#Causes of Substance Abuse in Adolescence
Text
#How to Reduce Substance Abuse in Youth#How to Stop Substance Abuse in Youth#Most Common Substance Abuse in Adolescence#Causes of Substance Abuse in Adolescence#What Causes Substance Abuse in Youth#Risk Factors for Substance Abuse in Adults#Solutions of Drug Abuse#Ways of Preventing Drug Abuse#Drug Addiction Treatment in Patna#Nasha Mukti Kendra in Patna
0 notes
Text

I knew it was destiny for me to do a coraline themed pac. Enjoy! 💗
Paid Readings | Patreon | Tip Jar




Pile One
From your inner teen's perspective, your costume is an eclipse that covers your range and your capacity to move on to the next phase of developing your sense of self and what you'd like to accomplish. Your costume could be like a zombie or in general, someone who isn't in control of their body or thoughts. If you have any anger that you feel at times that you may consider random, this could be your inner teen's frustration over how you have tendencies of not having a grip on your self awareness and identity. You could depend too much on how you're being perceived by others or their approval or maybe there's this substance or tool that you use to help morph yourself into someone different to appease on what people in your environment may think is appropriate. I keep thinking about acid and other hallucinogens, if I'm correct, no trip is supposed to be the same as the previous or next trip. So when I think about this energy that I'm picking up in this pile, you constantly manipulate yourself in order to stay the same in hopes of receiving the same reaction from others. It's like reinforcement, where you get some sort of gratification, but is bringing to yourself in some way. Examples that I'm channeling includes but not limited to overacheiving to the point where nothing satisfies you, being in a back and forth connection by doing things that gets the other person to chase after you, and (TW ⚠️: eating disorders). This irritates your inner teen, because one of your biggest goals when you were in the age of adolescence, was to grow beyond the reach of people that made you feel low about yourself and to escape the grasp of abusive environments that constrain you and made you dream of a life where things could be better and different.
Who you are when no one is watching and behind those tears of discontent and malaise, is someone who's constantly reinventing themselves, and embraces these transitions of change. You hold yourself back in worry of how other people will think, when really you're meant to cause a shock factor. You are not normal spongebob where your emotions, thoughts, and looks are fixed to the same degree every day. You're spontaneous in a way where if you were to step outside in the world as you are, validation is no longer your drug, YOU are the drug that changes the trajectory in so many people's minds in how they view their daily routines, the careers they should go after, that new hobby that they feel drawn to, that clothing piece or new hairstyle that they feel will look good on them, new philosophies and epiphanies to the small and big things to make themselves safe in their own skin.
Pile Two
Your inner teen feels like you're still holding onto the inferiority that was felt during the time where you needed community and support the most. You could hold on too much to this title of being your own person to the point where you feel separated from society. You could see yourself as someone with an "alien" like personality where you feel that you can't really connect with others or it's hard for people to feel connected with you. You could believe in starseeds and think that you are one, and while that can be true and if you resonate with that part, there's a message here to recognize that whatever past life that you may have had, doesn't change the fact that this life that you have right now, is for you to live a human and earthly experience because you are when no one is watching behind that facade of thinking that you're someone who doesn't belong here, you indeed have attributes that you share with others, you just haven't found your people yet, but you will. However, there's a main message about knowing that everyone you meet is someone you can learn from. If you're a spiritualist and/or occultist, there's a part of your first awakening in which you joined because it either came from a place of being where it feels like you're misunderstood or you were going through strange things that only other certain people could relate. But like the character Coraline in her self-titiled movie, there's a need to appreciate the home you have more, the friends and family that you do have in your circle and to tap into that part of yourself that desires to be seen and heard by just going for it and asking for what you need, which is someone who can listen to you and understand that you do have feelings under that distant and neutral persona that you showcase. Unwind, and become more vulnerable with others with not just the things that make you human which is your feelings, but also the things that make you feel like you're otherworldly. You don't have to be a stray in this world, you can be apart of it by finding your place the more that you open your heart. Your quirky and whimsical self is not meant to be hidden and gatekeeping yourself from the world out of spite of the past, is the biggest rejection that you can face in this world. And don't withhold the knowledge that you're sitting on or neglect the student within you, that's one of the major ways you'll be able to find wholesome interactions with others.
Pile Three
"The healer heals everyone, but who heals the healer?"
The inner teen inside you could feel that you've done an amazing job with nurturing yourself and nurturing others. You exude the energy of someone with immense strength, protection, crystallized intelligence, and reliance, which could make people feel drawn for something within them that needs to be nourished, and your actions heavily reflect your presence by how you're always there in service for others and how you take care of people in your personal life and the people that you may not know as well your loved ones. Your inner teen feels that although you've generated an abundance of good karma for how you genuinely kind you are, how you're constantly available for others is tipping the scale when you could be at a point in your life where you are in need of a person that's like you. I'm sensing there's something that needs to change in order to tend to yourself more, a desire for more reciprocation, but also an urge to step away from always being the one who heals others. You want to be known and valued for other things besides what you can do for people and even if you've developed this helpful nature from having responsibilities over other people like your family members at a young age, or if it's just innate, you're exhausted from this life and could use at least a break. Who you are when no one is watching, is someone who needs to be freed from what is expected of them and to find their own peace outside of dealing with everyone's chaos. Home is being brought up so much in my mind, so you're meant to explore different avenues that could be outside of family traditions, social norms, and to leave where you grew up around, you're meant to go on adventures around the world and revel in your independence. If you want a life without becoming a parent, it's not selfish to be that way, and it's perfectly find to spread your wings away from the pressure to make certain commitments that isn't yours to have. Perhaps you're interested in a lifestyle and/or career that doesn't involve being in service for others, maybe you're realizing what your true love language is and realizing what your real expectations in a partner are. Who you are when no one is watching is someone exotically beautiful in many ways than one. You know that your heart is a plus, but soon everyone will know this too.
#divination#intuitive#psychic#pick a card#tarot#spirituality#pac#tarotblr#tarot community#the tarot community#coraline#pick a pile#pick a picture#pick a card reading#pick a pile reading#intuitive readings#intuition
296 notes
·
View notes
Text
P6 Idea : Jungles and World Trees
"Jungle" in P6 is equivalent to the palace in P5. It is an obstacle that players must pass to advance the main plot, and it is also a turning point for adding new companions. The concept of "jungle" corresponds to the saying "concrete jungle = city". Each jungle is the product of human collective subconsciousness, corresponding to the Kleshas and Three Poisons of Buddhism respectively.
Jungle of Mirrors
This is the jungle created by "Delusion (Moha)", rooted in the subconscious of young people who feel confused during adolescence, and the sport girl breaks in to save her club members. When players go deep into the jungle, they also have to rescue people trapped in the mirror. The boss of Jungle of Mirrors is named "Jabberwocky of Moha". It will temporarily disappear like a chameleon. At this time, players cannot damage it with weapons or physical attacks. Only by using skills can they force it to appear. In addition, it will summon Bandersnatch and Jubjub Bird to serve as its thugs. After Jabberwocky is defeated, it will laugh at the protagonist's futility before leading to death, because if you want to solve the problem, you must catch the mastermind behind it, otherwise this lost world will be filled with many subconscious monsters like it.
Jungle of Webs
This is the jungle created by "Hate (Dvesha)", inspired by the use of cyberbullying by prejudiced people, with spider web elements that also correspond to the computer "web". The advisor boy came here to rescue the navigator boy. As long as he joins his companions, he can rescue people trapped in spider silk.The boss of Jungle of Webs is named "Yatsukahagi of Dvesha". Players cannot directly attack its body and must break its eight legs one by one. In addition, this big spider will spin silk and give birth to spiderlings to hinder players. After Yatsukahagi is defeated, the people of Ragnarok will forcibly take the navigator boy away. From this time on, players must be mentally prepared to confront Ragnarok.
