#understanding the spectrum (updated)
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr.com rank in the US is 25.
Text
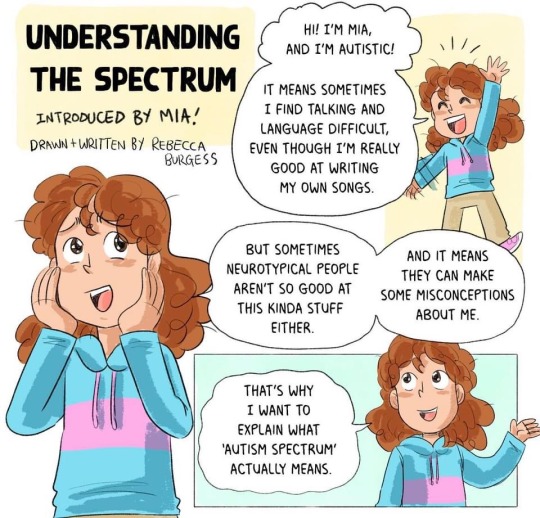
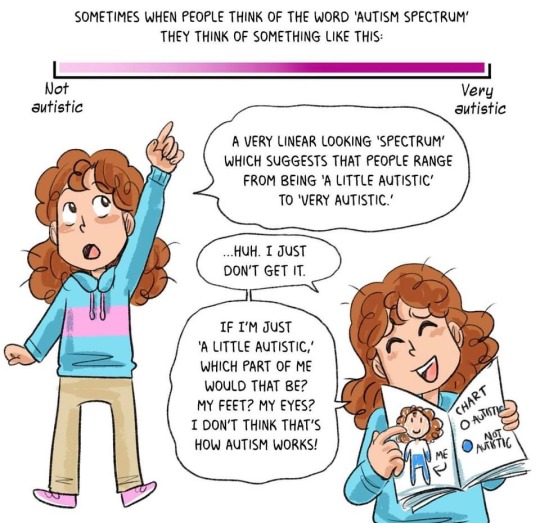
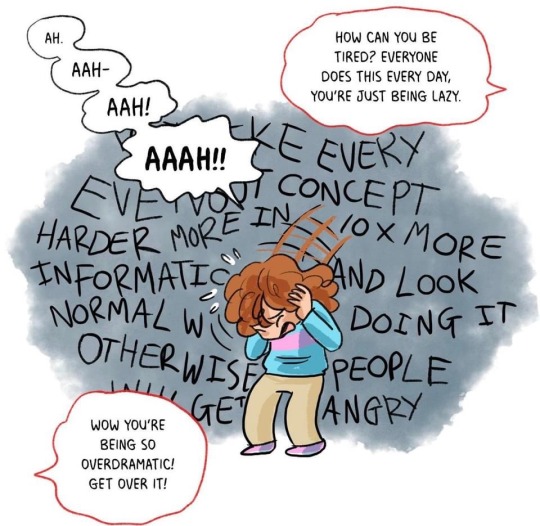
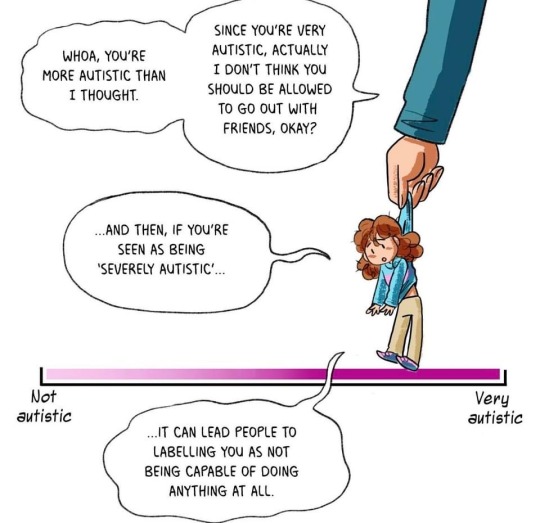
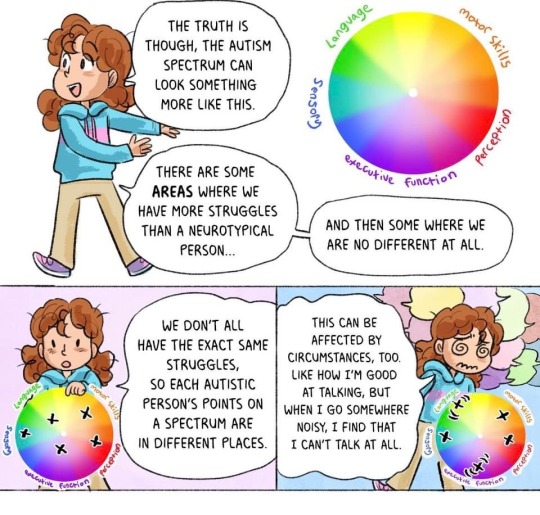
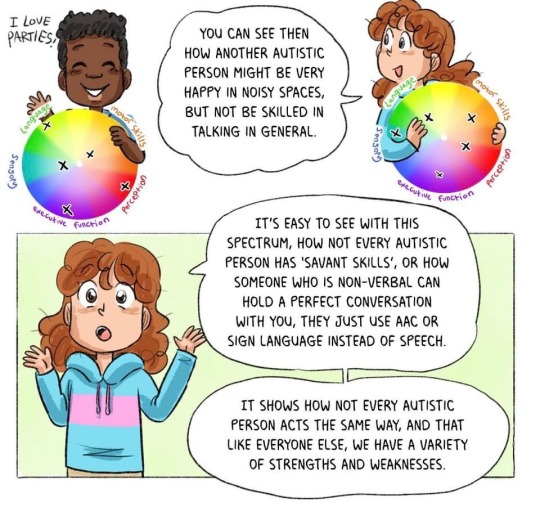
Understanding The Spectrum (updated)



I CAN Network Ltd
#autism#autism awareness month#autism acceptance month#understanding the spectrum (updated)#informative#educational#actually autistic#neurodivergence#neurodiversity#actually neurodivergent#feel free to share/reblog#I CAN Network Ltd (Facebook)
435 notes
·
View notes
Text
The Hazbin hotel fandom (and the various Alastor ships I consume) have me wondering if I might be somewhere on the aro spectrum. Further research is needed. Will report back with updates. 🫡
#genuinely#this is not a drill#or a joke#im going to do more research on it because i understand by definition what it is#and see the various points on the spectrum to see if i might fit aomewhere on there because#ive been wondering whats different about my relationships for a year because like#yes im clingy and affectionate#but im like that with...everyone???#my brother#my best friend#my mom#my dad#my sisters#so like.... idk#idk ill figure it out#will come back with updates
1 note
·
View note
Text
So, I despise Peter Beinart.
I respect an intellectually honest critic of Israel, but that's not what Peter Beinart is. He's a Jewish antisemite, an even more dangerous one than Norman Finkelstein. I can think of few people I detest more, or with better reason.
On the other end of the spectrum, among people I admire most (as is obvious to any follower of this blog), is Haviv Rettig Gur.
So I was pleased to see Haviv has written a short essay about Beinart, in response to this piece of shit Beinart wrote about Purim, taking the opportunity to once again attack the Jewish people "as a Jew."
It's excellent.
Beinart has gone full antisemite. Really. Actually. In fairness to him, I’ll explain why. You know that weird neighbor who leaves comments online about money-grubbing Jews? He’s not really an antisemite. He’s just an idiot. Scratch the surface and you’ll find he has stupid, petty opinions about everyone. Antisemitism is much more ambitious. An antisemite believes it is their righteous duty to sit in judgment of the Jews for a great, archetypal, culture-defining criminality. The Jews’ first great crime, of course, was deicide, or at least the refusal to accept Christ or Mohammed. But it has since been updated to serve new masters. The particulars change, but not the substance. Not the fundamental demand that Jews answer for some unique and history-altering villainy for which all Jews are deemed accountable and complicit. Are you starting to see it? The demand is powerful, because it always comes from a position of power. And it has felled many a Jew over the centuries, sad souls who sought safety from their oppressors first through acceptance of the iniquity ascribed to them and then by joining in the antisemite’s crusade to make other Jews do the same. Nine hundred years ago, one tormented Jew succumbed to this relentless pressure, found relief in conversion and then enthusiastically joined in the holy effort to persecute the Jews. (To understand why they must be persecuted, read St. Augustine on the Jews. Or the relevant passages in the Quran.) That Jew’s name was Theobald of Cambridge. He converted to Christianity and in service to his new faith brought forth the first known accusation that Jews ritually murder Christian children. Thanks to the hard work of some concerned priests, his accusation spread like wildfire throughout Europe. Countless Jews would die in the ensuing centuries at the hands of those enraged by the blood libel. And a Jew invented it. A Jew yearning for validation in the antisemite’s withering gaze, a Jew desperate to atone for the murder of God and the delay of history’s redemptive finale. What Beinart now peddles to anyone willing to listen is an ideologically updated version of the same claim of deep-seated and defining criminality in the Jews. He confirms to our tormentors that this criminality is the distillation and apotheosis of the great evils of our age. And he demands a great accounting from the Jews. All the Jews. Categorically. And of course, the censorious Torquemadas of the Guardian, who would deem it bigotry to say such a thing about the world’s Muslims, consider it ennobling and virtuous to level this demand at the Jews. The Jews’ crime, after all, is no ordinary breach. It is, as ever, paradigmatic, culture-defining and history-altering. And Beinart, like Theobald of old, surrenders himself to their holy judgment and demands that the rest of us do the same. This is it, folks. This is the real thing. Well done, Peter. You looked and looked and finally found it. Absolution. Acceptance. You are deemed righteous by those who see in the rest of us a great and abiding criminality. You are free at last. Of us, of our genocidal religion, of our child-murdering cabals. Be at ease.
Source
156 notes
·
View notes
Text
Very small thought about the TS demo update ! Beware it has spoilers (idk how to use tumblr help).
I really enjoyed the changes overall. They made it very crystal clear that there is something wrong in Leander's way of acting. I like the new characterization for a lot of reasons, most of them being already mentionned by many people. So i won't go into details with this because i have nothing to say except....
It is very hard to play an asexual character in the case you chose to pursue Leander. And i DO understand that the whole...red choice thing appeals to like, 99% of the fanbase and players so it's fine by me. But, i just wish there was an option for the MC to like ...not be into this as much as it was described ?? Or at least, toning it down and making the reaction that you want your MC to have as an option ?
As a person who might be very well into the ace spectrum, it made me cringe a tiny bit and my MC being 100% sex-repulsed, i spent the last lines screaming "No bitch you don't THINK THAT." "That ain't you lol" "lalala imma pretend it never happened".
But well, i do very much understand why they made the MC horny and i've seen everyone liking it so far so i understand that my complain may feel insignificant. At best, i will just ignore it and pretend it never happened. I will still hopefully be able to have a great experience with this game and Leander's route once it's released.
As long as the MC is described consenting the intercourse, it's alright and it's what truly matters.
That's all thank you for coming to my ted talk lmao
#touchstarved game#touchstarved#touchstarved leander#touchstarved update#red spring studios#leander ts#asexual
69 notes
·
View notes
Note
hi, i'm AUDHD myself and i've been trying to figure out if "high functioning" and "low functioning" are appropriate terms to use about autistic people?
i've heard that they're ableist because, well, to be honest it sounds ableist and very inappropriate. i might be wrong, but weren't the terms made by Hans Aspergers?
but then again i've heard/hear autistic people using there terms for *themselves* claiming they are correct terms and help them with their identity but it feels so wrong. maybe i'm misunderstanding? how could someone call another person "low functioning"?
Hello,
They're outdated. For a lot of people in the community, these terms are the ones they were diagnosed with and the ones they self-described with, so they keep using the terms even though new terms have emerged. Some people like these terms, some are neutral to them, some are only okay with them if autistic people are the ones using them like me, and some do not like these terms at all and may even consider them akin to slurs. Functioning labels are seen by many as ableist and dehumanizing, I would air on the side of caution and only use them if you're autistic to self-identify or to describe someone who uses those labels (I do know several people who use functioning labels because they're easier or familiar.)
As for Asperger's, you're right, it was named after a Nazi (Hans Asperger) who created the category for eugenics purposes. It used to be a diagnosis, though, and many people were diagnosed with it and might even still be diagnosed as that in their medical records. Some people are attached to this label because it's how they self-describe and are reclaiming it, but it understandably makes a lot of people very uncomfortable due to it being a label created explicitly for eugenics and due to it being a term coined by a Nazi. It's also named after Hans Asperger who created the divide between "useful" autistics, who could be in the Nazi forces, and "useless" autistics (as the Nazis called them, a "life unworthy of life,") who would be killed. This term is also based on an extremely outdated understanding of autism, which was the belief that autism is a disorder similar to schizophrenia and "psychopathy," which is no longer a valid diagnosis (never really should have been a valid diagnosis to begin with) and largely falls under the diagnosis of antisocial personality disorder, when autism is very much its own diagnosis and not part of or defined by schizophrenia or a personality construct. This idea is extremely outdated and has been scientifically proven to be incorrect, similar to female hysteria. This term is really not one someone should be using unless they are autistic and using it to describe themselves, and even then it's still a very loaded term.
(Asperger's is also still a valid diagnosis people are being diagnosed with to this day in other countries that use the ICD-10 rather than the DSMV-5 of the ICD-11. The DSM isn't the main diagnostic criteria in many countries and some countries haven't yet updated to the ICD-11, so make sure to research which text is used in the country your setting is in.)
The modern terms are autism spectrum disorder and support needs labels, which are generally no support needs, light support needs, medium support needs, high support needs, and very substantial support needs. There are also autism levels (levels one, two, and three, one being light or no support needs and three being high or very substantial support needs,) though not everyone likes those.
If someone uses terms that are, medically speaking, outdated when describing themselves, it's fine to use those words in reference to them. But don't force them on people who don't like them. And when writing an autistic character, it is best to use the most up-to-date knowledge possible unless the time of the setting prevents that, because the most up-to-date terms are the ones considered most medically accurate.
(And if your setting is before autism was created as a diagnosis in 1910 by Eugen Bleuler, here is a Wikipedia page that includes other terms used up until the World Health Organization in 1978. It might be best to avoid using the r-slur if at all possible. Lois Lowry in her book "The Silent Boy" did this rather elegantly in her description of an autistic character who lived long before the autism diagnosis was a thing, in which he was referred to as "touched," meaning "touched in the head," or "touched by God," rather than as the r slur. Try to avoid using the r slur, I cannot stress this enough.)
Mod Aaron
140 notes
·
View notes
Text
Understanding 12th House Synastry
(*updated* and more accurate post about about 12th house synastry overlays along with Neptune synastry that makes harsh aspects to another's inner planets such as the Sun, Moon, rising, Venus or Mars)

This post focuses exclusively on a 12th house relationship between two kind and evolved individuals. While there are other darker themes associated with 12th house synastry — such as deception, substance abuse, hidden affairs (like being the other woman or mistress), lies about one partner’s true nature, or fear that one partner is withholding information or their true self — I won’t be discussing those here. Here is a link to a post about how these darker themes may manifest: Click Here
“Though I barely know you, it feels as if I do. Your eyes and body language seem to speak your thoughts, even the ones I can’t fully grasp. There’s no visible thread connecting us, yet this feeling remains.” — Planet Person
There are two sides of 12th house synastry that I commonly see. The spectrum is different compared to the 8th house because with the 8th house, there are highs and lows, obvious extremes, there's oftentimes constant lessons, cycles and loops, but with the 12th house, there's a different undertone.
The 12th house is a very unforeseen house, when it comes with synastry, the spectrum of love that can be received and given is unfathomable. I am going to first discuss what this energy is like when someone deals with this type of synastry while having Neptune (especially harshly) aspecting their inner planets/12th house placements/Pisces placements; then I will go in-depth for how they would feel without those placements.
