#"Mental health disorders symptoms"
Text
10 Common Symptoms of a Mental Breakdown
10 Common Symptoms of a Mental Breakdown
Introduction
Feeling overwhelmed or having a tough time coping? You’re not alone. Many of us go through periods where it feels like the world is crashing down around us. This state often signals a mental breakdown, a term that describes a period of intense mental distress. During this time, managing day-to-day tasks can feel impossible. By understanding…

Vezi pe WordPress
#"Adult ADHD symptoms"#"Agoraphobia symptoms"#"Anxiety disorder signs".#"Anxiety symptoms"#"Bipolar disorder symptoms"#"Burnout symptoms"#"Depression symptoms"#"Emotional breakdown symptoms"#"Mental breakdown recovery"#"Mental breakdown symptoms"#"Mental health disorders symptoms"#"OCD symptoms"#"Panic attack symptoms"#"Post traumatic stress disorder symptoms"#"Psychological distress symptoms"#"PTSD triggers and symptoms"#"Schizophrenia symptoms"#"Signs of a nervous breakdown"#"Signs of mental illness"#"Stress symptoms"#"Types of mental disorders and their symptoms"#Anxiety#Depression#EmotionalHealth#MentalBreakdown#StressRelief#Symptoms
0 notes
Text
A recent review of the science behind the psychiatric discourse concluded that "no biological sign has ever been found for any 'mental disorder.' Correspondingly, there is no known physiological etiology". This conclusion also became clear to the APA's own DSM-5 task force when they began work on the new manual in 2002. As Whitaker and Cosgrove record, in reviewing the available research evidence it was plain to the committee members that "[t]he etiology of mental disorders remained unknown. The field [of mental health] still did not have a biological marker or genetic test that could be used for diagnostic purposes." Furthermore, the research also showed that psychiatrists could still not distinguish between mentally healthy and mentally sick people, and consequently had failed to define their area of supposed expertise. This issue was recently highlighted with reference to comments made by Allen Frances, the chair of the previous DSM-IV task force. When the DSM-IV was published in 1994, it stated that "mental disorder" was "conceptualized as a clinically significant behavioral or psychological syndrome or pattern that occurs in an individual and that is associated with present distress (e.g., a painful symptom) or disability (i.e., impairment in one or more important areas of functioning) or with a significantly increased risk of suffering death, pain, disability, or an important loss of freedom".
However, as the architect of the DSM-IV, Frances was later quoted by Greenberg as stating of the above definition, "[h]ere's the problem . . . There is no definition of a mental disorder . . it's bullshit . . . I mean you can't define it." The lack of knowledge on mental health and illness has haunted the entire history of psychiatry. Some have dismissed critics who highlight this fundamental hole in the science of psychiatry as "antipsychiatry" or "mental illness deniers." Such attacks on scholars who attempt to investigate the accuracy of the central pillars of psychiatric knowledge should further concern us, as it perhaps signals that plenty in the profession are already aware of the flimsy nature on which their "expertise" continues to rest. Together with an understanding of the history of the psychiatric profession—summed up by Scull as "dismal and depressing"—I would argue that it should be the duty of all social scientists concerned with the mental health field that, in good conscience and putting the needs of the public first, they remain highly sceptical of a psychiatric discourse that poses as expert knowledge on the mind but produces little actual evidence to back up the assertions made.
Bruce M.Z. Cohen, Psychiatric Hegemony: A Marxist Theory of Mental Illness
71 notes
·
View notes
Text
haikyuu!! neurodivergent headcanons 💕
tw: several listed mental illnesses, some of these are solely off of vibes but most of them I have reasons lol
note! I do not believe autism is a mental illness or something that is "wrong" with an individual, hence why the title is "neurodivergent" rather than "mental illness". just had to put that out there! to all my neurodivergent babies I love you!
a/n: hello! as a neurodivergent like myself (depression, anxiety, ptsd, bulimia, etc etc) i thought it would be really cool to do an analysis on one of my biggest hobbies (psychological illnesses) and relate them to haikyuu characters! some of them have a deeper explanation because I feel so strongly about it.
attention-deficit hyperactivity disorder (ADD/ADHD)
BOKUTO, hinata, NISHINOYA, atsumu, lev
generalized anxiety disorder (GAD)
sugawara, OIKAWA, asahi, yamaguchi, yachi, aone, akaashi, tendo
social anxiety disorder (SAD)
asahi, KENMA
post-traumatic stress disorder (PTSD)
oikawa
depression (MDD)
oikawa, KENMA, kuroo, suna, matsukawa, tendo
autism
sakusa, USHIJIMA, kageyama, kyotani, kenma
eating disorder(s) (AND, BND, BED)
OIKAWA, KENMA
obsessive-compulsive disorder (OCD)
oikawa
borderline personality disorder (BPD)
daishou
insomnia
kuroo, kenma, osamu
hypersomnia
suna
analysis under the cut
it's pretty obvious that bokuto struggles the most to self-regulate, even to others, but I personally believe that oikawa struggles the most with his mental health.
like almost everyone in haikyuu, oikawa is obsessed with volleyball, but he takes it to a point of overexertion and taking his anger and frustration at his own inadequacies out on others.
I really think oikawa's relationship between he and kageyama and he and ushijima are the ones that show how bad his anxiety is
ushijima and kageyama both don't understand the emotions oikawa is feeling which could be written off as them not understanding their talents, but I think it's something more
to me, I feel it is blatantly obvious that ushijima is autistic. he just so frequently seems to be unable to read the emotions of others or takes things literally when it's something else intended. I'm not autistic, though, so autistic community, let me know your thoughts!
bokuto and hinata both have an insane amount of energy, but struggle to be successful in school. sports works for both of them because their focus is constantly needed to be diverted or "all over the place" that it helps them be great players
kuroo is one of those other characters that I feel like I'm reaching to say he has mental health struggles but to me it just comes off in vibes. first of all, any kid with divorced parents should be in therapy so I feel there's definitely some struggles there.
I think kuroo is the type that hides his struggles and pretends they aren't happening. he puts a lot of pressure on himself to be the best at everything he does, and so he feels he doesn't have time to deal with the emotions that leave him feeling empty
kenma was someone I immediately felt was autistic. he has so many key factors like an obsession/hyperfocus on his hobbies and trouble socializing (social anxiety).
kenma has some of the strongest evidence toward my beliefs, specifically in this quote: "I'm not good with people, and I don't want to interact with them. and yet, I'm very concerned about what others think of me." like, tell me that doesn't radiate autistic/SAD vibes!!!!
idk what it is, like inadequacies or what but I genuinely believe oikawa has some kind of trauma. like he's definitely carrying something that so heavily effected him that it controls the choices he makes in life
I don't have much evidence that suna has depression, it's just a vibe because of his mannerisms and what he says. I think it's the kind where it's well-managed, but it shows up in physical symptoms like apathy more than anything.
atsumu gives ADHD vibes solely because of like how all over the place he is and how he can't always seem to properly get out what he's trying to say lol
sakusa is one that to me could be seen as "done with your bullshit" but I think he also hates crowds (like me, I mean who doesn't) and struggles socially probably because of anxiety or autism. not sure!
basing daishou off of vibes, too, because if I'm being honest all I've seen in the show is him having hostile relationships or being on-off with them, though its certain I could be reading too much into it, but that's the fun of headcanons.
do you agree with what I wrote? I would love to hear your thoughts!
#haikyuu!!#haikyu x reader#kuroo headcanons#haikyū!!#haikyuu headcanons#neurodiverse stuff#kenma x reader#fem!reader#kenma kozume x reader#kuroo tetsuro x reader#suna headcanons#suna x reader#suna rintaro fluff#sakusa kiyoomi x reader#atsumu miya x reader#osamu miya x reader#oikawa fluff#oikawa x reader#kageyama tobio x reader#hinata shoyo x reader#nishinoya yu x reader#ushijima wakatoshi x reader#tendo satori x reader#daishou x reader#bokuto kotaro x reader#kuroo x reader#yamaguchi tadashi x reader#akaashi keji x reader
279 notes
·
View notes
Note
if we're talking personality disorders (of the cluster b variety). obvi its not 1=1 but its far more likely and reasonable to say toga has bpd (with izuku or ochako being her "favorite person") than aspd. also when people call villains (or characters they don't like (← seen this one more than the first tbh)) "unsympathetic psychopaths", it really feels like they know nothing about aspd, personality disorders, and how they form. It also just feels kind of ableist towards real people with aspd? idk maybe i'm seeing things that's aren't there
These people know that aspd (and other personality disorders) form due to outside factors right? obvi there's the genetic factors but that just increases the possibility. these outside factors typically tends to be factors that is in some way traumatic for the person in question like emotional/mental abuse or neglect (*gestures to dabi*)
if anything, based off of that alone, toga being a "psychopath" just makes her more sympathetic in my eyes and people around her even more unsympathetic than they already are and I doubt anyone calling her a "psychopath" without aspd in mind wants that
.
.
.
this is also how i feel about people needless throwing around the word "narcissistic"* when it comes describing bakugo. (saying this as someone isn't a fan of him). bakugo with npd** could make him a more interesting if written correctly*** tbh and could probably be backed up in canon but in turn it would force people to seriously think and question if he actually had a good childhood and good parents… which from what i've seen alot of anti-bakugo people (including the ones that call him a "narcissistic") believe he has
*i'm sure there's bakugo stans out there call him "narcissistic" without npd in mind but atm i've only seen bakugo antis do that
**same with aspd
***without portraying bakugo as an ableist stereotype and/or excusing his actions
.
sorry abt the rant i'm just tired of the demonization surrounding personality disorders
You're definitely correct anon in saying that people tend to use words they either don't know the full meaning of or just mental health issues to demonise characters they don't like and this is a problem within all fandoms I have interacted with not only MHA.
When people use the words "psychopath" or "narcissist" it's rare to see them using it in the right context as most of the time it's used to demonise a character. For example take atla I have seen plenty of people label azula a psychopath but they do that to demonise and dehumanise her not to actually say that she is mentally ill. The same thing is done with characters like toga, Dabi, shigaraki and more!
Now I know that you're mainly quoting of the ask that @sapphic-agent sent me and actually she has made it clear that she doesn't view toga as psychopath and actually brought light to the issue of people dehumanising and purposefully misinterpreting the leauge. Now I don't know much about aspd in general but from what I have seen toga does seem to have some symptoms of aspd but it also makes sense to speculate that she may have BPD (none of this is cannonically confirmed but they would make for some interesting headcanons). Also like you mentioned it would be incredibly interesting to explore how toga got to such a mental state in the first place as mental health issues can happen to a variety of reasons for example or could be an environmental or social issue as we see that toga wasn't given the right support at home and was taught to simply build a mask and burry her urges deep down until it all broke and she broke, toga associated blood and cannibalism with love and self expression from early on. Also, it could be a biological factor since toga was born with a strong fascination for blood.