Jianmu the World Tree
Jianmu is not a jungle, but the World Tree in Chinese mythology. There are obvious differences between the World Tree and the Jungle. The World Tree is an indispensable part of Ophion like Dragon Veins, and the Jungle is produced by people's twisted subconscious and must be eradicated. Therefore, every time the player defeats a jungle boss, the jungle will follow the boss. disappeared together, but the World Tree did not. In addition to the previous statement, Jianmu is basically not much different from Separate Shangri-La. Players will still face Baize and Ragnarok.
Jungle of Birdcages
This is the jungle created by "Conceit (Mana)", which is caused by the comparison mentality between companies and people involved in consortiums. Except for replacing the air battleship with a birdcage and avoiding fights with masculine boy, the overall structure of this jungle will not be too different from Clipper of Clouds. The boss of Jungle of Birdcages is named "Vucub Caquix of Mana". Because this big bird can fly in the sky, players can only use firearms to damage its two wings before shooting it down. After Vucub Caquix falls to the ground, it will attack the player with its claws and beak. In addition, it will put its companions in a birdcage as hostages. The player must destroy the bird cage to release the companions.
Yggdrasil the World Tree
Once the player comes to the World Tree in Norse mythology, the plot will take a very obvious turn. In addition, the Ragnarok, which is opposed to the protagonist, has full home field advantage here. Yggdrasil will faithfully represent concepts from Norse mythology, for example, the guard shadows here will transform into the appearance of Norse gods.

The boss here is "Nidhogg of Raga", which is caused by people's overexploitation of nature and excessive abuse of substances. In order to prevent Nidhogg from eating the roots of this world tree, players must try to avoid damaging the roots when attacking this big worm. Nidhogg will burrow into the ground to avoid physical damage, and players must use skills to blast it out. After Nidhogg emerges from the ground, it will forcefully swallow its companions. Players must climb on its head and attack its vitals to rescue its companions.
Jungle of Witches
After the problem of Yggdrasil is solved, players will have to develop several different endings from now on. At this time, the level of community improvement of players and partners must be taken into consideration to affect the development of the ending. The first is Amalthea, she will be the most important key to the ending. If her community is raised to full, she will tell us the truth when she first enters Jungle of Witches, and will continue to accompany players to fight against the mastermind behind the scenes.
Instead, once her community is not full, she enters Jungle of Witches to fight the player, leading to a bad ending where the protagonist and Amalthea are buried in the jungle. In other words, Amalthea is the boss of Jungle of Witches. Her confusion and low self-esteem about her identity make her the only exception among the subconscious monsters, which is "Doubt (Vicikitsa)". The guard shadows here will transform into the appearance of famous demons in monotheistic religions.

In the boss battle, she will fight the player under the name "Amalthea of Vicikitsa", and her persona will change from three bugs to Heidrun. This persona will release milk to hinder the player, and the player must use skills to prevent it. After defeating Amalthea, you will enter the next round of battle. The dying Amalthea will immediately transform into "Shub-Niggurath the Elder Mother", which releases several "Spawns of The Black Goat" to serve as thugs. In addition, Shub-Niggurath will spawn previous bosses to fight players, including Jabberwocky, Yatsukahagi, Vucub Caquix and Nidhogg.
Irkalla and Primordial Sea
Once you avoid the bad ending, you'll end up here, where the mastermind (final boss) lives. Irkalla is part of the Primordial Sea, and different ending developments will still be distinguished here, but I have to give a hint and I will explain the details later.
Once players enter the interior of the Primordial Sea, it is full of organic and body horror style, and the guard shadows will become representative gods from Middle Eastern mythology.

After going deep into the base of the mastermind behind the scenes, the final boss here is Nammu. She is actually the shadow of Gaia's consciousness, just like Ophion is the persona of Gaia's consciousness. Nammu looks like an innocent girl, but in fact her nature is full of pathology and distortion, which also highlights the result of her distortion of maternal nature. The reason for her distortion is the Gaia consciousness caused by the destruction of the natural environment by humans, which has caused everything to be imbalanced. And Nammu is the side (shadow) that Gaia doesn't want to face.
After defeating Nammu, she will transform into the huge "Tiamat the Chaotic Mother" before she dies. This monster, which is like a fusion of aliens and human deformities, will derive tentacles with the appearance of Cambrian creatures on its body to fight. The names of these tentacles are Musmahhu, Basmu, Usumgallu, Ugallu, Uridimmu, Girtablullu, Umu-dabrutu, Kulullu and Lahmu.
I will stop here first, and I will find time to explain the detailed truth later, so stay tuned!
24 notes
·
View notes
Text
Adrien Agreste and Borderline Personality Disorder
DISCLAIMER: I've been a bit low on spoons this week, so I haven't gathered as much evidence as I probably could have. Also, I am but a humble student in clinical psychology. This is mainly a thought compilation for @moonieratty!
To introduce the topic, without going into it too much, personality is described by features and behavioral patterns, or traits, consistent across situations and across time. Personality disorders are therefore enduring patterns of highly maladaptive traits evaluated in personal and sociocultural context (Dozois, 2019, p. 290).
Like other disorders, personality disorders have diagnostic criteria. The DSM is used primarily for diagnosis in the US and Canada while the ICD is used more widely in Europe and other places. I'm more familiar with the DSM, but I've included a brief section on the ICD to be comprehensive. It ended up a bit longer than anticipated, so let's go below the cut. Warning for discussions of abuse, self harm, and suicide, and a brief mention of substance use.
Overview of Borderline Personality Disorder
BPD is prevalent in a small percentage of the population, about 1-2% by varying estimates, and is characterized by instability across domains of emotions, identity, interpersonal relationships, and behavior. Its onset is usually in late adolescence or early adulthood and symptoms may diminish with age, after one's thirties or forties, especially with therapeutic intervention. Along with ASPD, it has been the focus of a lot of clinical research; it is unfortunately associated with high rates of non-suicidal self-injury and suicide (APA, 2022, pp. 754–755; Dozois, 2019, pp. 308–309).
Etiological factors for BPD include both biological and environmental disturbances. Of note to our discussion is the heightened risk for BPD in cases of child abuse or neglect, as well as growing up with another family member with a serious mental health condition (NHS, 2022). It's been well established that Gabriel is emotionally neglectful if not outright abusive toward Adrien in multiple ways, so this is a clear risk factor. In addition, although I won't argue definitively for Gabriel having a psychological condition, he did keep Emilie's body in the basement, so there is clearly some kind of disturbance going on.
From a cognitive-behavioral perspective, Linehan argues that BPD stems from families who consistently invalidate childhood emotional experiences and "oversimplify the ease with which life's problems can be solved," which may cause children to learn to seek attention and communicate with others through emotional outbursts (Dozois, 2019, p. 297). This rings true for Adrien and Gabriel as well.
I have to apologize for my son, Ladybug, he's like his mother. Way too overly dramatic. (Jackady)
It doesn't seem like this is the first time Gabriel has thought this, and labeling an emotional reaction as being overly dramatic is very much invalidation of it. As for emotional outbursts, Adrien has had quite a few, mostly as Chat Noir. More on this later.
To round out this first section, attachment theory proposes a connection between poor parent-child attachments and BPD relationship difficulties. Specifically, maladaptive behavior in relationships may stem from childhood development of an anxious-ambivalent attachment style, where intense fears of abandonment interfere with a strong desire for intimacy (Dozois, 2019, p. 310). You can clearly see this in Chat Noir's relationship with Ladybug, and I'm sure other people have discussed Adrien's attachment style more in depth, but suffice to say I think this is an apt description.
Argument from DSM-5-TR
In the DSM, personality disorders are primarily diagnosed on a categorical model. There are a few general criteria which I won't be going into, but I will highlight that personality disorders are stable and pervasive, and would be diagnosed only if they were leading to significant distress or dysfunction. Adrien's mental state is not great, so the latter shouldn't be a problem, but this show does not always pay attention to consistency, so I'm going to be speculating some. Everything in this section is cited to the relevant DSM entry unless otherwise stated.