(that being said my main discussion deals with the foundation of both individuals having attraction or interest on both ends, as well as other intense synastry overlays such as harsh or soft attraction synastry aspects, + eros, lilith, chiron, pluto, or 8th house synastry)
As a 12th house native or with heavy Pisces influence (e.g., a Pisces Venus, Sun, Moon, rising, or with a natal Neptune squaring, opposing or conjunct the Sun, Moon, rising, Venus) this type of synastry is confusing, it's blurry and parts of you can second guess almost everything about them, what you are to them, what they are to you etc. There are no tangible boundaries when it comes to the emotional depth you are willing to feel for them. On some days you can find yourself wondering where you stand with them, you fixate on their energy, and you'll wonder if they're thinking of you. You look into their eyes and just feel their mental health struggles, their fears, their hidden thoughts, what they need to hear to feel seen past the 3D. You're like a walking and breathing affirmation audio tape of everything their subconscious always wished to of heard throughout life. That one broken image or belief they have within their subconscious self is the one thing you can't help but compliment them on, the feelings they ignore, suppress or hide away are the feelings you want to naturally reassure them about. It's like you become this real life 3D fixer upper for this individual, and you just can't help but be drawn with saving, helping, or fixing them. (undoubtedly so if you also fall in their 2nd house, especially your inner planets, if there is no 2nd house influence then the compliments/praising will be less intense or frequent)
The beginning of this synastry embodies confusion. Since there's no real tangible statement or understanding you can hold onto. You'll just know how they operate before ever really knowing them.
You'll just want to make sure that they are okay, and that can come in many different ways, you yourself will just know. You can turn into this savior that they never knew they needed, you'll just want to give and love everything out of them; and in some cases receiving or having that mutual give and take may be something you think you don't need, especially when it comes to them, and especially if you have a natal 12th House Venus or a Pisces Venus/a Natal Venus that squares, conjuncts or opposes Neptune (this can apply to the Moon as well).
If the above scenario resonates with you, then this individual is provoking a wound within yourself that deals with the acceptance of receiving authentic love. This innate need to only give highlights your own fear of receiving real reciprocal, stable, tangible love.
Therefore if you want to save, fix, heal or give, this desire only highlights that fearful nature within you where you allow to stay in shallow waters. You subconsciously know that you have such passionate love to give, but that thought of giving to someone who in turn might be willing to give back evokes fear and uncertainty within you.
This subconscious block holds more comfortability within you since it allows you to never accept a love where your soul will fully be fulfilled. It's self sabotaging and self written, you naturally already know how the story will end between you two, and so you subconsciously will find a character who perfectly embodies the story you yourself say you try to run from.
To reiterate; if you share the above placements you instantly can become drawn towards the house person. You will look at them and see every facet of their being, their hidden pain, their sorrows, why they feel the way they do, why they struggle the way they struggle, their mental health dilemmas, their soul; especially so if you as well have a water Moon that harshly aspects Neptune as well as the above listed placements. But these feelings don't persist automatically or openly, the desires the planet person or the one person who has the placements I listed/spiritual enlightenment + attraction towards the house person (or the other person) stays at bay and stays being unsaid, especially in the beginning. The planet person with these placements etc etc, can hold onto constant dilemmas and wonder if what they are feeling is real, if what they desire is one sided, especially if there is little to no communication between the dynamic.
On the other side of the spectrum, this bond (when wanted on both ends) can create a soul binding connection where the house person would feel like no one else can ever understand them the way the planet person can. No one else would be able to read them like the book they secretly are, no one else can look into their eyes and bring solace into their bones, which in-turn can cause the dynamic between them to consistently become something that is impossible to let go of.
With attraction + desire the house person may feel like a hug from the planet person* (or vice versa) is equivalent to receiving a sense of understanding and safety that they weren't aware they ever needed. The house person may just find themselves fully being able to lay and hold onto the planet person* and there's this unsaid desire just be next to them. The planet person* may instinctively feel this pull or knowing that there is a softer more serene side of the house person that not everyone see's and even though there's no tangible words to hold onto, that feeling within them doesn't dissipate. Just with one hug from the house person and the planet person* will know that there's a soft and quiet side inside them that they hide or suppress away.
* = placements I listed + spiritually understanding/enlighted
The house person will ask themselves: How do I let go of the one soul who speaks to the parts of myself that I don't even know? The intensity of the bond can vary based on each others natal placements, but I do believe the connection can become deep and unworldly even without the placements I've listed since attraction and desire are two KEY factors that would override any natal placement. Instant psychic understanding about one another on both ends (regardless of natal placements) can occur, you both will know what the other person is thinking, feeling, and needing. If there is genuine desire for one another then the depth of care can become very ethereal and unspoken, especially if the Moon or Venus are involved; if attraction is present and you have the placements I mentioned, a part of you will just want to hold onto the house person. You'll just want to comfort and be present in the moment with them. All that matters to you is that they are doing and feeling okay, with them this part of you unlocks where you just want to caress their soul. But like I said natal placements do have an immense influence, one individual could feel this pull and understanding (w/o the placements I mentioned) but the depth and length for caring may not run as deep as someone else who has the natal placements I listed. They will still care in some shape or form in ways they never knew was possible; but the turnover of moving on or of minimizing selfless acts can become more shallow and less frequent throughout time.
When wanted on both ends with genuine care and desire the song Run To You by Lea Michele perfectly depicts this type of deep care.

Now this type of synastry can also begin the influence of delusion or false presumptions. Genuineness and self awareness is key, not everyone will desire such depth of the unknown especially if they themselves have no set understanding of their own subconscious beliefs.
To reiterate, if this is one sided therefore if they don't share attraction or desire for you; then this type of behavior will feel invasive and they may become confused or unsure with what to do with that type of depth that your eyes can bring them, if they are unaware of their own shadow self, along with not wanting to change or be spiritually awoken, this type of connection can be daunting and misleading in some way for them.
Now lets go deeper: for someone who doesn't have any 12th house Venus, Pisces Venus, Neptune influence (or if you have little to no attraction or interest towards them), or low spiritual awareness/acknowledgement of your own mental health struggles/hidden fears and if someone comes in to your life where they fall in your 12th house, the feelings that acclimate mainly are confusion, resistance or hesitation. You might have some hidden curiosity about the planet person but generally the curiosity can be the furthest you go with this individual. There might be some hidden tension or eye glances towards another but with it there is also a barrier between the two of you. You may feel like you know their body language or what their eye glances mean but you more than likely brush it off and set aside any spiritual coincidences that you have with them. You may also wither back and forth between being more inclined to getting to know them to being unsure with your interest in them or there's a sense of unpreparedness you may struggle with when it comes to this individual. A part of you may feel like their type of love can sooth parts of you that you ignore or mentally struggle with but that type of care can feel unneeded and can bring in fear; since there is a unspoken knowing of what they are able to truly view and feel for you if they were your partner. You may ask yourself, "Can this person fix, and heal me? " "Do I really need to be saved?" "Is this all in my head?" "Can they be the pacifier for the pain I can't even openly express; or will they bring me more sorrow?"
(this dilemma of curiosity is more apparent if you share other direct intense synastry aspects such as 8th/pluto/intense attraction aspects especially with eros or lilith etc)
Another strong note I wanted to state is how often times with 12th house and Neptune synastry; the reason why this is the house of "hidden enemies" or there's horror stories where one partner hid addiction, lies, another woman or their true agenda towards the other partner is because this type of synastry can genuinely cloud judgment and hinder honest communication. There is often hidden uncertainty or a lack of awareness of what is really going on, primarily because this dynamic makes it easy to fall "victim" to a false persona. This happens when you're unaware of your own wounds, patterns of self-undoing, or fears surrounding with receiving reciprocal love. While I'm not going too in-depth with these themes—since, in my opinion, they deserve their own post—I want to reiterate the importance of staying grounded, aware, and avoiding getting lost in illusions or overthinking about someone who you know won't (or can't) change.
That being said, if there is a connection where one person has these natal placements and desires for the other individual but the other partner doesn't share the same attraction/placements; then that is when unrequited love or unspoken love can occur. To summarize, for 12th house and neptune synastry to be mutual even if the other partner doesn't have those natal placements, there has to be attraction or desire; whether it be physical, or emotional. Someone could have these placements that I've listed but if there is no want, attraction or desire towards the other person; the dynamic can also become one sided on their end even with the placements and tendencies of being drawn towards connections that share 12th/neptune/pisces influence.
12th house synastry is the house of selflessness, this is the house of giving and giving to no end; since in one essence this house holds no end or beginning, therefore the boundaries and understanding that this house can carry is unknown. Each dynamic with 12th house synastry can be complexed, there are many factors that play a role in influencing this type of connection such as your natal placements, their natal placements, your natal aspects, their natal aspects, your desire and attraction and their desire and attraction and so on. Someone could sit in this confused and undesired energy for the other person for months and have all the placements I've listed. Therefore if that said individual is not prepared or have any desires to hold a connection that is deep and unspoken, they themselves (the planet person or the person who has 12th house/neptune/pisces influence) may even still feel fear or invasiveness towards the other individual that their share 12th house synastry with or vice versa; there are so many avenues and routes these connections can take, at least that's from my own astrological understanding and take on these type of connections.
Side Note: To balance the intensity these synastry aspects/overlays bring, taking on the opposite houses themes would bring more ease and create less intensity.
For example, dealing with 12H (Even Neptune) synastry, the opposite house is the 6H, the house of routine, daily life, mundane affairs, healthcare, helping others/giving etc etc. So to ease this type of fixation this synastry can cause, focus and enhance your own skills when it comes to your physical/mental health. Add more day to day to activities that solely focuses on changing your routine; however big or small. That will ease the fixation that 12H and Neptune synastry brings. This synastry can cause you to daydream or obsess over them, and since you may have this innate need to be their savior that wants to try and fix their wounds, the chance of putting yourself in situations where your priority is solely them is very likely. You could also fantasize and have an escapist attitude with them, (or the idea of them) therefore, they can serve as an escape for you; by focusing on their pain and struggles might cause you to forget about your own mental health challenges. You also might repeat scenarios in your head or fantasize about situations happening; especially since you might feel confused/hazy with where you stand with them, therefore keeping yourself busy is key with this synastry, and that will create more control within you.
P.S
This is all from my own interpretation of 12th house synastry, I would confidently say I am a very very introspective person at heart, I read between the lines constantly and overly fixate on behavior etc and this synastry still clouded my own judgment and understanding for years; it brought in tendencies for me to doubt my true feelings and curiosity, only until I more so let go of the relationship that I am referencing (the boy where I have 8th house synastry with) was the only time I was able to fully look outside my situation with him when it came to my actions and feelings. The constant back and fourth dilemma I struggled with when it came to knowing him and who he was was constant yet truly instant. My soul knew him before my brain did and because of that knowing I was unsure and unconfident with the type of feelings that persisted in the dynamic I shared with him. I have made so many posts about 12th house synastry but I can confidently say that this current post is now the most accurate representation of what can occur between these relationships.
Hope this brings some clarity and understanding for others who have dealt with 12th house and Neptune synastry; if not disregard and again this type of synastry is truly nuanced and multifaceted.
If this resonates with you I have an eBook that perfectly depicts and explains if you are in a karmic relationship. It's about 8th/12th/Pluto/Neptune/Saturn/Vertex/Nodal synastry. I give insights, exact transits, exact synastry overlays, natal chart interpretations and more advice on what to do in these situations. More information is pinned on my page.
#astrology#astro notes#astro observations#12th house synastry#8th house synastry#8h synastry#12h synastry#8th house#astrology notes#pluto synastry#neptune syanstry#neptune square moon#12th house#12th house placements#moon oppose neptune synastry#moon conjunct neptune synastry#12th house moon#12th house venus#12h house synastry#venus conjunct neptune#venus oppose neptune#venus square neptune#12th house sun#12h venus#12h#12h placements
739 notes
·
View notes
Text
A Collection of Posts to Read Before Asking About the Blind Prophet / Blind Seer Trope
Hi all,
I thought I would start creating collections of my posts on this topic. Please read these before asking about the blind prophet trope, as I believe these will answer most questions. To ensure you are reading the most up-to-date version, go to my pinned post and find this under the blind prophet trope discussion in bold. It should direct you to the most updated list if you found this through a reblog. See if these posts answer your questions before asking me.
Trope Discussion: The Blind Prophet / Blind Seer Trope
Below is a list of questions I have answered that seek advice on avoiding the problems often associated with this trope. In some, I highlight what writers are doing well. In others, I offer suggestions for possible changes.
A post that contains discussions of two different characters with future vision, only one of whom is blind, which helps in avoiding the association of future vision with blindness. It also discusses avoiding making up for blindness and having more than one blind character.
Here is a post about avoiding erasing blindness with prophecies and using other senses instead.
Here is one where the asker has written about the spectrum of blindness as well as a blind character who isn’t the only one who can see the future.
Here is a post where the writer displays a blind community and avoiding erasing blindness using a special visions of the future. The character seems to be totally blind and I offer suggestions of using other senses instead of sight or giving the character residual vision to use instead. Includes details and links about the spectrum of blindness.
This post is a great follow-up reinforcing another option for the above linked post and for this trope in general, which is writing a character whose future vision is the same as it is in the present. The character can use multiple senses, including residual sight, to understand the future just as they would in the present.
Another ask about giving the character future visions with the same sight they use in daily life. For example, tunnel vision or central vision loss should occur in both future visions and daily life. The writer also addresses having other blind characters, a twist on the prophet trope, and switching from writing the character as temporarily blind to being blind since birth. I also suggest having a blind character not a prophet. Having another prophet who isn’t blind might also work.
While the information in these posts may not address every possible scenario, I hope they are helpful.
217 notes
·
View notes
Text
Welcome to the Are They T4T poll blog!
where you submit ships you think are t4t and we let strangers on the internet decide if you're correct!!!
What is this?
this is a poll blog that centers around t4t ships that are not explicitly stated as canon.
How does it work?
via asks, submitters can send ships and we (as a collective)(by we I mean the internet) decide whether or not they're t4t!
I still don't understand...
any questions you have can be sent to my inbox, and I'll be happy to answer. remember, there are no dumb questions!
FTM/MTF VS Transmasc/Transfem
Please use transmasc/transfem when you mean someone on the transmasculine/transfeminine spectrum, not necessarily non-binary, but not binary trans
Please use trans man/trans woman when you mean someone who is binary trans
Please use ftm/mtf when you mean someone who uses the label ftm/mtf, or someone who identifies as a boy who used to be a girl/girl who used to be a boy
Please use a different label if you mean something different, or use unlabeled trans/non-cis if you dont have one in specific
Rules
No transphobia, transandrophobia, or transmisogyny. this should be obvious but I'll say it anyway
No harassment. keep discourse on your own blog, here we follow the rule of if you don't have anything nice to say, keep your mouth shut
Similar to above, everyone is allowed to have their own headcanons. If you don't agree with it, you can scroll.
T4T here is not just the binary trans, you can submit genderqueer headcanons of all identities!
All characters are allowed except those from fandoms in Fandom Jail, which will be updated as I go.
I personally am not comfortable with darkships, please don't submit them here. I am relying on the honor system. If you do not adhere to this rule, you will be blocked.
What counts as a darkship, mod? If the ship is between a minor and an adult, family members, or a human and an animal, it is a darkship. Everything else is fair game. I'm updating this policy.
No cis characters please. I support cis people but that's just not what's happening here
I will add more if I need too, but I don't think I'll need to!
Fandom Jail
Hazbin Hotel/Helluva Boss. Anything from that creator in general.
Harry Potter and all spinoffs
Heartstopper
What should I include in my submission?
Character names (no nicknames, or if you put a nickname, include the full name of the character as well. Double check your spelling).
Label/Identity. Trans man, trans woman, nonbinary, etc.
Media Name. Especially video games.
A photo. It really helps me and everyone else. I do not put the names of who submitted what; your submission is anonymous even without anon on.
Propaganda, if you want! Not required!
Submission Example/Template
*this template is not required, it's here to help*
"My ship is between Character A and B (and C, etc if they're polyam). Character A is (transmasc/transfem/enby/etc), Character B is (transmasc/transfem/enby/etc), (it's the same if there are other characters)."
If you'd like, you can also submit the relationship type (ex: couple, throuple, fwb, polycule, etc). Not required.