Overall, toga and her mental state is heavily influenced from all of those factors and it would be interesting if she was cannoncially diagnosed and had that be explored in depth.
However, mha does already have a character who is heavily implied to be mentally ill which is twice. Twice is heavily implied within the show to suffer from DID (dissociative identity disorder) and I think the way horikoshi presents this is really interesting it's to the point that it's incredibly integral to twice's character whether that be his name or what his quirk is.
We see exactly how his mental state worsens in his backstory and how he has reached his breaking point multiple times. Twice is also presented as the most redeemable of the leauge and we see that even with that the system doesn't care for him as twice mercilessly kills him even though he had a high and good chance of being saved and redeemed.
I do wish that hori spent a bit more time delving deeper into twice and developing him before killing him off while also making his death have a long lasting impact between characters (specifically the league)


I think what's interesting is that hori doesn't demonise jin for his mental issues but addresses them in a serious manner and a lot of the scenes where we do see him struggling we are able to feel a lot of sympathy for him.
This ends up being the exact opposite of what people usually do by demonising mental health and using it to dehumanise characters. Horikoshi uses it to humanise his characters whether that be twice who struggles with DID or tamaki who struggles with social anxiety. These issues are brought to light and aren't a one time thing but it's something that's integral to their character.
Now, moving onto my final comment : yep it's bakugo!
I admit that I have seen many bakugo antis and critiques label bakugo as a narcissist. I also believe that they don't inherently speak of the mental disorder when labeling him in such a way but use the word in exchange of other terms for bakugo like self 'absorbed' or 'selfish' or 'only cares for himself' etc.
Now, I agree this is bad and shouldn't be done. I do however want to offer my own view on this subject (iam also a big bakugo critic/anti) I personally don't think that bakugo suffers from Narcissistic personality disorder and I don't think that mitsuki is abusive towards her son.
I think that the scene with mitsuki hitting bakugo was played in a comedic light. This is the only scene we see mitsuki act aggressive towards bakugo in the whole manga while in the other scene she expresses concern over her son (for example katsuki doesn't like rain etc). I think @delawaredetroit post surrounding this has the best explanation
I also want to add the fact that bakugo feels comfortable enough to sit next his mother. He is right in between his parents (he could of sat away from her closer to his father if he wanted to but he didnt). Bakugo also feels comfortable enough to express himself in such a manner whether that be him calling his mother "hag" or also shouting at her when he is equally pissed off.
I do think that because the manga had already made it clear that abuse was a theme that was in the story and gave us an example of abuse (the todoroki family) that many did raise their heads at this scene and may of been concerned that this is abuse when it's not but its hard to spot since it's being presented in such a weird manner.
You do have a point bakugo's behaviour comes from somewhere and that's not talked about enough. I personally think that horikoshi didn't explore how society influenced bakugo's behaviour and his raging quirkless discrimation (maybe it's because hori didn't want to paint bakugo in such a bad light so he didn't make him prejudiced against the quirkless and didn't explore the theme of quirkless discirmation that he implemented into the story). There is also the superiority and inferiority complexes that bakugo seems to have that could be a result of a mixture of factors (biological, social and environmental) Now his brash behaviour could come biologically from his mother and it turned worse due to his environment where he was built up to be this guy who had everything so he should be happy as he fits into the status quo.
Tldr: mental health shouldn't be used as an excuse but it also shouldn't be used to demonise characters either.
#mha#bnha#thanks for the ask#thanks for the ask!#thanks anon#thanks anon!#anti fandom#fandom critical#twice#my hero acedamia#my hero academia#toga#bakugo critical#boku no hero academia#asks#yeah its deffo a trend to demonise characters by using mental illnesses#i dont think people do recongise that though#since the words psychopath and narcissist are thrown around very casually#almost as if its equal to the word hypocrite#props to hori here#i know i critique him a lot but i give credit where its due#anti bakugo#anti bakugou#tagging to be safe#horikoshi critical
22 notes
·
View notes
Note
You seriously need to stop spreading misinformation and making these outrageous claims. They are rooted in pseudoscience, and what you’re saying is harmful to everyone, including yourself. Being a system requires high levels of dissociation, which is the result of trauma, and not even everyone with trauma develops that disorder. Most people claiming to be endo are either putting that label because they don’t consider their trauma severe enough to have a dissociative disorder (which is sad and rooted in misinformation), confusing their symptoms with another mental health disorder, or blatantly faking it. Promoting endogenic as normal strays people away from true recovery. I hope you eventually realize what you are doing is wrong. You most likely are genuinely ill, but this is wrong. If you are gonna have these medically incorrect views, you must keep it to yourself.
Pseudoscience, you say?
Do you... actually comprehend the gravity of the accusations you're making here?
Again, these are the quotes from Transgender Mental Health, a book by a reputable doctor that passed both peer and editorial review to be published by the American Psychiatric Association.
Your position here, then, is that the American Psychiatric Association is publishing pseudoscience!
This is a MASSIVE accusation to put out there with no evidence to back up your claims.
Additionally, the World Health Organization's ICD-11 has also basically said the same in regards to non-disordered plurality. Only, rather than use the term plural, it says that you can experience the presence of multiple "distinct personality states" without a disorder.
"Distinct personality states" being the ICD-11 and DSM-5's term for dissociative identities.
Is this pseudoscience as well in your opinion?
Because last time a group were accusing the World Health Organization of pseudoscience, they were trying convince people to not take their COVID shots!
#syscourse#pro endogenic#pro endo#systempunk#syspunk#covid#covid 19#anti vaxxers#world health organization#plural#systems#endogenic#plurality#multiplicity#sysblr#psychology#science#psychiatry#actually a system#actually plural
33 notes
·
View notes
Note
It's possible for alters to have their own mental health!!! Alters can have personality disorders that other alters don't have, I think what you're talking about is autism, ADHD and other disorders similar! (As those affect the brain and therefore affect the whole system, but personality disorders are a different sort of thing, so one alter can have a PD and the others might not!) We can provide links if you'd like ^^ /nm /info
Hey there Anon! Thank you for the offer. We also received the following anon from (probably) another user, which I'd like to address here as well:
Alters can have personality disorders: (link)
“✘ MYTH: ALTERS CAN’T HAVE THEIR OWN MENTAL HEALTH ISSUES IF THE MAIN SURVIVOR DOESN’T HAVE THEM.
They actually can, and many do. It’s extremely common for individual alters to battle depression, anxiety, OCD, bipolar, eating disorders, self harm, etc., while other members of the system experience no such thing. Some extremely differentiated systems may even need that system member to come forward and take medications that the rest of the system does not need and will not get. ..and their brain’s neurology responds accordingly.
But, make no mistake, most expressions of mental illness amongst alters are incredibly real and valid and should be treated as such.”
(cut up a little, the source is above, we're pretty sure the source is reliable, it seems so. We've also had other systems say this too, and to us that's how it works, as only one of us as far as we know are affected by NPD)
Firstly, I feel the paragraph that was cut out of the Beauty After Bruises section is very important for further context and explanation. It's quoted here below:
One note about some disorders, however. Non-verbal, poor eye contact, savant-like, or sensory-processing-disorder alters can be extremely common traits in DID systems. However, it’s important not to just jump to calling these parts “autistic” if the system as a whole is not autistic. It’s possible for alters to behave in ways that mimic their understanding of SYMPTOMS in other disorders they know about, while not actually possessing the neurology for them. This is a complicated subject we could try to elaborate more on at some point, but it’s just an encouragement to pause and not automatically label some parts as having certain conditions just because they show a few traits of them. It can cause a great deal of conflation and misrepresentation of those illnesses. It may also be purely based on discriminatory or uneducated stereotypes of those conditions that were adopted into a young child’s mind. So, it’s just helpful to check for that possibility first!
As Beauty After Bruises is saying here, neurology takes a place in this discussion. It seems as if this resource is mostly stating that alters can all struggle with mental illness, and can appear to struggle singularly with those illnesses symptoms -- in which case, the "This alter is a symptom holder" is exactly the language we feel comfortable with. Until we are able to research more, we're wary about spreading potential misinformation about how brains work.
As mods, we absolutely want to do our best to avoid spreading misinformation. From our understandings, NPD and similar personality disorders are caused by a structural shift in the brain -- something physical and concrete. Here's some of our resources we found on NPD.
Source 1: “They analyzed a total of 34 test subjects, of which 17 suffered from a narcissistic personality disorder… Using magnetic resonance imaging (MRI) methods, the scientists measured the thickness of the patients' cerebral cortex… The findings revealed that those subjects suffering from narcissistic personality disorder exhibited structural abnormalities in precisely that region of the brain, which is involved in the processing and generation of compassion.”
Source 2: “The decreased brain white matter microstructures among three clusters were found in the association, projection/thalamic and connection pathways of white matter in young adult males with NPD. The abnormal white matter brain regions may be one of the neuropathological basis of the pathogenesis of young males with NPD, and it may be related to white matter development in early adulthood."
Based on these sources, the moderators are most comfortable using the language of alters being symptom holders. Both sources indicate that NPD affects the structural nature of the brain, which would impact all of the members of the system. However, like Beauty After Bruises was suggesting, that doesn't mean that various alters don't reflect those symptoms in different ways. It's absolutely possible for alters to struggle more or less with disorders, or even seemingly not at all.
I hope this clarifies our perspectives. Thank you!
70 notes
·
View notes
Note
I'd love to hear about your thesis topic (if you're not already sick to death of talking about it 😂)!
Aa, thank you for reaching out, it's so nice of you to ask!!
I'm definitely not sick of talking about it yet! I suspect that it may be the other way around and people around me are starting to get sick of hearing about it 😅
The topic is broadly a mental health disorder which supposedly plagued early 18th century Britain interpreted through a philosophical lens.
More specifically, there was this physician and philosopher called Bernard de Mandeville, who was one of those people who had thoughts on absolutely every topic imaginable, spanning from economical and social theory to medicine (he was also a huge classics nerd but with people in the 1700s, that probably goes without saying).
Supposedly to gain more patients for his practice, he wrote this wonderfully weird medical treatise on how to deal with hypochondria (the name can be misleading, but back then it referred to an unspecified mental health issue close to our current understanding of depression). It is written in a form of a dialogue between a doctor and a patient, and it discusses various symptoms of the disease as well as practical advice on how to treat it (including some great wine recommendations and seemingly endless quotes from Horace and Ovid for some reason).