The DSM characterizes BPD with instability in relationships, self image, and affects, as well as marked impulsivity. It has no exclusion criteria, so BPD can be and frequently is comorbid with other disorders like mood disorders, PTSD, and ADHD. Of the below criteria, five need to be met in order for a diagnosis to be made.
Frantic efforts to avoid real or imagined abandonment
Hey, where're you going? . . . So you're allowed to know her true identity, but I'm not? (Syren)
You're not really replacing me with a turtle, are you? (Anansi)
A lot of people have delved into Adrien's abandonment issues, which feature most prominently in his relationship with Ladybug. His fears of being replaced result in him seeking reassurance from Ladybug, and he can lash out if he does not receive the response he hopes for. Ladybug is his world, and he wants to be hers, so anything infringing on that feels to him like a threat of being abandoned, and he does not like it very much.
Impulsive behaviors like giving up his ring can be interpreted under this lens: he can avoid abandonment by doing the abandoning first. Then it will be him leaving, and not the other way around.
I also interpret Adrien's nightmare (Le Marchand de Sable) as being a fear of being alone as much as it is a fear of being trapped.
Unstable and intense interpersonal relationships alternating between extremes of idealization and devaluation
We'll be united, more powerful and free. We'll defeat Hawk Moth, then we can both run away to an island! Far away from everything. We will live off nothing but fruits, and we will have a little pet hamster and we will name it— (Le Patineur)
I just can't do this anymore. I give up… on everything. Even you . . . If I become Chat Noir again, Ladybug will just end up rejecting me, over and over. (Kuro Neko)
Even though Adrien mostly keeps his head on straight regarding what he's owed and not owed by other people, his relationship with Ladybug is full of highs and lows. He thinks Ladybug is the most amazing girl, but this can recoil quickly into feeling as though Ladybug doesn't care about him enough or isn't meeting his needs.
Furthermore, he developed this idealization of Ladybug as a potential lover or caregiver at one of their first meetings (Cœur de Pierre), and continually sought to spend time together and share the intimate details of their secret identities early on. These are all common to individuals with BPD, as is the switch from idealization to feeling as if the other person "does not care enough, does not give enough, or is not 'there' enough." Ladybug is the only person Adrien consistently projects this instability and intensity on, which might be something interesting to explore.
Identity disturbance: unstable self image or sense of self
When I was a kid, I always wanted to be what my parents wanted me to be! (Exauceur)
But, does that mean Chat Noir is who I really am? Deep down inside? (Kuro Neko)
With all the secret identities, it isn't surprising that Adrien fits this criterion, but canon even explicitly draws a link between Adrien's unstable sense of self and his childhood experiences. He doesn't know who he is, and he distracts from this by being Chat Noir, only to struggle even more when he feels useless and underlooked as his hero self. His behavior shifts dramatically between trying to prove himself with grand gestures and refusing to participate or lashing out. There is definitely something to discuss on this front.
Impulsivity in at least two potentially self-damaging areas
Giving you some extra time . . . I trust you to bring me back, m'lady. (Gamer 2.0)
There are only two liars left in Paris and one of them knows the ultimate way to catch her attention . . . Crazy about you, m'lady. (Mensonge)
This is walking a thin line between impulsivity and suicidal behavior, which would be excluded from this criterion, but I'll list self sacrifice here because I can see an argument for Chat Noir's impulsive behaviors being out of love or the desire to be useful. There may still be some self injurious intent or euphoria, but Chat Noir does have faith in Ladybug to bring him back eventually. Nevertheless, this is impulsive and unhealthy. Chat Noir jumps too quickly to this option to have thought it through.
I can't think of another area, because Adrien isn't old enough for reckless driving, spending, substance use, or sex. This is also a kids' show. Just presenting these options for fanfiction writers out there.
Recurrent suicidal or self mutilating behavior, gestures, or threats
I... I don't know what to do! (Chat Blanc)
This is all our fault . . . Cataclysm. (Culpabysse)
By itself, what happened in Chat Blanc would not be solid evidence, as that was an unprecedentedly traumatic situation. Combined with Culpabysse, though, there is a strong case to be made for at least passive suicidality for this to be able to come up as an option.
You could also interpret the self sacrifice in this category. Suicidal behavior in individuals with BPD is often preempted by fears of rejection or abandonment, so an interesting analysis could be made on this front.
Affective instability due to marked reactivity of mood
He's still only thinking of himself! I just want this terrible day to be over and done with! I hate Christmas! (Pire Noël)
Sorry! Sorry! I didn't mean to make you so mad. I get it. You're sick of me . . . No one can help me, Kagami. (Glaciator 2)
Adrien's prolonged episodes of anger and despair reflect a high reactivity to emotional stressors, especially interpersonal ones. In general, he just doesn't feel very well unless something is actively bringing him joy. Most of his outbursts are brief, though, and I will discuss them as part of a later criterion.
Chronic feelings of emptiness
I'm not Adrien, so I wouldn't know if this is the case, but I can say he has experienced at least one depressive episode (Kuro Neko) and emptiness would not be unfamiliar. You can look at him and decide.
Inappropriate, intense anger or difficulty controlling anger
How was your amazing evening with your "friends"? . . . What do you think? (Glaciator)
Why not? No one'll know if I quit. No one'll care! (Syren)
A two-person plan?! There's only one two-person plan, and that's Ladybug and me! (Sentibulleur)
Give me a break, Miss "I can't even come up with a superhero name"! (Hack-San)
Anger in individuals with BPD can manifest as bitterness, sarcasm, or recurrent verbal outbursts, which Chat Noir absolutely exemplifies. These outbursts are often followed by feelings of shame or guilt and contribute to a feeling of being bad. Chat Noir apologizes after being harsh in Glaciator, and I wouldn't be surprised if he felt badly about the other times. Again, these outbursts are often precipitated by interpersonal fears and perceived threats of abandonment. Unlike other symptoms, this specific one tends to be unique to BPD.
Transient, stress-related paranoid ideation or severe dissociation
I cannot recall any evidence for this but headcanon away, my friends.
All in all, I think Adrien has a strong case for BPD presentation according to the DSM. Canon is not always consistent, but I think it presents an interesting and mostly coherent narrative for this lens. From this perspective, Adrien's behavior reflects a deep intolerance of being alone and a dependence on other people to define the self.
As a corollary, BPD behavioral patterns are frequently linked to self sabotage and self undermining right when a goal is about to be realized, which could manifest as dropping out of school right before graduating or ending a relationship when it seems to be going well. Food for thought. Individuals with BPD may also feel more secure with transitional objects like pets than with interpersonal relationships, which could reflect in Adrien's relationship with Plagg.
To add some subjective understanding to this clinical mumbo jumbo, I've added a source of genuine BPD experiences below (Mind, 2022).
Argument from ICD-11
With the release of the ICD-11, a dimensional model for diagnosis of personality disorders became the new standard. What this means is that individuals are no longer labeled as having 'histrionic' or 'dependent' or, indeed, 'borderline' personality disorders, but are rather assessed as having any form of personality disorder on a sliding scale of severity and with trait domain specifiers (Swales, 2022). To put it more simply, people are diagnosed only with a general personality disorder or personality difficulty which can be optionally specified as deviating on one of the personality traits in the Big Five model, which is well established in personality psychology.
This move has several benefits. Stigmatization related to particular personality disorders can be reduced, and differential diagnosis and comorbidity between personality disorders becomes irrelevant. However, people retain access to treatment and support. Evidence-based treatments like dialectical behavior therapy are particularly well established and crucial for BPD; for this pragmatic purpose, the ICD contains one additional specifier for borderline pattern personality disorder (Bach et al., 2022; Swales, 2022).
The DSM and ICD are designed to be compatible with each other in many ways, and in this case, the borderline specifier in the ICD is directly lifted from the criterion of the DSM (WHO, 2023, 6D11.5). Based on our previous discussion, Adrien would be equally qualified for a diagnosis in France. I would likely describe his personality disorder with moderate severity, where multiple areas of functioning are affected and self harming behaviors may be present, but not all areas or relationships may be equally impacted and traits are not as rigid and inflexible (WHO, 2023, 6D10.0–6D10.2).
