy buzzing through me and it quickly turns into irritation because all I want to do is SLEEP, but I can’t! I fvcking can’t; and it kills me.
Theses are the times where any passive suicidal ideation become more active thoughts. Mostly about prescription drugs and overdosing. (Or things like drinking windex.)
Anyways —
I don’t ever act on these thoughts because I do like living (thank you very much >:o ); but that doesn’t mean those kinds of thoughts don’t happen. In fact ---a whole spiraling intrusive thought chain decides to party in my head until I DO fall asleep, or find something to distract me. (Not a fun time.)
First — let’s just get this out of the way; Bipolar — aka the episodes, whether depressive, manic, or mixed — , are not caused by purely external events. It’s literal chemicals in the brain playing limbo with your mental health.
Now, can external events trigger an episode? Absolutely.
In fact, sleep is one of the strongest triggers for people with Bipolar disorder.
And I quote:
“ — It is essential that people with bipolar disorder practice good sleep hygiene. Ideally, you should go to sleep and wake up in a regular, predictable pattern and avoid activities that interfere with this schedule, including staying up late, drinking alcohol, and consuming caffeine. In order to promote a restful and regular sleep, create a ritual for yourself to get your mind and body prepared for bed. If you struggle to sleep, be sure to talk to your doctor about it so you can identify whether these sleep disturbances are a symptom of a mood episode and gain control over your sleep cycle before it triggers mood switching.”
— bridgestorecovery.com ‘Understanding Bipolar Disorder Trigger And How to Prevent Them’
I have stated this before here and here
But blackouts can happen when you're in a manic state; these last few months I've had at least three black outs, spanning from a day, to a couple of days.

/End of part 2 <333 /
[Prev] [Next]
PPT Essay: [1], [2], [3], [4], [5], [6], [7] , [8], [9]
And of course the MV:
youtube
Visuals of a Depressive Episode: (1), (2)
Journal Entries: 1, 2, 3, 4, 5
PPT Essay Extras: (1), (2), (3), (4), (5)
#part 2#after this i'll liveblog some more#lmao#seeing as it's 10 minutes from midnight#my thougts#bipolaire#bipolar disorder#manic depression#actually bipolar#mental health#neurodiversity#neurodivergencies#dpr ian#dpr we gang gang#christian yu#fvcking moodswings ⚡️✌️#a scoup of life 🔫🦆#Youtube
96 notes
·
View notes
Text
Roscoe Dillon's Psychiatric Assement
I decided to do a psychological evaluation for The Top (Roscoe Dillon), and make it as accurate to a real-world evaluation as was feasible for a guy who's canonically a ghost.
I do not have a doctorate in psychology and cannot diagnose real people, but I am working on my master's in psychology and feel reasonably capable of diagnosing a fictional person who cannot be harmed by my diagnosis if I am wrong.
I tried to be as accurate as possible in my presentation of all conditions included---but feel free to correct me if I made any horrible mistakes.
TW for: Mental health problems; suicide; the Dillon family's horrible ideas about mental health
Iron Heights Penitentiary
1961 Broome Street
Central City, MO
Complete Evaluation: Adam Brooks, M.D.
Date of Exam: 7/31/2019
Time of Exam: 4:45:22 PM
Patient Name: Dillon, Roscoe Neyle
Patient Number: 111044554
History: Roscoe Dillon is a 36-year-old male prisoner of Iron Heights Penitentiary. He is currently unmarried and has no children, but he is in a long-term relationship with a woman named Lisa Snart. He was referred to me by Correctional Officer Robert Morrison after he attempted to hang himself in his cell. This attempt left him unconscious for two days, and it was only after he woke up that I was able to begin the process of evaluation.
Roscoe’s chief complaint was, quote, that “I am a failure, and therefore the tops have turned against me”, and stated that his motivation for his attempted suicide was his belief that he had failed his girlfriend, Lisa, as well as, quote, “my own lofty expectations of myself”. Roscoe also describes and displays symptoms of a mood disorder, with psychotic features, and specifically reported symptoms of depression. While he was unable to provide me with a coherent explanation of how long his symptoms have lasted, Correctional Officer Morrison reports that he has been chronically displaying symptoms since he was incarcerated in Iron Heights Penitentiary nine months ago.
Current Symptoms: Roscoe reports a depressed mood, a loss of pleasure in spinning his tops, problems with his appetite (“I did not realize until recently, but I do not think I have eaten more than a meal a day in quite some time”), difficulty in concentrating, feelings of worthlessness, and a death wish, the latter of which precipitated his attempted suicide. Correctional Officer Morrison also reports that when he is on guard duty, he sees Roscoe sleep only rarely, suggesting a level of insomnia. Roscoe himself was unable to confirm this, but did admit that he thought it was quite likely that he “had not been sleeping well of late”. He attributed this disruption in his sleep to racing, anxious thoughts. Roscoe also reports extreme agitation and a general inability to keep still, which he displayed throughout the evaluation in the form of rocking back and forth in his seat. Also throughout the evaluation, he displayed extremely pressured speech. It was often difficult to understand what he was attempting to say, and this communication barrier seemed to add to his agitation throughout.
Suicidality: Roscoe attempted suicide three days ago, and, while he has not actively attempted suicide since, he has not expressed a desire to live.
Prior Manic/Depressive Episodes: Roscoe has had four prior manic episodes and four prior depressive episodes, three of which involved an attempted suicide. During his first major manic episode, he threatened to blow up half the world with a spinning atomic grenade unless he was made king of the world.
Severity/Complexity: Based on the risk of morbidity without treatment, his personal descriptions and the descriptions of Correctional Officer Morrison of interference with his functioning, his psychotic symptoms, and his recent attempted suicide, Roscoe’s Bipolar Disorder is estimated to be severe.
Associated Signs and Symptoms: In addition to his mood symptoms, Roscoe also displays a number of symptoms of psychosis. He demonstrated mood-congruent delusions of failure, as well as a delusion of passivity, claiming that, quote, “the tops are punishing me for my failures. They are the ones who are making everything spin and spin and spin”. Besides these delusions, Roscoe also reported visual hallucinations, in the form of distorting shapes and colors and the world around him spinning in a fashion that is similar to what might be experienced by an individual with vertigo, and auditory hallucinations, in the form of his father, girlfriend, and girlfriend’s brother talking to him while he was in his cell alone. Furthermore, while Roscoe’s speech was generally organized enough to be comprehensible, he frequently made top puns, and references to rotation and spinning, that had seemingly little relevance to the topics that were being discussed. Roscoe seems to have a degree of insight into his condition, stating that, quote, “I am quite aware that I am mad”, but not to the extent that he recognizes that his delusions of failure and passivity are irrational.