One thing that particularly fascinates me about the text is that it shows a kind of proto-therapeutic approach to the treatment of mental health issues and it places a lot of emphasis on the developing relationship between the doctor and the patient. The wife of the hypochondriac who suffers from the same illness as her husband is also present, so at times, I'm attempting to go for a slightly feminist angle (Mandeville was not exactly a feminist but some of his ideas about gender were genuinely progressive for a guy writing in the early 1700s).
I'm writing it under the philosophy department, so I sadly had to minimise the historical context in my actual writing. I did research it however! A lot has been said about how hypochondria characterised British people specifically and how an increasingly easy and comfortable life of the upper-middle class may have paradoxically contributed to it. It's also been linked to philosophers/men of letters since it seemed to have affected this group of people in particular (perhaps most famously David Hume who is my supervisor's number one guy).
The result I ended up with is a bit chaotic, but I genuinely had a ton of fun researching the topic! I got a chance to engage in one of my most favourite things in the world, which I guess could be called amateur psychoanalysis of people from the 18th century.
I've also argued by the end that it is useful to study early modern texts (and by extension all historical texts) since it helps us to see which aspects of the human experience remain unchanged over time. (Spoiler: although wine is no longer recommended as a cure, we don't differ that much from people living three centuries ago in all of the important ways. Most notably, we all need positive interactions with others for our mental well-being and to some extent, we all crave others' approval).
Actually getting it printed soon — then it's just anxiously awaiting feedback and then onto the defense.
Hope my answer is not too long or incoherent and thanks again for asking!
#thesis#thesis era#asks#✨#I can't write concisely I swear#writing an abstract was painful#philosophy#1700s
37 notes
·
View notes
Text
No mental disorder meets the scientific definition of “disease” recognizable to pathologists: a departure from normal bodily structure and function (Szasz, 2001). This reality is clearly understood by the current and previous directors of the NIMH who acknowledge the speculative status of existing biological theories (Insel, 2011) and caution that DSM diagnoses are “heuristics” not to be misconstrued as “natural kinds” or “real entities” (Hyman, 2010). It is therefore confusing to observe these same individuals state elsewhere that mental disorders “are recognized to have a biological cause” (Insel, 2010; p. 5) and are “real illnesses of a real organ, the brain, just like coronary artery disease is a disease of a real organ, the heart” (Hyman at the 1999 White House Conference on Mental Health, quoted in Albee & Joffe, 2004). Use of the term “disease” in the context of mental disorder reflects an expanded definition in which cellular pathology is replaced with subjective report of distressing or impairing psychological symptoms, the presence of biological correlates, or the assumption of an underlying disease state as yet undiscovered by science (e.g., “…mental disorders will likely be proven to represent disorders of intercellular communication; or of disrupted neural circuitry”; APA, 2003b). From this perspective, any DSM diagnosis is eligible for disease status (Peele, 1989), and what constitutes a “brain disease” is subject to the vagaries of the individuals in charge of determining the disorders and symptom criteria sets that comprise the latest version of the APA's diagnostic manual. [...] Given the limitations of existing knowledge about the biological basis of mental disorder, declarations that mental disorders are “brain diseases” (Volkow, n.d.), “broken brains” (Andreasen, 1985), or “neurobiological disorders” (CHADD, 2012) are perhaps best understood as the product of ideological, economic, or other non scientific motives.
–Brett J. Deacon, “The biomedical model of mental disorder: A critical analysis of its validity, utility, and effects on psychotherapy research.” Clinical Psychology Review 33 (2013), 846–861. http://dx.doi.org/10.1016/j.cpr.2012.09.007
180 notes
·
View notes
Note
Hi! Please feel free to ignore this, I am not trying to hate at all! Just curious!/gen
Why do you tak care of Rhea but not other vent littles?/lh /gen /curious
I know your mental health isn't the best, so I now that could be reason, I just thought that if it was, you would take a step back form Rhea too.
Again no hate what so ever!/gen
sending lots of love
Sorry if this came off as rude or offensive!/gen
Dear Anon
I am Mod E, I dont normally answer asks in anyway on Vaggie's blog. Im just here to monitor the inbox, make special announcements, and block problematic blogs, however, Mod Ocean (aka Vaggie) and I agreed that its probably best that I handle your ask in particular in order to allow you to help you get a better understanding of what actually is going on here.
We know you meant nothing offensive in your ask and that you are genuinely concerned about Mod Ocean and her mental health. However 'stepping back' from Rhea is not possible. This is because Mod Ocean and Rhea are the same person.
Now its a little hard for me to explain. Im going to be using terms generally used by systems (I myself am part of a system) but I want to make it ABUNDANTLY CLEAR:
MOD OCEAN DOES NOT HAVE DID AND IS NOT A SYSTEM NOR IS SHE CLAIMING TO BE A SYSTEM!
IT IS JUST EASIER FOR MYSELF (MOD E, A MEDICALLY RECOGNIZED SYSTEM) TO EXPLAIN THIS USING SYSTEM TERMINOLOGIES!
Mod Ocean has a diagnosis of BPD. One of the effects of BPD is (quote taken from the NHS website) "disturbed patterns of thinking or perception – "cognitive distortions" or "perceptual distortions" " I personally dont like the use of the term 'disturbed' here but that is straight from this website: https://www.nhs.uk/mental-health/conditions/borderline-personality-disorder/symptoms/
There isnt a lot of research into BPD and how these distortions manifest in individuals but for Mod Ocean, it manifests in almost alter-like personalities that have taken on an appearance and have histories all their own. They tend to 'come to front' to help Mod Ocean process the extreme emotional disregulation that comes with BPD.
Mod Ocean is my best friend, she has been a massive support in my own journey of discovering that im part of a system and encouraging me to speak to a therapist. Rhea is real. She has her own thoughts and feelings that can be hurt. I can always tell there is a massive difference when im talking to Ocean vs when Im talking to Rhea or Jadie vs when im talking to Vaggie.
So your ask was sent with good intentions, yes. But you also sent it under an incorrect assumption. Vaggie cannot take a step back from Rhea.
This is also part of the reason why Mod Ocean isnt always comfortable handling other vent regressors. They are always welcome to reach out to her, vent and cry and that but when they start getting violent/aggressive towards themselves or her is when she has to step back.
I hope this makes sense and helps explain the situation a bit better. If you have any further questions please reach out to me on my blog @the-hellion-collective and ill answer any questions you may have to the best of my ability.
~Mod E 👾
#hazbin hotel age regression#hazbin hotel agere#hazbin hotel roleplay#hazbin hotel rp#sfw age regression#caregiver vaggie#hazbin hotel#sfw age dreamer#hazbin hotel vaggie#vaggie#Mod E#important
16 notes
·
View notes
Text
The clinical description of PTSD captures the experience of, for example, a soldier who goes back home … Trauma in Palestine is collective and continuous. PTSD is when your mind is stuck in a traumatic loop. In Palestine, the loop is reality. The threat is still there. Hypervigilance, avoidance – these symptoms of PTSD are unhelpful to the soldier who went home, but for Palestinians, they can save your life. We see this more as ‘chronic’ traumatic stress disorder.
Samah Jabr quoted in an article by Bethan McKernan in The Guardian. ‘Chronic traumatic stress disorder’: the Palestinian psychologist challenging western definitions of trauma
Chair of the Palestinian ministry of health’s mental health unit says the clinical definition of PTSD does not fit the reality in Gaza
15 notes
·
View notes
Text
This is kind of just an unhinged meta rant about Rymin so do with it what you will. It's about Ryan's parents and how, despite having very little screentime, they really play into the story and the disagreements that Ryan and Min-gi have.
Ryan's dad only has one line and it's to give exposition to the fact that he's from a large family. That's all any of the Akagis say about Ryan. They aren't paying any attention to him or what he's doing in the BBQ scene in the twin tapes. Ryan is the exact middle child, and I think that was chosen intentionally to drive this point home. Them overlooking him leads to a lot of his outbursts throughout the season (quotes may not be exact because im not going back to look) -- "Our parents are probably wondering where we are. Or, at least... yours are." (the old west car), "Why doesn't anyone care about how I feel?" (the art gallery car), "At least your parents actually care about you!" (the mega maze car), and "No one cares about me unless I'm doing... something." (honestly cannot remember which episode and I'm too lazy to look it up). Ryan's parents' absence from book four is purposeful -- their lack of presence says just as much about Ryan as Min-gi's parents presence says about Min-gi.
Ryan has a big personality. He's a performer. He loves dressing up in crazy outfits and he loves looking cool. I don't think these things necessarily stem from emotional neglect as a child, but they are affected by it. He craves attention and he hasn't been getting it, and that leaves him with severe issues when it comes to dealing with his feelings. All of those quotes I mentioned are him lashing out, seeking attention from Min-gi, hoping that Min-gi will notice how much he's hurting from being ignored -- but every time, Min-gi redirects back to his own family issues.
Min-gi is from the opposite situation. I don't have as much to say here because the show is much more blatant about it, but his parents give him too much attention. They hover, they tell him what to do and how to do it. He is being slowly crushed by their expectations. He wants the same things as Ryan -- to make music, to perform, albeit for... lets say artsier reasons than Ryan does. But he's been taught those things are childish. He needs to be the responsible one, and clearly he's the only one with a good head on his shoulders, considering what Ryan is like. He lashes out at Ryan constantly, especially in the early part of the season, for continually dragging him into impulsive plans.
He wants Ryan to conform to societal norms, like he does, like his own parents taught him, so that Ryan will stop getting them into messes. However, Min-gi doesn't see that Ryan's personality and mental health issues don't give him the option to conform (creds to tumblr user vexahlla for that phrasing ... her tags on this post made my brain explode). He says "I couldn't get into uni if I tried" (the mega maze car). This is a whole other rant but Ryan also displays symptoms of bipolar disorder throughout the season which indicates to me that his brain chemistry would not physically allow him to slow down and follow a "typical" life path without genuine help (not the needling Min-gi was doing in the astro queue car). I think these problems that the show alludes to would have been alleviated a lot more if he'd had more help from his parents, but again, he's dealt with emotional neglect since he was tiny.
So Ryan and Min-gi end up as an unstoppable force and an unmovable object (which... now that i think about it... is a pretty accurate description of them as people, too). They both want to play music, but Ryan needs it immediately, because he needs the attention that he's not getting at home. He wants to get away, and fast. However he doesn’t realize that getting away without Min-gi is pointless, because Min-gi is who he actually wants attention from anyway. On the other hand, Min-gi can't leave immediately, especially when he thinks there's a particular life path he needs to follow. Both desperately want the other in their life, which keeps driving them back together, but they butt heads because their upbringings are so opposite.
This issue doesn't exactly get resolved in book four, but it doesn't need to, either. Book four ends with Ryan and Min-gi apologizing, and agreeing to stop sweeping things under the rug, actually try to look at each other fully, and see where the other person is coming from. So it's definitely a start to mending the gap between them and i think that's enough.
#rymin#infinity train#keeperofthebox talks#Theres so much more i want to say but its not really directly related to this point and i wouldnt know how to phrase it anyway#ryan akagi#min gi park#Im going to go listen to me and michael by mgmt and cry now
169 notes
·
View notes
Text
10 Common Symptoms of a Mental Breakdown
10 Common Symptoms of a Mental Breakdown
Introduction
Feeling overwhelmed or having a tough time coping? You’re not alone. Many of us go through periods where it feels like the world is crashing down around us. This state often signals a mental breakdown, a term that describes a period of intense mental distress. During this time, managing day-to-day tasks can feel impossible. By understanding…