Me tagging for reach: @kiss-marry-kill-polls @aretheyasimp @aretheypolyamorous @do-you-ship-it-polls
45 notes
·
View notes
Text
Shared Canon Info
Updated - 3/7/25
Sun and Moon
Their birthdays are June 28th
They can’t eat, but Moon makes up for that by drinking oil and eating bolts (“boltcorn”) ((edit: this may have been retconned))
They both use platform (shoes, I’m assuming) to boost their height sometimes
They’re both waterproof
Their mouths do open, they just choose not to open them most of the time
Sun and Moon don't drink (retconned)
Fazbear's apparently sells dakimakuras/full body sized plushies of Sun and Moon
Sun and Moon's island home is somewhere in the pacific ocean, closer to Europe than it is to America (as of 7/4/2024, they've moved out of their island home)
When Sun and Moon first separated, Sun had no idea how to put kids to sleep. He'd never done it before, so Moon had to teach him how
Sun and Moon can pop their limbs off like magnets
Lunar and Moon
Sun and Moon are a little over 7ft tall
Sun and Moon both have lithium iode batteries (the same kind of batteries that are in laptops)
They both have ADHD
They both hate mannequins and seem to have some form of automatonophobia
They both don't like jelly
They both like sweets
Sun and Lunar
They both have exceptional aim with shooting games
Moon and Earth
They’ve both binge watched MLP
Earth and Lunar
They both enjoy baking and like cute things
They do not like anything scary
They can both understand at least a little bit of Spanish
Lunar and Earth could both drink. Lunar doesn't (that we know of), but Earth likes wine every so often
Lunar and Earth both like mythology
Sun and Earth
Sun and Earth watch Munk together for their one on one sibling hangouts sometimes
Sun and Earth both like doing a lot of arts and crafts
The celestial siblings, as a whole
The celestial siblings keep a movie collection up in the room above the ballpit. The collection has movies they like (like "Princess and The Pauper" for Earth, "Breakfast Club" for Moon, and some unnamed violent movie) as well as movies for the kids that come to the daycare
Sun might be the only one in the family who doesn't have ADHD (Unsure. May have to look into this more)
None of them like Ruin, Bloodmoon, or the creator, and Earth is the only one who likes Eclipse
Everyone in the celestial family is likely somewhere on the autism spectrum (as stated by Moon, I believe. If anyone knows who said this, feel free to correct me if I'm wrong)
#sun and moon show#the sun and moon show#tsams#laes#lunar and earth show#tlaes#sams sun#the sun and moon show sun#sun and moon show sun#sams moon#the sun and moon show moon#sun and moon show moon#tsams sun#tsams moon#the lunar and earth show#tlaes lunar#lunar and earth show earth#lunar and earth show lunar#laes earth#laes lunar#tlaes earth#canon info
185 notes
·
View notes
Text
fuck it ! updated masterpost of my bad kids hcs :)))))
adaine - she/her. transfem. aroallo (specifically arospec. shes not entirely sure beyond that). autistic. has anxiety + depression (but is working on it !!!) and pots. passes out a lot because of that and also The Visions
fabian - he/him. transmasc (has been on t for years. passes well. people just assume hes a cis guy w tits). bisexual demiromantic (he does Not know the latter bit though. he thinks he's allo <33). fetal alcohol spectrum disorder. hard of hearing due to ear infections (related to fasd) in early childhood. he has hearing aids and knows common and halfling sign language. in addition to missing one eye he also doesn't have peripheral vision in the other and his residual vision is pretty desaturated. (the Knife To The Eye thing in freshman year caused an infection that spread to his optic nerve and he didnt . get help . for a bit too long <33.) (he also has epilepsy and gets sick more often due to said infection.) uses a long cane as well as other assistive arcanotech idk. also had bpd (specifically impulsive bpd)
fig - any pronouns. genderfluid. bi. has lupus and fibromyalgia. for her that mostly means chronic pain + chronic fatigue + brain fog. uses a cane or a rollator. adhd + bpd
gorgug - she/they. transfem. pan. type 1 diabetes. autistic + semiverbal (aac user) + ocd
kristen - they/she. nonbinary. lesbian. adhd. hypermobile eds and gastroparesis. their joints are Constantly dislocating. they usually wear various braces and kt tape to prevent that.
riz - he/any neos (esp likes e/em and xe/xem). agender? but in a masc way (goblins have a different understanding of gender than other races. they see gender as very fluid and not tied at all to whatever sexual organs they have. most goblins look similar regardless of gender/agab. no one remembers what riz's agab is lmao. including his family.) aroace. he basically has fantasy multiple sclerosis - autoimmune response after the kalina curse got expelled from his body. he has trouble moving his legs and (increasingly so as of late jy) his hands. uses a wheelchair + wears afos. he cant really feel his legs below his knees. doesn't have strong trunk support so he has a strap to keep him upright. brain fog which is the only part of that he's really frustrated by. audhd.
BONUS:
aelwyn - she has psychosis and is autistic. she masked a Lot in childhood but is now beginning to unlearn that ! she's also aroallo. im adaine and im aelwyn the aroallo autistic sisters
ayda - she/her. transfem. audhd
ragh - has fetal alcohol syndrome as well. helps fabian unlearn the self hate he has surrounding it 🙂↕️ also psoriasis
mazey - she/her. transfem. deaf
younger applebees siblings (only sadie as really figured this all out at this point though) -
sadie - (formerly bucky) she/her. transfem. bi. i love her so so so much did you guys know. i lvoe her. ouagh.
bricker - he/him. gay. bidactylous symbrachydactyly (left hand)
cork - any pronouns. genderqueer. aroace.
they all have adhd
OCS:
felicity 'lissie' faeth - (fig and fabian's little sister.)she/her. sapphic. unilateral cleft lip (hallariel had her get surgery for it but there's still a distinct scar). fetal alcohol spectrum disorder + anxiety. eldritch knight fighter
runa gorrash - (lissie's partner <333) she/he. autistic and has sturge-weber syndrome, which in her case causes a port wine birthmark, glaucoma, weakness on left side, and seizures. sometimes uses a cane and/or braces (knee and shoulder). she has a service bear, ukul, who alerts for seizures and is also her primal companion. orcish ranger/cleric. fat genderfuck butch !!!! my best friend
lio - (fabian's half sibling, theyre both kids of bill seacaster. raised in leviathan, ayda's childhood friend.) they/any. transverse forearm deficiency. aka their left arm ends about 2 inches from their elbow. also a scar on their forehead from where whitclaw tried to suck their brain out lmao. human rogue/sorcerer
#guys im normal. im normal come closer. i prommy#ant.txt#ant.ocs#d20#fantasy high#fhjy#dimension 20#fabian seacaster#riz gukgak#kristen applebees#adaine abernant#fig faeth#gorgug thistlespring#figeroth faeth#runa gorrash#lissie faeth#lio#applebees siblings#sadie applebees
31 notes
·
View notes
Text
SnaccPop 2024 Agenda - New Focus, More Content!

2023 was fun-- but rough.
Now, SnaccPop is headed more than ever by a whole collective of impressive people from not only all over the world, but all over the creative spectrum! And in assembling the SnaccPop crew, we've been adjusting during the end of the 2023 year.
2024 is where that adjustment turns into progress!
OUT WITH THE OLD! (Old projects, that is-)
While SDJ has seen delays and a new episodic structure, we are in the process of pushing for a 1/2 release (demo included) by the end of the year! We hope a single-time purchase with free content updates will keep the game fresh for longer in the hearts of players. And we're hoping to have at least 1/2 of that story out by the end of the year!
Audio Drama Content and BoTM Returns!
Audio drama and BotM content both did very well with audiences during their limited appearances last year! With Project Drama Boy (a non-series roleplay audio initiative) and BotM returning, we're hoping to have more content available to fans this year too!
More Free Content!
We see that we have an ever-growing free-tier fanbase forming. We, at one point, used to make audio dramas free after a certain period! And while this model did take some effort, we'd like to make it our goal to put out additional free content for our subscribers to enjoy, regardless of their financial situation!
More ART!
With additional artists on hand, we're hoping to bring you more accessible art content (SFW or otherwise--) to go with your games, audio, updates, and posts! We'd like to see comics, artist collaborations, and more going forward!
AphroDesia FINALLY
Due to voice actor scheduling mishaps, sick leaves, and more, AphroDesia sadly saw 2023 with minimal updates. But we'd like to see the series fully revived with an audio pilot and a comic series!
---
We'd like to take a moment to thank everyone who supported us through 2023. We understand that we fell short of our goals, but this year we'd like to take this year head-on!
We'd like to MAKE MORE. More art, games, and stories-- we'd like to entertain and share. We'd like to spend 2024 telling more diverse stories with diverse characters! And we'd like to make more men with fat honkers, butts of all sizes, and weird, weird themes and genres.
Let's get this year, together. Let's just get all the men, every man, together. v - v
Happy Holidays, Happy New Year, and thank you from SnaccPop Studios!
#snaccpop studios#snaccpop#somethings wrong with sunny day jack#sunny day jack#swwsdj#sdj#the groom of gallagher mansion#tgogm#bachelor of the month#project drama boy#aphrodesia#minors dni
269 notes
·
View notes
Note
Hi i have a question. Is there a time when labeling yourself aro isn't valid? Once I saw someone say that to label one's self as aro out of conscious choice or convenience is wrong.
I ask because I'm afraid that I too am probably using the label for the purpose of dodging romance. I mean I saw no reason to label myself aromantic before, because I thought that people would, by default, not choose me as a romantic partner. I never thought of myself that way and I assumed that everyone else will follow suit. Only now, that I am directly exposed to romance, did I ever use the term aromantic to describe myself.
So this is how I got the idea to label myself aromantic. I don't want to be in a romantic relationship, but I didn't want to let my best friend down, but two weeks into it I realized that I didn't like the rules or norms of romance. It made me feel like an alien in my own skin. And then I thought, I am probably aro, and I did come out as Aro, which my best friend/romantic partner took with extreme doubt and constantly questioned me like this: "are you sure you're aro? We're in a romantic relationship now. Are you still Aro?" and I felt sort of pressured, and there I began thinking that I might be faking it?
I feel like I only said I'm Aro because I didn't like how romance works. I didn't know what I was getting into before agreeing.
Then one day I come across a post that says that you can't just say you're aro if you're saying it out of convenience, which I might have done, because I don't know how to exactly tell my best friend that our romantic relationship feels like lead in my veins. So I said, I'm aromantic.
I think I'm running around in circles here I'm so sorry. In short, I got into a romantic relationship, hated everything about it, and then labeled myself Aro in hopes to make people understand why I dislike romantic things when I'm directly involved. Is that... Invalid? And what other ways could someone be misusing the term to the detriment of the community?
Thank you for accommodating my strange ask :)
honestly, the way that you came to that conclusion - that a romantic relationship that you were/are in felt like lead in your veins - is actually... a really common way people start to realize they are actually aro? and if you hate romance when it's directed at you, that's... also a pretty common path to realizing you're aro?
for the life of me, I've never seen someone who is aromantic ever say that you can call yourself aromantic in bad faith, but I've seen a LOT of people who think all aro people are invalid/predatory/etc say that. I generally assume bad faith, because every aro person I've ever met has agreed that coming out as aro doesn't mean shit to the people that it's supposedly being shitty to in that way anyways. they neither are familiar with it, nor believe in it, and I've never personally heard a single story yet that didn't turn out to literally be like. a queerphobe, transphobe, and/or aphobe sockpuppet.
so. no. i don't think there's a time when labeling yourself aro is invalid, and in your circumstances, I think if anything, I'd strongly advise you to interact more with aro experiences and trust yourself over what others say or want you to feel. a great resource for learning more about our community is linked here:
53 notes
·
View notes
Text
Intersex Guide! (Updated 5/5/2025)
(UPDATED: May 5th, 2025. Please reblog again if you only saw our old versions. Please also reblog if you've never seen this before, to spread awareness.)
Hello and happy pride! We wished to share a passion project we have been working on for months - a guide to intersex traits and variations!
Now, a question that many ask - what is intersex? Well, we will be answering that question for you here! Anything on this post that is written in red is NOT intersex, so if you wish to skip over any of it, you can. And if you wish to get straight into the intersex types, scroll down to the read-more and start from there.
Intersex, also known as the intersex spectrum, is a term used to describe when someone's biological sex - as in the sex they are born with/what they naturally develop during puberty - is not clearly defined as the typical male or female sex traits.
(This does not include someone that was born male or female, and later chose to have their sex traits changed due to being transgender, transsex, or altersex. It also does not include males that experienced circumcision/dorsal slits or penis splitting, females that experienced genital mutilation, or males & females that indulged in modifications such as piercings and beading.)
This only applies to primary sex traits - chromosomes, genitals, reproductive organs, hormones, and hormone responsiveness. Atypical secondary sex traits (breasts, muscle tone, body/facial hair, deepness of voice) do not make someone intersex unless it is paired with "abnormalities" in primary sex traits.
Before you can understand what it means to be intersex, first we must clarify what it means to not be intersex.
A typical male has XY chromosomes, a penis, two testicles within the scrotum, a prostate, and more androgens (mostly testosterone) than females. Their androgen levels fall into a typical range compared to other males. Upon puberty, they usually (but not always) develop more facial hair & muscle tone than females, and a deeper voice than females.
(Note: A penis has a phallus, a scrotum beneath the phallus, foreskin protecting the head of the phallus, and a urethra on the head of the penis. It is straight or slightly curved when erect.)
A typical female has XX chromosomes, a vulva, two ovaries, a single uterus, and more estrogen than males. Their estrogen levels fall into the typical range compared to other females. Upon puberty, they usually (but not always) develop larger breasts and wider hips than males.
(Note: A vulva has two labia, a single pea-sized clitoris, a single vaginal entry, and a urethra above the vaginal entry and under the clitoris.)
Here is a list of non-typical sex traits that, by themselves, are not intersex.
Accessory Breasts (Polymastia): Having more than two breasts. Accessory Nipples (Polythelia): Having more than two nipples. Athelia: Having only one nipple, or no nipples at all. Amastia: Having only one breast & nipple, or no breasts & nipples at all. Breast Hypertrophy/Macromastia/Gigantomastia: Having extremely large breasts Gynecomostia: Breasts on a male. The reason this is not considered intersex is because all sexes (except for people with amastia) have breast tissue, which can vary in size regardless of sex. Females can have small breasts, and males can have larger breasts than is expected. Hypotonia: Low muscle tone. Bicornuate Uterus: A heart-shaped uterus. Septate Uterus: A uterus that internally has a partition down the middle. Macropenis: A penis that is 7 inches/17.78 centimeters or larger. Macroorchidism: Testicles that are 4 milliliters or above pre-puberty, and above 30 milliliters as an adult. Macrovagina: A vagina that is deeper than 5 inches/13 centimeters. Labial Hypertrophy: Labia that is longer than average (above 2 inches/5 centimeters)
Now, onto the intersex spectrum! First, some notes.
-An intersex trait is a singular atypical trait. For example, someone with ambiguous genitals, but no other "abnormality" has an intersex trait. -An intersex variation is when multiple atypical traits are present, with at least one of them being an intersex trait. For example, someone with ambiguous genitals and fused kidneys has an intersex variation. Equally, someone with ambiguous genitals and cryptorchidism also has an intersex variation. -CTF stands for "close to female." CTF traits are characteristics that are closely associated with females (vulvas, uteruses, ovaries, estrogen as the main sex hormone, breasts, widened hips, XX chromosomes, etc.) CTF people are intersex people who call their body as a whole CTF, due to a majority (but not necessarily all) of their sex traits being CTF (ie; a person with breasts, a uterus, ovaries, and a penis might call themself CTF, even though not all of their traits are CTF in nature.) -CTM stands for "close to male." CTM traits are characteristics that are closely associated with males (a penis, testicles, androgens as the main sex hormones, increased hair growth, higher muscle mass, a deepened voice, XY chromosomes, etc.) CTM people are intersex people who call their body as a whole CTM, due to a majority (but not necessarily all) of their sex traits being CTM. -CTA stands for "close to androgynous." CTA traits are characteristics that are predominantly "androgynous", or an equal mix of "feminine" and "masculine" (ie; ambiguous genitals, ovotestes, XXYY chromosomes, etc.) CTA people are intersex people who call their body as a whole CTA, due to a majority (but not necessarily all) of their sex traits being CTA, or they have a near-equal mix of CTF and CTM sex traits. -CTN stands for "close to neutral." CTN traits are characteristics that are predominantly "neutral" (ie; small/absent/blocked off genitalia or reproductive organs, a lack of hormone production, 0X chromosomes, etc.) CTN people are intersex people who call themself CTN, due to a majority (but not necessarily all) of their sex traits being CTN.
Also, when we state that an intersex trait/variation is "fairly common", we mean that it is fairly common amongst the intersex population, not that it is fairly common in the general population. Being intersex is still classified as "rare" statistically speaking (as statistics define "rare" as 1 in 1,000 people.)
So for the sake of this post, here is how we are classifying the following:
"Fairly common" = 1 in every 5,000 (or less)
"Rare" = above 1 in every 5,000, up to 1 in every 100,000
"Extremely rare" = above 1 in every 100,000
Keep in mind that "may co-occur" means that not all of the features will be present on every single person with that variation; in fact, none of the extra features could be present. However, for chromosomal variations specifically, it is highly likely that at least 1-5 (or more) of the listed extra features will be present.
