#ToSD
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Average visit duration of Tumblr.com is 10 mins and 25 secs.
Text
This is a constant problem. I’m tired of people badmouthing the ToSD as some form of syscourse power move.
1. The ToSD has nothing to do with endogenic systems. Stop using it to either support or deny their existence.
2. The ToSD is well researched and well supported. Stop trying to say it’s underresearched.
3. “The ToSD is just a theory!!!” Please research what scientific theories entail. I am also trying to do the same, as I definitely don’t know enough. But I know it’s different from fucking gravity.
4. “I know people who don’t fit the ToSD!” Did you know I don’t have any parts who feel like ANPs? I guess I don’t fit the ToSD either woaaah. Except I do because the ToSD is not about how an individual labels or perceives themselves, it’s about the literal fucking presentations of dissociative disorders.
Sigh.
32 notes
·
View notes
Text


Undertale Community Project 2024
My art for @arerona 's Undertale Community Prodject other on DeviantArt.
I'm really not involved in the Undertale community any more, but I've done this every year since 2018, so no point in stopping now :P
Given I re-worked Tales Of Stardust to be an original for my school work last semester, it definitely made this a lot harder than I expected. As you'll see, I reverted some of the designs back to their pre-2020s vs, to make a stronger visual difference between the two iterations of the story. Story wise, I went with the re-written version ( I really do love it so much more!), which is why older viewers will notice a significant difference in their meeting.
Anyway,
I got a little carried away with these two pieces, I intended for them to be a lot simpler than this, since I'm very short on time (drowning in school work again, rip me), but I am very happy with the end product even with the extra time needed to make these beauties, especially the bottom one :)
Speedpaint below ⬇️
----
- - -
[Commissions] [Instagram] [Cara]
#undertale#fanart#digital art#digital painting#sans#tales of stardust#undertale au#undertale community project#tosd#artists on tumblr#my art#speedpaint
5 notes
·
View notes
Text
Selves and Self-States
Please, have a rambling explanation of how we view and define dissociation within plurality, multiplicity, and CDDs. We’d love to hear from you, and we have links to free sources for any who ask (as we don’t want them taken down).
Structural Dissociation
Under the theory of structural dissociation (TOSD), the emotional parts (EPs) are initially unintegrated due to overwhelm, but remain separate as a result of the phobia of the apparently normal parts (ANPs) who live daily life. This phobia can manifest as denial of the EPs’ existence, refusal to communicate with EPs, and inability to accept the EPs’ experience as belonging to the ANP (the condition to integration).
Both in complex dissociative disorders (CDDs) and other traumagenic structural dissociation (SD), the publication of the TOSD (the Haunted Self) defines some EPs as elaborated; the EPs are the traumatized selves. I have trouble with this because of the required multiple ANPs to qualify tertiary SD.
If a self (as opposed to a self-state) can be an EP, some systems would qualify as having only one ANP, or possibly none at all. However, if a self is an ANP, each could have any number of associated EPs, or self-states.
Self-States
I like self-states because everybody has them, and it fills in some of the gaps left by the TOSD. Self-states aren’t inherently stuck in trauma, but a trauma-holding self-state would fit the phobia associated with traumagenic unintegration. It also leaves room for those who share self-states between selves, and for those whose selves contain multiple self-states without barriers between their states.
Elaboration occurs as self-states are collected within the boundaries of a self. Self-states are built out of experience, from tiny fragments of sensation or emotion to a developed set of reactions and behaviors to stimuli. It is one self-state when experiences are accepted in, like a mosaic. Some self-states have self-states, contained like marbles in a bowl. Some self-states are small, but uncontained, marbles rolling about all on their own.
Selves
Selves are differentiated from self-states by their sense of ‘me’ as opposed to the ‘not-me’ of the other selves. Some self-states develop a sense of ‘me’ with ease, and this is especially true in those whose boundaries were laid before the self-states of the body obtained a singular, collective sense of ‘me’ (which occurs around the time a body reaches double digits of age).
The Haunted Self notes traumagenic SD occurs more easily in children, but does not give the age of every patient used as an example. Several of the EP self-states are elaborated, and some have their own selves. The ambiguity is in how old the bodies were when these selves formed, and an EP with a self formed after 12 would be synonymous to a CDD formed after the cut-off age.
This is part of why we believe non-traumagenic plurality is possible, but there is another; if a self-state is unintegrated (and non-traumagenic dissociation is scientifically recognized), elaboration can be achieved by adding experiences. Having a self to stick to encourages elaboration, and self-states can get that by introspecting.
New Selves
Self-states that coalesce (or otherwise don’t integrate into other selves) before forming a sense of ‘me’ might explain how some selves are elaborated as soon as they appear. Self-states that never form a self might remain as marbles rolling around free, for any self to bring into its boundaries while out in the body or to front alone for specific scenarios.
Selves always have dissociative boundaries; by definition, dissociation is non-association, unintegration (which is how systems who work on lowering barriers can go between having boundaries and not, they’re integrating).
Amnesia
I would say memory barriers between selves who were at front and selves who weren’t differs from amnesia; they didn’t forget, they just weren’t there. The selves that weren’t there might have left because the brain was expecting trauma, or because their front can only hold one self at a time. Keeping these memories separate involves keeping them within the boundaries of a self, and those memories are smaller self-states like the marbles in the bowl. Amnesia as a self losing memories they once had is more like removing those self-states from the boundaries of that self.