View On WordPress
#"Adult ADHD symptoms"#"Agoraphobia symptoms"#"Anxiety disorder signs".#"Anxiety symptoms"#"Bipolar disorder symptoms"#"Burnout symptoms"#"Depression symptoms"#"Emotional breakdown symptoms"#"Mental breakdown recovery"#"Mental breakdown symptoms"#"Mental health disorders symptoms"#"OCD symptoms"#"Panic attack symptoms"#"Post traumatic stress disorder symptoms"#"Psychological distress symptoms"#"PTSD triggers and symptoms"#"Schizophrenia symptoms"#"Signs of a nervous breakdown"#"Signs of mental illness"#"Stress symptoms"#"Types of mental disorders and their symptoms"#Anxiety#Depression#EmotionalHealth#MentalBreakdown#StressRelief#Symptoms
0 notes
Note
i disagree with a lot of your views on mental health just given my own research and knowledge of mental illness and the dsm-5.
i think the inherent issue with it is the categorization. organizing things by how they present behaviorally feels very unscientific. we need to do a lot more research to lean into like a sort of biological taxonomy. one big example is that schizophrenia and bipolar disorders have a LOT of overlap in brain areas, and while they are not identical areas, treating bipolar as something closer to anxiety and depression seems like a poor way to treat it, especially if you're looking from biological and medical perspectives.
i'm not as familiar on ptsd and personality disorders, but there's a lot of overlap there, and considering my own experience "developing a cluster b personality disorder" from trauma (i say this in quotations because i do not actually like the diagnostic system and would rather remain undiagnosed), i wouldn't be surprised if there was neural overlap in like, activity, connectivity. There's probably other stuff too we haven't really looked into. I feel like there's so much more we can do to look into the neurology of mental illness than we're doing as is. Focusing on symptoms too much, and even neurology wise plasticity can be a problem. Did you know bullying can change the way your brain works?! (Reductive way of saying it, but there's a bit of research on bullying +plasticity, also i'm off track.)
i also feel as though the clinical/general applied psych community could do a lot more pulling from basic research. we only get the moolah if we work through their lens (i'm a cognitive neuroscientist), so like. i wish therapists and psychiatrists would look a little more into our readings sometimes...
i've been doing a lot more reading on dimensional models, and i kind of like what it's putting down. part of me worries that having neurological profiles of mental illnesses might end up sort of labelling neurotypical people in the same sort of essentialist way a lot of diagnostic labels do with mentally ill people (reason i would like to remain undiagnosed). But I think the idea of quote unquote "neurotypicals" with tendencies (something discussed both in literature and in clinical settings where mental illness is defined as symptoms + distress) and similar brain patterns to those with adhd, autism, ocd, depression, psychosis etc sort of forming community with those who have those disorders proper. i think we could learn a lot from one another! coping mechanisms, how to deal with big stressors, learning what sets us off in situations with better coordination and less yappy narcs than group therapy. perhaps it's idealist, but i'm a bit of a dreamer.
i hope you read this and consider my point of view, even if it did meander a bit XD
It took me awhile to be able to sit and take this in, and even still I'm having a hard time comprehending chunks of it so if my response ends up misinterpreting anything feel free to send another anon to clarify.
I do agree that we're still not at a perfect stage of "all of these things are 100% properly understood", and by no means do I feel psychiatry has managed to hit a perfect stride when it comes to diagnostics either. Things can and do still get misdiagnosed for various reasons, and there's definitely disorders that get seen as "similar" because of behavior that brain-structure wise may be worlds apart.
I also agree that in concept, having spaces that allow currently undiagnosed/traits of/self-suspected people, or those who just have a few similar symptoms that find themselves relating to, is certainly not a horrible idea. Having peer-to-peer support spaces shouldn't necessarily depend on whether or not a doctor has given you the "stamp of approval," and in some cases I've even seen well-vetted, non-specific spaces that foster this in a very positive manner.
But in the spaces dedicated for a specific disorder, the language used in them is.... not that. It isn't someone who suspects they have it asking for advice on how to see a doctor, or another saying "I relate to x symptom, what do the people here with y disorder find helpful for mitigating this?"
It's often rife with people who, whether due to comorbid disorders, malingering, or active faking, are spreading vast and wild misinformation that causes harm to both those already diagnosed (possible to adapt false behaviors and receive improper care if doctors assume misdiagnosis), and those actively seeking one (may exaggerate/lie about symptoms or use key words found online that lead a doctor to assume malingering, even during real cases).
There's so many takes that disregard the medical misinfo to fixate on validating "all" experiences, regardless of when those experiences indicate a different disorder. And if that gets called out, then you're fakeclaiming every single person there somehow. And if the space is actively pro-self dx, then they're often prone to telling people that no psychiatrist should be trusted (ESPECIALLY if they tell you your self dx is wrong) and that a diagnosis doesn't matter anyway because it's all some grand conspiracy to further oppress you.
And outside of that, even when someone has similarities, traits, or specific relatable symptoms, there's times where those of us experiencing a specific disorder want to feel a sense of community with those who have the same type of experience, and not just someone who understands "by proxy" or as an outsider.
I have plenty of people who don't have a dissociative disorder in my life who can relate to certain symptoms I have, or can understand in a sympathetic manner when I talk about my experiences and frustrations. But I don't know anyone else with DID, let alone that I know is being honest about it. I don't have a sense of community or belonging-- I feel isolated. And the internet hasn't made me feel more of a sense of community in having DID, but instead it's managed to make me feel more shut-out due to how wide-spread the horribly reductive rhetoric around it is.
I don't have this in regards to having autism or adhd. Hell, I'm even less strict about my views around posts and self-recognition of those because 1. they're often found due to social irregularities that a person experiencing them may be able to pick up on, and 2. people are much more receptive to when misinformation, infantilization and ableism in regards to them is called out.
This has turned into a bit of my own meandering but basically, a lot of my frustration at the moment is stemming from the internet's treatment of DID (and dissociation in general), and there's definitely things I've said about disorders in general that I think there are exceptions to, but it can be hard for me to sit down and think about/talk about those things while I'm wrapped up in my frustrations about this thing specifically.
4 notes
·
View notes
Text
PMDD (Post Menstrual Dysphoric Disorder)
[CW menstruation, mental health. Quoted source altered to be trans-friendly] [artist imagery created in response to artist’s own experiences dealing with PMDD]
Premenstrual dysphoric disorder (PMDD) is a health problem that is similar to premenstrual syndrome (PMS) but is more serious. PMDD causes severe irritability, depression, or anxiety in the week or two before your period starts.
Symptoms of PMDD include: Lasting irritability/anger. Feelings of: despair, suic*de, or anxiety. Panic attacks. Mood swings. Lack of interest in daily activities & relationships. Trouble thinking/focusing. Tiredness/low energy. Food cravings/binge eating. Trouble sleeping.