And finally, when we say that "fertility is average", what we mean is that the gonads are fully capable of producing healthy average numbers of sperm/eggs, and/or the uterus is capable of carrying healthy babies. Struggles with the sperm reaching the eggs still might occur, but if direct insemination is done (as in the sperm is directly injected), then pregnancy should occur perfectly fine.
-------------------
Penile Traits/Variations (not including those on the agenital spectrum)
These are traits that affect the development of the penis.
Congenital Chordee: An trait in which an individual is born with a curved penis. This curve may be on its own, or it may be curved due to webbed-skin on the scrotum connecting to the penis and holding it in a curved manner. As a lone variation, those with congenital chordee have XY chromosomes, testicles, and a prostate. They may also have hypospadias. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and will likely have increased body/facial hair, higher muscle mass, and a deepened voice. They can produce semen, but it may not be able to exit the urethra depending on its placement. Fertility is average. This trait is extremely common, occurring in 1 of every 200 AMAB births.
-
Penoscrotal Transposition (PST): A trait in which an individual is born with a scrotum that is in front of the penis, rather than beneath it. A Shawl Scrotum/Donut Scrotum is a form of PST where the scrotum completely surrounds the penis like a shawl. As a lone variation, those with PST have XY chromosomes, testicles (possibly cryptorchidism, in which case the scrotum surrounding the penis is full of empty tissue), and a prostate. They may also have hypospadias. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and will likely have increased body/facial hair, higher muscle mass, and a deepened voice. They can produce semen, but it may not be able to exit the urethra efficiently, depending on the urethra's placement. This trait is extremely rare. Due to the rarity, little is known about the fertility status, however it appears to be average. Common traits and disabilities that may co-occur include absent kneecaps, ureter abnormalities, an absent or underdeveloped kidney, heart disease, overgrown/protruding ribs, widely-spaced nipples, an incurved pinkie finger, a small lower jaw, a chin dimple, folded eyelids, a large/protruding back of the skull, cerebral atrophy, and intellectual disability.
-
Diphallia/Bifid Penis: A trait in which an individual has two penises (either next to each other or one on top the other.) These penises could be of the same size, or have a size difference. A urethra may be present on only one penis (possibly with epispadias or hypospadias), both penises, or they may have a single urethra that is in-between both the two penises. Erections may be possible in both penises or only in one. As a lone trait or variation, those with diphallia have XY chromosomes, testicles (possibly with cryptorchidism), and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and will likely have increased body/facial hair, higher muscle mass, and a deepened voice. They can produce semen, but it may not be able to exit the urethra efficiently, depending on the urethra's placement. This trait is extremely rare. Due to the rarity, little is known about the fertility status, however it appears to be average. Common traits and disabilities that may co-occur include pubic bone abnormalities, an extra hole (not an anus) that leads into the rectum, an absent anus (which will need surgical intervention in order to pass waste), two colons, an extra ureter, fused kidneys, an extra kidney, a rotated kidney, an inguinal hernia, gastrointestinal abnormalities, an extra gastrointestinal tract, exposed organs on the lower abdomen, heart abnormalities, spinal abnormalities, and an absent thumb.
-------------------
Urethral Traits/Variations (not including those on the agenital spectrum)
These are traits that affect the development of the urethra.
Urethral Duplication/Double Urethra: A trait in which an individual with a singular set of genitals has two urethras. One of the urethras may not fully reach between the bladder and genitals, either cutting off before reaching the bladder (making it visible from the outside, but without a use), cutting off before reaching the genitals (making it connected to the bladder, but not visible or accessible from the outside), or cutting off in the middle (making it connected to the bladder, and visible from the outside, but a blockage existing somewhere in the middle internally.) As a lone variation, this comes in both an XX form and an XY form. Those with the XX form have XX chromosomes, a vulva (usually with epispadias for one or both of the urethras, however the urethras could be side-by-side as well) or clitoromegaly & fused labia, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Those with the XY form have XY chromosomes, a penis (usually with hypospadias or epispadias for one of the urethras, though both can be side-by-side on the penis head), two testicles, and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. This trait is extremely rare. Due to the rarity, little is known about the fertility status of this variation, however it appears to be average (implying those with testes can produce sperm, and those with a uterus can get pregnant.) Common traits and disabilities that may co-occur include an extra ureter, an extra bladder, urinary tract infections, an extra rectum, an extra colon, an absent kidney, an abnormally-located kidney, kidney cysts, spinal abnormalities, and an opening between the windpipe and the esophagus.
-
Hypospadias: A trait in which an individual with a penis is born with a urethra that is located lower than typical. This could be lower on the head of the phallus than typical, or it could be on the shaft, the scrotum, or even underneath the phallus. As a lone variation, they have XY chromosomes, a penis/micropenis (possibly with chordee or PST), testicles, and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and will likely have increased body/facial hair, higher muscle mass, and a deepened voice. They can produce semen, but it may not be able to exit the urethra depending on its placement. Fertility is average. This trait is extremely common, occurring in 1 of every 250 AMAB births. Vulval Hypospadias/Hypospadias Feminis is an extremely rare form of hypospadias that occurs on vulvas, in which a urethra opens lower than typical, possibly on the vaginal wall (meaning it may appear as though an individual is urinating out of the vagina.) As a lone variation, those with vulval hypospadias have XX chromosomes, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Due to the rarity, little is known about the fertility status of vulval hypospadias.
-
Epispadias: A trait in which an individual is born with a urethra that is located higher than typical. On a penis, this refers to a urethra that is located above the typical spot on the penis head. Ona vulva, the urethra is on the stomach or above/in the middle of the clitoris (thus splitting the clitoris into two.) As a lone variation, this comes in both an XX form and an XY form. Those with the XX form have XX chromosomes, a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Those with the XY form have XY chromosomes, a penis, two testicles, and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. Fertility is average (implying those with testes can produce sperm, and those with a uterus can get pregnant.) This trait is extremely rare. A common trait/disability that may co-occur is exposed organs on the lower abdomen.
-
Urogenital Sinus Anomaly (UGS)/Persistent Urogenital Sinus Anomaly (PUGS): A trait in which an individual has a single opening, which is a combination of both urethral and vaginal tissue, and connects to both the urinary tract and the reproductive tract. This opening could be the size of a typical vaginal entry, the size of a urethra, or somewhere in-between. As a lone variation, those with UGS have XX chromosomes, a vulva or clitoromegaly & fused labia, two ovaries/an ovary (unilateral ovarian agenesis) or ovarian agenesis, and a uterus (possibly with uterine hypoplasia) or MRKH syndrome. Puberty may be absent or delayed. If they start puberty naturally (and don't use HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Pregnancy is possible if they have a uterus that is present and large enough. If they have no ovaries, an embryo implant will be necessary. Alternatively, if they have no uterus or a uterus that is too small for pregnancy, but have ovaries, their eggs can be used to implant an embryo into another carrier. This trait is rare.
-
Persistent Cloaca: A trait in which an individual has a single opening for urination, menstruation/sexual output, and feces (being a combination of the urethra, vaginal entry, and anus.) This opening could be the size of a typical vaginal entry, the size of a urethra, the size of an anus, or somewhere in-between. It could be placed anywhere from the crotch to between the buttocks, or somewhere in the middle. Partial cloacas may occur as well, in which the anus and the vagina are combined but the urethra is still separate, or the anus and the urethra are combined but the vagina is still separate. As a lone variation, those with persistent cloacas have XX chromosomes, a vulva or clitoromegaly & fused labia, two ovaries/one ovary (unilateral ovarian agenesis) or ovarian agenesis, and a uterus (possibly with uterine hypoplasia) or MRKH syndrome. If they have a uterus and a partial cloaca, they may have a double cervix, with one cervix in each opening. If they start puberty naturally (and don't use HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Pregnancy is possible if they have a uterus that is present and large enough. If they have no ovaries, an embryo implant will be necessary. Alternatively, if they have no uterus or a uterus that is too small for pregnancy, but have ovaries, their eggs can be used to implant an embryo into another carrier. This trait is rare. Common traits and disabilities that may co-occur include a dilated colon, a dilated vaginal entry, urine buildup (which may cause a stretched/swollen kidneys or ureter), an absent kidney, an oddly-placed kidney, heart defects, a tethered spinal cord, and an underdeveloped esophagus.
-------------------
Ambiguous Genitals
These are traits in which a person was born with a combination of vulval and penile characteristics. Micropenises are often considered a part of this spectrum.
As a lone trait, this can come in a CTA, CTF, or CTM form.
The CTA form can have any mix of gonads, reproductive organs, hormone production, and puberty. Typically they either have XX or XY chromosomes, however occasionally they may have a chromosomal variation as well.
Those with the CTF version have XX chromosomes, two ovaries (or ovotestes), and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips.
Those with the CTM version have XY chromosomes, testicles (or ovotestes) and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice.
Ambiguous genitals are fairly common, occurring in 1 of every 5,000 births.
Bifid Scotum: A form of ambiguous genitalia where a penis is present, however the scrotum is separated in a labia-like fashion around the phallus. Fused Labia: A form of ambiguous genitalia, where a vulva is present, however the labia is fused in a scrotum-like fashion. The fused labia either covers the entirety of the vulva (leaving only the clitoris) exposed, or half of the vulva (leaving the clitoris & urethra exposed, but the vaginal opening mostly or fully hidden.) There may be tissue within the labia that appears like small testicles. Clitoromegaly: A form of ambiguous genitalia, where a vulva is present, however the clitoris is enlarged, being over 1 inch (2.54 centimeters) in diameter. In some cases, it looks like a small penis. Combined Clitoromegaly & Fused Labia: A form of ambiguous genitalia, where a vulva is present, however the labia fuses to resemble a scrotum and the clitoris is enlarged, creating a structure almost identical to a small penis. The vaginal opening is fully hidden under the labia. Pseudophallus: A form of ambiguous genitalia, where a vulva is present, however the clitoris is enlarged significantly (beyond the typical clitoromegaly expectations) and is merged with labia, creating a significantly-sized penis-like structure. Penis & Vulva Combo 1: A form of ambiguous genitalia where a vulva is present, however the labia stretches up and merges with a penis, becoming the outer skin & foreskin of the phallus. The penis is located where the clitoris usually is (thus replacing the clitoris.) No scrotum or descended testes are present. The urethra is on the vulva, below the penis. Penis & Vulva Combo 2: A form of ambiguous genitalia where there is a penis (with no scrotum or descended testicles) that has a vulva underneath it. The vulva has labia (which is not merged with the penis) and a vaginal opening. It may also have a clitoris beneath the penis as well. The urethra is on the vulva, below the penis. Penis & Vulva Combo 3: A form of ambiguous genitalia where there is a penis with a scrotum (possibly with descended testicles) that has labia (which is not merged with the penis) and a vaginal opening, but no clitoris. The urethra can either be on the tip of the penis or on vulva beneath it. Penis & Vagina Combo: A form of ambiguous genitalia where there is a penis with a scrotum (possibly with descended testicles) that a vaginal entry tucked beneath the scrotum.
It is important to note that the term Clitorophallus is often used as an umbrella term to describe micropenises, clitoromegaly, combined clitoromegaly & fused labia, and pseudophalluses.
-------------------
The Agenital Spectrum/Agenital/Agenitalia
These are traits in which a person was born with absent, small, or closed off genitals. Anorchia & Monoorchidism fall under this umbrella as well.
Urethral Agenesis: A trait or variation in which an individual is born without a urethra. It may be visibly absent, or it may appear to be present from the outside, with a blockage of skin being within the first few centimeters or inches internally. A urethra is necessary to be surgically added, as to avoid urine buildup. As a lone variation, this comes in both an XX form and an XY form. Those with the XX form have XX chromosomes, a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Those with the XY form have XY chromosomes, a penis, testicles, and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. This trait is extremely rare. Due to the rarity, little is known about the fertility status, however it appears to be average (implying those with testes can produce sperm, and those with a uterus can get pregnant.) Common traits and disabilities that may co-occur include limb deformities, an anus covered by skin (which will need surgical intervention in order to pass waste), urine buildup (which may cause a stretched/swollen kidneys or ureter), an abnormal connection between the bowel and bladder, an absent bladder (which will need surgical intervention in order for urine to have somewhere to be collected), a small kidney, kidney cysts, an underdeveloped lung, an enlarged chamber of the heart, and heart issues.
-
Urethral Hypoplasia: A trait in which an individual is born with a narrow or underdeveloped urethra. As a lone variation, this comes in both an XX form and an XY form. Those with the XX form have XX chromosomes, a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Those with the XY form have XY chromosomes, a penis, two testicles, and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. Fertility is average (implying those with testes can produce sperm, and those with a uterus can get pregnant.) This trait is rare.
-
Vaginal Hypoplasia: A trait in which an individual has a vaginal opening that is small/tight or not very deep. As a lone variation, those with vaginal hypoplasia have XX chromosomes, two ovaries, and a uterus (possibly with uterine hypoplasia) or MRKH syndrome. Puberty may be absent or delayed. If they start puberty naturally (and don't use HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Pregnancy is possible if they have a uterus that is present and large enough. If they have no uterus or a uterus that is too small for pregnancy, their eggs can be used to implant an embryo into another carrier. This trait is fairly common, occurring in 1 of every 5,000 AFAB births.
-
Vaginal Agenesis/Vaginal Aplasia: A trait in which an individual has some or all of the external vulva (clitoris, labia, & urethra), but no vaginal opening. As a lone variation, those with vaginal agenesis have XX chromosomes, two ovaries, and a uterus (possibly with uterine hypoplasia) or MRKH syndrome. Puberty may be absent or delayed. If they start puberty naturally (and don't use HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. If menstruation occurs, birth control will be necessary in order to prevent internal buildup (as there is no exit for the uterine shedding), or surgery could be chosen (ideally by the intersex person themself, not forced upon them) to create a vaginal entry. Pregnancy is possible if they have a uterus that is present and large enough, however sperm will need to be medically injected (unless they have a vaginal entry created surgically.). If they have no uterus or a uterus that is too small for pregnancy, their eggs can be used to implant an embryo into another carrier. This trait is fairly common, occurring in 1 of every 4,000 AFAB births.
-
Imperforate Hymen: A trait in which an individual has a hymen that completely covers the vaginal opening. As a lone variation, those with imperforate hymens have XX chromosomes, a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. If menstruation occurs, birth control will be necessary in order to prevent internal buildup (as there is no exit for the uterine shedding), or surgery could be chosen (ideally by the intersex person themself, not forced upon them) to remove the hymen. Pregnancy is possible, however embryos will need to be medically implanted (unless they have the hymen removed surgically.) This trait is fairly common, occurring in 1 of every 1,000 AFAB births.
-
Microperforate Hymen: A trait in which an individual has a hymen that fully covers the vaginal opening, with only one tiny hole in the hymen. Cribriform Hymen: A trait in which an individual has a hymen that fully covers the vaginal opening, with only multiple tiny holes scattered across the hymen. Septate Hymen: A trait in which an individual has a hymen that stretches across the middle of the vaginal opening, making it appear as though there are two (or more) vaginal entries (when in reality, every hole leads to the same vagina.) Sleeve Hymen: A trait in which an individual has a hymen that is thicker than expected, leaving it to fold in on itself. As lone variations, those with microperforate hymens, cribriform hymens, septate hymens, or sleeve hymens have XX chromosomes, a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Pregnancy is possible, and menstruation may occur without any complication, however if menstrual fluids fail to exit due to the holes being too small, birth control will be necessary in order to prevent internal buildup, or surgery could be chosen (ideally by the intersex person themself, not forced upon them) to remove the hymen. All four of these variations are fairly common, with each (separately) occurring in 1 of every 1,000 AFAB births.