Not all selves have memory barriers between them, or amnesia for memories they had. A body can have either function, both, neither, or a mix between different selves.
An Invitation
Our system functions very visibly within these parameters, and we can scale up or down to any feature we have. One day, I’d like to write a more professional introduction of our theory, but for now I’ll settle for introducing the language.
I’d like to know how this does or doesn’t fit you, because the goal is to find words that work for every version of unintegration. If you have something to say, any format (reblogs, comments, direct messages, posts, anything) is appreciated.
#osddid#did osdd#cdd system#adaptive system#traumagenic system#polyfragmented system#pluralgang#plurality#tosd
7 notes
·
View notes
Text
|| The "Emotional" Part of the Personality ||
Summary: an EP is a part that encapsulates the complex mental systems involving traumatic experiences & memories, and is disconnected & disoriented from the life they live in the present.
EPs are the "threat response" & "autonoetic traumatic memory" activation systems of the mind. These systems include: fight, flight, freeze, fawn, pain-experiencing & pain-numbing, re-experiencing traumatic memories, being disoriented to the present, and "owning" memories.\...\- In primary structural dissociation, one EP includes all of these systems & subsystems. In secondary & tertiary structural dissociation, these systems are divided between multiple EPs, and different EPs can exhibit the same threat responses in different situations. Additionally, threat response systems are frequently activated in succession (eg. freeze to fawn to flight), and will often result in multiple EPs being active at the same time, with one "experiencing" EP, and one or more "observing" EPs.
Example: "freeze" EP is experiencing & personifying a traumatic situation, while "flight" EP and "fawn" EP are observing it.
The latter two are not personifying the experience, because "freeze" EP is not behaving the way "flight" EP and "fawn" EP would or want to. In this situation, all three EPs are active, because all three responses may be needed for the traumatic situation. Each EP is, essentially, "waiting their turn" to be active so that they can protect themselves through their threat response activation system.
When these parts are more autonomous & elaborated, it can cause conflict if multiple EPs are active at one time. One EP may be critical of another, and might take drastic measures, such as self-harm, to activate a different threat response system, and thus, a different EP.\...\- With regards to re-experiencing traumatic memories, EPs may remember only metaphorical representations of the trauma, a complete recall of the event, fragments of a single event, or similar aspects of multiple traumas recalled as only one memory or event.
Because the EP's memories are subjective reproductions of an event, and not an exact replica, different EPs may have vastly different perceptions & responses to the same traumatic situation. Two EPs may even have completely separate memories regarding a single event. Furthermore, the activation of traumatic memories will often obstruct access to other memories available to the ANP, resulting in the EP being unable to recall episodic, semantic, or even procedural memories. This restriction can cause EPs to become stuck in a loop of re-experiencing a traumatic event, with no way to orient themselves to the present.
If the EP can be re-oriented enough to gain access to non-traumatic memories, they can grow beyond their activation systems. The more an EP is activated by trauma-related stimuli, the more benign life experience they gain. After a while, they may begin to develop a set of personal memories unrelated to their trauma. This can cause an elaborated sense of self, resulting in an "Emancipated EP." In this case, the EP is able to expand their episodic, semantic, and procedural memories past what their activation systems demand of them, allowing the EP to have their own set of wants, needs, interests, and desires.
The Emancipated EP will continue to be activated by trauma-related stimuli, however, they may be able to re-orient themselves to the present on their own, and will begin to become activated through positive stimuli that is unique to their episodic memories. Emancipation may cause conflict with other EPs, as well as phobic ANPs. The more an EP is activated in daily life by benign stimuli, the more an ANP may feel out of control, or even threatened by the presence of the Emancipated EP, who still holds traumatic memories. However, an Emancipated EP is still not fully integrated with their present reality. While they have synthesized their traumatic memories & activation systems with their benign memories and personality, they are still activated & disoriented by trauma-related stimuli.
It's important to remember that EPs are representatives of threat response activation systems & autonoetic traumatic memories. EPs are never trying to make things difficult on purpose. Rather, they are responding to innate biological systems they have no control over. EPs are also greatly affected by something called "conditional triggers," specifically with regards to their activation, but that requires an entire thread on its own. I will reply to this tweet with that thread once I have it written.
A final note: please remember that DID is complex, and alters are not only their labels. It can be hard to define whether a part is an ANP or not, and you should never force labels onto your parts against their will.
Take what feels right to you, and leave the rest.
Common EP Roles/Experiences:
- apprehension/fear part
- pain-numbing part
- pain-experiencing part
- 4Fs of survival part(s)
- attachment-seeking part
- care-seeking part
- recuperation from injury part
- "sick" or "ill" part
- "negative" sexual part
- aggressive part
Common EP Feelings:
- extreme emotions
- psychosomatic pain
- intense sensory experiences
- feeling overwhelmed
- suicidal ideation or behaviors
- pervasive sadness
- grief, loss, & mourning
- hope & longing
- feeling as if "nothing good happens"
- desire for caregiving
All of this information was taken from the Theory of Structural Dissociation, as written in the original paper from 2004.
Source:
Please excuse any typos.
I am not a professional nor an expert.