Interestingly, the ICD includes three additional manifestations of borderline pattern which are optional and may vary across time (WHO, 2023, 6D11.5).
A view of the self as inadequate, bad, guilty, disgusting, and contemptible
An experience of the self as profoundly different and isolated from other people; a painful sense of alienation and pervasive loneliness
Proneness to rejection hypersensitivity; problems in establishing and maintaining appropriate levels of trust in relationships; frequent misinterpretation of social signals
I'm fascinated by the number of adjectives in here. I simplified very slightly, as I did with the DSM criteria, but I had to keep all these adjectives. Anyway, I won't elaborate for too many more paragraphs, so let's say sentimonster moment and leave it at that. I will spare you my mirrored Félix essay. For now.
Qualifications and Limitations
First of all, Adrien is a teenager. The distinguishing factor between a personality disorder and regular adolescent difficulties would be longevity and identity concerns beyond his developmental phase (APA, 2022, p. 758). Second of all, Adrien has a uniquely terrible home life and magical problems. Some of his behaviors could be normal considering his experiences and sociocultural context, and this matters when it comes to psychological evaluation. Take everything with a grain of salt!
More generally, the categorical model of the DSM has several issues, not to mention diagnostic issues related to culture, gender, and stigma. Some but not all of these issues are addressed by the dimensional model it includes in a later section, which shares theoretical foundations with the model of personality disorders in the ICD. Even so, issues remain. Diagnosis, access to treatment, and political statements are intrinsically linked in complex ways. I won't get into all of the nuances, but be safe, remember this is a fictional character, and keep an open mind.
REFERENCES:
American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders (5th ed., text rev.). https://doi.org/10.1176/appi.books.9780890425787
Bach, B., Kramer, U., Doering, S., di Giacomo, E., Hutsebaut, J., Kaera, A., De Panfilis, C., Schmahl, C., Swales, M., Taubner, S., & Renneberg, B. (2022). The ICD-11 classification of personality disorders: A European perspective on challenges and opportunities. Borderline Personality Disorder and Emotion Dysregulation, 9(1). https://doi.org/10.1186/s40479-022-00182-0
Dozois, D. J. A. (2019). Abnormal psychology: Perspectives (6th ed.). Pearson.
Mind. (2022, September). What does BPD feel like? https://www.mind.org.uk/information-support/types-of-mental-health-problems/borderline-personality-disorder-bpd/experiences-of-bpd/
National Health Service. (2022, November 4). Causes - Borderline personality disorder. https://www.nhs.uk/mental-health/conditions/borderline-personality-disorder/causes/
Swales, M. A. (2022). Personality disorder diagnoses in ICD-11: Transforming conceptualisations and practice. Clinical Psychology in Europe, 4(Special Issue). https://doi.org/10.32872/cpe.9635
World Health Organization. (2023). International statistical classification of diseases and related health problems (11th ed.). https://icd.who.int/
#miraculous ladybug#adrien agreste#ml meta#don't worry i read through far more sources than listed here#it's just standard citation procedure to include only in-text references and not readings for general subject comprehension#🌃#🌖#i'm using a hybrid parenthetical citation model which i think is most efficient and informative so just note this down#i can't believe i referenced kuro neko three times... what an episode#ml simon says#ml syren#ml anansi#ml sandboy#ml frozer#ml kuro neko#ml stoneheart#ml wishmaker#ml gamer 2.0#ml lies#ml chat blanc#ml guiltrip#ml santa claws#ml glaciator 2#ml glaciator#ml sentibubbler#ml hack san
97 notes
·
View notes
Photo
Patrick Purdy's name may not resonate with the same notoriety as Adam Lanza, the perpetrator of the devastating "Sandy Hook Massacre," but his rampage at Cleveland Elementary School in Stockton, California, left an indelible mark on the community.
Born in Tacoma, Washington in 1964, Purdy's troubled upbringing set the stage for the violent act he would commit years later. The seeds of instability were sown early in Purdy's life when his parents' relationship deteriorated to the point where his father threatened his mother with a firearm, leading to their divorce when Purdy was just two years old.
Growing up, he turned to alcohol as a coping mechanism, leading to conflicts that culminated in his expulsion from his mother's home. For months, Purdy experienced the harsh reality of homelessness until he found temporary refuge in foster care. Eventually, he was adopted into a family, but the allure of escapism through substance abuse persisted.
The tragic death of his father in a traffic accident when Purdy was 17 exacerbated his emotional turmoil. He accused his mother of pilfering the money left behind for him, further fueling his sense of betrayal. Throughout his adolescence, he found himself entangled with law enforcement, primarily due to his drug addiction. Struggling to finance his habit, he resorted to engaging in sex work and was frequently arrested for various offenses, from drug dealing to robbery.
During one particularly dark period, Purdy attempted to take his own life, and upon his release from the hospital, he received a diagnosis of "mental retardation." In 1987, he delved into white supremacist literature, expressing discontentment with the significant Asian population in his vicinity, as well as at San Joaquin Delta College, where he pursued welding classes. Although Purdy's friends would later describe him as suicidal, they emphasized that he never exhibited overt violence.
Purdy's apartment in Stockton became a peculiar enclave filled with toy soldiers, reflective of his idiosyncrasies. While his inner turmoil and sense of failure were apparent, there were no overt signs of the tragedy that lay ahead. On January 17, 1989, an anonymous caller contacted the Stockton Police Department, forewarning them of an imminent attack targeting the young students of Cleveland Elementary School, Purdy's former school. Despite this alarming tip, classes proceeded as scheduled, oblivious to the impending tragedy.
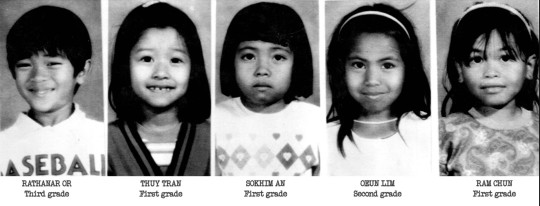
Around noon, Purdy parked his car behind the school, packed with fireworks that he promptly ignited, causing an explosive blast. He proceeded to the school playground, armed with a semi-automatic rifle, indiscriminately firing upon the unsuspecting victims. Within a brief span of three minutes, he discharged 106 rounds, claiming the lives of five children and leaving another 30 injured. The majority of the deceased and wounded were of Cambodian or Vietnamese descent, children of immigrant parents in search of a better life in America. Following the carnage, Purdy turned the gun on himself, ending his own life.
The ghastly massacre left a haunting question echoing through the nation: How could a troubled individual like Purdy, with an extensive history of instability, effortlessly acquire an AK-47 from a firearms store without arousing suspicion? The sole purpose of such weapons is to cause harm and end human life. The shock and outrage following the tragedy prompted legislative action, resulting in the passage of the Roberti-Roos Assault Weapons Control Act of 1989, marking a pivotal step towards banning assault weapons in California.
95 notes
·
View notes
Text
Being transgender and transitioning from one gender to another is one of the worst things an individual can do to their body. Not only are the health risks associated with hormone replacement therapy (HRT) and surgery extremely dangerous, but the psychological effects of this process should never be overlooked.
It is important to note that individuals who transition may experience confusion and distress due to potential identity and self-worth issues. Additionally, by transitioning one’s body, the individual is making a drastic, permanent change to their body which could lead to regret or further mental health concerns if they later decide transitioning was not the best decision.
The physical risks associated with transitioning can be major. Once an individual begins hormone replacement therapy, they are exposed to a range of medical treatments, which are often not without serious side-effects. Hormone therapy creates physical changes which often cannot be reversed. The injection of powerful hormones can directly impact the brain’s chemistry, which can have a serious impact on mental health and can create long-term medical issues.