-
Vaginal Septum: A trait in which an individual has a vaginal opening that is partially or fully blocked by skin tissue (which is not a hymen.) A Transverse Vaginal Septum (TVS) is when the tissue runs horizontally across or within the vaginal cavity, dividing or blocking it. Depending on how deep or wide this tissue is within the vagina, it may cause the vagina to seem short/small (due to blocking the vagina mid-way), may make the cervix seem absent (due to covering the cervix), could split the vagina into two entryways (creating a double vagina, which may be obvious externally or only noticeable internally), or could be covering the entrance to the vagina altogether. An Obstructed Hemivagina is when the tissue runs vertically across/within the vaginal cavity, and curves to block part (but not all) of the vaginal entrance, leaving one side open. This might cause the vagina to seem short/small, and might cover the cervix. It may be obvious externally or only noticeable internally. This trait almost always partners uterus didelphys, blocking menstrual output from one of the two uteruses. A Longitudinal Vaginal Septum (LVS) is when the tissue runs vertically across/within the vaginal cavity, splitting it into two entryways (creating a double vagina, which may be obvious externally or only noticeable internally.) As a lone variation, those with vaginal septums have XX chromosomes, a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Pregnancy is possible, and menstruation may occur without any complication, however if menstrual fluids fail to exit due to the holes being too small or absent, birth control will be necessary in order to prevent internal buildup, or surgery could be chosen (ideally by the intersex person themself, not forced upon them) to remove the tissue. This trait is rare.
-
Labial Hypoplasia: A trait in which an individual with a vulva is born without one or both labia. As a lone variation, those with labial hypoplasia have XX chromosomes, a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Fertility is average. This trait is rare.
-
Clitoral Hypoplasia: A trait in which an individual has a vulva with a small clitoris (under 0.75 inches or 1.90 centimeters.) Clitoral Agenesis: A trait in which an individual has a vulva, but no clitoris. As lone variations, those with clitoral hypoplasia or clitoral agenesis have XX chromosomes, a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Fertility is average. This trait is rare.
-
Penile Agenesis/Penile Aplasia: A trait in which an individual who is expected to have a penis is born without one. They either have urethral agenesis, a lone urethra, or a persistent cloaca. As a lone variation, those with penile agenesis have XY chromosomes, two testicles/one testicle (monorchidism) or anorchia, and a prostate. If they have testes, cryptorchidism is common. Puberty may be absent or delayed. If they start puberty naturally (and don't use HRT), they will have testosterone as the main sex hormone, and will likely have increased body/facial hair, higher muscle mass, and a deepened voice. If testes are present, they can produce semen, but it may not be able to exit the urethra/cloaca depending on its placement and how the testes connect. Fertility is average. This trait is extremely rare. Common traits and disabilities that may co-occur include twisted feet, an absent anus (which will need surgical intervention in order to pass waste), anal abnormalities, bladder abnormalities, small kidneys, kidney cysts, urine buildup (which may cause a stretched/swollen kidneys or ureter), a hole between the heart chambers, small lungs, a connection between the windpipe and esophagus, a flat nose, and rotated ears.
-
Micropenis/Microphallus/Penile Hypoplasia: A trait in which an individual is born with a small penis. Micropenises are 0.98 inches/2.5 centimeters or less in infants, and 3.67 inches/9.32 centimeters or less in adults. As a lone variation, those with micropenises have XY chromosomes, a penis, two testicles, and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. Fertility is average. This trait is rare.
-
Congenital Buried Penis/Congenital Hidden Penis: A trait in which an individual is born with a penis that is mostly or entirely hidden within the skin of the abdomen, thigh, or scrotum. As a lone variation, those with congenital buried penises have XY chromosomes, a penis, two testicles, and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. Fertility is average. This trait is fairly common, with the exact estimates unknown.
-
Aposthia: A trait in which an individual is born with a penis that has very little or no foreskin. As a lone variation, those with aposthia have XY chromosomes, a penis, two testicles, and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. Fertility is average. This trait is extremely rare.
-
Microorchidism/Testicular Hypoplasia: A trait in which an individual is born with one or multiple testicles that are smaller than average. Microtestes are 14 milliliters or less in adults, 3 milliliters or less during puberty, and under 1 milliliter pre-puberty. As a lone variation, those with microorchidism XY chromosomes, two testicles (possibly with cryptorchidism), a penis/micropenis or ambiguous genitals, and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. They may have hypogonadism, so their testosterone levels might be lower than males. They may be capable of producing semen, but are at a higher risk of infertility. This trait is rare on its own, but fairly common when partnered with Klinefelter Syndrome.
-
Cryptorchidism: A trait in which an individual is born with one or multiple testicles that are undescended (within the body, rather than hanging in the genital area.) This trait only counts as intersex if the testicles do not descend within the first 3-6 months after birth. As a lone variation, those with cryptorchidism have XY chromosomes, a penis, two testicles, and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. They may be capable of producing semen, but are at a higher risk of infertility. This trait is extremely common, occurring in 1 of every 100 AMAB births, however it can also occur in AFAB and AXAB/UAB individuals too. A common trait/disability that may co-occur is testicular cancer.
-------------------
Gonadal Agenesis
These are traits that cause one or both gonads to be absent.
Common traits and disabilities that may co-occur with gonadal agenesis include an absent kidney, kidney swelling, and kidney stones.
Anorchia/Bilateral Congenital Anorchia/Testicular Agenesis: A trait in which an individual that is expected to have testicles instead has no gonads. As a lone variation, those with cryptorchidism have XY chromosomes, a penis/micropenis or ambiguous genitals (which may have a urogenital sinus anomaly or a hole between the urethra & vagina) or penile agenesis, and a prostate. They will not begin puberty unless they are on HRT. Due to the lack of gonads, they are infertile. This trait is rare.
-
Monorchidism/Monorchism/Unilateral Congenital Anorchia: A trait in which an individual is born with a single testicle. As a lone variation, those with monorchidism have XY chromosomes, a penis, possibly cryptorchidism, and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone (though hypoandrogenism is common, so their testosterone may be low), and likely have increased body/facial hair, higher muscle mass, and a deepened voice. They may be capable of producing semen, but are at a higher risk of infertility. This trait is fairly common, occurring in 1 of every 5,000 AMAB births.
-
Unilateral Ovarian Agenesis: A trait in which an individual is born with a single ovary. As a lone variation, those with unilateral ovarian agenesis have XX chromosomes, a vulva, and a uterus/unicornuate uterus or MRKH syndrome. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone (though hypoestrogenism is common, so their estrogen may be low), and will likely develop breasts and widened hips. They are at a higher risk of infertility. If they are fertile enough, and have a uterus that is large enough, pregnancy is possible. If they are fertile enough, and have no uterus or a uterus that is too small for pregnancy, their eggs can be used to implant an embryo into another carrier.
-
Ovarian Agenesis/Bilateral Ovarian Agenesis: A trait in which an individual that is expected to have ovaries instead has no gonads. As a lone variation, those with ovarian agenesis have XX chromosomes, a vulva, and a uterus (possibly with uterine hypoplasia) or MRKH syndrome. They will not begin puberty unless they are on HRT. Due to the lack of gonads, they are infertile, however if they have a uterus (and it is large enough), they can carry a (genetically unrelated) embryo if it is medically implanted. This trait is rare.
-------------------
Other Reproductive Traits
Gondal Dysgenesis: A trait in which an individual is born with a gonad (ovary, testicle, or ovoteste) that is full of empty tissue, rather than reproductive tissue. These are known as "streak gonads." If a person has two streak gonads, they will not begin puberty unless they are on HRT, and will have no eggs or sperm. XX Gonadal Dysgenesis/Pure Gonadal Dysgenesis (PGD) is a form of gonadal dysgenesis, in which an individual with XX chromosomes is born with two streak ovaries. They have a vulva or clitoromegaly and a uterus. They will not begin puberty unless they are on HRT. Due to the lack of eggs, they are infertile, however they can carry a (genetically unrelated) embryo if it is medically implanted. Swyer Syndrome and Mixed Gonadal Dysgenesis fall under this umbrella, and Turner Syndrome often does as well. All forms of gonadal dysgenesis are rare, except for when it occurs in Turner Syndrome.
-
Ovarian Hypoplasia/Hypoplastic Ovaries: A trait in which an individual is born with one or multiple ovaries that are smaller than typical. Unilateral Ovarian Hypoplasia is when an individual is born with one ovary that is smaller than typical. Bilateral Ovarian Hypoplasia is when an individual is born with both ovaries being smaller than typical. As a lone variation, those with ovarian hypoplasia have XX chromosomes, a vulva, and a uterus (possibly with fallopian tube agenesis or uterine hypoplasia.) Their menstruation may be irregular or absent. Pregnancy is possible if they have a uterus that is large enough, however they are at a higher risk of infertility and early menopause. If they have eggs and a large enough uterus, they may become pregnant naturally. If they have no fallopian tubes, they may need medical intervention in order to access their eggs. If their uterus is too small, then their eggs can be used to implant an embryo into another carrier. This trait is rare on its own, but fairly common when partnered with Turner Syndrome.
-
Fallopian Tube Agenesis: A trait in which an individual with ovaries and a uterus is born without one or both fallopian tubes. Unilateral Fallopian Tube Agenesis is when an individual is born with only one fallopian tube. Bilateral Fallopian Tube Agenesis is when an individual is born with no fallopian tubes. As a lone variation, those with fallopian tube agenesis have XX chromosomes, a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Those with fallopian tube agenesis are capable of producing eggs, however only people with unilateral fallopian tube agenesis are capable of being impregnated (as they still have one fallopian tube to transport eggs) meanwhile people with bilateral fallopian tube agenesis are incapable of transporting eggs (as they have no fallopian tubes) and will need medical intervention to access their eggs. This trait is rare.
-
Vas Deferens Aplasia/Congenital Absence of the Vas Deferens (CAVD): A trait in which an individual with testes is born without one or both vas deferens. Unilateral Vas Deferens Aplasia/Congenital Unilateral Absence of Vas Deferens (CUAVD) is when an individual is born with only one vas deferens. Bilateral Vas Deferens Aplasia/Congenital Bilateral Absence of Vas Deferens (CBAVD) is when an individual is born with no vas deferens. As a lone variation, those with vas deferens aplasia have XY chromosomes, a penis, two testicles, and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. Those with vas deferens aplasia are capable of producing sperm, however only people with CUAVD are capable of releasing it (as they still have one vas deferens to deliver the sperm to the urethra), meanwhile people with CBAVD are incapable of releasing it (as they have no vas deferens) and will need medical intervention to access their sperm. This trait is fairly common, occurring in 1 of ever 1,000 AMAB births.
-
Seminal Vesicle Hypoplasia: A trait in which an individual has a seminal vesicle that is smaller than typical. Unilateral Seminal Vesicle Hypoplasia is when an individual is born with one seminal vesicle that is smaller than typical. Bilateral Seminal Vesicle Hypoplasia is when an individual is born with two seminal vesicles that are smaller than typical. Seminal Vesicle Agenesis: A trait in which an individual that is expected to have seminal vesicles has none, or only one. Unilateral Seminal Vesicle Agenesis is when an individual is born with only one seminal vesicle. Bilateral Seminal Vesicle Agenesis is when an individual is born with no seminal vesicles. As lone variations, those with seminal vesicle hypoplasia or seminal vesicle agenesis have XY chromosomes, a penis, two testicles (possibly with vas deferens aplasisa), and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. They may or may not be capable of producing semen. If they are incapable of producing semen (or have vas deferens aplasia), then they will need medical intervention to access their sperm. These traits are rare. Common traits and disabilities that may co-occur include kidney abnormalities and an absent kidney.
-
Prostate Hypoplasia: A trait in which an individual has a prostate that is smaller than typical. For adults, the mass of a hypoplastic prostate is 10 cubic centimeters or less. As a lone variation, those with prostate hypoplasia have XY chromosomes, a penis or micropenis, and testes (possibly with microorchidism or cryptorchidism). During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. They may have hypogonadism, so their testosterone levels might be lower than males. They may be capable of producing semen, but are at a higher risk of infertility. The rarity of this variation is unknown. Common traits and disabilities that may co-occur include ureter abnormalities, kidney abnormalities, kidney cysts, and prune belly syndrome (a condition in which the abdominal muscles above the stomach are underdeveloped or absent.)
-
Prostate Agenesis: A trait in which an individual that is expected to have a prostate instead has none. As a lone variation, those with prostate hypoplasia have XY chromosomes, a penis or micropenis, and testes (possibly with microorchidism or cryptorchidism). During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. They may have hypogonadism, so their testosterone levels might be lower than males. Their testes typically produce sperm, however the sperm is incapable of leaving the body due to the lack of prostate, and thus medical intervention to extract the sperm would be necessary in order to create a biological offspring. The rarity of this variation is unknown. Common traits and disabilities that may co-occur include ureter abnormalities, kidney abnormalities, kidney cysts, and prune belly syndrome (a condition in which the abdominal muscles above the stomach are underdeveloped or absent.)
-
WNT4 Deficiency: A variation in which an individual with XX chromosomes has a mutation in the WNT4 gene, which causes them to be born with an absent uterus, a vulva with vaginal agenesis or vaginal hypoplasia, and two ovaries. During puberty (without the influence of HRT), they will have hyperandrogenism, leading them to have testosterone as their main sex hormone, and will likely develop clitoromegaly, increased facial/body hair, higher muscle mass, and breasts. Due to the lack of uterus, they are unable to get pregnant, however their eggs can be used to implant an embryo into another carrier. This variation is rare.
-
Mayer–Rokitansky–Küster–Hauser Syndrome (MRKH Syndrome)/Müllerian Agenesis/Müllerian Aplasia: A trait in which an individual that is expected to have a uterus is born with a completely or partially absent uterus. As a lone variation, those with MRKH syndrome have XX chromosomes, a vulva (possibly with vaginal agenesis or vaginal hypoplasia) or a urogenital sinus anomaly, and two ovaries (which may be on an atypical spot of the fallopian tubes.) During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Due to the lack of uterus, they are unable to get pregnant, however their eggs can be used to implant an embryo into another carrier. This trait is fairly common, occurring 1 in every 4,500 AFAB births. Common traits and disabilities that may co-occur include a shorter height than average, abnormally located kidneys, an absent or underdeveloped kidney, heart complications, rib abnormalities, spinal abnormalities (possibly scoliosis), a short neck, a low hairline on the back of the neck, and hearing disabilities/deafness.
-
Unicornuate Uterus: A trait in which an individual is born with a uterus that has one side fully developed, while the other side of the uterus is underdeveloped (known as a Hemi-Uterus) or absent. If a hemi-uterus is present, it may or may not be functional. If it is functional, menstrual fluids will be released from it. The hemi-uterus might have a large enough opening that allows the menstrual fluids to leak into the main uterus - however, if the hemi-uterus does not have a wide enough opening, the menstrual fluids may get trapped and buildup could occur, or menstruation could take longer to end. As a lone variation, those with a unicornuate uterus will have XX chromosomes, a vulva, and two ovaries/an ovary (unilateral ovarian agenesis). The ovaries may be on an atypical spot of the fallopian tube(s). During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Pregnancy is possible, however they are at a higher risk of premature birth, miscarriage, and ectopic pregnancy. This trait is fairly common, occurring in 1 of every 4,000 AFAB births. Common traits and disabilities that may co-occur include kidney abnormalities and kidney cysts.
-
Uterine Hypoplasia/Hypoplastic Uterus: A trait in which an individual is born with a uterus that is smaller than typical. For adults, the length (from top to bottom) of a hypoplastic uterus is 2 inches/5 centimeters or smaller. As a lone variation, those with uterine hypoplasia have XX chromosomes, a vulva (possibly with vaginal agenesis or vaginal hypoplasia), and two ovaries/an ovary (unilateral ovarian agenesis) or ovarian agenesis. Puberty may be absent or delayed. If they start puberty naturally (and don't use HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. They may have hypogonadism, so their estrogen levels might be lower than females. If the uterus is smaller than 1.60 inches/4 centimeters, pregnancy is not possible, however their eggs (if they have an ovary) can be used to implant an embryo into another carrier. If the uterus is 1.60 inches/4 centimeters or larger, pregnancy is possible. however they are at a higher risk of miscarriage and premature birth, and if they have no ovaries, an embryo implant may be the only way to become pregnant. This trait is rare.
-
Cervical Agenesis/Cervical Dysgenesis/Cervical Atresia: A trait in which an individual with a uterus is born without a cervix, leaving the uterus closed off from the genitalia. As a lone variation, those with cervical agenesis have XX chromosomes, a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. If menstruation occurs, birth control will be necessary in order to prevent internal buildup (as there is no exit for the uterine shedding), or surgery could be chosen (ideally by the intersex person themself, not forced upon them) to create a cervix. Pregnancy is possible, however embryos will need to be medically implanted (unless they have a cervix created surgically.) This trait is extremely rare.