✨️Transcribed from Twitter with permission from @/ColubridC✨️
#did/osdd#dissociative identity disorder#dissociation#other specified dissociative disorder#ToSD#psychology
8 notes
·
View notes
Note
I know this probably isn't the type of question you usually get, but could you explain action tendencies in TOSD? I'm currently reading The Haunted Self and struggling to understand all the clinical language.
I suggest checking out this site! They've got some great info.
11 notes
·
View notes
Text

noisome critter of no particular renown. disliked for it's incessant yammering, and beloved for it's nuanced thoughts on horseflies, the public opinion of the critter stays perfectly neutral at all times.
0 notes
Text
Alright, I'm going to further reply to this in a reblog since I hate the format of commenting.
You are claiming that C-DID isn't real because DID is already a complex dissociative disorder/CDD. While yes, DID is a CDD, I believe that what you are claiming is feeding into a lack of nuance and potential false dichotomy. Since the 80s and the usage of MPD, modifiers such as "complex" and "polyfragmented" have been used to further specify certain systems/system structures that differ from other presentations of DID.
Although I acknowledge that he is highly controversial, it is important to acknowledge Richard Kluft as one of the pioneers of the "complex" specifier in the early 80s. Although it is highly outdated at this point, Kluft's paper on "extremely complex MPD" [link] is an important source when it comes to the history of DID terminology.
Due to the somewhat vague nature of the label "complex DID", many clinicians have moved away from the term for most purposes, and instead use the specifier "polyfragmented". However, C-DID is not a completely clinically retired term.
Here is a paper that uses both the terms "complex DID" and "polyfragmented". It's also generally a very good study and open-access.
Here is a behavioral health program that uses "polyfragmented", but describes it as "a complex sect of dissociative identity disorder".
Here is another clinic which uses "complex dissociative identity disorder".
While the term isn't as widely used in clinical settings, the specifically complex structure of some pwDID has been recognized since the use of MPD. C-DID tends to be used to refer more to the internal structure of certain systems, while the more broad term of CDD refers to disorders that fall under tertiary dissociation in the theory of structural dissociation (TOSD).
TL;DR: polyfragmended DID and complex DID mean the same thing, and they've both been used as terms in clinical settings.
(Also, I will not be making any statements on the term HC-DID.)
it's exhausting trying to argue with people who genuinely believe that RAMCOA and "variations of DID" like and HC-DID is real and don't want to accept the fact that they're feeding into a racist conspiracy theory and making it harder for actual systems to get diagnosed
#firefly flickers#long post#anti endo#psychology#theory of structural dissociation#tosd#did#complex dissociative disorder#c did#pf did#polyfrag#polyfragmented#cdd#osddid#dissociative identity disorder#system discourse#syscourse#sorta?#tagging just in case
22 notes
·
View notes
Note
Sorry if this is annoying/you have been asked this already but we have been seeing more and more posts trying to deny that Alters/headmates are separate people and that they are actually just you but separated by amnesia barriers.
it’s very confusing to us since we have OSDD 1 and view ourselves as distinctly different people just inhabiting the same body
is that wrong of us to think? (We also get confused since a lot of said posts say it’s “scientifically accurate” but we have checked the DEM multiple times and talked to our therapist and we can’t seem to find where it says that headmates can’t be separate people)
I actually haven't been asked this in a long time.
First off, the "amnesia barriers" thing is an AI talking shit about nothing in Google results. It's inaccurate, and I wish it would go away. Dissociative barriers are not only caused by amnesia, and the result of them is not always amnesia, but that's me being pissy.
Now, as for how people view themselves.
You do you, boo ❤️
Fuck the haters.
I'm going to explain this as simply as possible. This is a very general overview.
The ToSD asserts that no one is born with an integrated sense of self. During normal, uninterrupted development, childrens' action and defense systems begin to cohesively work together to create... The person you would become, I suppose. You learn to prioritize your needs and wants and create plans for yourself using a cohesive set of thoughts. For example, you're hungry but also need a shower. Your experiences have shaped you to prioritize and perform actions in certain ways. Some people will eat first, then shower, some will shower first and eat second. And these decisions are influenced by the totality of all of your experiences.
In CDDs, these action systems become separated-- dissociated away, not hidden by amnesia. If your parents were particularly cruel around food, you may have pushed those needs away, and that action system develops within itself, beginning its own prioritization process. In many cases, we lose access to those systems, and they no longer play a normal part in our decision-making.
For many, we don't have any access to those parts that we originally rejected. Some parts become alters, some parts are just fragments, but we struggle to cohesively and strategically place those needs in our day to day lives. We struggle to communicate with those parts. They have drastically different wants and needs and priorities, and access to their own unique coping skills (that may or may not be good for the system as a whole).
At any given time, we only have full, cohesive access to parts of our lives, skills, techniques, needs, thoughts, the list keeps going.
This is "parts of a whole."
This is what parts language is.
It's what I believe and it's what's helped my system.
This does not have anything to do with how autonomous or individualized alters can become, how separate, how they view themselves.
Some people relate much more heavily to this particular framework, some can understand but don't like it applied to them, some don't feel it applies at all to their system.
It's a mechanism of how CDDs develop, and within this framework, you can use whatever language you prefer. Not all parts work is parts focused. Alters can see themselves as their own people, they can wish for their own lives and dream of having their own body. Therapists can and do empathize with these feelings, and they play no part in the success or failure of treatment.
Are you all working together to stay alive and keep out of jail? Does your whole system understand they share a body?
Yes? Great, you're good to go. Use whatever language feels right.