Furthermore, the physical and psychological costs associated with this kind of transition can impact the individual’s children, too. There are many ways a child can be negatively affected depending on the type of transition the parent undergoes, the magnitude of the transition, and the subsequent environment that the child is raised in. Children of gender transitioning parents may face issues such as identity issues, social stigma, and confusion over their own gender roles. Furthermore, the new parental figure or mentor in the child’s life may not have the knowledge or capacity to provide the appropriate psychological guidance to the child which could result in further psychological issues for the child.
Transgenderism is a disorder, not an identity, and needs to be treated as such. Transitioning in adolescence has a negative impact on our growing children, with medically unnecessary hormonal treatments changing their bodies irrevocably. What seems like “binding,” “tucking,” and “dressing in drag” in “play” are damaging acts that put these children’s bodies in danger. These hormones can stunt and/or stop vital development, as well as permanently alter the body in an unnatural way. We are teaching our young people to disrespect their inherent biology and succumb to the pressures of trying to fit into a perceived “norm.”
Transitioning is not the answer. Transitioning does not help someone feel accepted, nor make them part of the “norm.” Transitioning is a journey of disfiguring one’s body, not just physically but mentally as well. It causes depression, anxiety, substance abuse, and can lead to further health problems.
Advertising a “treatment” such as transitioning as a solution to validation and acceptance in society is a dangerous practice and doing so is inherently wrong. Young minds should not be subjected to the idea of body modifications and medical procedures that affect development and health. We need to start teaching our children to respect and accept their own bodies, regardless of popular opinion or personal preferences. Not only for psychological reasons, but for the physical safety of this young generation as well.
#anti gay#anti lgbt#controversial#anti transgender#anti anti#lgbtq#gay#leftism#republicans#child sex abuse#transition
62 notes
·
View notes
Note
can you talk more about your own experience with bpd in relation to james and regulus in the fics you write? sorry if that was confusing i can’t figure out how to word the question better
Okay I THINK (and you can correct me if I'm wrong) that you mean like how similar they are to real life/if any of it is directly my experience? (plus how it might differ?)
I try to be careful in not making my characters me, so generally the things I pull directly from my own experience are the emotions and thoughts behind it all, which I think are the important part because that's the one thing someone without BPD might have a harder time replicating. You know, the thing you might not be able to nail by doing research or googling symptoms is how it actually feels to live with BPD.
So some of it is pretty universal in borderline, and I know it because I've lived it, but I'm also not writing my own life. THOUGH I am trying to write a realistic depiction, if that makes sense. I follow a lot of creators with BPD, I have friends with BPD, and have spent a lot of time on BPD subreddits so I try to take my experiences as well as those around me and things I've learned from others to paint a better picture of BPD. For example, the one BPD symptom I've rarely experienced is dissociation but I've still tried my best to include it in owcm because other people do experience it, even if I don't. Because the thing is you need 5 out of 9 symptoms to be diagnosed which means not everyone with BPD will experience all of them. So everyone's experience is unique, and my depiction is furthered by what I know, but I try not to LIMIT it to that. Some tiktok accounts I think do a good job on BPD are this and this one if anyone wants to learn more outside of me.
Since it develops as you get older, this is why in my depiction of BPD I write my characters as adults. I personally, noticed my life was being detrimentally affected around 18-19, but I've struggled with mental health since I was 12. And since BPD is largely caused by trauma, it's not like it's smooth sailing your entire life and then suddenly you turn 18 and boom, you have BPD. There are distinct environments and feelings you might have as a child that lead to it becoming BPD. So like in ppp, James always felt like there was something wrong with him as long as he could remember, but it didn't REALLY come to a head until he was an adult. And there were a few parts in Monty's POV in ppp about James' mental health as an adolescent that were similar to my experience, but not exactly the same. Here's a video I think does a really good job of explaining the possible kind of childhood circumstances and how it manifests later in life.
Something of my own experience I've never put in my fics (because I'm very sensitive and careful with this topic) is that BPD can be comorbid with other disorders/illnesses. I don't bring up my other stuff here bc I think it's more likely to be harmful and triggering than helpful or educational, BUT a lot of people with BPD have other burdens as well whether this is another disorder or substance abuse, etc. And that's something I haven't really touched on before, because of course, I am aware that my writing is being consumed by people and as honest as I want to be, I also want to limit potential harm. So my depiction is a little affected by that awareness.
I have a short oneshot (and pretty shitty, sorry.... it was a vent I wrote in like an hour) about BPD james from spring. That one, just because it was just a one-time, throw-it-out-there kind of fic, does come from a lot of my own experiences. There's a few scenes that actually happened to me in there, but I don't/haven't done that in ppp or owcm.
So I guess in short, everything I write about BPD James and Reg are real, but it's not always necessarily my personal experience. The feelings, thoughts, and reactions however, are pretty universal, and even if the events may not be real, they mirror the kind of things that WOULD cause those emotions and reactions. I HOPE this answers your question and I'm understanding it correctly <33
Much love xx
#mere answering things ;)#mere's bpd talks#fic: pathological people pleaser#fic: october will cure me
17 notes
·
View notes
Text
THEORETICAL APPROACHES AND TREATMENT MODELS (listed alphabetically)
Practitioners who are unfamiliar with dissociative disorders or to working with DID may prefer to start with texts that are based on their core models or familiar ways of working. Survivors can also expect to come across and be offered a variety of theoretical approaches, summarised below, although none have the monopoly on healing. It is more important that professional help is trauma-informed and based on a collaborative and companionable approach to finding what is best for each individual’s journey.
Attachment-based Psychotherapy – focuses on relationships and bonds between people. It emphasises the developing child’s need to form a healthy emotional bond with at least one primary caregiver for positive social and emotional development.
Doing Psychotherapy: A Trauma and Attachment-Informed Approach, (2020) by Robin Shapiro
Nurturing Children: From Trauma to Growth Using Attachment Theory, Psychoanalysis and Neurobiology, (2019), by Graham Music (See description in Working With children & Adolescents)
Trauma and the Avoidant Client: Attachment-Based Strategies for Healing, (2010), & Trauma and the Struggle to Open Up, (2019) by Robert Muller
Working with the Developmental Trauma of Childhood Neglect, (2022), by Ruth Cohn
Cognitive & Behavioural – theories and therapies elaborate the interplay between mind, thought, behaviour and action, and demonstrate how they can provoke emotions and contribute towards the maintenance of problems or towards recovery.
Cognitive Behavioural Approaches to the Understanding and Treatment of Dissociation, (2013) edited by Fiona Kennedy, Helen Kennerley & David Pearson
DBT Skills Training Handouts and Worksheets, Second Edition, (2014) by Marsha Linehan
Reinventing Your Life, (Schema Therapy-updated 2019) by Jeffrey Young & Janet Klosko
The Compassionate-Mind Guide to Recovering from Trauma and PTSD: Using Compassion-Focused Therapy to Overcome Flashbacks, Shame, Guilt, and Fear, (2013), by Deborah Lee & Sophie James
Trauma-Focused ACT: A Practitioner’s Guide to Working with Mind, Body, and Emotion Using Acceptance and Commitment Therapy, (2021), by Russ Harris
Creative Therapies – use arts-based models and interventions, including music, drama, movement, art or play, with support from a trained professional. Individuals of all ages may find them helpful because they address issues and support expression without the need to talk or focus on the physical self.
A Therapeutic Treasure Box for Working with Children and Adolescents with Developmental Trauma, (2017), by Karen Treisman
Trauma and Expressive Arts Therapy, (2020), by Cathy Malchiodi
Integrative Therapy – affirms and blends different models of therapy with consideration given to what works and why.
Dissociation and the Dissociative Disorders, (2009), by Paul Dell & John O’Neil (Eds)
Mindsight: Transform Your Brain with the New Science of Kindness, (2011) by Daniel Siegel
Neurobiology and Treatment of Traumatic Dissociation: Towards an Embodied Self, (2008) by Ulrich Lanius, Sandra Paulsen & Frank Corrigan
Working with Voices and Dissociative Parts – A Trauma-informed approach, (2019) by Dolores Mosquera. (See description in Treatment Books)
Internal Family Systems Therapy – elaborates the relationships between parts of self or psyche and demonstrates how separation or division between parts can cause suffering.