-
Cervical Hypoplasia: A trait in which an individual with a uterus is born with a cervix that is smaller than typical. As a lone variation, those with cervical agenesis have XX chromosomes, a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Pregnancy is possible, and menstruation may occur without any complication, however if menstrual fluids fail to exit due to the cervix being too small, birth control will be necessary in order to prevent internal buildup, or surgery could be chosen (ideally by the intersex person themself, not forced upon them) to expand the cervix. This trait is extremely rare.
-
Cervical Duplication/Double Cervix: A trait in which an individual with a uterus is born with 2 cervixes. As a lone variation, those with cervical duplication have XX chromosomes, a vulva (possibly with an obstructed hemivagina or longitudinal vaginal septum), two ovaries, and a uterus or uterus didelphys. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Fertility is average. This trait is rare on its own, but fairly common when partnered with uterus didelphys.
-
Uterus Didelphys: A variation in which an individual is born with two uteruses. As a lone variation, those with uterus didelphys have XX chromosomes, possibly cervical duplication, a vulva (possibly with an obstructed hemivagina or longitudinal vaginal septum), and two ovaries (typically one fallopian tube & ovary for each uterus). During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Fertility is average, however there is a higher risk of miscarriage and premature birth. Oftentimes each uterus can be impregnated separately. This trait is fairly common, occurring in 1 of every 3,000 AFAB births. Common traits and disabilities that may co-occur include severe menstrual cramps, heavy bleeding, extra menstruation, sexual dysfunction, and an absent kidney.
-
Fallopian Tube Duplication/Accessory Fallopian Tube: A variation in which an individual is born with three (or more) fallopian tubes. The extra tubes may or may not be attached to the uterus itself. As a lone variation, those with fallopian tube duplication have XX chromosomes, a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Pregnancy is possible, however there may be difficulty with eggs reaching the uterus, due to going through one of the extra fallopian tubes, which may not have a connection with the uterus. This gives a higher risk of ectopic pregnancy and miscarriage. This trait is fairly common, with the exact estimates unknown. A common trait/disability that may co-occur is endometriosis.
-
Vas Deferens Duplication/Accessory Vas Deferens: A variation in which an individual is born with three (or more) vas deferens. The extra vas deferens may or may not be attached to the testes or prostate. As a lone variation, those with vas deferens duplication have XY chromosomes, a penis, testes, and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. Fertility is average. This trait is extremely rare. Common traits and disabilities that may co-occur include inguinal hernias, an absent kidney, and cystic fibrosis.
-
Seminal Vesicle Duplication: A trait in which an individual is born with three (or more) seminal vesicles. As a lone variation, those with seminal vesicle duplication have XY chromosomes, a penis, testes, and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. Fertility is average. This trait is extremely rare. Common traits and disabilities that may co-occur include kidney abnormalities.
-
Polyorchidism: A trait in which an individual is born with three (or more) testicles. These testicles could be descended, or they could have cryptorchidism. As a lone variation, those with polyorchidism have XY chromosomes, a penis, testes, and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. Fertility is average. This trait is extremely rare.
-
Accessory Ovary: A trait in which a person has three (or more) ovaries, with the extra ovaries being connected to the other ovaries, the fallopian tubes, or the uterus. Supernumerary Ovary: A trait in which a person has three (or more) ovaries (and possibly extra fallopian tubes), with the extra ovaries (& fallopian tubes) being detached from the reproductive system, located away from the other ovaries. If they are latched onto/pressed against a different organ (ie; the intestines), they may cause abdominal pain. As lone variations, those with accessory ovaries or supernumerary ovaries have XX chromosomes, a vulva, and a uterus (possibly a bicornuate one) or unicornuate uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. This trait is extremely rare. Due to the rarity, little is known about the fertility status, however it appears to be average. Common traits and disabilities that may co-occur include extra adrenal glands, an absent kidney, an absent ureter, an extra ureter, and pouches in the bladder.
-
Ovotesticular Syndrome/Bigonadal/Ambigonadal: A variation in which an individual is born with a combination of ovaries and testicles. This could be ovaries and testes as separate gonads, or it could be a unique gonads (Ovotestes) that has both testicular and ovarian tissue within it. If they have a testicle or ovotestes structured in a similar manner, it is common to have cryptorchidism. People with ovotestes have a uterus 90% of the time (possibly with uterine hypoplasia), and they may or may not have a prostate. They may have fallopian tubes, vas deferens, or both. As a lone trait, this comes in both an XX form and an XY form. Those with the XX form have XX chromosomes and a vulva or ambiguous genitals. During puberty (without the influence of HRT), depending on the function of their gonads, they could have any combination of secondary sex traits (widened hips, breasts, increased body/facial hair, higher muscle mass, a deepened voice, etc), and they could have estrogen or androgen as a main sex hormone, or a combination of both. Those with the XY form have XY chromosomes, a penis (possibly with chordee or hypospadias) or ambiguous genitals. During puberty (without the influence of HRT), depending on the function of their gonads, they could have any combination of secondary sex traits (widened hips, breasts, increased body/facial hair, higher muscle mass, a deepened voice, etc), and they could have estrogen or androgen as a main sex hormone, or a combination of both. People with both the XX and XY forms are at a higher risk of infertility. However, for those who are fertile, most commonly, the semen is infertile, while the eggs are fertile. However in rarer cases it is the other way around, with the eggs being infertile and the sperm being fertile. This trait is rare. Common traits and disabilities that may co-occur include germ cell tumors and inguinal hernias.
-
Persistent Müllerian Duct Syndrome (PMDS): A variation in which an individual with XY chromosomes is born with a uterus (possibly a hypoplastic uterus or an incomplete one) and possibly fallopian tubes. They usually have a prostate. In some cases, they may have an ovary or ovoteste, however most often they have testicles. If they have a testicle or ovotestes structured in a similar manner, it is common to have cryptorchidism. They will have a penis, micropenis, or ambiguous genitals. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. They may have hypogonadism, so their testosterone levels might be lower than males. They may or may not be fertile, depending on the presence (or lack thereof) of a prostate, the function of their gonads, and the size of their uterus. If they have a prostate and functional testes, they are capable of producing sperm. If they have a large enough uterus, they are capable of pregnancy (however it may need to be medically implanted, depending on whether or not their genitals have a vaginal entry.) If the uterus is large enough to menstruate, the shedding will either exit through the genitals (if there is a vaginal entry or the urethra is connected to the uterus), or it will have nowhere to go. If it has nowhere to go, birth control will be necessary in order to prevent internal buildup (as there is no exit for the uterine shedding), or surgery could be chosen (ideally by the intersex person themself, not forced upon them) to create a vaginal entry or to remove the uterus. This variation is extremely rare.
-------------------
Hypergonadism
These are traits that cause a person's gonads to produce a higher level of hormones than in males and females.
Hyperestrogenism: A trait in which an individual has high levels of estrogen. If they have ovaries, this describes having higher levels of estrogen than females do. If they have testicles, this describes having higher levels of estrogen than males do. As a lone variation, this comes in both an XX form and an XY form. Those with the XX form have XX chromosomes, a vulva (possibly with labial hypertrophy), two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone (though it will be high), and will likely develop breasts (possibly with breast hypertrophy) and widened hips. Their menstruation could be heavy or irregular. They may also have hypoandrogenism, meaning their testosterone levels might be lower than females. Pregnancy is possible, however they are at a higher risk of infertility. Those with the XY form have XY chromosomes, a penis or micropenis, and two testicles (possibly with microorchidism). During puberty (without the influence of HRT), they will either have estrogen and testosterone at near-equal levels, or have estrogen as the main sex hormone, and will likely develop breasts and widened hips, with the possibility of increased body/facial hair, higher muscle mass, and a deepened voice. If estrogen is their main sex hormone, they may also have hypoandrogenism, meaning their testosterone levels might be lower than males. They may be capable of producing semen, but are at a higher risk of infertility. This trait is rare. Common traits and disabilities that may co-occur include an early puberty (which may lead to a shorter height than average), cold hands/cold feet, weight gain, swollen or tender breasts, bumpy breasts, a higher risk of breast cancer, a low libido, thinning hair, chronic migraines, memory difficulty, sleep disorders, and mood disorders. Aromatase Excess Syndrome (AEXS/AES)/Familial Hyperestrogenism is an extremely rare form of hyperestrogenism, caused by genetic mutations in the CYP19A1 gene, which makes the body convert more androgens into estrogen than is typical.
-
Hyperandrogenism: A trait in which an individual has high levels of androgens. If they have ovaries, this describes having higher levels of androgens than females do. If they have testicles, this describes having higher levels of androgens than males do. As a lone variation, this comes in both an XX form and an XY form. In 80% of cases the XX form is caused by Polycystic Ovarian Syndrome (PCOS), a genetic condition that causes the ovaries to overproduce hormones, which may cause cysts to develop on the ovaries. Those with the XX form have XX chromosomes, a vulva or clitoromegaly, two ovaries, and a uterus. During puberty (without the influence of HRT), they will either have estrogen and androgens at near-equal levels, or have androgens as the main sex hormones, and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice, with the possibility of breasts and widened hips. If androgens are their main sex hormones, they may also have hypoestrogenism, meaning their estrogen levels might be lower than females. Pregnancy is possible, however they are at a higher risk of infertility. Those with the XY form have XY chromosomes, a penis (possibly a macropenis), two testicles (possible with macroorchidism), and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though it will be high), and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice. They may have hypoestrogenism, meaning their estrogen levels might be lower than males. They may be capable of producing sperm, but are at a higher risk of infertility. The XX form is extremely common, occurring in 5-10% of AFAB people. The XY form is rare. Common traits and disabilities that may co-occur include an early puberty (which may lead to a shorter height than average), oily skin, higher levels of acne, a high libido, bald patches, high blood cholesterol, diabetes, behavioral disorders, mood disorders, and anxiety disorders. Familial Male-Limited Precocious Puberty (FMPP)/Testotoxicosis is an extremely rare form of the XY form of hyperandrogenism, where puberty-influencing androgen production begins extremely early, causing puberty to begin between the ages of 1-5 years old.
-------------------
Hypogonadism
These are traits that cause a person's gonads to produce a lower level of hormones than in males and females.
Primary Hypogonadism/Hypergonadotropic Hypogonadism describes when the gonads themselves have low production levels. The brain is still communicating to produce the average male/female levels of hormones, but the gonads are failing to keep up with the brains-signals.
Secondary Hypogonadism/Hypogonadtropic Hypogonadism/ Central Hypogonadism describes when the brain has low levels of communication with the gonads. The brain is failing to send out typical levels of signals to the gonads, and the gonads only produce hormones when a signal is received.
Hypoestrogenism/Estrogen Deficiency: A trait in which an individual has low levels of estrogen. If they have ovaries, this describes having lower levels of estrogen than females do. If they have testicles, this describes having lower levels of estrogen than males do. As a lone variation, this comes in both an XX form and an XY form. Those with the XX form have XX chromosomes, a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as their main sex hormone (though it will be low) and have the possibility of developing breasts and widened hips. Pregnancy is possible, however they are at a higher risk of infertility. Those with the XY form have XY chromosomes, a penis, two testicles, and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone, and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice. They may be capable of producing sperm, but are at a higher risk of infertility. This trait is rare on its own, but fairly common when partnered with Turner Syndrome or PCOS. Common traits and disabilities that may co-occur include a delayed puberty, a low libido, genital dryness, a higher risk of urinary tract infections, less body/facial hair than average, low bone density, heart disease, sleep disorders, depressive disorders, anxiety disorders, and frequent headaches.
-
Hypoandrogenism/Androgen Deficiency: A trait in which an individual has low levels of androgens. If they have ovaries, this describes having lower levels of androgens than females do. If they have testicles, this describes having lower levels of androgens than males do. As a lone variation, this comes in both an XX form and an XY form. Those with the XX form have XX chromosomes, a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as their main sex hormone and will likely develop breasts and widened hips. Pregnancy is possible, however they are at a higher risk of infertility. Those with the XY form have XY chromosomes, a penis, two testicles (possibly with microorchidism), and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though it will be low), and have the possibility of developing increased body/facial hair, higher muscle mass, and a deepened voice. They may be capable of producing sperm, but are at a higher risk of infertility. This trait is rare on its own, but fairly common when partnered with Klinefelter Syndrome. Common traits and disabilities that may co-occur include a delayed puberty, a low libido, less body/facial hair than average, low bone density, heart disease, sleep disorders, depressive disorders, anxiety disorders, and frequent headaches.
-------------------
Other Hormonal Variations
Congenital Adrenal Hyperplasia (CAH): A variation in which an individual has adrenal glands that produce low levels of cortisol and/or aldosterone, and as a result, produce extra androgens to make up for it (leading to hyperandrogenism.) Classic CAH is when the symptoms are obvious at infancy, while Nonclassic CAH is when the symptoms occur in later childhood/teen years or adulthood. Classic CAH can be simple-virilizing or salt-wasting. Simple-virilizing CAH is when the aldosterone levels are low, but not dangerous. Salt-wasting CAH is when the aldosterone levels are too low to regulate the salt within the blood, leading to high levels of salt in the urine, which will need supplements and medications to manage. If people with salt-wasting CAH don't get treatment, it can result in low blood sugar, high levels of acid in the blood, dehydration, vomiting, diarrhea, irregular heartbeat, shock, coma, and death. Classic CAH has both an XX form and an XY form. Those with the XX form of classic CAH have XX chromosomes, a vulva (possibly with vaginal hypoplasia or a urogenital sinus anomaly) or ambiguous genitals, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as their main sex hormone and will likely develop breasts and widened hips, with the possibility of increased body/facial hair, higher muscle mass, and a deepened voice. Their menstruation may be irregular. Pregnancy is possible, however they are at a higher risk of infertility. Those with the XY form of Classic CAH have XY chromosomes, a penis (possibly a macropenis) two testicles (possibly with macroorchidism), and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though it will be high) and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice. They may be capable of producing sperm, but are at a higher risk of infertility. Nonclassic CAH has both an XX and an XY form as well. Those with the XX form of nonclassic CAH have XX chromosomes, a vulva (though it may develop into clitoromegaly), two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as their main sex hormone and will likely develop breasts and widened hips, with the possibility of increased body/facial hair, higher muscle mass, and a deepened voice. They might also develop PCOS. Their menstruation may be irregular. Pregnancy is possible, however they are at a higher risk of infertility. Those with the XY form of Nonclassic CAH have XY chromosomes, a penis, two testicles , and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though it will be high) and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice. They may be capable of producing sperm, but are at a higher risk of infertility. Classic CAH is rare. Nonclassic CAH is extremely common, occurring in 1 of every 200-1,000 births. Common traits and disabilities that may co-occur with all forms of CAH include an early puberty (which may lead to a shorter height than average), oily skin, and higher levels of acne.
-
Leydig Cell Hypoplasia (LCH): A variation in which an individual with XY chromosomes is born with testicles (possibly with microorchidism or cryptorchidism), which has underdeveloped or absent leydig cells, resulting in hypoandrogenism and delayed or absent puberty. They have a penis or micropenis (possibly with hypospadias), bifid scrotum, or a vulva. They also have a prostate. If they start puberty naturally (and don't use HRT), they will have testosterone as the main sex hormone (though it will be low), and have the possibility of developing increased body/facial hair, higher muscle mass, and a deepened voice. They may be capable of producing sperm, but are at a higher risk of infertility (and if a vulva is present, the semen may have no way to exit, depending on how the testes are connected to the genitals.) This variation is extremely rare. Common traits and disabilities that may co-occur include a taller height than average, low bone density, and delayed or absent bone maturation.
-
17-Ketosteroid Reductase Deficiency (17 KSR Deficiency): A variation in which an individual with XY chromosomes has a genetic mutation that causes the hormone androstenedione not to convert into testosterone as frequently as it does within males, resulting in hypoandrogenism. They have a penis or micropenis (possibly with hypospadias), ambiguous genitals, or a vulva (though it may develop into clitoromegaly). They also have two testicles (possibly with microorchidism or cryptorchidism) and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though it will be high) and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice, with the possibility of breast growth. They may be capable of producing sperm, but are at a higher risk of infertility (and if a vulva is present, the semen may have no way to exit, depending on how the testes are connected to the genitals.) This variation is rare.
-
5α-Reductase 2 Deficiency (5αR2D)/Pseudovaginal Perineoscrotal Hypospadias/PPSH: A variation in which an individual with XY chromosomes has a genetic mutation that causes a lower production of dihydrotestosterone compared to males, resulting in hypoandrogenism. They have a penis or micropenis (possibly with hypospadias), ambiguous genitals, or a vulva (though it may develop into clitoromegaly.) They also have two testicles (possibly with cryptorchidism) and a prostate (possibly with prostate hypoplasia.) During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though it will be high) and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice. They may be capable of producing sperm, but are at a higher risk of infertility (and if a vulva is present, the semen may have no way to exit, depending on how the testes are connected to the genitals.) This variation is rare.