Past Psychiatric History
Withdrawal History: While Roscoe reports a fondness for fine wines, he also claims that he has never experienced serious withdrawal from any substance, and there is no available evidence to contradict this assertion.
Psychiatric Hospitalization: Roscoe was briefly psychiatrically hospitalized after an attempted suicide at the age of seventeen, but was removed after only two weeks. This was done at the behest of his parents and over the protest of at least one of the nurses at the facility. He has also been hospitalized in the prison infirmary for mental health problems twice before, once as the result of a manic episode and once as the result of a depressive episode.
Outpatient Treatment: Roscoe has never received outpatient treatment.
Suicidal/Self Injuries: As previously mentioned, Roscoe has attempted suicide four times. At the age of seventeen, he deliberately overdosed on his parents’ prescription medicine, and was only saved because his mother found his body thirty minutes afterward. At the age of twenty-four, he attempted to jump off of a bridge but was stopped by an off-duty firefighter, who tackled him to the ground before he could actually carry his plans out. At the age of twenty-nine, Roscoe died of a brain hemorrhage induced by the combination of his newly-developed telekinetic powers and the Flash’s super-speed vibrations, but was able to return to life via the possession of several corpse bodies, which he modifies to resemble his own. Due to his unusual manner of existing, his fourth attempted suicide, which he carried out at the age of thirty-two, was actually a completed suicide, in the sense that he deliberately abandoned his host body in order to return to an incorporeal state, and, had he not subsequently possessed a new host body, this psychiatric assessment would never have occurred. While all of this sounds impossible, it has been repeatedly and independently verified by several doctors, police scientist Barry Allen, several other members of the police force, and a coroner, so I am forced to accept the story as true. His most recent suicide attempt occurred two days ago; he attempted to hang himself in his cell with his bedsheets and was only saved by the quick actions of Correctional Officer Morrison. Roscoe does not appear to engage in non-suicidal self injury.
Addiction History: Roscoe vehemently denies any history of substance abuse, and, while it is clear that he drinks a number of alcoholic beverages, there is not sufficient evidence to prove that he has any substance abuse problems.
Psychotropic Medication History: Roscoe has been prescribed lithium by previous doctors, and does take it with at least some regularity when he is not in prison. Due to what I can only assume was an organizational oversight, however, he has not had access to lithium since he arrived at Iron Heights Penitentiary nine months ago (as confirmed by Correctional Officer Morrison).
Other Psychiatric History: Roscoe has been psychologically evaluated twice before whilst incarcerated. He has previously been diagnosed with Bipolar 1 Disorder, which is consistent with his current symptoms, as well as with Autism Spectrum Disorder. These previous psychological evaluations indicate that, when he is not in the midst of a mood episode, Roscoe struggles with social communication and interaction, and evidently has since he was a child. Although he doesn’t seem to understand why, he is aware that he has never had many friends, and he reports, quote, that “I did not like school. The children there made fun of my tops.” He also engages in stereotypies (rocking, hand waving, and especially spinning), particularly when distressed, and has an intense, nearly all-consuming interest in tops. He can monologue about tops for hours on end, and will do so if you allow it. Roscoe is also averse to loud noises and adheres to a variety of strict eating, washing, and dressing routines. In spite of all this, Roscoe insistently denies that he is on the autism spectrum, and will angrily insist that he is, quote, “neither a freak nor retarded” when the topic is brought up around him.
While his severe mood episode likely obscured most of his autistic symptoms, I did notice his rocking in his chair, and I likewise noted that his speech, although rapid and pressured, was also quite stiff (bordering on monotonic) and formal. He insisted on referring to me as “Dr. Adam Brooks” throughout the evaluation. He also only made eye contact once during the evaluation, and the contact he did make was sustained and intense enough that it was clearly not a natural behavior for him. His apparent fascination with tops might also explain the persistent top puns that littered his speech, as well as why he specifically believes that tops, rather than any other object, are punishing him.
Social/Developmental History
Roscoe Dillon is a single, 36-year-old man. He is American, and, although he was born in New York City, he and his family moved to the suburbs of Central City when he was eight years old, and he has lived in the Central/Keystone area ever since. He has a long history of criminal activity. He has been arrested more than four dozen times, most commonly for grand theft and armed robbery, and has been incarcerated on six separate occasions, although he has served out only one complete sentence. He is notorious for escaping from prison, and his repeated deaths also have put an early end to some of his sentences. Currently, he is serving a ten-year sentence for armed robbery, with possibility of parole, but the chances are extremely high that he will escape from prison well before the end of his sentence. I only hope that he doesn’t do so through suicide.
Relationship/Marriage: Roscoe is in a long-term relationship with Lisa Snart. She was once an Olympic-level figure skater who performed for the Futura Ice Company, but became involved in a life of crime shortly after Roscoe’s first death. She is currently incarcerated in the women’s wing of Iron Heights Penitentiary. In spite of this, the two appear to have a mostly functional and healthy romantic relationship. That being said, Roscoe’s intense level of attachment to Lisa is worrying; his primary motivation for attempting suicide was the belief that she would be happier if he was dead, and he also noted that if anything ever happened to her, he would probably kill himself.
Children: Roscoe has no children.
Barriers to Treatment
Emotional: While I have not personally evaluated Roscoe before, other prison psychiatrists who have worked with him state that he is violently opposed to the idea that he might be mentally ill or in need of treatment. This appears to stem from a belief that admitting to mental illness would be tantamount to admitting to being incompetent or a failure. He has also stated that he only takes lithium because Lisa, his girlfriend, asks that he do so. His current psychotic symptoms, which limit his insight, are another potential barrier to treatment, but these will be addressed via the treatment plan.
Environmental: Warden Gregory Wolfe strictly limits the number of patients who are permitted to attend therapy sessions with me. Getting Roscoe approved for therapy will likely prove very difficult.