Researchers do not know for sure what causes PMDD or PMS. Hormonal changes throughout the menstrual cycle may play a role. A brain chemical called serotonin may also play a role in PMDD. Serotonin levels change throughout the menstrual cycle.
PMDD affects up to 5% of [menstruating people] of childbearing age. Many [people] with PMDD may also have anxiety or depression.

Treatments include: SSRIs, birth control pills, stress management.

Thanks for reading. ♥ I never see anyone mention this, I thought I'd say something.
Personal notes: I have found the supplement "Jubilance" (oxaloacetate) to be a huge help. Not a total fix, but a great relief. And therapy helps me a lot, too! Track your cycles, too!!
Source: https://womenshealth.gov/menstrual-cycle/premenstrual-syndrome/premenstrual-dysphoric-disorder-pmdd
#PMDD#post menstrual dysphoric disorder#mental health#reproductive health#art#artist#mcromwell#marandart#expressive art#menstruation#menstrating#tw periods#tw menstruation#long post
76 notes
·
View notes
Text
Going Deeper Into Imitated DID
Imitated DID is a hypothetical condition where patients supposedly experience symptoms of DID due to iatrogenesis or social contagion.
Now, as a tulpa, I of course am certain that it's possible that believing you have alters when you don't and repeatedly interacting with them could make somebody plural. So I wouldn't normally say the possibility is completely baseless. But many of these cases they're talking about are cases of people with actual histories of childhood trauma and symptoms of DID that go far beyond simply having headmates.
There are significant flaws in this "research" that need to be called out.

Right from the start, this headline hints at the real purpose of this paper. It's about protecting therapists from lawsuits over false diagnoses.
Right from the start, the paper makes it clear that their hypothetical Imitated DID isn't recognized by the DSM. The DSM acknowledges intentional factitious disorders where symptoms are forcefully manifested, and malingering.
Imitated DID, where symptoms are unconscious, is a condition made up by these authors.
So what are signs of Imitated DID?
Well...

If you pay attention, you'll notice some of these are redundant.
Highly dramatic presentation/exaggeration
pseudologia fantastica (also known as pathological lying)/persistent lying
lack of consistent work history
"la belle indifference" (a lack of distress)
selective amnesia
There are some pretty big flaws in this.
As acknowledged in the earlier quote, there are many cases of DID with "flamboyant" presentations.
A lack of consistent work history shouldn't be an indicator of a disorder being fake in people with severe mental illnesses.
DID often compartmentalizes stress, meaning the current fronter may not be distressed at the moment while other alters are.
And telling clinicians, essentially, to suspect patients may be faking because they're seeking hospitalization seems like an EXTREMELY dangerous practice.