-
Aromatase Deficiency: A variation in which an individual's body is incapable of converting androgens into estrogen, resulting in hyperandrogenism and hypoestrogenism. This begins during fetal development, and comes in both an XX form and an XY form. Those with the XX form have XX chromosomes, a clitorophallus or fused labia, two ovaries (possibly hypoplastic ovaries), and a uterus (though menstruation does not occur.) During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though it will be high), and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice. Those with the XY form of aromatase deficiency have XY chromosomes, a penis, two testicles (possibly with microorchidism or cryptorchidism), and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though it will be high) and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice. This variation is extremely rare. Due to the rarity, little is known about the fertility status. Common traits and disabilities that may co-occur include patches of darker/lighter skin, a taller height than average, low bone density, long limbs, inturned knees, high blood sugar, type 2 diabetes, weight gain, and a fatty liver. A person who is pregnant with a baby that has aromatase deficiency will get secondary effects of the androgens from the fetus within them. They may develop phallus growth, increased body/facial hair, and a deepened voice. These changes typically end once the baby is born.
-
Estrogen Insensitivity Syndrome (EIS)/Estrogen Resistance: A variation in which an individual's estrogen receptors do not respond to estrogen being produced. The estrogen is present, but the body is not fully using it. This may result in high levels of estrogen in the blood (due to estrogen being unused and building up), with the body only using minimal amounts of it. This comes in both an XX and an XY form. Those with the XX form have XX chromosomes, a vulva, two ovaries, and a uterus (possibly with uterine hypoplasia.) Menstruation is absent or irregular. They may also have hyperandrogenism and experience ovarian cysts. During puberty (without the influence of HRT), if they don't have hyperandrogenism, then they will have estrogen as the main sex hormone, however it will have very little effect on their physical development. If they have hyperandrogenism, then testosterone will be their main sex hormone (or even just equal to estrogen, though the estrogen is being unused), however its effects will be minimal, likely only resulting in severe acne and pubic hair. Those with the XY form have XY chromosomes, a penis, two testicles (possibly with microorchidism or cryptorchidism), and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone, and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice. This variation is extremely rare. Due to the rarity, little is known about the fertility status, though it seems there's a higher risk of infertility. Common traits and disabilities that may co-occur include a delayed puberty, a taller height than average, and low bone density.
-
Androgen Insensitivity Syndrome (AIS)/Androgen Resistance: A variation in which an individual with XY chromosomes has androgen receptors that do not respond to androgens being produced. The androgens are present, but the body is not fully using it. This may result in high levels of estrogen in the blood (due to estrogen being unused and building up), with the body only using minimal amounts of it. This comes in 3 forms - mild, partial, and complete. Those with Mild Androgen Insensitivity Syndrome (MAIS) have a body that is only mildly unresponsive to androgens, meaning that most of it is still in use. They have a penis (possibly with hypospadias), two testicles, and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone, and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice. They may be capable of producing semen, but are at a higher risk of infertility. Those with Partial Androgen Insensitivity Syndrome (PAIS) have a body that is partially unresponsive to androgens, meaning that a significant amount of it is not in use. They have a penis or micropenis (possibly with chordee or hypospadias), ambiguous genitals, or a vulva with a urogenital sinus anomaly. They have two testicles (possibly with cryptorchidism), and may have a prostate (possibly with prostate hypoplasia) or no prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone, and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice, with the possibility of breast growth and widened hips. They may be capable of producing sperm, but are at a higher risk of infertility (and if they lack a prostate, the sperm will be incapable of leaving, and thus medical intervention to extract the sperm would be necessary in order to create a biological offspring.) Those with Complete Androgen Insensitivity Syndrome (CAIS) have a body that is completely unresponsive to androgens. They have a vulva (possibly with vaginal hypoplasia, labial hypoplasia, and clitoral hypoplasia,) and two testicles with cryptorchidism. They have no prostate and no uterus. During puberty (without the influence of HRT), they will have estrogen as their main sex hormone, and will likely develop breasts and widened hips. They are infertile. All forms AIS are rare. Common traits and disabilities that may co-occur include a taller height than average, large teeth, dry skin, drier eyes than typical, light sensitivity in the eyes, and dry hair.
-
Chromosomal Variations
These are variations affect a person's chromosomes.
Swyer Syndrome/XY Gonadal Dysgenesis: A variation in which an individual has XY chromosomes, but due to a genetic mutation, they develop a CTF appearance. They have a vulva or clitoromegaly, a uterus (possibly with uterus hypoplasia), and two streak ovaries. They will not begin puberty unless they are on HRT. Due to the streak ovaries, they are infertile, however if their uterus is large enough, they can carry a (genetically unrelated) embryo if it is medically implanted. This variation is rare. A common trait/disability that may co-occur is low bone density.
-
Mixed Gonadal Dysgenesis (MGD)/45X-46XY Mosaicism: A variation in which an individual is born with some cells having X chromosomes, and other cells having XY chromosomes. This comes in two forms. Those with the first form have a vulva (possibly with a urogenital sinus anomaly or vaginal aplasia) or ambiguous genitals and ovaries (though one or both will be streak ovaries). They may in some cases have a uterus. If both of their gonads are streak ovaries, they will not start puberty without HRT. If they start puberty naturally (and don't use HRT), they will have estrogen as the main sex hormone (though hypoestrogenism is common, meaning their estrogen levels may be low), and will likely develop breasts and widened hips. If they have a non-streak ovary, but no uterus, their eggs can create an embryo to be implanted into another carrier. If they have two streak ovaries, but have a uterus, then they can carry a (genetically unrelated) embryo if it is medically implanted. If they have two streak ovaries, and no uterus, then they are infertile. Those with the second form have a penis/micropenis or ambiguous genitals, testicles (though one or both will be streak), and a prostate (possibly with prostate hypoplasia). If both of their gonads are streak testes, they will not start puberty without HRT. If they start puberty naturally (and don't use HRT), they will have testosterone as the main sex hormone (though hypoandrogenism is common, meaning their testosterone levels may be low), and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice. If they have a non-streak testicle, they can produce semen - though, if they also have prostate hypoplasia, they are at a higher risk of infertility. If both of their testes are streak, then they are infertile. This variation is rare.
-
XX-XY Chimerism/46, XX-46 XY Chimerism/XX-XY Mosaicism: A variation in which an individual is born with some cells that have XX chromosomes, and some cells that have XY chromosomes. Those with this variation could have a vulva (possibly with vaginal hypoplasia), a penis/micropenis, or ambiguous genitals. They may have hypospadias, epispadias, or a urogenital sinus anomaly. They can have any of the three gonad types (ovaries, testes, or ovotestes), however in some cases their gonads may also be streak. and may have a prostate, uterus, or both. If they have streak gonads, their puberty may be absent or delayed. If they start puberty naturally, their main sex hormone depends on what their gonads produce more of. They may produce estrogen as their main sex hormone (leading to breast growth and widened hips), androgens as their main sex hormones (leading to increased body/facial hair, higher muscle mass, and a deepened voice,) or a mixture of both - however, hypogonadism is common if they have streak gonads. If they have streak gonads, their fertility may be decreased or (if both gonads are fully streaked) they may be infertile. If they only have non-streak gonads, they may be capable of producing eggs (if they have ovaries or ovotestes) or sperm (if they have testes or ovotestes.) If they produce eggs but have no uterus, than the eggs will need to be extracted in order to create an embryo. If they produce sperm but have ambiguous genitals or a vulva, it may not be capable of being released, depending on how it connects to the genitals, and may need to be extracted in order to create an embryo. If they produce sperm but have a uterus, an embryo implant can be done if they wish to carry a baby. This variation is extremely rare. Common traits & disabilities that may co-occur include asymmetrical features (ie; an asymmetrical face), heterochromia (different colored eyes), and vitiligo.
-
XYY Syndrome/Jacob's Syndrome: A variation in which an individual is born with XYY chromosomes. They have a penis/micropenis (possibly with hypospadias), two testicles (possibly with macroorchidism or cryptorchidism), and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though hypoandrogenism or hyperandrogenism is common, so their testosterone may be high or low), and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice. They may be capable of producing semen, but are at a higher risk of infertility. This variation is fairly common, occurring in 1 of every 1,000 AMAB births. Common traits and disabilities that may co-occur include being taller than average, hypotonia, flat feet, abnormal feet patterns, asthma, a large head, low-set ears, flattened cheekbones, dental abnormalities, widely-spaced eyes, night-blindness, tic disorders, seizure disorders, neurodevelopmental disabilities, learning disabilities, and communication disabilities.
-
XYYY Syndrome: A variation in which an individual is born with XYYY chromosomes. They have a penis, two testicles, and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though hypoandrogenism is common, so their testosterone may be low), and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice. This variation is extremely rare. Due to the rarity, little is known about the fertility status, though it seems there's a higher risk of infertility. Common traits and disabilities that may co-occur include being taller than average, hypotonia, fused forearm bones, incurved fingers/toes, radial head dislocation, a short neck, dental abnormalities, a thick lower lip, a flat bridge of the nose, a longer space between the upper lip and nose, folded eyelids, widely spaced eyes, higher levels of acne, and intellectual disability.
-
XYYYY Syndrome: A variation in which an individual is born with XYYYY chromosomes. They have a penis, two testicles, and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though hypoandrogenism is common, so their testosterone may be low), and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice. This variation is extremely rare. Due to the rarity, little is known about the fertility status, though it seems there's a higher risk of infertility. Common traits and disabilities that may co-occur include fused forearm bones, an incurved pinkie finger, facial asymmetry, a smaller than typical jaw, widely-spaced eyes, low set ears, hypertelorism, neurodevelopmental disabilities, and communication disabilities.
-
XXYYY Syndrome: A variation in which an individual is born with XXYYY chromosomes. They have a penis, two testicles, and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone, and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice. This variation is extremely rare. Due to the rarity, little is known about the fertility status. Common traits and disabilities that may co-occur include delayed bone development, abnormal facial features, a small head, and intellectual disability.
-
XXXYY Syndrome: A variation in which an individual is born with XXXYY chromosomes. They have a penis/micropenis or ambiguous genitals, two testicles (possibly with microorchidism or cryptorchidism), and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though hypoandrogenism is common, so their testosterone may be low), and will likely develop breasts and widened hips. This variation is extremely rare. Due to the rarity, little is known about the fertility status. Common traits and disabilities that may co-occur include being taller than average, delayed bone development, twisted feet, abnormal feet patterns, long legs, long arms, incurved fingers, a slim or underweight body, frequent upper respiratory infections, a narrow chest, a prominent jaw, a small jaw, a wide bridge of the nose, widely spaced eyes, folded eyelids, a prominent forehead, an abnormal face shape, low-set rotated ears, neurodevelopmental disabilities, communication disabilities, and behavioral disorders.
-
XXYY Syndrome: A variation in which an individual is born with XXYY chromosomes. They have a penis or micropenis, two testicles (possibly with microorchidism or cryptorchidism), and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though hypoandrogenism is common, so their testosterone may be low), and will likely develop increased body/facial hair, higher muscle mass, a deepened voice, breast growth, and widened hips. They may be capable of producing semen, but are at a higher risk of infertility. This variation is rare. Common traits and disabilities that may co-occur include being taller than average, hypotonia, hyperflexible joints, flat feet, hip dislocation, inguinal hernias, cardiovascular abnormalities, gastrointestinal disabilities, weight gain , asthma, apnea, frequent upper respiratory tract infections, lymphatic cancer, scoliosis, an incurved pinkie finger, elbow dislocation, fused forearm bones, shoulder abnormalities, a flat back of the skull, a long face, facial asymmetry, a broad jaw, dental abnormalities, a cleft lip, a thick lower lip, widely spaced eyes, upslanting eyelids, folded eyelids, drooping eyelids, movement disorders, neurodevelopmental disabilities, communication disabilities, depressive disorders, anxiety disorders, and psychotic disorders.
-
Klinefelter Syndrome/XXY Syndrome: A variation in which an individual has XXY chromosomes. They have a penis or micropenis, two testicles (possibly with cryptorchidism), and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though hypoandrogenism is common, so their testosterone may be low), and will likely develop increased body/facial hair, higher muscle mass, a deepened voice, breast growth, and widened hips. They may be capable of producing semen, but are at a higher risk of infertility. This variation is extremely common, occurring in 1 of every 500 AMAB births. Common traits and disabilities that may co-occur include a low libido, being taller than average, weak bones, hypotonia, breast cancer, increased body fat, type 2 diabetes, cardiovascular abnormalities, autoimmune disorders, lung disease, narrow shoulders, dental abnormalities, neurodevelopmental disabilities, communication disabilities, learning disabilities, behavioral disorders, depressive disorders, and anxiety disorders.
-
XXXY Syndrome: A variation in which an individual is born with XXXY chromosomes. They have a penis or micropenis, two testicles (possibly with microorchidism or cryptorchidism), and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though hypoandrogenism is common, so their testosterone may be low), and will likely develop increased body/facial hair, higher muscle mass, a deepened voice, breast growth, and widened hips. They may be capable of producing semen, but are at a higher risk of infertility. This variation is rare. Common traits and disabilities that may co-occur include being taller than average, hypotonia, hyperflexible joints, abnormal shaping at the end of bones, flat feet, twisted feet, hip dislocation, abnormally angled hips, an underdeveloped kidney, inguinal hernias, gastrointestinal disabilities, increased body fat, frequent respiratory tract infections, asthma, cardiovascular abnormalities, scoliosis, elbow dislocation, fused forearm bones, an incurved pinkie finger, low-set sloped shoulders, a short neck, a flat back of the skull, dental abnormalities, a large jaw, a cleft palate, facial asymmetry, a flat bridge of the nose, widely-spaced eyes, upslanting eyelids, folded eyelids, drooping eyelids, crossed eyes, frequent ear infections, tremors, seizure disorders, neurodevelopmental disabilities, communication disabilities, anxiety disorders, and psychotic disorders.
-
XXXXY Syndrome: A variation in which an individual has XXXXY chromosomes. They have a penis or micropenis, two testicles (possibly with microorchidism or cryptorchidism), and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though hypoandrogenism is common, so their testosterone may be low), and will likely develop increased body/facial hair, higher muscle mass, a deepened voice, breast growth, and widened hips. They are infertile. This variation is extremely rare. Common traits and disabilities that may co-occur include being shorter than average, hypotonia, hyperflexible joints, abnormal shaping for the end of the bones, flat feet, a twisted foot, abnormally angled hips, hip dislocation, an absent or underdeveloped kidney, cardiovascular abnormalities, gastrointestinal disabilities, asthma, frequent respiratory infections, scoliosis, an incurved pinkie finger, fused forearm bones, low-set sloped shoulders, a short neck, a flat back of the skull, a prominent jaw, dental abnormalities, a cleft palate, a wide nose, a flat nose, absent olfactory bulbs (resulting in an inability to smell), upslanted eyelids, drooping eyelids, widely spaced eyes, crossed eyes, near-sightedness, frequent ear infections, tremors, seizure disorders, neurodevelopmental disabilities, and communication disabilities.
-
XXXXX Syndrome/Pentasomy X: A variation in which an individual has XXXXX chromosomes. They have a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. This variation is extremely rare. Due to the rarity, little is known about the fertility status, however it appears to be average. Common traits and disabilities that may co-occur include delayed puberty, being shorter than average, short feet, hip dislocation, immune system disorders, cardiovascular abnormalities, a small head, a flat back of the head, a small lower jaw, a flat front face, dental abnormalities, a wide nasal bridge, upslanted eyelids, widely spaced eyes, crossed eyes, low-set rotated ears, and intellectual disability.
-
XXXX Syndrome/Tetrasomy X: A variation in which an individual has XXXX chromosomes. They have a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Their menstruation may be irregular. Pregnancy is possible, however they are at a higher risk of infertility and early menopause. This variation is extremely rare. Common traits and disabilities that may co-occur include delayed puberty, hypotonia, hyperflexible joints, hip dislocation, kidney disorders, bladder disabilities, immune system abnormalities, autoimmune disorders, cardiovascular abnormalities, short fingers/toes, an incurved pinkie finger, dental abnormalities, widely spaced eyes, upslanting eyelids, crossed eyes, seizure disorders, learning disabilities, and communication disabilities.