Family History
Roscoe’s maternal great-uncle, Rufus Neyle, was repeatedly hospitalized for Bipolar 1 disorder. Previous evaluations of Roscoe strongly suggest that the Dillon and Neyle families viewed this as shameful and did everything they could to cover it up.
Roscoe’s maternal aunt, Rachel Dylan (neé Neyle), received outpatient treatment for major depressive disorder. Previous evaluations of Roscoe indicate that Roscoe’s father described his aunt as, quote, “weak” for seeking treatment for her condition.
Roscoe’s first cousin, Ralph Dylan, is known to have been diagnosed with autism spectrum disorder. Previous evaluations of Roscoe strongly suggest that his parents viewed this as an embarrassment; Roscoe evidently claimed that his father once referred to this cousin as, quote, “a retarded freak”; this likely contributes to Roscoe’s vehement denial that he is himself on the autism spectrum.
Roscoe’s paternal grandfather, Roland Dillon, is suspected to have had major depressive disorder. He is also known to have committed suicide at the age of 52. Previous evaluations of Roscoe indicate that his father, Reginald Dillon, perceived this as having brought shame on the family name.
Roscoe’s mother, Rosa Dillon (neé Neyle), is suspected to have anxiety and a potential alcohol abuse disorder. Previous evaluations of Roscoe suggest that she often seemed quite anxious and agitated, and he has stated that she often drank wine to, quote, “calm her nerves”. Roscoe has also claimed that his father did not know of this, or at least refused to admit that he did.
Family psychiatric history is otherwise negative. There is no other history of psychiatric disorders, psychiatric treatment or hospitalization, suicidal behaviors or substance abuse in closely related family members.
Medical History
Adverse Drug Reactions: None known.
Allergies: None known.
Compliance: Roscoe is notorious for non-compliance with medical instructions. While he does take lithium fairly regularly, at his girlfriend’s bequest, he never attends outpatient therapy when not incarcerated, and attempts to avoid therapy while incarcerated as much as he can, even to the point of getting himself sent to solitary confinement rather than having to attend therapy sessions. He seems to despise psychologists and psychiatrists on principle, and is known to make attacks on their professional competency when he disagrees with their assessment of his mental state (which is quite often). As a result, his mental health problems generally go mostly untreated.
Some of this hostility likely stems from the fact that Roscoe’s first psychological evaluation whilst incarcerated came at the hands of Jonathan Crane, a psychologist who was later stripped of his medical license for experimenting on his patients with an unregulated drug of his own invention. This drug, which the newspapers dubbed “Fear Toxin”, was a blend of synthetic cortisol, epinephrine, norepinephrine, indolealkylamines, phenylethylamines, arylcyclohexylamines, serotonin inhibitors, and dopamine enhancers, and was used to induce fear-based hallucinations in its victims. While it cannot be conclusively proven, the evidence seems to suggest that Roscoe was subjected to this drug as a part of the “evaluation” given to him by Crane, and if this assumption is correct, I fear that Roscoe cannot be entirely blamed for his distrust of the psychiatric profession.
Exam: Roscoe Dillon is six feet tall, and, when healthy, weighs around 175 to 180 pounds. When I evaluated him, however, he was badly underweight, weighing only about 147 pounds. His hair and clothes were noticeably disheveled, he had dark circles under his eyes. His body language and his facial features displayed obvious distress and depression. He seemed agitated throughout the evaluation and repeatedly rocked back and forth in his chair. He almost never made eye contact. He exhibited speech that was rapid and pressured—almost to the point of incomprehensibility at times—but which was otherwise properly articulated and generally coherent. His affect was congruent with his mood, and his conversation revealed clear evidence of delusions of failure and passivity, as well as of visual and auditory hallucinations. Except when discussing his specific delusions and hallucinations, his associations were intact, his thinking was logical, and his thought content appeared appropriate. Roscoe’s suicidal intentions were undeniable, given the bruises that were still around his neck from his attempt to hang himself, but he no longer appeared to be actively suicidal. He also denied any specific homicidal ideas or intentions. Roscoe’s cognitive functioning, vocabulary, and fund of knowledge are intact and age-appropriate, and his short-term and long-term memory and ability to abstract are likewise intact. His ability to do arithmetic calculations is not only intact but is bordering on the genius range, which is consistent with his general talent for engineering and inventing. Roscoe is oriented to person, place, time, and situation. Judgment is fair, but is compromised by his psychotic symptoms. Roscoe’s insight into his problems is not completely absent, but is severely limited by his mood episode and psychotic symptoms. There are also signs of autism spectrum disorder, but at present these are largely overwhelmed by his mood and psychotic symptoms.
Diagnoses
F31.5 [296.54] Bipolar 1 Disorder, currently depressive, severe with mood-congruent and mood-incongruent psychotic features.
F84.0 [299.0] Autism Spectrum Disorder, requiring support.
Instructions/Recommendations:
The patient should be confined to the infirmary until further notice, because the patient was very recently actively suicidal, and is still in the midst of a severe depressive episode with psychotic features. I will conduct therapy within the infirmary.
Once the patient has recovered to the point that he is no longer clearly psychotic or a suicide risk, I strongly recommend weekly therapy sessions, even if this is unlikely to take place due to Roscoe’s notorious tendency to avoid therapy at any cost.
Start 600 mg of Lithium, 2 to 3 times/day. Roscoe has Bipolar 1 disorder and a history of suicide attempts; he should have been on lithium from the second he came through the penitentiary doors. I don’t know what oversight caused this, but this problem needs to be resolved now.
Start 3 mg of Risperidone, once a day. This is for the psychotic symptoms.
Notes and Risk Factors:
Global Assessment of Functioning: 12
Risk Factors:
Z62.881 [V15.42] Psychological Abuse in Childhood
While never confirmed, almost every mention of his parents Roscoe has made indicates that his father was demanding, perfectionistic, critical, and verbally abusive when Roscoe did not live up to his expectations.
Z65.1 [V62.5] Imprisonment or Other Incarceration
Serving ten-year sentence for armed robbery (with possibility of parole) in Iron Heights Penitentiary
Z72.881 [V71.01] Adult Antisocial Behavior
1. Roscoe is a career criminal. While he sometimes commits crimes alone, he more often works alongside his girlfriend, Lisa, or in tandem with an organized group of costumed criminals known as “the Rogues”.