We are parts, but we're also people within our own rights, and that's okay.
It's a huge framework. Explore it.
#not syscourse#pro syscourse conversation#sysconversation#did#osdd#osddid#cdd system#cdds#dissociative identity disorder#parts language#tosd#plural#plurality#multiplicity#system safe#endogenic safe#pro endo#syspunk is appalled
60 notes
·
View notes
Note
On the same note as your last post on the ToSD, I feel like pwCDDs who "don't apply" to the theory, feel like they don't apply because "apparently normal" and "emotional" are charged words and can be heavy to use, in a way. Like, our trauma holders are EPs in the interpretation of what an emotional part is, but they don't feel like they are emotional, so we don't use EP for them. Same with our hosts, or alters who don't remember the trauma, or alters who function better than everyone else, or in general everyone else who fit into what an ANP is but don't feel like they are apparently normal.
I don't know, it seems obvious to say this lmao but I think a lot of people with a CDD don't want to use ToSD terminology, and it's fine to use a different terminology just like parts/people language, you do you. But they also don't research what the ToSD actually says, they just assume "oh emotional part means they act like a child and have a chronic nervous breakdown going on" or "oh apparently normal part means they are so well adjusted and can't have problems ever"
^^^
Lord knows I’m at fault of this too. I need to look more into the ToSD as well. It wasn’t until within the last year that I started looking into what EP and ANP actually meant due to a friend of mine explaining that I didn’t actually need to ID with those labels.
So much of these communities are determined to make everything a label, and lord knows I’ve struggled with that too.
10 notes
·
View notes
Text
Updating blog
I'm updating my blogs, moving stuff around and getting all my story content over here + I figured if this blog is going to be my creative space blog & my main one is for general reblogging and posts, I might as well move my art over here too.
I've still got another 14 things to reblog, but those will be later so it's less of a wall of spam in one go ^^;
Enjoy the comic, that's Tales Of Stardust, my first story & comic (albeit a later iteration of it, I think that iteration is 2019 or 2020).
Later today there will be some more TOSD art coming, and my among us story An Imposter's Fate.
2 notes
·
View notes
Text
Hey, so this might just be brief, considering everything happening in our life right now. But I need something to focus on lol
DID Research has a few pages on the theory of structural dissociation, and you can find those here: https://did-research.org/origin/structural_dissociation/
Give that a look, I skimmed it because I dont have the brain energy but I know they have good stuff.
Here is another article I found. Again, I just skimmed this, but it seems to have some really helpful information. However, I think they use the word core. You can read that here: https://www.natajsawagner.com/blog/structural-dissociation-model
And finally, here is a tiktoker we really enjoy watching, going into detail about how the theory of structural dissociation works. You can view that here: https://vt.tiktok.com/ZSYRQpP7C/
We can make another post going into better detail of how we personally sort anps and eps, just dont have a lot of energy right now. And practically no communication.
Disclaimer: due to the fact we skimmed the articles, there may be information that we personally do not agree with. So please take these sources with the knowledge we aren’t in the right headspace. If needed, we can readdress this topic at a later date.
Disclaimer 2: All three links do talk about different traumas and potentially upsetting material, please be mindful and look after yourselves as you read/view.
- Blurry (they/them)
stereotypes abt systems r so funny to me bcuz.
host [me, hi] is not an anp, but instead a trauma holder of some of our most traumatic memories, with worsened symptoms of bpd and hpd. and i do actually do more than just sit around and front. because i have several roles actually. [sleep + social caretaker]
actually also, we have NO anps, the closest we have is a robot former host who is NOT normal because they STRAIGHT UP cant feel hunger or exhaustion due to us not having time to eat breakfast before going to school when it was hosting.
our main caretakers are not sweet, or soft, or cozy. one doesnt care for people and is actively intimidating to others without trying [and hes not interested in changing that idea], and the other is actively hostile towards people and is only interested in taking care of daily tasks
being social and friendly isnt a requirement but an optional thing, to the point we have social caretakers because so few of us are enjoyable to talk to or enjoy talking to people.
the Hosting situation [1 main host who is always fronting, 3 primary cohosts who are almost always in cofront, and 5 more cohosts who often get pulled to front. and we still have regular host changes every year or more.] instead of having no host, or a """""""""core""""""""" host
we have 10 introjects out of dozens of brainmade alters.
furthermore, we dont split the same fictional guy over and over! instead we have ~30 anger holders and 20+ protectors. b. because? i dont know. man too angry to associate
we DO have an evil alter and among being the only alter who we warn people abt interacting with, he has also eaten a mattress!
#actually did#did system#did#dissociative identity disorder#endos do not touch this post#osdd#actually cdd#anti endo#blurry rambles#theory of structural dissociation#tosd#educational#astrophel rambles
28 notes
·
View notes
Text
|| The "Apparently Normal" Part of the Personality ||
Summary: an ANP is a part that encapsulates survival & daily functioning, and has failed to integrate and personify traumatic memories & the activation systems related to those memories.
ANPs are the "survival" and "daily functioning" activation systems of the mind. These systems include: play, exploration of the environment, managing energy levels through rest, sleep, eating, & drinking, interpersonal cooperation, and reproduction & caretaking.
In tertiary structural dissociation, these activation systems are divided between multiple ANPs, resulting in a collection of parts - who are often disconnected from each other - that attempt to manage daily life by remaining dissociated from traumatic memories & EPs.