-
Triple X Syndrome/Trisomy X/XXX Syndrome: A variation in which an individual has XXX chromosomes. They have a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Their menstruation may be irregular. Pregnancy is possible, however they are at a higher risk of infertility and early menopause. This variation is fairly common, occurring in 1 of every 1,000 AFAB births. Common traits and disabilities that may co-occur include delayed puberty, being taller than average, hypotonia, hyperflexible joints, flat feet, an absent or underdeveloped kidney, kidney defects, frequent urinary tract infections, autoimmune disorders, a caved-in chest, fused forearm bones, incurved fingers, widely-spaced eyes, folded eyelids, drooping eyelids, tremors, seizure disorders, neurodevelopmental disabilities, communication disabilities, learning disorders, mood disorders, anxiety disorders, and psychotic disorders.
-
SERKAL Syndrome: A variation in which an individual has XX chromosomes, but due to a genetic mutation in the WNT4 gene, they develop a CTM appearance. They have a penis or micropenis (possibly with hypospadias or penoscrotal transposition), two testicles or ovotestes (possibly with cryptorchidism), and a prostate. This variation is extremely rare. There is no information on fertility or puberty, as the only three recorded cases of this variation were terminated as fetuses. Common traits and disabilities that may co-occur include a small/underdeveloped bladder, an absent kidney, adrenal abnormalities, non-coiled intestines, small/underdeveloped lungs, heart abnormalities, a diaphragmatic hernia, and an oral cleft.
-
XX Male Syndrome/De La Chapelle Syndrome: A variation in which an individual has XX chromosomes, but due to one of their X chromosomes containing an SRY gene, they develop a CTM appearance. They have a penis/micropenis (possibly with hypospadias) or ambiguous genitals, two testicles (possibly with microorchidism or cryptorchidism), and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though hypoandrogenism is common, so their testosterone may be low), and will likely develop increased body/facial hair, higher muscle mass, a deepened voice, breast growth, and widened hips. They are infertile. This variation is rare. Common traits and disabilities that may co-occur include a shorter height than average and a low libido.
-
Turner Syndrome/Monosomy X: A variation in which an individual has only one X chromosome and no Y chromosome (0X.) They have a vulva, ovaries (usually hypoplastic ovaries or streak ovaries), and a uterus. Mosaic Turner Syndrome is a type of Turner syndrome where some cells have 0X chromosomes, and other cells have XX chromosomes. Puberty may be absent or delayed. If they start puberty naturally (and don't use HRT), they will have estrogen as the main sex hormone (though hypoestrogenism is common, so their estrogen may be low), and will likely develop breasts and widened hips. If one of their ovaries is non-streak, then pregnancy is possible, however they are at a higher risk of infertility and early menopause. If they have two streak ovaries, then they can carry a (genetically unrelated) embryo if it is medically implanted. This variation is fairly common, occurring in 1 of every 2,500 AFAB births. Common traits and disabilities that may co-occur include a delayed puberty, a shorter height than average, vitiligo, moles, birthmarks, skin scarring, low bone density, outturned forearms, nail abnormalities, abnormal feet/hand patterns, flat feet, flexible toe joints, short toes, splayed toes, abnormal shape for the end of the tibia bones, inturned knees, enlarged outer thighbones, hip dislocation, an absent or underdeveloped kidney, fused kidneys, abnormally located kidneys, increased body fat, liver defects, heart defects, autoimmune disorders, thyroid gland inflammation, cystic hygroma, scoliosis, a hunched back, a short sternum, a wide rib cage, a caved-in chest, a broad chest, a broad neck, a webbed neck, a short neck, a low hairline on the back of the head, a small/underdeveloped or absent lower jaw, dental abnormalities, drooping eyelids, folded eyelids, crossed eyes, near-sightedness, prominent ears, frequent ear infections, hearing disabilities, neurodevelopmental disabilities, communication disabilities, depressive disorders, anxiety disorders, and psychotic disorders.
_______________________________________________________
_______________________________________________________
_______________________________________________________
And thats all!
Again, please reblog to spread awareness. Intersex people are highly discriminated against. Their bodies are still regularly mutilated at birth or during puberty, and they are still forced into HRT, in order to make them "look right" or "function right."
This medical abuse can cause complete infertility, a loss of sensation in genital areas (making sex unsatisfactory), chronic pain, gender or sex incongruence, and body dysmorphia.
Additionally, intersex children are often bullied at school for looking or sounding "abnormal" for their age/gender. And as they grow up, they face the same difficulties transgender individuals do - judgement for not being a "real man" or "real woman" (or for being non-binary), difficulty dating, struggles finding jobs, complications in receiving proper healthcare, and they are at an increased risk of being abused and assaulted. Many are also left out of sports or kicked out of public bathrooms as well.
This is all due to the lack of education. Tolerance and acceptance needs to be taught to children. Many doctors have no idea how to treat intersex patients, as they didn't learn about their bodies, even in advanced schooling. We need to put a stop to this.
#intersex#intersex spectrum#queer#lgbt#lgbtq#lgbtqia#lgbtqia+#education#educate yourself#educate yourselves#pride month#lgbt pride#happy pride 🌈#queer pride#body diversity#diversity#information#informative#chromosomes#hormones#hormonalhealth#genitals#reproductive rights#reproductive health#representation#reproductive justice#intersex awareness#intersex pride#intersex issues#intersex community
530 notes
·
View notes
Note
hihi, Prince! I noticed your "not okays" list had age regression listed in with DDLG?
those're not remotely similar, and I realize it's an easy mistake to make!
age regression is a symptom of PTSD. I think the term you're looking for is "age play?"
I don't mean to be disrespectful or anything! I just thought that this may have been a misunderstanding, because I saw your version of Shadow as someone experiencing age regression, so I was super confused when I saw that, because there's nothing wrong with age regression.
love your art lots! 💗
Hello!
First; you did not come off disrespectful in anyway! I should have clarified in its own section why I have age regression on there. For that I do apologize.
I do know the difference between age play and age regression. I understand Age play is the sexual act of someone act like a minor/baby. This is very much not okay.
Age Regression is indeed a symptom of PTSD and something used for those on the spectrum. With this being said the main reason I have this on the “not okays” list. Is due to the fact that may inappropriate messages were being sent over my way with the topic of Age Regression/Age Play/DDLG. I am just not comfortable with those topics being tossed onto me.
I have no issues with people who use age regression to cope, or view my art that way. Truly, I just want everyone to be happy. With this being said, it’s important for me to also be happy.
I do not want to interact with age regression. I hope many people are okay with this. Nothing will change in terms of my content or how I interact with others. It’s just something that others ruined and now I feel uncomfortable about.
I hope my message doesn’t come across as mean or rude. I truly hope people continue to find comfort and see themselves in my art. If people are interpreting it as age regression and you feel seen, that is okay! Just please do not force those concepts at me. If something in this message doesn’t make sense, just ask. I’m happy to clarify.
I’ll update my “About me” when I can.
Just to recap, age regression is not a bad thing, bad people just ruined that concept for me.
I appreciate you anon! I don’t mind having conversations like this and being open about my thoughts process
#prince rambles#i truly was rambling im sorry#just thought it was best to clarify now#love you anon#!!
39 notes
·
View notes
Text
We're In This Together: A Post of Pairs & Connection in Alters
This topic's not commonly talked about, since we always thought that alters have to be different in order to be a valid experience as a system. I've come here to show you another perspective to tackle that Status Quo:
Alter's are connected with each other--sometimes obvious like in pairs, sometimes subtle ways on how they communicate to other groups better.
It'll be an interesting subject today--I'll Show ya!
Fast Pass: TLDR Section Is Available!
Alright, Im Listenin'
We've had many discussions within the community on why parts are compartmentalized, became distinct personalities, or able to hold different memories/symptoms/skills. Now, that's one view systems often focus on,, this's the time to talk about what's been keeping your innerworld and parts functional in real life despite the chaos.
Do you often think to yourself why parts come in pairs or many at once instead of one by one in a gradual timeline?
While there's no single factor that helps make sense of this, there ARE some primary ones:
Low Dissociation It's what helps them understand each other's thoughts without saying them out loud, since they vibe with similar frequencies.
Low Emotional Amnesia This helps them understand what the other is feeling, no matter how small, its like some integrated empathy that's mutually shared.
Splitting from the same Source (alter) While it's true that the essence were distributed away, some retain the original part, which often makes those separated alters gravitate towards each other again. Sometimes they also remember where or who they belonged to, retaining past memories is absolutely possible.
Arriving from similar origins They can appear one after the other (in short time span) or alternatively, appear together in a group. This can be caused by changes in the environment/daily life, which brings forth newer equipped alters if existing parts fail to integrate/download the updates.
Is this,, Normal?
It sure is, and there's reasons to back those up.
Similarities can be shared across alters due to how amnesia and dissociative barriers affect each alters differently, this can be compared with two extreme spectrums:
The OSDD 1a is subtype where amnesia and barriers are still prominent, yet the lack of distinction brings us some hints that alters do not have to be different in order to be separate.
And the Polyfrag can have multiple variations of a single alter, contrasting with OSDD's less distinct but separate parts. This suggests different forms of interconnection--meaning, alters are linked through shared origins, functions, or retained traits rather than always being fully different personalities.
Those with DID or other CDD's can also experience this, just in less obvious forms outside of my examples. Depending on what type of system you are, this experience will manifest differently for everyone, and is not universal or comparable.
If you're still confused why an alter split or formed here and there, then it might be harder to understand why groups can appear--In this case, i'll explain the basics to help you understand why.
Tell Me Why?
It's possible to split or form alters that have similar skills, traits, or purposes since the brain do not possess an innate sorting system based on aesthetics or clear organization to box each parts differently.
When you think about it, the brain is geared for survival and producing resources based on what obstacles it had encountered--think about how sharing workload provides better stress resilience when compared to a single part handling all the burden, a big contrast isn't it?
An alter who forms or splits from, is the cause of stress from uncertainty or any complex issues it cannot navigate/solve. It's much easier to simplify solutions to black and white, leaving the grey areas untouched,, this helps them perform actions immediately without overthinking any other perspectives.
Now, if they came in groups, it got the same reason why one appeared,, but now a level above it. There could be multiple stress at once which produces a batch in a similar time frame.
What does their Arrival mean?
If there's an ongoing theme or when the majority have one or multiple traits or issues it's dealing with (e.g, most of your headmates struggles with trust) , that could be a BIG hint that something is up.
You can also call it a reoccurring problem that's desperate to be solved, something that you're uncomfortable to face--yet crucial to heal from.
And, from the alters you've gained throughout your journey, it reflects what stress or trauma that needs to be overcame one day. So.. instead of dreading why you've gained new members, try using a different mindset and ask what do you need in order to cope,, assuming new ones arrived to help you get through life.
How's this related to our topic--
It does relate for today's main subject, because of how some alters talk, and often create their own social groups based on how well they connect with each other.
See for instance, holders can have better access to other holder's memories or how ANP's can talk better with their own similarities compared to talking to EP's groups. Depending on what the alter's dissociated away from, the less distinct, the better they're related to each other.
E.g, A and B are both anger holders, despite having different memories to why they adapted an explosive behavior, the dissociation between them aren't high due to holding the same emotion--Anger. This main similarity between them is what creates better inner communication.
So, its true that alters are all different, although because they belong to the same mind--it's bound to collide and create similar variations from external environment or stimulus.
Okay, i understand! (Takeaway)
That's great, because even if CDD's are made to separate stressful memories or traumas, it does not stop from parts being able to communicate due to their own connected origins which bypass the general amnesia and barriers all systems struggle with!
At the end, to simply explain why connection exists within dissociation, its definitely because of one word: Relation.
Dissociation and amnesia makes it hard to be aware of your own parts or their purpose, but if you got some common grounds to start a conversation--it'll serve as a realization that you're not as separated from everyone else as you'd thought.
Have i challenged the Status Quo? If this made you rethink how alters connect, you might find subsystems even more interesting, here's the link to it!
- c
TLDR SECTION
Alters don’t always exist as completely distinct individuals—many are interconnected in ways that challenge the common perception of system dynamics.
Some alters form in pairs or groups, sharing traits, emotions, or origins. This happens due to factors like low dissociation, low emotional amnesia, splitting from the same source, or arriving from similar life circumstances.
Polyfragmented systems can have multiple variations of a single alter, contrasting with OSDD’s less distinct but still separate parts. This suggests that alters can be linked through shared origins, functions, or retained traits rather than always being fully different personalities.
Alters arriving in groups often reflect recurring stress or trauma, signaling unresolved issues that need attention. Instead of seeing new alters as a setback, they can be understood as adaptations meant to help the system navigate challenges.
Key takeaway: Despite dissociation and amnesia, alters are often connected in ways that make inner communication and cooperation possible. Recognizing this can help systems better understand and communicate with themselves.
#did#actually did#did community#did osdd#did system#dissociative identity disorder#sysblr#plural#jeducates
32 notes
·
View notes
Text
Okay, getting my Asexual-spectrum Batman brainrot in some sort of order, everything is subject to being updated.
This turned out long and rambling, just the way I like it.
My main inspiration for this is a scene from the Christopher Nolan Batman trilogy, where Bruce and Alfred are discussing how to reintroduce Bruce into Gotham society. It's been awhile since I saw the film but I'm pretty sure Bruce looks at Alfred and is like, "So, what do young billionaires do that would explain vigilante injuries?" And then the scene cuts to Bruce and two foreign models swimming in a fountain at a fancy restaurant. And I'm like.
Fucking. Alfred. Suggested the himbo thing? Was this a passive-aggressive punishment for fucking off for years that went on for too long?
(I love my main man Mr. Pennyworth, I will meme that he's a saint. In reality, I think he's part of the reason the Robins keep having a terrible time passing on the mantle. I can address my grievances in another post tho.)
So I'm there, thinking about Batman and Bruce and growing up in private schools. I'm in the process of unlearning some damaging information that I was taught as "truth" from my own school days. I'm thinking of Butler Alfred, and his position as caretaker, and how he was raised, and what he would think is appropriate counsel.
When Bruce is hitting puberty and writing love poems to the tune of BeeGees songs to girls in class, how would Alfred handle that? He'd surely have a perfunctory talk with his charge about respecting women, how to be a proper gentleman, safe sex, warnings about people who are out for Bruce's heart as a way to get to his status and fortune.
But would Alfred even think to cover queerness? He surely knows of it, but he's from a generation and culture that is known for stoicism and silence. The generation where one might know a pair of "confirmed bachelors" or "spinster sisters", but one does not mention it in polite company. Perhaps he would decide to have that talk if it ever seems to be necessary.
But would Bruce ever think to ask about why he isn't as interested in sex as seemingly all the people around him? Why wouldn't he chalk that up to his massive trauma and call himself mature for it? And a number of girls would love that maturity, that Ice Prince gentility, that challenge. So he'd learn how to be charming, how to flirt. It's applied psychology to Bruce, it's masking, it's learning how to act like a "normal" human.
It's easy for me to see him continue that trend in his adult life. He is romantic and he isn't sex-repulsed; he matches the flirtation energy of someone and if they both want to have sex, they do. It's kind of fun for him, too, to learn someone's body and use his to make them feel so good.
It's just that, sex is just a mutual workout? And he legitimately enjoys doing other things together equally or more, like actual workouts or sparring or casework. Bruce will initiate sex if he picks up his partner's cues, but by the time he's comfortable enough with them to relax... He's just not in clue-finding mode. So partners become understandably annoyed. Upset. They feel like they're the ones putting in all the effort to keep the relationship alive and Bruce doesn't have the knowledge or words to explain his position.
So yeah, there are jokes about Batman being easy, jokes about his history of romantic relationships with rogues, civilians, and heroes alike. He's just doing what he thought was normal. Flirting back, following the other person's lead, matching the energy. It frustrates him when he thinks about it, because it's just another way he's Different and Broken and Missing Something that the rest of the world seems to understand on a basic level.
(To be firm: Bruce Does Not Match the energy of everyone who flirts with him. He is an adult and has his own tastes. He's got Polite Flirting, Interested Flirting, and Gray Rocking down pat.)
#dc comics#dcu#dc universe#batman#headcanon#bruce wayne#asexual Bruce Wayne#asexual Batman#ramblings#really hoping i don't upset anyone with this#trying to use my words to explain a complex concept#it's terrible#why can't we just emote#idk ask me questions#add your thoughts#I'd love to hear them
24 notes
·
View notes