Electronically Signed
Adam Brooks, M.D.
On: 7/31/2019, 9:45:24 PM
#flash rogues#flash comics#roscoe dillon#the top#iron heights penitentiary#golden glider#fanfic#tw suicide#tw characters who don't understand mental illness#tw mental illness
6 notes
·
View notes
Text
Granada TV Series Review: "The Devil's Foot"
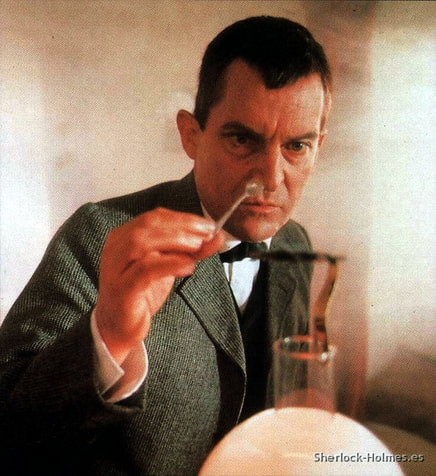
With this post, I am resuming a series of reviews that has been on hold for far too long: a couple years ago, I began watching the entirety of the Granada TV adaptations, starring Jeremy Brett as Sherlock Holmes. I have reviewed every episode up to (and including) the Granada version of The Sign of Four.
I resume the series with the next episode to air after The Sign of Four: "The Devil's Foot." This episode originally aired on April 6, 1988. It is based on the story entitled "The Adventure of the Devil's Foot," one of the stories in the collection called His Last Bow. The story was published in England in 1910, and appeared in America in 1911. Reportedly, Sir Arthur Conan Doyle ranked it #9 on his list of his dozen favorite Holmes stories.
The Granada adaptation follows the story pretty closely. Viewers who are sensitive to horrific images may wish to be warned that a couple of the characters who die in the story are filmed with spooky, open eyed looks of horror on their faces, and one other character is shown foaming at the mouth. It's a pretty creepy episode overall, with the most bizarre sequence being one in which Holmes exeriments with the effects of the strange powder that he suspects led to the death of two people, as well as the lunacy of two others. In the original story, the effects of the powder are described from Watson's point of view, while in the adaptation, we are given Holmes's point of view, which includes him bleeding from the eyes as he relives his struggle with Professor Moriarty on the edge of the Reichenbach Falls. In fact, one of his hallucinations shows both him and Moriarty falling to their deaths, which never happened, of course. The sequence is a bit disturbing, and the music that accompanies it is an interesting mixture of violins, synthesizer and drums.
One interesting addition to the plot happens towards the beginning of the episode. Watson makes no reference to Holmes's famous addiction to cocaine at the beginning of the story, providing this description: "Holmes’s iron constitution showed some symptoms of giving way in the face of constant hard work of a most exacting kind, aggravated, perhaps, by occasional indiscretions of his own." However, the adaptation shows Holmes with his cocaine syringe, with some rubber tubing wrapped around his upper arm. Watson enters and Holmes immediately tries to hide the evidence of his drug use, and though the good doctor does not criticize his friend, he is clearly troubled by the knowledge that Holmes has not shaken his addiction. Later in the episode, Holmes buries his syringe in the sand on the beach, wiping away the evidence with his hand.
Even though I found Brett to be fairly compelling in his performance, it is clear that the effect from his medication for his bipolar disorder was beginning to show. He looks a bit puffy, and his focus sometimes seems to be lacking a bit. Edward Hardwicke, who played Watson (and does a fine job in this episode) was quoted long ago as saying that Brett was smoking about 60 cigarettes a day, which could hardly have helped his health at the time. Still, the quality of the episode doesn't seem to be faltering too badly at this point, and I found it to be an engaging story, for the most part. Fans of the great detective may be a bit surprised by Holmes's decision after he discovers the identity of the murderer.
While it was hardly my favorite episode of the series thus far, I still think it was well worth watching, and a faithful adaptation of its source material. You can watch the episode on YouTube below. (Which reminds me, I shall be attempting to fix some of the dead links in earlier reviews in this series. But that process will take a bit of time.)
youtube
4 notes
·
View notes
Text
10 Common Symptoms of a Mental Breakdown
10 Common Symptoms of a Mental Breakdown
Introduction
Feeling overwhelmed or having a tough time coping? You’re not alone. Many of us go through periods where it feels like the world is crashing down around us. This state often signals a mental breakdown, a term that describes a period of intense mental distress. During this time, managing day-to-day tasks can feel impossible. By understanding…

View On WordPress
#"Adult ADHD symptoms"#"Agoraphobia symptoms"#"Anxiety disorder signs".#"Anxiety symptoms"#"Bipolar disorder symptoms"#"Burnout symptoms"#"Depression symptoms"#"Emotional breakdown symptoms"#"Mental breakdown recovery"#"Mental breakdown symptoms"#"Mental health disorders symptoms"#"OCD symptoms"#"Panic attack symptoms"#"Post traumatic stress disorder symptoms"#"Psychological distress symptoms"#"PTSD triggers and symptoms"#"Schizophrenia symptoms"#"Signs of a nervous breakdown"#"Signs of mental illness"#"Stress symptoms"#"Types of mental disorders and their symptoms"#Anxiety#Depression#EmotionalHealth#MentalBreakdown#StressRelief#Symptoms
0 notes
Text
ADHD Informative Post Pt. 2
Causes
As stated in the first part (on @fqiryinfo Instagram), a heavily theorized cause of ADHD is a lack of dopamine to the pre-frontal cortex. Genetics obviously play a major role in that, however scientists are also researching the possibility of brain injuries, exposure to environmental risks (like lead) during pregnancy or early childhood, alcohol or tobacco use during pregnancy, premature delivery, and low birth weight as possible risk factors. Having these risk factors does not necessarily equal having ADHD. Another neurotransmitter besides dopamine that may contribute to ADHD symptoms is norepinephrine. Certain parts of the brain have been noted to be decreased in volume, as well as low iron and zinc levels causing a higher risk for ADHD symptoms and even a higher severity of symptoms. Despite common misconceptions, ADHD has *no* connection with sugar currently noted and has nothing to do with parental styles.