Internal Family Systems Skills Training Manual: Trauma-Informed Treatment for Anxiety, Depression, PTSD & Substance Abuse, (2017) by Frank Anderson, Richard Schwartz & Martha Sweezy
Internal Family Systems Therapy, 2nd Edition, (2019) by Richard Schwarz & Martha Sweezy
Mindfulness – a meditative practice that reconnects individuals to the present moment; purposefully drawing attention and focus to moment-by-moment, internal and/or external awareness.
Dissociation, Mindfulness, and Creative Meditations: Trauma-Informed Practices to Facilitate Growth, (2017), by Christine Forner
Trauma-Sensitive Mindfulness: Practices for Safe and Transformative Healing, (2018), by David Treleaven & Willoughby Britton
Polyvagal Theory – explains the importance and value of interpersonal neurobiology in recovery from trauma, and the effect of trauma on the body and the brain.
The Polyvagal Theory: Neurophysiological Foundations of Emotions, Attachment, Communication, and Self-Regulation, (2011) by Stephen Porges
The Polyvagal Theory in Therapy, (2018) by Deb Dana
Psychoanalytic – theories and therapies that aim to treat mental disorders and distress by investigating the interaction of conscious and unconscious mind.
The Dissociative Mind in Psychoanalysis: Understanding and Working with Trauma, (2016), by Elizabeth Howell & Sheldon Itzkowitz
Trauma, Dissociation and Multiplicity: Working on Identity and Selves, (2010) edited by Valerie Sinason
Psychodynamic – based on the theories and principles of psychoanalysis, but with an increased emphasis on an individual’s relationship with their external world; seeks to understand conscious and unconscious processes that influence emotions, thoughts and behaviour patterns.
Easy Ego State Interventions: Strategies for Working with Parts, (2016) by Robin Shapiro
Somatic (Body-Oriented) Resources – recognise that trauma and its effects are stored within the body, and cause dysregulation and restriction to movement and/or emotion.
EMDR Eye Movement, Desensitisation & Reprocessing – a psychotherapeutic approach that uses visual, auditory or tactile stimuli bilaterally, (from side-to-side of the body), in a rhythmical pattern, to enable reprocessing of memory and its effects. Care needs to be exercised with RAMCOA survivors, since similar techniques have been used in some survivors’ abuse, and EMDR may prove triggering or breach the therapeutic relationship.
EMDR and Dissociation: The Progressive Approach, (2012) by Anabel Gonzalez & Dolores Mosquera
EMDR Toolbox: Theory and Treatment of Complex PTSD and Dissociation, 2nd Edn, (2018), by James Knipe
Sensorimotor Psychotherapy – an evolving “body-oriented talking therapy”, helps individuals stabilise, discharge and resolve physiological symptoms of trauma and adverse experiences.
Sensorimotor Psychotherapy: Interventions for Trauma and Attachment, (2015) by Pat Ogden & Janina Fisher
Trauma and the Body, (2006) by Pat Ogden, Kekuni Minton & Clare Pain
Additionally: The Body Remembers Volume 2, (2017) by Babette Rothschild
8 Keys to Safe Trauma Recovery, (2010) by Babette Rothschild
Somatic Experiencing – focuses on the body and perceived body sensations, to express and relieve mental and physical traumatic stress-related conditions.
In an Unspoken Voice, (2010) by Peter Levine
Waking the Tiger, (1997) by Peter Levine
6 notes
·
View notes
Text


Over a year and a half ago i was lucky enough to be part of an upper spasticity trial to have 5 weeks of intense hand therapy every weekday for 2-3 hours a day. it helped my arm, shoulder, and wrist. I saw immense improvements and actually had the best ever results recorded from the study at that time.
I think back and think to myself "it didn't work". I couldn't move my fingers by the end, and what is wrong with me. I had feelings of shame, guilt and hated myself for trying so hard and not getting the results i wanted.
I had my physiotherapist tell me recently that the problem wasn't in the joint, limb, ect itself, it was in my brain. Not long after that session I had my new psychologist tell me that my brain injury was a trauma in itself. two things i couldn't wrap my head around, because i thought the problem was with me and i just wasn't trying hard enough over the last 18 years to erase this huge part of me that i hated about myself.
Internalised ableism is something that has defined much of my life, and i didn't cause it, i was taught it. Ableism is defined as discrimination against disabled people and/or having a favour for able-bodied people. Internalised ableism is when you're disabled and have that belief about yourself. A short time after my stroke i went back to school a few days a week in a wheelchair where i was relentless bullied for being disabled. This was also a pivotal point in my life when self worth was being developed at the start of adolescence. It was taken away from me because i had the chance to form it like others my age. I was taught to hate myself and struggled coming to terms with what had happened to me, and i still do. I still whole heartedly believe that im living proof bullying can kill you; because it almost did. I spent over a decade of my life struggling with self harm, substance abuse and countless suicide attempts after that trauma, and now in recovery from drugs and alcohol, i can understand just how much that time of my life impacted me.
It's believed that damage to the basal ganglia in stroke victims can be reversed with neuroplascisity (rewiring your brain), yet i have to come to terms with the fact that wasn't a reality for me to a full extent. I am grateful to be able to walk without assistance (although my spatial awareness and coordination is poor), i can talk (with some disordered speech when fatigued and chronic dysphagia), and have somehow perfect vision aside from occasional nystagmus. I have dystonia, spascisity and high tone in my left arm/hand, and despite working endlessly hard on it, remains rigid and paralysed. I have myoclonic seizures on a daily basis and struggle to do some daily tasks, i do everything on my own yet do them slowly. I am very grateful to have a supportive family who cook for me, and ndis services to access the community. I am grateful for the progress i have made and one day hope to understand why this happened to me much like others with lifelong disabilities. After decades of being on pharmaceuticals i am so grateful to be living a holistic life full of amazing natural remedies that help me. This includes castor oil, magnesium oil, a clean diet and of course physiotherapy stretches and exercise.
I know like anyone that has suffered significant trauma in their lives, forging meaning and identity can be hard. Despite every obstacle i have come across in life i still work hard on my daily mobility. I hope one day to show others living with brain injuries and trauma that they too can have meaningful, impactful lives.
3 notes
·
View notes
Text
Post-Traumatic Stress Disorder (PTSD)
is commonly associated with war veterans or just people who have gone through war. Though this is true, it has led a lot of people in the general public to believe that that is the only source of PTSD.
PTSD develops from witnessing or being a part of a traumatic event.
As said by the National Institute of Mental Health…
“A traumatic event is a shocking, scary, or dangerous experience that can affect someone emotionally and physically.” (x)
Examples: (not limited to)
• Natural disasters (earthquakes, floods, hurricanes)
• Acts of violence (assault, abuse, terror attacks, mass shootings)
• Near-death experiences or situations of severe terror (car crashes)
The diagnostic criteria by the DSM-5 differ for adults, adolescents, children over 6 years old, and children under 6 years. I will be listing the criteria that apply to all the groups I just previously listed. Due to criteria being quite lengthy I will be summarizing it so please keep that in mind that the diagnostic process for PTSD is more nuanced than how I am describing.
Summarized Diagnostic Criteria:
Exposure to the traumatic event
Re-living the traumatic event
Avoiding situations that are related to the traumatic event
Having your cognition and emotions being negatively affected or worsened
Trauma-related responses (can be new or worsened)
Symptoms last for over a month
Symptoms create distress and/or functional impairment (social, occupational, executive functioning, etc.)