Basically, the biggest sign that DID is imitated, according to them, is that patients are ashamed of having DID. I think The Plural Association's article did a good job at breaking down the flaws with this mentality better than I can so let me just link to that:
The use of shame as a criterion for diagnosing a mental health disorder is deeply problematic and raises significant ethical and practical concerns. At its core, this approach implies that people with genuine DID must internalize negative societal attitudes – such as pluralphobia or ableism – in order to be recognized and validated by the mental health system. This not only perpetuates harmful stereotypes and stigmas but also places an undue burden on people who are already grappling with complex mental health challenges.
Shame is a deeply personal and subjective emotion that can be influenced by a myriad of factors, including cultural norms, personal beliefs, and past experiences. It can also vary between Headmates. To use it as a diagnostic criterion risks pathologizing normal emotional responses and invalidating the diverse experiences of people with mental health conditions. Moreover, it can discourage people from seeking help, as they may fear being judged or misunderstood based on their emotional responses.
Instead of relying on shame as a diagnostic criterion, mental health professionals should strive to create an environment that fosters understanding, acceptance, and validation. This involves recognizing and challenging societal prejudices, such as pluralphobia and ableism, and advocating for a more inclusive and compassionate approach to mental health care. It’s crucial to remember that mental health disorders are not a sign of personal failure or weakness, but rather, they are complex conditions that require empathy, understanding, and appropriate care. And as Brene Brown explains, in order to empathize with someone, you must be willing to believe them as they see it, and not how you imagine their experience to be.
The only thing I'll add is that being less ashamed is a natural response to feeling less alone. As plurals continue to gather and support each other, there will be less shame for symptoms of switching and voice hearing.
People in the LGBT community are much more confident coming out today than they were 50 years ago as stigma has been fought back. Likewise, people who have talked to other systems and heard their stories will feel less ashamed than someone who is completely isolated.

Quick reminder: While people may not like the idea of having DID as a whole, not all symptoms are viewed as bad. For example, in a comparison with Schizophrenic voice hearers, it was found 69% of DID systems said they would miss their voices if they were gone.
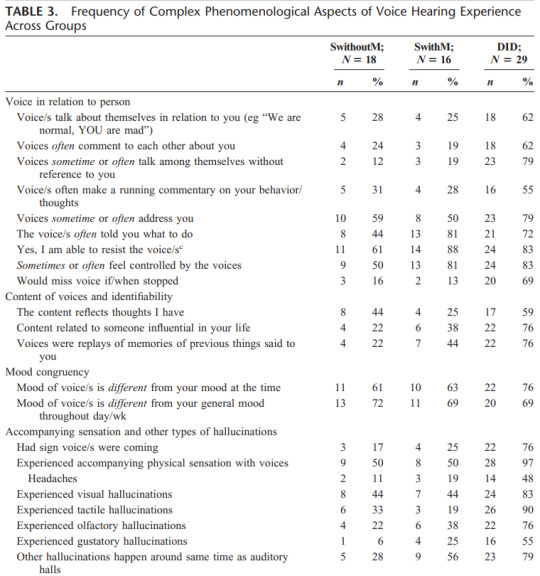
Presenting a black and white narrative that paints any systems with a positive outlook towards aspects of their diagnosis is not only problematic, but actively contradicts the science.
Back to that one flamboyant presentation of DID though...
That number seems shockingly low and should be an immediate red flag. Only 1 of their group of 71 they judged to have "genuine DID" showed overt symptoms???
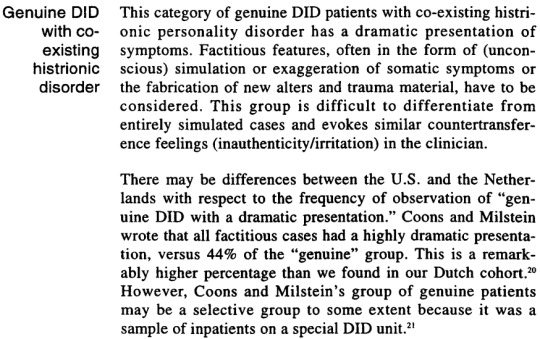
Or... this is a matter of biases of individual clinicians, and what one considers to be dramatic presentations may not be what another considers to be dramatic presentations?
It seems almost dishonest how they ignore the existence of this sort of bias while looking for environmental factors.
But that would mean admitting that the "imitative DID" hypothesis is based on the subjective opinions of clinicians that's being treated as fact.
Correct me if I'm wrong, but hysteria was already outdated as a term and considered offensive and sexist by the late 90s, right?
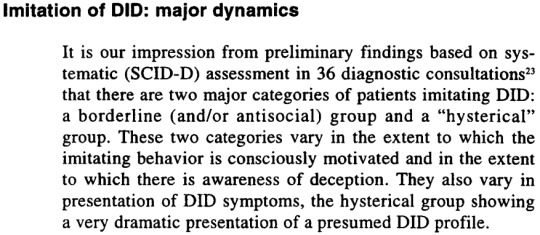
Alright... let's get into the Borderline patients.

There are even more issues here. Take this, for instance:
Some of them are involved with drug or alcohol abuse.
How many? How does it compare to the "genuine DID" group? Some is a weasel word with no significance that could lead to patients being ignored just because they use drugs or alcohol.
As most people know, self-medicating with drugs and alcohol is common in trauma survivors.
And I want to point out that BPD has a high comorbidity with DID. So how do they go about differentiating BPD imitating DID from "genuine DID" with comorbid DID?
And finally... the part about the child alters... just really sounds made up. There are not a bunch of people out there using child alters as some sort of metaphor for a lost childhood.
If you're wondering... the article gives no further details on how to differentiate these internal representations from "genuine child alters." It's just a mystical skill you gain from experience, I guess?

If you read this and are remembering how one of the common features in imitated DID was supposed to be exaggerated and dramatic presentations, congratulations on paying attention and applying your critical thinking skills! 🏅
Is it expected that people need to dissociate during the interview to have their symptoms believed?
Anyway, this goes back to the selective amnesia claim from the beginning. One huge problem I have with this is that if you had a small system with one overzealous protector or a persecutor, it would make sense to switch and have amnesia for those moments specifically. Those alters are likely the ones with poorest communication and strongest dissociative barriers.
The first case study for this presentation is a woman they call Sandra. The paper details how she had a history of trauma, prostitution and drug use. It goes on to say her main support came from a "much older boyfriend."


The whole thing comes off as weirdly sexist, stopping just short of calling her a slut and gold digger. It culminates in this line.

And at this point, I'm absolutely livid.
The clinicians looked at her history, and decided that the DID was likely imitated BEFORE THEY EVEN OBSERVED HER.
I cannot stress how problematic this is for their study when they're admitting to this sort of bias from the moment a patient checks in.

I wonder if her case would have still been deemed groundless if this had been published first, and it was known the clinicians were biased against her from the beginning.
To me, this reads as if a group of doctors were seeking to prove a hypothesis of "imitated DID." They need to find patients who they can use as examples. Then this woman comes in with a lifestyle they dislike. They immediately judge her on her history, and are then able to "confirm" their impressions of her after observing her.
It feels incredibly slimy and unethical.