Treatment - Medication
Medicated treatment is typically broken down into three groups. These are long-lasting stimulants (like Adderall XR, Vyvanse, Biphentin, and Concerta), long-lasting non-stimulants (like Strattera), and short/immediate-acting stimulants (like Dexedrine, Dexedrine Spansule, Ritalin, and Ritalin SR). XR stands for extended release while SR stands for sustained release. This is not necessarily a medication, but iron supplements have been noted to help allivieate ADHD symptoms which makes sense with the noted iron deficiency being a risk. However, zinc supplements didn't have as much of a positive effect.
Treatment - Non-Medication
Psychoeducation: strategy instruction (sleep management, anger contron, etc.), self-talk development, organizational skills developments, information on ADHD, community resources, and support groups
Behavioral Intervention: rewards and consequences, environmental management, ADHD coaching, and lifestyle changes
Social Intervention: social skills training and parenting skills training
Psychotherapy: self-talk strategies, cognitive behavioral therapy (CBT), interpersonal therapy, family therapy, expressive arts therapy, and supportive counseling
Educational/Vocational Accomodations: academic remidation and specialized academic/workplace interventions
Comorbidities
"More often than not, ADHD is further complicated by comorbidity with one or more psychiatric disorders.... An adult with ADHD is six times more likely to have at least one other psychiatric disorder than an adult without ADHD." (Thomas E. Brown, PH.D.). A quote from a book to all those who would like to argue against those who believe comorbidities don't exist. Even a study found 70% of 579 children carefully diagnosed with ADHD fully met the diagnostic criteria for one or more psychiatric disorders. Cases of ADHD not complicated by another disorder are rare.
As for the disorders ADHD is often comorbid with, that would be learning disorders, anxiety disorders, mood disorders (especially Bipolar Disorder), OCD, ODD, conduct disorder, substance use disorders, and personality disorders. Bipolar disorder especially, but but mood disorders in general stem from similar neurobiology so it makes for them to be so comorbid. (Bipolar 1 is even more comorbid than Bipolar 2.) Personality disorders are reported to be present in more than 50% of adults with ADHD. Of that 50%, the most common are cluster B and C disorders with 25% of them having two or more personality disorders. Of the papers I've read, none of them mention Autism as an actual comorbidity of ADHD however that's probably because it falls under the other disorders of early childhood they frequently mentioned.
Our Own Experiences
We are professionally diagnosed with ADHD. We have genetic links on both sides of our family, as well as a lack of iron (not diagnosed with iron deficiency but we do experience symptoms at times). We were diagnosed at 13 with the inattentive type. Originally we tried Strattera as a medication, but it didn't work so we switched to another medicine and it's been working ever since (heavy dissociation messes with the effectiveness though). We have recently decided to ask to start taking iron supplements to help with symptoms. As for comorbidities, we have a comorbid mood disorder (depression however the disorder type was never specified), generalized anxiety disorder, and social anxiety disorder diagnosed. We also experiences symptoms of BPD, but it's not been talked about with the mental health group we talk to so we avoid saying for sure we have it despite the genetic and trauma links. Obviously this is just in regards to this post, but yeah!
18 notes
·
View notes
Note
I'm so sorry if you've gotten this question a thousand times, but do you have any non-biased list of ASPD symptoms or things people with ASPD tend to do/think? I've been questioning if I have it but I can't find any list of symptoms that isn't extremely ableist
Well, part of that is because the diagnostic criteria's phrasing is pretty ableist. I can give you a quote from the most recent DSM (DSM-V TR, 2022) which is the book that professionals in the USA diagnose out of. I cannot give you the current criteria for ASPD outside of the US, because the ICD-11 has gotten rid of individual personality disorders in favor of a general "Personality Disorder" diagnosis with 3 severities but no clusters or individual disorders. I can give you the previous criteria from ICD-10, however.
(From DSM-V TR, 2022 - "Antisocial Personality Disorder, Diagnostic Criteria")
"A. A pervasive pattern of disregard for and violation of the rights of others occurring since age 15 years, as indicated by three (or more) of the following:
1. Failure to conform to social norms with respect to lawful behaviors, as indicated by repeatedly performing acts that are grounds for arrest
2. Deceitulness, as indicated by repeated lying, use of aliases, or conning others for personal profit or pleasure.
3. Impulsivity or failure to plan ahead
4. Irritability and aggressiveness, as indicated by repeated physical fights or assaults.
5. Reckless disregard for safety of self or others
6. Consistent irresponsibility, as indicated by repeated failure to sustain consistent work behavior or honor financial obligations.
7. Lack of remorse, as indicated by being indifferent to or rationalizing having hurt, mistreated, or stolen from another
B. The individual is at least age 18 years.
C. There is evidence of conduct disorder with onset before age 15 years.
D. The occurrence of antisocial behavior is not exclusively during the course of
schizophrenia or bipolar disorder."
The important thing to remember is that the DSM specifically states it is not meant to be used like a cookbook, where a list of ingredients makes a final outcome. That is to say, having ASPD isn't as simple as having 3/7 of the numbered criteria and fitting the lettered criteria. There is nuance to understanding what ASPD looks like and feels like, the diagnostic and associated features sections, development criteria that must also make sense (aka what, as far as we currently know, are either genetics and/or environments that cause ASPD) within your life experience, as well as differential diagnosis to make sure the symptoms don't fit better elsewhere.
The associated features section of the DSM-V TR section on ASPD is fairly long, so I am unable to put all of that here.
The differential diagnosis section of the DSM specifically mentions a few types of disorders to look out for that may appear to be ASPD based on symptoms alone, which I can list here.
Substance Use Disorder: If someone would also qualify for a substance use disorder diagnosis, then ASPD is only diagnosed if ASPD symptoms were present from young childhood and to present day. Both can be diagnosed, even if both were present in childhood and adulthood, but it is not ASPD if no ASPD traits were shown in childhood prior to the use of substances.
Schizophrenia and Bipolar disorders: If ASPD symptoms are only present during episodes associated with Bipolar disorder (manic episodes) or Schizophrenia (psychosis), then that isn't considered ASPD.
Other Personality Disorders: ASPD *can* co-occur with other personality disorders, but you want to research all of them to be certain that it a different PD doesn't fit better than, rather than in addition to, ASPD.