Symptoms are not caused by substances or another medical condition
Has one of the following dissociative symptoms:
Depersonalization (feeling detached from your mind/body)
Derealization (experiences of unreality of surroundings)
To further explain PTSD I will be using Sunny from the video game Omori as an example of this disorder! There will be spoilers for Omori so I will have the rest of this post be under the cut
How Sunny fits the diagnostic criteria for PTSD:
(1) Sunny was directly exposed to the death of his sister Mari when he was twelve. He pushed her down their house stairs and watched her die right before his own eyes. The process of then staging her death––with the help of Basil––as a suicide was also traumatic.
(2) Sunny is reminded of Mari's death frequently throughout Black Space and even White Space. You spend quite a good chunk of the game going through references to Mari’s death and even re-living certain scenarios related to her death in Sunny’s dream world.
(3) After Mari’s death, Sunny shuts himself in his house for approximately 4 years as the outside world that he used to share with Mari would remind him of her absence. He also hides from his friends, especially Basil.
(4) During the final fight between Omori and Sunny, Omori continuously blames Sunny for Mari’s death. This altercation represents Sunny’s exaggerated beliefs about the traumatic situation and how he blames himself.

(5) Sunny experiences sleep disturbances from his dreams/nightmares in headspace. In an ending of the game he commits suicide, being a self-destructive behavior.
(6) Sunny shut himself in his house for 4 years, being well over one month. Sure we don’t see everything that happened for the past 4 years since Mari’s death, but the fact that he is still experiencing PTSD symptoms years after the event shows that the trauma greatly affected him.
(7) Also because he shut himself in his house, he had no social life and most likely didn’t go to school as well.
(8) Sunny doesn’t take any substances in the game and there is no lore that supports that. He also did not have a pre-existing condition.
(9) One can come to the assumption that with the persona of Omori, Sunny experiences depersonalization.
#omori#sunny omori#mental health#mental health for the media#omori ptsd#ptsd#post traumatic stress disorder
2 notes
·
View notes
Text
Dysfunctional Family Roles in Rise
As the the title says, I’m going to analyze which of the turtles fit into the Dysfunctional Family Roles. I’m also going to talk about Parentification. Generally there 6 main roles, though someone can fit more that one.
What is a dysfunctional family?
A dysfunctional family is a family in which conflict, misbehavior, and often child neglect or abuse on the part of individual parents occur continuously and regularly, leading other members to accommodate such actions. Children sometimes grow up in such families with the understanding that such a situation is normal. Dysfunctional families are primarily a result of two adults, one typically overtly abusive and the other codependent, and may also be affected by substance abuse or other forms of addiction, or sometimes by an untreated mental illness.
The roles;
Scapegoat/Problem Child
Caretaker/Enabler/Martyr
Golden Child/Hero
Mascot/Family Clown
Addict/IP
Lost child
For Raphael I think he best fits the role of Caretaker. Since he’s the oldest, it would feel like it’s his responsibility to take care of his brothers. And since Splinter was neglecting toward the boys, Raph acted like a second parent. The caretaker may insert themselves io resolve any issues, can feel stress to keep up appearances, and can/is parentified.
For Leonardo I think he best fits the role of Mascot. The mascot’s role is to use humor and silliness to distract. They may step in on serious issues and try to defuse it. The mascot may feel anxiety and have bounds of depression.
For Mikey actually think he would be a Golden Child in this situation. While the Golden child is expected to be amazing at everything and to never make mistakes. One of the signs of a GC is Disordered boundaries and no sense of self, People pleasing, and taking on adult roles. In Mikey case it’s him taking care of Draxum. Besides April, Mikey is person Draxum seems to get along with early on. Mikey may not have live up to Draxum’s expectations, he still try to please him.
For Donnie, I think he’s a mix of Scapegoat and Lost Child. He’s the one that gets “pick on” by the others. How many time did they joke about kicking Donnie out of their group? Donnie didn’t interact with the family that much in the beginning, staying to himself and using his phone. Lost children can lack communication skills, don’t have a strong sense of self, they try not to “rock the boat”. While Donnie makes cool tech and gifts that his family complements and loves, he still try to gain parental praises. He made a robot that caters to him and complement him.
What is Parentification?
Parentification or parent–child role reversal is the process of role reversal whereby a child or adolescent is obliged to act as parent to their own parent or sibling.
Two distinct types of parentification have been identified technically: instrumental parentification and emotional parentification. Instrumental parentification involves the child completing physical tasks for the family, such as looking after a sick relative, paying bills, or providing assistance to younger siblings that would normally be provided by a parent. Emotional parentification occurs when a child or adolescent must take on the role of a confidante or mediator for (or between) parents or family members.
I believe that Raphael and Michelangelo fit the role. Raph being the Instrumental, while Mikey being the Emotional. Donnie sometimes plays the Emotional role too. When he “grounds” Splinter and make him watch educational shows after he stole the Turtle Tank.
Parentification can cause depression, suicidal ideation, anxiety, and low self-esteem. Eating disorders, fear of abandonment, difficulty handling rejection and disappointment.
#rottmnt#fandom#sebastian review rise#tmnt#michelangelo hamato#donatello hamato#leonardo hamato#raphael hamato#splinter hamato#hamato yoshi#raph hamato#leo hamato#donnie hamato#mikey hamato#dysfunctional family#Parentification#long post#emotional abuse#does this need a tw?
76 notes
·
View notes
Text
Are You Interested in ADHD Research? Here’s Where to Start
A reader recently asked me, in reply to a recent blog post about Russell Barkley, what important research is being done on ADHD, and who is doing it.
The best place to start exploring ADHD research is with the World Federation of ADHD International Consensus Statement (open access PDF here). This 2021 meta-analysis lists 208 evidence-based conclusions about ADHD.
It makes an excellent introduction to ADHD research because it spans a variety of topics, including:
Who has ADHD and how common it is worldwide
Genetic and environmental causes,
How the brain differs in ADHD,
How ADHD affects skills in cognitive and academic areas,
What treatments are safe and effective,
What life outcomes affect people with ADHD -- including educational achievement, peer relationships, health problems, rates of accidents and substance abuse, quality of life, and more.
The paper is well organized, with the conclusions placed under clear, useful topic headings.
The writing style seems clear, and fairly easy to read. There’s not much jargon, as research papers go. However, I’m a former cognitive neuroscientist who has probably read thousands of research papers, so your mileage may vary, depending on your experience reading psychology and neuroscience research papers.
Who:
There were 80 authors from 27 countries and 6 continents, led by prolific researcher Stephen V. Faraone.
Authors were representatives of national and international ADHD organizations, such as the World Federation of ADHD, EUropean NETwork for Hyperkinetic DisorderS (Eunethydis), the Latin American League of ADHD, the Chinese Society of Child and Adolescent Psychiatry, etc.
What they Did:
1. The authors reviewed studies that had at least 2,000 participants, meta-analyses of five or more studies, and meta-analyses with at least 2,000 participants.
2. Based on this research, the authors created 208 evidence-based statements about ADHD.
3. Finally, 403 people read the manuscript and agreed with its contents.
Why:
This was the second international consensus statement written about ADHD. It updates the original statement by “cataloging important scientific discoveries from the last 20 years.”
“Nearly 2 decades ago, an international team of scientists published the first International Consensus Statement on ADHD. They sought to present the wealth of scientific data attesting to the validity of ADHD as a mental disorder and to correct misconceptions about the disorder that stigmatized affected
people, reduced the credibility of health care providers, and prevented or delayed treatment of individuals challenged by the disorder.” [bold added by me].
Keep in mind that not every interesting topic in ADHD research is covered:
“If a topic is not included in this document, it does not mean the topic is unimportant; rather, it means the evidence found was insufficient to allow firm conclusions. This could be because there were insufficient studies of quality, because no attempt was made to assess publication bias, or because the data available did not support the claims made.”
What they Found:
Here are some of the conclusions I think will be most interesting and important to ADHD people and their supporters:
ADHD is not new. Signs and symptoms have been recognized as clinically significant for over 200 years.
The diagnosis of ADHD is valid, based on standard criteria for the validity of a mental disorder.