Some ANPs may be professionals with a strong, long-standing career. Others may be loving (yet often inattentive due to dissociation) parents. Many more may experience overwhelming dissociation & disowned feelings, making them feel like they are barely treading water.
ANPs are NOT defined by being emotionless (or only experiencing "good" emotions), "strong enough to handle it," able to excel in daily life with no problems, perfectly rational paragons, or any of the other baseless stereotypes & assumptions people make. Many ANPs may very well have those traits, but that isn't, inherently, what makes them an ANP. In many cases, ANPs may NOT be well-equipped to handle daily life, and struggle greatly with even the concept of surviving.
They are still ANPs.
When it comes to dissociation, ANPs often experience "negative" symptoms of dissociation, such as memory loss, DP/DR, feeling apathetic, and "zoning out."
ANPs often lack memories related to trauma, and are unable to feel or identify certain sensory & somatic experiences. Quite a few ANPs do have access to some traumatic memories - despite the stereotype, ANPs often don't experience full amnesia. Rather, the memories lack personification. It feels as if it happened to someone else, or they have no emotional connection to those memories.
ANPs are the people who tell a "totally funny" story about something that happened to them as a child, and are confused and upset when people tell them "... that's kinda fucked up." They know of the trauma, but they have no ability to feel NOW what they felt THEN.
For "positive" symptoms, ANPs will experience an intrusion of traumatic memories, either full or in part, and they can be emotional, somatic, or both. These symptoms can be triggered by both internal and external factors, and often, the ANP is unaware of the trigger. This will result in the ANP feeling inexplicably upset or sick/in pain, disconnecting from the experience, and, finally, being deactivated completely & replaced by the appropriate EP.
This often causes either full or partial amnesia while the EP is active.
Other than traumatic memory intrusions that result in deactivation, an ANP may experience various positive dissociative symptoms, such as:
- hearing the EP's voice internally
- an EP controlling physical movements
- feeling pain or other sensory experiences.
Due to these intrustions, ANPs often - if not always, in the case of pre-cooperation stages - are phobic of not only the traumatic memories, but of the attached EPs, as well. An ANP may try to interact with an EP, but since the EP is liable to activate traumatic responses at any moment without the ANP's awareness, the ANP cannot predict nor control these intrusions of positive symptoms.
Fearing what they can't control, the ANP fears the EP.
If there are multiple ANPs, they may become avoidant of each other, based on conflicting trauma-related issues. This can go either one or both ways, depending on the ANPs and their reasons for avoidance. Most often, conflicting ANPs will be hyper-critical of each other.
Finally, when it comes to the formation of ANPs, they often split or elaborate when an existing ANP has become too affected by recurring dissociative symptoms to function without activation of an EP. They may also form in conjunction with an EP during or after a traumatic event.
The EP holds the activation responses needed to survive the threat, and the ANP holds the responses needed to function in a life outside of the trauma the EP holds.
A final note: please remember that DID is complex, and alters are not only their labels. It can be hard to define whether a part is an ANP or not, and you should never force labels onto your parts against their will.
Take what feels right to you, and leave the rest.
[Bonus] Common ANP Roles/Experiences:
- working professional part
- parent or caregiver part
- apathetic & detached part
- connection avoidant part
- denial/self-avoidant part
- "positive" sexual part
- friends & connection part
- exploration & play part
[Bonus] Common ANP Feelings:
- emotional numbing
- feeling disconnected from life
- apathy
- inability to feel certain sensory experiences
- feeling "out of control"
- avoidant/fearful of intimacy
- desiring freedom
- feelings of denial / "nothing bad happened"
All of this information was taken from the Theory of Structural Dissociation, as written in the original paper from 2004.
Source:
Please excuse any typos.
I am not a professional nor an expert.
✨️transcribed from Twitter with permission from @/ColubridC✨️
#dissociative identity disorder#did/osdd#dissociation#ToSD#other specified dissociative disorder#psychology
7 notes
·
View notes
Note
Animals in top hats please? Sorry if it's too specific lol







99 notes
·
View notes
Note
(I've been re-watching certain episodes, and that one part in the Head Cannon finally hit different, because like- that's not the usual "inner thought" Church we see, like when he tried to get Sarge to give him money for the afterlife or went into Caboose's head, he's definitely like- THE Alpha, not "I'm just a guy who thinks he's a ghost haunting a robot body" Church. the way he talks about "I've been running this mess all by myself for years" YEAH. UH. he HAS been running this mess all by himself for years, because all the Fragments got taken away! and the way he's kinda like, tired with everything? it reminded me when Tex tried to Save Alpha without his memories. so like- Church has Alpha IN THERE, but probably doesn't notice half the time because Church's thoughts are usually screaming so loud, and Alpha doesn't even "remember" he's the Alpha. he's got double amnesia. man, Omega might've actually helped in there. he was even all excited like- :Nothing can stop us now, Church!". sorry for all that, but DANG)
ruby you don’t understand. we had the theory that “end of season 10 alpha” and “entirety of bgc church” were two separate entities long before head cannon came out. do you know how unbelievably validating it was to watch it. we literally theorized/headcanoned that alphas mindscape would be a facility in the snowy mountains. okay. obviously not exactly matching how the map looks but can you imagine the pop off.