(From ICD-10 Dissocial Personality Disorder)
"Personality disorder characterized by disregard for social obligations, and callous unconcern for the feelings of others. There is gross disparity between behaviour and the prevailing social norms. Behaviour is not readily modifiable by adverse experience, including punishment. There is a low tolerance to frustration and a low threshold for discharge of aggression, including violence; there is a tendency to blame others, or to offer plausible rationalizations for the behaviour bringing the patient into conflict with society."
(It is worth noting the word "gross" used in the phrase gross disparity is referring to a secondary definition of gross, meaning large/important/marked/prominent. They are not being bluntly ableist on main in the ICD).
In the ICD, they note exclusions, which I believe is similar to the differential diagnosis section in the DSM, for Emotionally Unstable Personality Disorder (BPD) and Conduct Disorders.
Overall, this criteria has its own serious issues for both versions, but it is the diagnosing criteria (current for the DSM and recent but not current for the ICD, as mentioned above) for Antisocial/Dissocial Personality Disorder and therefore needs to be a part of any research into self diagnosis.
I would highly recommend looking into the DSM entry itself for ASPD as it is lengthy but thorough (and yes, somewhat stigmatizing) in its explanation of how ASPD tends to present itself. Putting the term PDF after DSM-V TR definitely does (cough) not (cough) produce some results that would aid you in this, and idk why anyone would do that when there is a perfectly legal way to buy the DSM for over $100 for a PDF version.
I hope this helps!
#aspd-culture-is#aspd culture is#aspd culture#actually aspd#aspd#aspd awareness#actually antisocial#antisocial personality disorder#aspd traits#dsm v#dsm v tr#dsm#icd 10#icd 11#icd#icd10#icd11#anons welcome
9 notes
·
View notes
Text
was going through my notes app and found my list of smurfs disability headcanons that ive built up over time, and i just straight-up directly quoted the DSM-5 on brainy's bit? my psychology special interest strikes again

people who know me irl think i only have one special interest (the smurfs) but little do they know im also super interested in psychology and what symptoms together qualify as what disorders.
i also have it written on the note that handy smurf can't be diagnosed with bipolar disorder, because even though he does have manic episodes and depressive episodes, those episodes don't last long enough for him to qualify for a diagnosis. in order to qualify for bipolar 1, manic episodes need to last at LEAST a week; and in order to qualify for bipolar 2, hypomanic episodes need to last at LEAST 4 days.
5 notes
·
View notes
Text
14
Bria was able to get out of her modelling contracts without being held liable. Her manager threatened a lawsuit for abuse and trafficking. She was still working on her deal with Converse. The high tops she designed were selling fast! Her fans begged their parents to let them buy them. Some said yes but others said no. They were not going to buy a twenty-dollar pair of shoes. The media reported on her being in rehab.
Her publicist put out a statement saying she was getting help for her mental health. She asked for privacy for her and her family. Bria was doing a lot better! She had regular meals and a routine. Every night, she crawled into bed and slept. She was evaluated for bipolar disorder. Since the symptoms were similar to her ADHD, it was hard to get a diagnosis.
Mike visited her after forty-eight hours. She no longer looked tired. Rather, she was the woman he loved. She had her usual ADHD energy. He was thrilled! She was hanging on by a thread when she was hospitalized. When they went to her room, Micha was there to greet them. He sniffed his leg before rubbing against it. Hi, human. He sighed. It was inevitable. The cat was not going to give up on him. She joked about cats choosing people who hated them. He laughed.
Rob was going to bring Mowgli when they were in the studio. She thought that was an awesome idea. He laughed because he missed her energy. Micha went to his cat tree and climbed up. He made himself comfortable before lying down. After an afternoon of playing, it was time for a nap. He needed his energy to run around later.
“The other day, we discussed whether his name is pronounced Mika or Mischa during group therapy. I call him Mika but some of them thought his name was Mischa. It was a twenty-minute discussion.”
“Mika or Mischa. I thought his name was Mika, like mine.”
“That's what I said. I guess it's Mischa. I guess I could call him either because he doesn’t listen to me anyway.”
He laughed. Rob was experiencing the same thing with Mowgli. Cats were strange animals. They were picky about what they liked and didn’t like. But they noticed a change in him since getting Mowgli. He was less anxious and depressed. Mowgli distracted him from the thoughts in his head. He also provided him with unconditional love. As a kitten, he made him laugh because he was always getting into something. He meowed when he needed help.
Sometimes he cleaned his apartment with him in a baby wrap. He loved hearing him purring. Where did he get the wrap? One of his neighbours gave it to him as a joke after he brought him home. Her baby was too big for it, so she was trying to get rid of it. Did he want it? Sure. He figured if he didn’t use it, he could donate it.
But he loved it the first time he was placed inside. Brad joked that he had changed him. What the hell did you do to Rob Bourdon? He had to admit it was adorable! Yes, he was aware that cats ate meat and he was okay with that. Depriving them of that would be abusive. He wouldn’t get a cat. Maybe a dog. He could see the other guys getting a dog. Maybe Chester would get all sorts of animals. Dave was also an animal lover.
They came together and talked about what they should name their band. They tried to register the domain Lincoln Park but it was already taken. Joe brought up her suggestion of Linkin Park. How was that spelt? L-i-n-k-i-n Park.
“To quote her. That sounds awesome”, Joe said.
They laughed. Finally! They had their band name. Dave stepped away for a while to tour with his band, Tasty Snax. They were a Christian ska and punk band, who were going around the country playing different Christian music festivals. In his place, they brought in Scott Koziol and Ian Hornbeck. Where was Bria? They heard she was in rehab.
Yes, that was true. Mike went through everything. She was so exhausted physically. They were angry because she could have died. At the time, they were trying to get her out of her contracts. He was happy to report that was successful. They were thrilled and relieved! Could they visit her? He thought that was possible. Though, he would check with her to see if it was a good time. Where was her cat? He was with her. The centre she was at was pet-friendly.