And I of course have more concerns with this.
Voice hearing is a very common experience among DID systems from a young age, as are abuser introjects. And imaginary friends lasting until adulthood is generally uncommon in singlets.
Were these imaginary friends and voices always there or did she invent them after hearing about DID? If they were always present, that should be researched more carefully.
When they say she "attributed" her negative behavior to the angry imaginary friend, are they meaning the voice is telling her what to do and she obeyed, or does she actually feel like she becomes that person as is indicative of a switch? It's never explained, but I assume it's the latter. And it's concering that OSDD (DDNOS at the time) wasn't presented as a possible explanation for the perceived lack of amnesia.
Even if the voices weren't fronting, this might be enough for a Partial DID diagnosis today.
And her amnesia "feeling like denial" is, again, the opinion of one clinician or group of clinicians treating her. If another group of clinicians observed her, would they have drawn the same conclusions?
This is a woman who had childhood trauma. She seemingly had multiple "personality states." She heard voices as is common in 90% of DID cases. She experienced DP/DR. She reported amnesia, even if the psychiatrists dismissed it as denial.
As far as I can tell, the ONLY reason for denying the diagnosis is that it was originally suggested by a DID patient who recognized similar symptoms in Angy.
That's it!
It feels like what really led to the denial of her diagnosis was pure ego. Not wanting to admit a DID system was capable of recognizing traits of their disorder when psychiatrists had previously missed them all.
This is where I'm leaving off...
There's more to talk about in this paper. SO MUCH MORE.
But this post is long enough as it is.
I'll try to come back and take on the rest of the pseudoscientific mess later, including the part where they discuss how they want to apply this theory to protect therapists from legal damages. For now, this is where I'll leave you.
Thank you for reading.
Continue to Part 2
#syscourse#psychiatry#psychology#science#psych critical#plural#plurality#endogenic#multiplicity#systems#system#plural system#endogenic system#pro endo#pro endogenic#bpd#borderline personality disorder#system stuff#sysblr#mental health#csa tw#child abuse tw#abuse tw#sa tw#imitated did
80 notes
·
View notes
Text
Roscoe Dillon's Psychiatric Assement
I decided to do a psychological evaluation for The Top (Roscoe Dillon), and make it as accurate to a real-world evaluation as was feasible for a guy who's canonically a ghost.
I do not have a doctorate in psychology and cannot diagnose real people, but I am working on my master's in psychology and feel reasonably capable of diagnosing a fictional person who cannot be harmed by my diagnosis if I am wrong.
I tried to be as accurate as possible in my presentation of all conditions included---but feel free to correct me if I made any horrible mistakes.
TW for: Mental health problems; suicide; the Dillon family's horrible ideas about mental health
Iron Heights Penitentiary
1961 Broome Street
Central City, MO
Complete Evaluation: Adam Brooks, M.D.
Date of Exam: 7/31/2019
Time of Exam: 4:45:22 PM
Patient Name: Dillon, Roscoe Neyle
Patient Number: 111044554
History: Roscoe Dillon is a 36-year-old male prisoner of Iron Heights Penitentiary. He is currently unmarried and has no children, but he is in a long-term relationship with a woman named Lisa Snart. He was referred to me by Correctional Officer Robert Morrison after he attempted to hang himself in his cell. This attempt left him unconscious for two days, and it was only after he woke up that I was able to begin the process of evaluation.
Roscoe’s chief complaint was, quote, that “I am a failure, and therefore the tops have turned against me”, and stated that his motivation for his attempted suicide was his belief that he had failed his girlfriend, Lisa, as well as, quote, “my own lofty expectations of myself”. Roscoe also describes and displays symptoms of a mood disorder, with psychotic features, and specifically reported symptoms of depression. While he was unable to provide me with a coherent explanation of how long his symptoms have lasted, Correctional Officer Morrison reports that he has been chronically displaying symptoms since he was incarcerated in Iron Heights Penitentiary nine months ago.
Current Symptoms: Roscoe reports a depressed mood, a loss of pleasure in spinning his tops, problems with his appetite (“I did not realize until recently, but I do not think I have eaten more than a meal a day in quite some time”), difficulty in concentrating, feelings of worthlessness, and a death wish, the latter of which precipitated his attempted suicide. Correctional Officer Morrison also reports that when he is on guard duty, he sees Roscoe sleep only rarely, suggesting a level of insomnia. Roscoe himself was unable to confirm this, but did admit that he thought it was quite likely that he “had not been sleeping well of late”. He attributed this disruption in his sleep to racing, anxious thoughts. Roscoe also reports extreme agitation and a general inability to keep still, which he displayed throughout the evaluation in the form of rocking back and forth in his seat. Also throughout the evaluation, he displayed extremely pressured speech. It was often difficult to understand what he was attempting to say, and this communication barrier seemed to add to his agitation throughout.
Suicidality: Roscoe attempted suicide three days ago, and, while he has not actively attempted suicide since, he has not expressed a desire to live.
Prior Manic/Depressive Episodes: Roscoe has had four prior manic episodes and four prior depressive episodes, three of which involved an attempted suicide. During his first major manic episode, he threatened to blow up half the world with a spinning atomic grenade unless he was made king of the world.
Severity/Complexity: Based on the risk of morbidity without treatment, his personal descriptions and the descriptions of Correctional Officer Morrison of interference with his functioning, his psychotic symptoms, and his recent attempted suicide, Roscoe’s Bipolar Disorder is estimated to be severe.
Associated Signs and Symptoms: In addition to his mood symptoms, Roscoe also displays a number of symptoms of psychosis. He demonstrated mood-congruent delusions of failure, as well as a delusion of passivity, claiming that, quote, “the tops are punishing me for my failures. They are the ones who are making everything spin and spin and spin”. Besides these delusions, Roscoe also reported visual hallucinations, in the form of distorting shapes and colors and the world around him spinning in a fashion that is similar to what might be experienced by an individual with vertigo, and auditory hallucinations, in the form of his father, girlfriend, and girlfriend’s brother talking to him while he was in his cell alone. Furthermore, while Roscoe’s speech was generally organized enough to be comprehensible, he frequently made top puns, and references to rotation and spinning, that had seemingly little relevance to the topics that were being discussed. Roscoe seems to have a degree of insight into his condition, stating that, quote, “I am quite aware that I am mad”, but not to the extent that he recognizes that his delusions of failure and passivity are irrational.
Past Psychiatric History
Withdrawal History: While Roscoe reports a fondness for fine wines, he also claims that he has never experienced serious withdrawal from any substance, and there is no available evidence to contradict this assertion.
Psychiatric Hospitalization: Roscoe was briefly psychiatrically hospitalized after an attempted suicide at the age of seventeen, but was removed after only two weeks. This was done at the behest of his parents and over the protest of at least one of the nurses at the facility. He has also been hospitalized in the prison infirmary for mental health problems twice before, once as the result of a manic episode and once as the result of a depressive episode.
Outpatient Treatment: Roscoe has never received outpatient treatment.
Suicidal/Self Injuries: As previously mentioned, Roscoe has attempted suicide four times. At the age of seventeen, he deliberately overdosed on his parents’ prescription medicine, and was only saved because his mother found his body thirty minutes afterward. At the age of twenty-four, he attempted to jump off of a bridge but was stopped by an off-duty firefighter, who tackled him to the ground before he could actually carry his plans out. At the age of twenty-nine, Roscoe died of a brain hemorrhage induced by the combination of his newly-developed telekinetic powers and the Flash’s super-speed vibrations, but was able to return to life via the possession of several corpse bodies, which he modifies to resemble his own. Due to his unusual manner of existing, his fourth attempted suicide, which he carried out at the age of thirty-two, was actually a completed suicide, in the sense that he deliberately abandoned his host body in order to return to an incorporeal state, and, had he not subsequently possessed a new host body, this psychiatric assessment would never have occurred. While all of this sounds impossible, it has been repeatedly and independently verified by several doctors, police scientist Barry Allen, several other members of the police force, and a coroner, so I am forced to accept the story as true. His most recent suicide attempt occurred two days ago; he attempted to hang himself in his cell with his bedsheets and was only saved by the quick actions of Correctional Officer Morrison. Roscoe does not appear to engage in non-suicidal self injury.
Addiction History: Roscoe vehemently denies any history of substance abuse, and, while it is clear that he drinks a number of alcoholic beverages, there is not sufficient evidence to prove that he has any substance abuse problems.
Psychotropic Medication History: Roscoe has been prescribed lithium by previous doctors, and does take it with at least some regularity when he is not in prison. Due to what I can only assume was an organizational oversight, however, he has not had access to lithium since he arrived at Iron Heights Penitentiary nine months ago (as confirmed by Correctional Officer Morrison).
Other Psychiatric History: Roscoe has been psychologically evaluated twice before whilst incarcerated. He has previously been diagnosed with Bipolar 1 Disorder, which is consistent with his current symptoms, as well as with Autism Spectrum Disorder. These previous psychological evaluations indicate that, when he is not in the midst of a mood episode, Roscoe struggles with social communication and interaction, and evidently has since he was a child. Although he doesn’t seem to understand why, he is aware that he has never had many friends, and he reports, quote, that “I did not like school. The children there made fun of my tops.” He also engages in stereotypies (rocking, hand waving, and especially spinning), particularly when distressed, and has an intense, nearly all-consuming interest in tops. He can monologue about tops for hours on end, and will do so if you allow it. Roscoe is also averse to loud noises and adheres to a variety of strict eating, washing, and dressing routines. In spite of all this, Roscoe insistently denies that he is on the autism spectrum, and will angrily insist that he is, quote, “neither a freak nor retarded” when the topic is brought up around him.