inner “church” acted exactly like end of season 10 alpha!!! he was tired! hes been running this mess all by himself for years!! he knows it’s a mess!!! church doesn’t know it’s a mess! the mindscape versions of the characters are who they think of themselves as. and like sure you can make the argument that church really thinks of himself as a worn down and apathetic man who doesn’t want to do this shit anymore. OR we can look at the way bgc church actually acts and that he is incredibly motivated and engaged and that it would be kind of weird for him to see himself as not caring about what happens with omalley when he’s actively fighting him.
hey, isn’t it strange that church can externally feel nothing when omalley enters him even though he’s internally engaging with omalley the same way everyone else was? it’s almost seems as if his internal and external self are completely separated and unable to communicate with each other! i wonder if there’s a word for that…. maybe a dissociative disorder………. maybe one that’s known to be covert that we already know that church has but seemed to be absent for the entirety of bgc…………… wouldn’t that be wild.
#asks#rubykgrant#rvb#leonard church#alpha church#the theory was a lot less refined at that point bc we didn’t know we were plural yet#the way we write them now has a lot more nuance and understanding of dissociative and plural stuff#but still. alpha and church. yaaay#i love hiiimmmmmmmmmm#disclaimer of i think the tosd is flawed and uses incredibly dehumanizing language for systems/system members that we should move on from#BUT i think bgc church is sooooooo anp. he’s literally an anp. alpha is an ep.#look me in the mouth and tell me i’m wrong
24 notes
·
View notes
Note
Adding on since I was tagged, but I mostly followed a similar situation with @snowglobe-system but I talked about some of the things that were involved into being reasons I shifted from anti-endo to pro-endo as well here but since that's a slightly old post (at least relative to the amount of healing and thinking about the topic) I'll still give a "short" (Feathers definition of "short") run down of present observations and aspects of the change of stance in my experience.
For me, a lot of being an anti-endo came from a place of having a false understanding of what psychological research is, misunderstandings of the strength of validity of the ToSD (and also the comfort that feeling as though something was FACTUALLY known about my condition gave me as opposed to the uncomfortable truth that most things about the human condition, clinical or not, is largely unknown and speculative), a clinging to the sense of superiority and ego boost of "non-cringiness" of not being endo, a trauma centered clinging to the past bad experiences I've had with endos reinforced by some negative experiences that I saw going on, a generalized echo chamber within anti-endo social groups, and just an honest to god lack of interest or care to actually hear out experiences from the other side.
Honestly a large consistent feeling I had on the "anti-endo" side was a large amount of frustration from endos which was partially because 1) I would see them trying to derail topics about trauma that I was trying to work on into syscourse debate and it made me annoyed and 2) a lot of inappropriately projected frustration and pain that I was experiencing in early recovery towards endos under the idea that "they made this look fun and fetishized / romanticized" the disorder without really, you know, having anything other than the CONCEPT of an endo (and a certain toxic tulpa blog, same blog was one of the largest reinforcers to my anti-endo thinking tbh) in mind. Relating to the point on "lack of interest" I don't take that as a "I didn't care to consider the implications of my beliefs" but more so that I literally didn't have the mental space or energy to really consider as I spent most of my days just trying to survive and the concept of non-traumagenic plurality was something I literally could not care about with how bad my symptoms and day to day life was. I think its important for people to be able to acknowledge when they have an opinion because they can't currently "afford" or dedicate time to contemplating otherwise because that is 100% okay and fine! But it can become a bit dangerous / reinforcing to a toxic mindset and prevent the eventual growth if that is one of the largest reasons behind the shunning of a group but you instead claim it to be another reason as it might prevent you from actually re-evaluating your beliefs when you DO gain the ability.
Largely for me, changing stances was something that came pretty naturally the more I recovered and the less the symptoms burdened me. With less day to day stress I had less to project, I had more time and space to consider things beyond basic survival, the more care and compassion I had for others, the more trust and benefit of the doubt I could offer to others, and the more I learned that I could let personal grievances and conflicts aside for mutual peace and benefit.
Along with that, I got a lot more insight and engagement with my eastern culture, my family's history and inter-generational trauma with colonization and how colonization appears systemically in Modern Western Society, delved deeper into Buddhist and Buddhist philosophy, got trained in culturally and trauma-informed mental health care, and just really lost my trauma-driven addiction to conflicts and "winning" and gained a lot more of an appreciation for the ability to non-judgementally discuss experiences with one another.
Overall, I'm pro-endo solely in the sense I would rather open up discussion and talk about experiences in a non-clinical manner rather than force every experience into the Western Clinical Perspective when not everything that appears atypical in western society / culture is inherently something that has to be pathologized.