Micha was not a happy cat. All he wanted to do was run around downstairs, but his human was being mean. He pawed at the door of her bedroom and meowed. Nope. She was not letting him out. Why? Because she didn’t want him getting in everyone’s way. She would open the door when it was time for dinner. Meow. Knock knock. The door opened, giving him an escape. She was annoyed because she had to go down and find him. Well, she had to go downstairs anyway because she had visitors. She got up from her bed. It was her parents. Jasper grabbed Micha.
“I don’t think you’re supposed to be out here.”
Meow! No, she confirmed he wasn’t. They went up to her room. After closing the door, he put him back on the floor. Thank you. How was she doing? She was okay. Just tired. That was why she wasn’t participating in any of the activities. Why was she tired? She shrugged because she didn’t know. Was she eating? Yeah. They made sure she had three meals a day. Breakfast, lunch and dinner. She ate until she was full, though her stomach couldn’t hold that much food.
She was underweight because of the cocaine. The goal was to get her back to where she was before. Her normal weight was around a hundred and thirty pounds. Currently, she was at a hundred and ten pounds. Her unhealthy weight loss contributed to her having symptoms of a heart attack. She brought up being screened for bipolar disorder.
They talked about that. If she was diagnosed, they would do everything they could to help her. That was what Mike said. It was true. She wanted to go back to making music because it made her happy. Of course. Just because she had a mental illness, it didn’t mean her career was over. It just meant she had to be mindful of how much she was taking on. Meow! Micha went back to pawing at the door. Let me out! Let me out!
They got up and he ran out as fast as his paws could take him. He ran into the kitchen and meowed at the humans walking by. I’m hungry! Humans, I’m hungry! He was given his dinner in a fancy cat bowl. Yum! Thank you, human! It tasted like chicken! Micha, you’re supposed to wait for me. He grumbled as he continued eating. Everyone grabbed a plate, silverware and their drinks before sitting down at the table. Her meal was made separately so it didn’t come into contact with gluten. Thank you. She saved two seats for her parents. Everyone was winding down from the day. They talked to each other while they ate or they ate quietly.
@zoeykaytesmom @feelingsofaithless @alina-dixon
1 note
·
View note
Text
My mental health journey LOL
Note: Not exact quotes, but the general idea lol
Me, watching psych videos, taking psychology courses, going though psychiatric nursing in the nursing program, reading the DSM-V, and taking psychological assessments for fun: hmmm, I think I might be bipolar.
My 1st psychiatrist: So you mentioned bipolar but I think it may just be major depressive disorder and generalized anxiety with panic disorder. lets try wellbutrin.
Wellbutrin: *almost kills me*
My 1st psychiatrist: Oops! Lets try lexapro and buspar and ativan 1mg 3x a day for your depression and anxiety. Also, ADHD is a possibility but the meds might not be good for you due to the anxiety so lets wait.
Lexapro: *Makes mood fluctuations worse - now going from happy to depressed to pissed off to giddy to severely depressed all in one day*
My 1st psychiatrist: Weird. But lexapro can do that. Here's some Lamictal, it stabilizes mood.
Lamictal: *Helps*
My mental health: *stable but not great*
Me: I don't think these do much, I'm gonna stop.
My 2nd psychiatrist: So based on your history I think we should restart all your meds.
Me: Do you think maybe it's bipolar?
My 2nd psychiatrist: Nah, let's stick with your previous med combo.
Me: OK sure, maybe they did help.
My mental health: *no better than the 1st time*
Me: Nah, I think I'm gonna stop this isnt it.
My 3rd psychiatrist: Hi, first of all - who let you take 3mg of Ativan for years? That's not good. We're not gonna do that. Oh, you're off all your meds? That's fine - let me see how you are baseline.
*months later*
Me: Hey, do you think it could be bipolar or ADHD?
My 3rd psychiatrist: Could be ADHD but I think if we went with stimulants your anxiety would be horrible again and you do have mood fluctuations but they could just be based on your situation. Do you want meds to help? You can always stop them later. We can try the lexapro and buspar again and once your anxiety is under control we can talk about meds for that.
Me: Nah, I'm ok I don't want meds. Besides the lexapro by itself made my mood swings so bad I felt like I was loosing my mind.
My 3rd psychiatrist: That's cool, if you change your mind lemme know.
Me: K.
My 3rd psychiatrist: Hey, so I'm leaving and you're gonna have a new doc.
Me: :(
My 4th psychiatrist, after one session: Right, so you're bipolar.
Me:

My 4th psychiatrist: So your mood got worse on lexapro alone? SSRIs do that with bipolar. Your anxiety is likely a symptom of your bipolar which is why the buspar didn't really help. The ativan was what was calming it because it was basically sedating you to a degree. You say you think it's situational but going through your file you report continued mood fluctuations despite what's going on in your life. You don't adapt to change well, which is also a bipolar symptom. So we should try Vraylar.
Me: That's brand name only, my insurance won't approve it. I'm already fighting them for Taltz, which is also brand name only, so I don't want to throw another thing at them that could distract from that. Besides, I don't want meds in general, let alone anti-psychotics.
My 4th psychiatrist: Anti-psychotics don't mean I think you're psychotic, it's just the type of medication class. We could always try quietipine, that's the same type of med but a generic.
Me: I don't want meds. Especially not that type because I know all the side effects and they scare me.
My 4th psychiatrist: Then why are you here?
Me: I need to have a psychiatrist to approve therapy.
My 4th psychiatrist: OK, we will revisit this.
Me, out of curiosity: *checks after visit notes, sees diagnosis of bipolar, unspecified and adjustment disorder with mixed disturbance of emotions and conduct*
Me: That sounds fucking rude. >:(
Me, to my therapist: They said I'm bipolar >:(
My therapist: Hear them out...
Me: Do you think maybe possibly it could be bipolar personality disorder?
My therapist: I remember you mentioning that when we first started our sessions together, I can't diagnose so you should bring it up with your psychiatrist.
Me, to myself: Nah, not gonna do that.
My 4th psychiatrist: So, meds?
Me: Fine, but I only want to go back on Lamictal because I don't want to take antipsychotics.
My 4th psychiatrist: What side effect is the one making you feel that way?
Me: Tardive Dyskinesia.
My 4th psychiatrist: That's such a rare thing that really only happens to people on high doses for years and years. Mostly seen with schizophrenia, in my experience, due to the high doses needed. You'd be on 25mg.
Me: Nope. Lamictal or I walk.