While his severe mood episode likely obscured most of his autistic symptoms, I did notice his rocking in his chair, and I likewise noted that his speech, although rapid and pressured, was also quite stiff (bordering on monotonic) and formal. He insisted on referring to me as “Dr. Adam Brooks” throughout the evaluation. He also only made eye contact once during the evaluation, and the contact he did make was sustained and intense enough that it was clearly not a natural behavior for him. His apparent fascination with tops might also explain the persistent top puns that littered his speech, as well as why he specifically believes that tops, rather than any other object, are punishing him.
Social/Developmental History
Roscoe Dillon is a single, 36-year-old man. He is American, and, although he was born in New York City, he and his family moved to the suburbs of Central City when he was eight years old, and he has lived in the Central/Keystone area ever since. He has a long history of criminal activity. He has been arrested more than four dozen times, most commonly for grand theft and armed robbery, and has been incarcerated on six separate occasions, although he has served out only one complete sentence. He is notorious for escaping from prison, and his repeated deaths also have put an early end to some of his sentences. Currently, he is serving a ten-year sentence for armed robbery, with possibility of parole, but the chances are extremely high that he will escape from prison well before the end of his sentence. I only hope that he doesn’t do so through suicide.
Relationship/Marriage: Roscoe is in a long-term relationship with Lisa Snart. She was once an Olympic-level figure skater who performed for the Futura Ice Company, but became involved in a life of crime shortly after Roscoe’s first death. She is currently incarcerated in the women’s wing of Iron Heights Penitentiary. In spite of this, the two appear to have a mostly functional and healthy romantic relationship. That being said, Roscoe’s intense level of attachment to Lisa is worrying; his primary motivation for attempting suicide was the belief that she would be happier if he was dead, and he also noted that if anything ever happened to her, he would probably kill himself.
Children: Roscoe has no children.
Barriers to Treatment
Emotional: While I have not personally evaluated Roscoe before, other prison psychiatrists who have worked with him state that he is violently opposed to the idea that he might be mentally ill or in need of treatment. This appears to stem from a belief that admitting to mental illness would be tantamount to admitting to being incompetent or a failure. He has also stated that he only takes lithium because Lisa, his girlfriend, asks that he do so. His current psychotic symptoms, which limit his insight, are another potential barrier to treatment, but these will be addressed via the treatment plan.
Environmental: Warden Gregory Wolfe strictly limits the number of patients who are permitted to attend therapy sessions with me. Getting Roscoe approved for therapy will likely prove very difficult.
Family History
Roscoe’s maternal great-uncle, Rufus Neyle, was repeatedly hospitalized for Bipolar 1 disorder. Previous evaluations of Roscoe strongly suggest that the Dillon and Neyle families viewed this as shameful and did everything they could to cover it up.
Roscoe’s maternal aunt, Rachel Dylan (neé Neyle), received outpatient treatment for major depressive disorder. Previous evaluations of Roscoe indicate that Roscoe’s father described his aunt as, quote, “weak” for seeking treatment for her condition.
Roscoe’s first cousin, Ralph Dylan, is known to have been diagnosed with autism spectrum disorder. Previous evaluations of Roscoe strongly suggest that his parents viewed this as an embarrassment; Roscoe evidently claimed that his father once referred to this cousin as, quote, “a retarded freak”; this likely contributes to Roscoe’s vehement denial that he is himself on the autism spectrum.
Roscoe’s paternal grandfather, Roland Dillon, is suspected to have had major depressive disorder. He is also known to have committed suicide at the age of 52. Previous evaluations of Roscoe indicate that his father, Reginald Dillon, perceived this as having brought shame on the family name.
Roscoe’s mother, Rosa Dillon (neé Neyle), is suspected to have anxiety and a potential alcohol abuse disorder. Previous evaluations of Roscoe suggest that she often seemed quite anxious and agitated, and he has stated that she often drank wine to, quote, “calm her nerves”. Roscoe has also claimed that his father did not know of this, or at least refused to admit that he did.
Family psychiatric history is otherwise negative. There is no other history of psychiatric disorders, psychiatric treatment or hospitalization, suicidal behaviors or substance abuse in closely related family members.
Medical History
Adverse Drug Reactions: None known.
Allergies: None known.
Compliance: Roscoe is notorious for non-compliance with medical instructions. While he does take lithium fairly regularly, at his girlfriend’s bequest, he never attends outpatient therapy when not incarcerated, and attempts to avoid therapy while incarcerated as much as he can, even to the point of getting himself sent to solitary confinement rather than having to attend therapy sessions. He seems to despise psychologists and psychiatrists on principle, and is known to make attacks on their professional competency when he disagrees with their assessment of his mental state (which is quite often). As a result, his mental health problems generally go mostly untreated.
Some of this hostility likely stems from the fact that Roscoe’s first psychological evaluation whilst incarcerated came at the hands of Jonathan Crane, a psychologist who was later stripped of his medical license for experimenting on his patients with an unregulated drug of his own invention. This drug, which the newspapers dubbed “Fear Toxin”, was a blend of synthetic cortisol, epinephrine, norepinephrine, indolealkylamines, phenylethylamines, arylcyclohexylamines, serotonin inhibitors, and dopamine enhancers, and was used to induce fear-based hallucinations in its victims. While it cannot be conclusively proven, the evidence seems to suggest that Roscoe was subjected to this drug as a part of the “evaluation” given to him by Crane, and if this assumption is correct, I fear that Roscoe cannot be entirely blamed for his distrust of the psychiatric profession.
Exam: Roscoe Dillon is six feet tall, and, when healthy, weighs around 175 to 180 pounds. When I evaluated him, however, he was badly underweight, weighing only about 147 pounds. His hair and clothes were noticeably disheveled, he had dark circles under his eyes. His body language and his facial features displayed obvious distress and depression. He seemed agitated throughout the evaluation and repeatedly rocked back and forth in his chair. He almost never made eye contact. He exhibited speech that was rapid and pressured—almost to the point of incomprehensibility at times—but which was otherwise properly articulated and generally coherent. His affect was congruent with his mood, and his conversation revealed clear evidence of delusions of failure and passivity, as well as of visual and auditory hallucinations. Except when discussing his specific delusions and hallucinations, his associations were intact, his thinking was logical, and his thought content appeared appropriate. Roscoe’s suicidal intentions were undeniable, given the bruises that were still around his neck from his attempt to hang himself, but he no longer appeared to be actively suicidal. He also denied any specific homicidal ideas or intentions. Roscoe’s cognitive functioning, vocabulary, and fund of knowledge are intact and age-appropriate, and his short-term and long-term memory and ability to abstract are likewise intact. His ability to do arithmetic calculations is not only intact but is bordering on the genius range, which is consistent with his general talent for engineering and inventing. Roscoe is oriented to person, place, time, and situation. Judgment is fair, but is compromised by his psychotic symptoms. Roscoe’s insight into his problems is not completely absent, but is severely limited by his mood episode and psychotic symptoms. There are also signs of autism spectrum disorder, but at present these are largely overwhelmed by his mood and psychotic symptoms.
Diagnoses
F31.5 [296.54] Bipolar 1 Disorder, currently depressive, severe with mood-congruent and mood-incongruent psychotic features.
F84.0 [299.0] Autism Spectrum Disorder, requiring support.
Instructions/Recommendations:
The patient should be confined to the infirmary until further notice, because the patient was very recently actively suicidal, and is still in the midst of a severe depressive episode with psychotic features. I will conduct therapy within the infirmary.
Once the patient has recovered to the point that he is no longer clearly psychotic or a suicide risk, I strongly recommend weekly therapy sessions, even if this is unlikely to take place due to Roscoe’s notorious tendency to avoid therapy at any cost.
Start 600 mg of Lithium, 2 to 3 times/day. Roscoe has Bipolar 1 disorder and a history of suicide attempts; he should have been on lithium from the second he came through the penitentiary doors. I don’t know what oversight caused this, but this problem needs to be resolved now.
Start 3 mg of Risperidone, once a day. This is for the psychotic symptoms.
Notes and Risk Factors:
Global Assessment of Functioning: 12
Risk Factors:
Z62.881 [V15.42] Psychological Abuse in Childhood
While never confirmed, almost every mention of his parents Roscoe has made indicates that his father was demanding, perfectionistic, critical, and verbally abusive when Roscoe did not live up to his expectations.
Z65.1 [V62.5] Imprisonment or Other Incarceration
Serving ten-year sentence for armed robbery (with possibility of parole) in Iron Heights Penitentiary
Z72.881 [V71.01] Adult Antisocial Behavior
1. Roscoe is a career criminal. While he sometimes commits crimes alone, he more often works alongside his girlfriend, Lisa, or in tandem with an organized group of costumed criminals known as “the Rogues”.
Electronically Signed
Adam Brooks, M.D.
On: 7/31/2019, 9:45:24 PM
#flash rogues#flash comics#roscoe dillon#the top#iron heights penitentiary#golden glider#fanfic#tw suicide#tw characters who don't understand mental illness#tw mental illness
6 notes
·
View notes
Last Seen Blogs

the-grimreaper
The_Grim_Reaper

kinnyuwu
♡𝓚𝓲𝓷𝓷𝔂♡

crocheting-cub
Untitled

1of1team
1team, 2team, Red Team, Blue Team

kinky-mommy-75
Kinky Mommy