Some Posts Relating to this Topic: Some Nuance in Colonialism in Western Societal Systems Discussion on the Theory of Structural Dissociation's Assumptions + lack of cultural sensistivty / responsiveness of people when discussing it A Large Breakdown of Tulpacourse Components of Discussion; parts involve talking about non-western perspectives of self if you'd like to skip past the tulpacourse centered talk Discussion / Explanation and Original Discussion of What I Call the "Standardized Singular Self" that is Pushed and Its Role in Racism / Colonialism (also relating to tulpacourse, but syscourse in general)
I do believe that the clinical label of "DID" is a trauma disorder, but even then I do believe that the DSM-V and ICD do mental health a large disservice placing mental conditions into categorical boxes rather than dimensional measures, particularly since most research suggests that most mental health conditions lie on a spectrum of symptoms rather than clear and concrete differences. Therefore, I believe the debate of "does DID have to have trauma" is a bit of a circular, uninteresting, and non-practical discussion as the very concept of DID - as I would say with most disorders - is not the more concrete. (Doubly so since trauma is actually not in the diagnostic criteria for DID so there is room for clinician interpretation and for an individual who does not have the standard trauma in the standard developmental time frame to be diagnosed with it)
I think a more interesting discussion - even on the clinical end - is "Can an individual without trauma and/or trauma outside of the typical developmental window for CDDs develop dissociative amnesia, dissociative fugue, and alternate identity states and if so, what conditions may influence it and how may these symptoms / experiences present differently than the typical presentation of CDDs within the developmental window?" because..
It defines "DID" and "CDD" in a more dimensional and quantitative measure than the categorical and qualitative measures that the DSM diagnosis provides and allows for much more nuanced and precise research / data to be collected
It defines what I am interested in researching more clearly than "DID" or "CDD"
It does not assume that something people report to exist does not; Science should accommodate practical evidence of something contrary existing and explore why the contrary information does not apply to the theory at hand OR adjust to include and account for the contrary evidence
Some Sources and Readings Related: The DSM-V actually already acknowledges that dimensional approaches are more appropriate and some of the changes from DSM-IV reflect this; a large reason for the maintence of the categorical approach to describing mental illness is that it conclics with the medical model / insurance model and risks complicating clinical practices (x) Dimensional vs Categorical Readings, neutral and/or from both sides (x) (x) (x)
Also @indigochromatic cause I think you'd like this discussion + they're also a great blog to look at. @hiiragi7 also might be worth looking into too.
Hi! Feel no pressure to answer, but I have a few questions (regarding DID)
So I'm aware of what an endo system is, but I'm a bit confused on why it would be considered valid since the condition is directly caused by trauma, which is the thing that endos lack. Could you please explain your perspective on it? And maybe your perspective before you became pro-endo?
Hey! I've been sitting on this ask for a few days now. I do want to start out by thanking you for reaching out to me and asking about my perspective. Please note that you are not obligated to agree with me, or to change your mind just from my answer to your questions. I like having you as a mutual, and I will continue to do so regardless of your syscourse stance.
I'm going to grab a term that some of my mutuals in the DID community have used, and say I'm really more pro syscourse conversation than I am pro endo- pro endo is just the easiest way to communicate my basic stances.
I think the most important thing to understand here is that a lot of the time, the "are endos real" debate suffers from both sides fundamentally misunderstanding what the other's stance actually is. While there is a small subsection of the endo community claiming that DID isn't trauma based- which I vehemently disagree with, DID is absolutely trauma based, and that's backed by all of the research- that's not the majority.
Most endogenic systems are not claiming to have DID. They are claiming to experience themselves as more than one. I am by no means an expert on this, but I know that it is a very western-centric view to assume that everyone subscribes to being one singular self. If you want to learn more about non-western views on the self and on plurality, I would recommend looking at @system-of-a-feather's blog. They make great posts on the subject!
And- here's a real kicker- not everyone with a CDD- CDD standing for complex dissociative disorders and including the likes of DID, OSDD, P-DID, UDD, etc- actually identifies as plural. Not everyone with even DID identifies as plural. So if someone with a CDD can identify as one, what's stopping someone who doesn't have a CDD from identifying as more than one? This post puts it pretty well, so I'm just going to link it here! And if you're looking for scientific backing on endo systems? Dr Colin Ross, one of the very well known DID researchers, believes in non-traumagenic self states.
Basically, I'm choosing to believe people when they talk about their subjective personal experiences.
Now you did also ask about my anti-endo days and I will also gladly talk about those. I will admit, I was the worst kind of anti-endo. I was the type of person who would throw even other CDD systems under the bus as fakers because I wanted to seem more legitimate. Everyone who didn't present the "right" way was a faker. And endos, my goodness. They were the worst fakers of them all.
It was an extremely reactive position to take. I was suffering from my plurality, therefore everyone who wasn't had to be faking. They were making a mockery out of me! At least, that's how I perceived it.
And then I started interacting with endos, and pro endos. I realized that they were also real people, not just an abstract concept to make fun of to make myself look more legitimate. And I started reading blogs that had the rawest, realest content about CDDs that I'd come across thus far... and they were pro endo. And the arguments as to why were really good.
Somewhere along the way, I realized that the things that were leading me to being anti endo were the same things that made me into a transmed when in the 2010s. I believed that people had to meet a minimum quota of suffering to be real. In a way, I was defining people by it. And ultimately, if they are lying? It costs me nothing to believe them. I'd rather believe some liars than not believe people who are telling the truth. I've had enough experience with people not believing me. It sucks. I didn't want to keep doing that to others.
That's about the end of this yap session! Seriously, thanks again for asking, I really enjoyed writing this post. I hope I answered in a way that makes sense to you!