My 4th psychiatrist: -__- fine.
Me: Also could we do the buspar again? My anxiety sucks.
My 4th psychiatrist: No. It'll make it worse because your anxiety is a symptom and adding buspar is gonna mess with your existing chemical imbalance and make the lamictal not fight it as well.
Me: >:( I'm pretty sure my anxiety is it's own thing.
My 4th psychiatrist: We'll see.
Me: *back on lamictal. dose started at 50mg and is currently up to 150mg. I was taking buspar as prescribed by my primary doc and I have stopped taking that after switching to 150mg of lamictal*
My 4th psychiatrist: So, how we doin?
Me: I feel better, but I think it's the weather change and the sun being out longer.
My 4th psychiatrist: I'm glad it's working. Let's keep going and I'll check in after a month.
Me: K
Me: *out of curiosity, checks after visit notes: sees diagnosis of bipolar, unspecified, and the adjustment disorder with mixed disturbance of emotions and conduct* Ok, I mean that's what it said last time. And maybe the meds are working and it's not just the change of seasons.
Me: .... wait a minute. *Sees it also now says Bipolar personality Disorder*
Me:

Apparently the moral of the story is only *I* am allowed to suggest I am bipolar and shit and no one else is even though the reason I ever started looking for mental health help in the first place was to figure out what is wrong with my head and fix it.
#also note: I didn't doctor hop on purpose. the first place i went to was money hungry and shitty -the second i had to stop going to because#i couldnt afford to keep going and the third place i had a doc and they left for a different position as mentioned a little above#i was also treated briefly by my old primary care doc and that didn't go well and my second primary care doc did try to help with the buspa#but i stopped that because MAYBE my 4th psych doc is on to something#all i know is since stopping the buspar but keeping up with the lamictal my anxiety hasnt worsened at least#and rn its hard to say if its gotten better because im stressed out over this exam so i cant judge it atm until that's over and i know if#i passed the class or not
1 note
·
View note
Text
What are Mood Swings | Instantly Understand 5 Causes
1) What are Mood Swings?

“Has it ever happened to you that you feel grumpy one minute and happy the next?”
That you are joyful and chirpy jumping around the house at the moment and the other second you are lying on your bed rethinking your whole life?
Don’t be afraid, these emotions are just caused by your hormones and do not purely mean anything. These are merely just mood swings. A mood swing is a sudden or intense change in an emotional state. During a mood swing, a person may quickly switch from feeling happy and upbeat to feeling sad, irritable, or angry. All these can be counted as mood swings symptoms to help you rectify when you are experiencing one!
Did you know the 7 benefits of laughing therapy?
2) What are Mood Swings in Men & Women? 5 Common Causes
Often mood swings are associated with women but the truth is that these mood swing disorders are faced by all genders. Usually, the main contributors to mood swings are diet, sleep, and substance abuse. The most common causes of mood swings affecting anyone and everyone are:
Bipolar disorder
It is referred to as a mental health condition or a mood-related disorder that causes extreme mood swings that include emotional highs (mania or hypomania) and lows (depression). An individual with bipolar MDD, also referred to as clinical depression, is a significant medical condition that can influence multiple areas of their life.

Your body and brain take a time-out from the rest of the world when it is at sleep. Bedtime is the time when your body heals the most. Hence when you are short on shut-eye, you tend to experience crankiness and depression. Meaning that sleep deprivation can cause you to have contentious moods wings.
Due to high-level mood swings, sleep deprivation can cause you to have bad mood swings for no reason. Studies show that sleep-deprived people report increases in negative moods (anger, frustration, irritability, sadness) and a decrease in positive moods.
Low blood sugar
Have you ever gotten “hangry” — hungry and angry at the same time — low blood sugar may have been to blame. This happens to some people when they go long between meals. Low blood sugar may make you feel mad, upset, lonely, or confused. You even may feel the need to cry or scream.
To regain yourself, it is recommended that you eat something. Your brain, the center of your thoughts and emotions, needs glucose to do its job. If you don’t have enough glucose “feed your brain,” meaning you have low blood sugar levels, your brain can go “haywire”. Even though it appears like you are overwhelmed by anything around you, this can be a physical response to low blood sugar/glucose (hypoglycemia).
Stress
Stress can occur at any point of life, at the office due to work, at home due to chores, or any other reason. Chronic stress can lead to mood swings disorder, negative thoughts and you might feel sad, angry, or bitter. You can start feeling better when you distract yourself from the core reason for your stress. Daily exercise is also known to be an escape from stress

It may be surprising to know for a few that even caffeine can cause mood swings to some people. Consumption of Coffee, soda and other beverages can be the reason for your mood swing. Because caffeine encourages your nervous system, it can cause you to feel more alert than usual. If you consume it often, your body gets used to its effects. By that point, if you attempt to cut back results in mood swings depression, for example, it forces you to feel tired, annoyed, nervous, or anxious.
Read some that’ll make your day!
spread-happiness quotes make your day!
3) What are Mood Swings & How to Control Them?

Mood swings might be difficult to manage but here are some steps you can take to help ease them:
Create a schedule: Try to create a routine for yourself, especially when it comes to eating and sleeping.
Focus on what you are feeling right now: Exercise daily: Exercising regularly has several benefits for nearly all aspects of your health, including mood. It relaxes and frees your muscles providing you be more calm and stable.
Get sufficient sleep: A good night’s sleep is important, and being sleep-deprived can influence your mood.
Eat a healthy diet: A balanced healthy diet can improve your mood and keep you healthy. Here are some tips for sticking to a healthy diet.
Practice relaxation: Engage in calming practices like yoga or meditation whenever having insatiable moods.
Avoid stress: Easier said than done, right? If it is impossible for you to bypass the stress, try deviating from the reason of stress with the help of music and talking to friends etc.
Talk it out: Find someone to talk to, such as a friend, family member, or professional counselor.
Above mentioned were some of the natural remedies for mood swings and irritability to answer your question of ‘how to control mood swings naturally’
Need some personal advice? Talk to us at GoodLives | Mental Health Services
0 notes
Last Seen Blogs

les-reading-blog
Untitled

psy-facto
Psychology Thoughts
viennajetschko
Cartoons and lousy jokes

sunwzo
watch it

plotmania
fated to love you