#sysconversation#pro-endo#pro endo#actuallydid#research#discussion#tosd#theory of structural dissociation
63 notes
·
View notes
Text
The Continuum of Dissociation
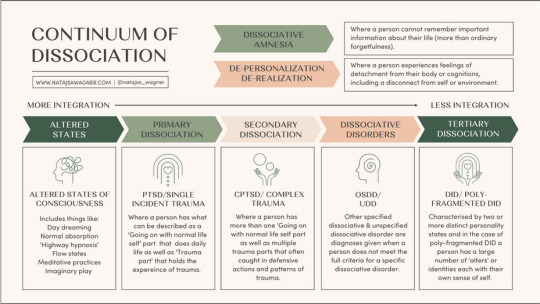
[Image description:
An infographic describing the continuum of dissociation and the theory of structural dissociation. From left to right (more integrated parts to less integrated parts), are:
Altered states - Altered states of consciousness: Includes things like daydreaming, normal absorption, 'highway hypnosis', flow states, meditative practices, and imaginary play
Primary dissociation - PTSD / single incident trauma: Where a person has what can be described as a 'Going on with normal life' part that does daily life, as well as a 'Trauma part' that holds the experience of trauma
Secondary dissociation - C-PTSD / complex trauma: Where a person has more than one 'Going on with normal life' part as well as multiple trauma parts that often are caught in defensive actions and patterns of trauma
Dissociative disorders - OSDD / UDD: Other specified and unspecified dissociative disorders are diagnoses given when a person does not meet the full criteria for a specific dissociative disorder
Tertiary dissociation - DID / polyfragmented DID: Characterised by two or more distinct personality states, and in the case of polyfragmented DID, a person has a large number of 'alters' or identities, each with their own sense of self
Outside of the parts model, but still within dissociation, are:
Dissociative amnesia: Where a person cannot remember important information about their life (more than ordinary forgetfulness)
Depersonalisation & derealisation: Where a person experiences feelings of detachment from their body or cognitions, including a disconnect from their self or environment
End image description]
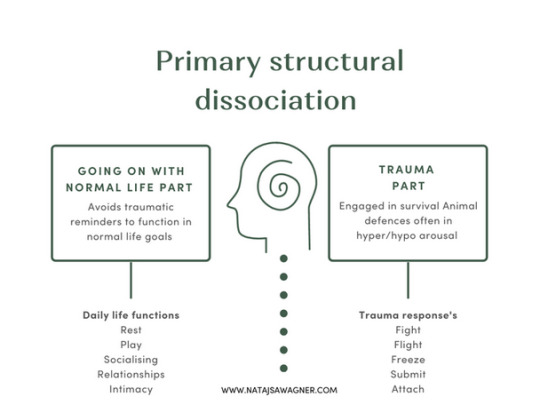
[Image description:
An infographic describing primary structural dissociation.
In primary structural dissociation, there is a 'Going on with normal life part', which avoids traumatic reminders to function in normal life goals. Daily life functions include rest, play, socialising, relationships, and intimacy.
There is also a trauma part, which is engaged in survival / animal defences and is often in hyper- or hypoarousal. Trauma responses (defences) are: fight, flight, freeze, submit, and attach.
End image description]
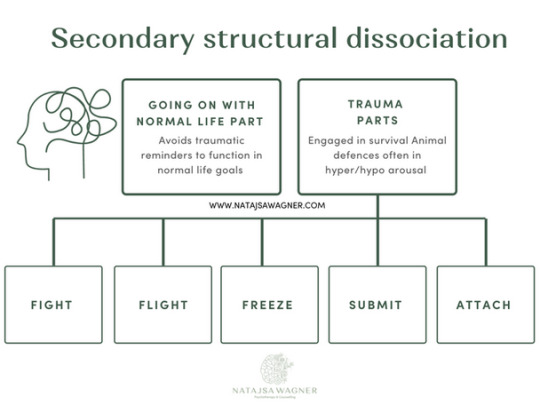
[Image description:
An infographic describing secondary structural dissociation.
In secondary structural dissociation, there is a 'Going on with normal life part', which avoids traumatic reminders to function in normal life goals.
There are also multiple trauma parts, which are engaged in survival / animal defences and is often in hyper- or hypoarousal. Trauma responses (defences) are: fight, flight, freeze, submit, and attach.
End image description]

[Image description:
An infographic describing tertiary structural dissociation. It gives an example of a system, the collection of all alters (parts) within a person.
In tertiary structural dissociation, there are multiple 'Going on with normal life parts', one or more of which may be called the 'host(s)', who are engaged in daily life. Examples of going on with normal life parts are a worker alter, a caregiver alter, and a partner alter.
There are also multiple trauma parts, which are alters engaged in survival defences. Examples of trauma parts are a gatekeeper alter (who decides who fronts), fight alters (e.g. Ann, a 24 year old primar protector part, and Don, a 30 year old persecutor part), flight alters (e.g. Sally, an 8 year old trauma holder), freeze alters (e.g. Marcus, a 10 year old trauma holder), submit alters (e.g. Pia, an 18 year old trauma holder), and attach alters (may be called 'littles', e.g. Lily, a 4 year old and Jack, a 6 year old, both trauma holders).
End image description]
- Natasja Wagner
#actually now that i read the 1st its kinda shitty. starts off good but when it gets to OSDD & DID it loses it - where are the DLP & TPs?#wheres the text explaining that DPDR and DA arent part of the ToSD but still dissociative disorders (which i added in the description)?#maybe i'll make a better one.#actually all of these are shit. lol#described#described in post#structural dissociation#dissociative identity disorder#primary dissociation#secondary dissociation#tertiary dissociation#altered states of consciousness#dissociation#theory of structural dissociation#dogpost
109 notes
·
View notes