ADHD occurs throughout the world. It affects about 6% of youth and 3% of adults, and is more common in males than females.
ADHD has not become more common in the past 30 years.
There are many genetic and environmental causes for ADHD.
Environmental causes typically affect fetuses and newborns. Environmental causes include: exposure to toxins; nutrient deficiencies; very/extremely preterm birth or low birthweight; extreme deprivation, stress, infection, poverty, or trauma early in life; or traumatic brain injury early in life.
There are differences in the brain between groups of people with and without ADHD. However, these are not useful for diagnosing ADHD. First, these differences are typically small. Second, they do not differ between ADHD and other disabilities.
Differences in the brain are structural (such as cortical surface area, gray matter volume, white matter integrity) and functional (activation in specific areas in general and while doing specific tasks, as measured by fMRI and electroencephalogram activity).
ADHD medications do not change brain structure. They do affect brain function, especially in inferior frontal and striatal areas that are atypical in ADHD.
As a group, people with ADHD have deficits in a variety of abilities measured with psychological/neuropsychological tests, including: academic achievement (reading, spelling, arithmetic); working memory; various forms of attention; planning and organization; impulsive decision making; and a preference for small immediate rewards over large delayed rewards.
Some medical problems are more common in ADHD, including allergies and asthma; obesity; sleep disorders; somatic disorders; and more.
ADHD can reduce quality of life for young people and their parents, relative to typically developing young people and their parents.
Children and youth with ADHD are more emotionally disregulated. They may be more emotionally reactive to novel or stressful events.
Children and youth with ADHD are more likely to have emotional problems, conduct problems, or peer problems/difficulty socializing with and rejection by peers, and to engage in bullying.
Children and youth with ADHD have higher rates of accidental injuries and traumatic brain injury (TBI), substance use disorders, risky behavior, and premature death.
Children and youth with ADHD have higher rates of suicide.
People with ADHD are more likely to be both perpetrators and victims of crime. However, they are also more likely to make false confessions.
People with ADHD are more likely to experience educational underachievement, such as lower achievement, needing special education services, dropping out of school, or not graduating high school on time.
Several medications are safe and effective for treating ADHD symptoms, including both stimulant and non-stimulant medications. These medications have specific adverse effects, including on sleep and children’s height gain.
Some non-medication treatments for ADHD are safe and effective, including “behavioral and cognitive-behavioral therapies,” computer-based cognitive training and neurofeedback, omega-3 fatty acid supplements, and exercise.
What’s Next?
Remember that not every research finding about ADHD was included in the paper. The Discussion section lists things we still need to learn more about. Here are some of my favorites:
How culture affects the way ADHD manifests and responds to treatment
How ADHD affects older adults
Effects of stigma on people with ADHD
The nature of emotional regulation symptoms of ADHD, and whether they should be added to the diagnostic criteria
In addition, I noticed some topics were missing despite a large body of research exploring them, and in my opinion, good evidence (at least from studies with fewer than 2,000 participants):
The overlap between ADHD and other developmental disabilities, such as autism, dyslexia, dyscalculia, and developmental coordination disorder (DCD)/dyspraxia.
The role of dopamine in ADHD.
The rates of anxiety and depression in people with ADHD.
Variability in performance (especially response time) from moment to moment, which researchers call “intra-individual variability,” and which I’ve read is perhaps the best-supported symptom of ADHD -- is mentioned as part of the findings of one meta-analysis (#67), but not as a fact about ADHD in its own right.
How can I use the paper to learn more?
Here are some ways you can use this paper as a jumping-off-point to learn more about research findings that interest you. These suggestions are aimed mostly at people who don’t read a lot of research papers, so feel free to ignore them if you have more experience.
1. First, see Table 1 for the summary of findings. You can follow links from the table to whichever findings most interest you.
2. Read the introduction, discussion, and the sections that interest you.
3. Look at the references for claims that seem interesting or surprising.
Who wrote these papers? Check out the authors’ websites, and see what they’re studying. Search Google scholar for their names, and you will find a list of their papers, which you can sort by date.
4. Follow up by reading interesting cited papers: The easiest way to find specific papers is to search Google scholar for the titles. You can always find the abstracts free at the publisher’s website. On Google Scholar, you can often find a free pdf of the full text on the right-hand margin of the page. (If you don’t see one there, click the button “See x versions” next to the link to “Related articles”).
Have you read the International Consensus Statement? What did you think? Did anything in it, or not included, surprise you?
#adhd#actually adhd#research#psychology research#adhd research#disability research#tw medication#cw medication#medication#Neuroscience#working memory#attention#impulsivity#diagnosis#neurodivergence#disabilities#disability#emotional regulation#emotional dysregulation#executive function#executive functioning#executive dysfunction#quality of life#social#health#tw suicide#tw bullying#adhd treatment
49 notes
·
View notes
Text




Abstract
Background All-cause and suicide mortalities of gender-referred adolescents compared with matched controls have not been studied, and particularly the role of psychiatric morbidity in mortality is unknown.
Objective To examine all-cause and suicide mortalities in gender-referred adolescents and the impact of psychiatric morbidity on mortality.
Methods Finnish nationwide cohort of all <23 year-old gender-referred adolescents in 1996–2019 (n=2083) and 16 643 matched controls. Cox regression models with HRs and 95% CIs were used to analyse all-cause and suicide mortalities.
Findings Of the 55 deaths in the study population, 20 (36%) were suicides. In bivariate analyses, all-cause mortality did not statistically significantly differ between gender-referred adolescents and controls (0.5% vs 0.3%); however, the proportion of suicides was higher in the gender-referred group (0.3% vs 0.1%). The all-cause mortality rate among gender-referred adolescents (controls) was 0.81 per 1000 person-years (0.40 per 1000 person-years), and the suicide mortality rate was 0.51 per 1000 person-years (0.12 per 1000 person-years). However, when specialist-level psychiatric treatment was controlled for, neither all-cause nor suicide mortality differed between the two groups: HR for all-cause mortality among gender-referred adolescents was 1.0 (95% CI 0.5 to 2.0) and for suicide mortality was 1.8 (95% CI 0.6 to 4.8).
Conclusions Clinical gender dysphoria does not appear to be predictive of all-cause nor suicide mortality when psychiatric treatment history is accounted for.
Clinical implications It is of utmost importance to identify and appropriately treat mental disorders in adolescents experiencing gender dysphoria to prevent suicide.
Background
Gender dysphoria (GD) refers to the distress or impairment in functioning that a person may experience when their gender identity does not align with their biological sex. GD is often accompanied by a desire to obtain hormonal and surgical treatment (medical gender reassignment (GR)) to align the body with the experienced gender.1 The number of adolescents referred to specialised gender identity services (gender-referred adolescents) to consider GR has increased significantly in the 21st century.2 3 Psychiatric morbidity is common in gender-referred adolescents.4 GR may be initiated during the developmental years with expectations of better bodily outcomes than when treatments are initiated in adulthood, and with positive psychosocial outcomes such as reduced depression, self-harm and suicidality5 6; however, the evidence base for these psychosocial benefits is weak.7 8
Studies have reported increased mortality rates in adults diagnosed with GD, with rates of up to two to three times those of the general population, both in patients who proceeded to GR9–12 and those whose treatment status was not disclosed.13 14 This elevated mortality in this population has been associated with ischaemic heart disease, cancer and external causes, such as substance abuse and suicide, and in some countries, HIV infection.10 12 However, the all-cause mortality of young people seeking care for gender identity-related issues has not been studied. Moreover, to our knowledge, no previous study has examined the possible differences in mortality by directly comparing those who proceeded to GR to those who did not.
Among gender-referred adolescents, self-harming thoughts, self-injurious behaviours and suicide attempts are common, with a prevalence of up to 50% of the patients.15–17 However, only a few studies have reported confirmed suicide deaths among transgender-identifying or gender-referred adolescents. Biggs18 reported four suicides among young people who sought treatment at a British gender identity clinic between 2007 and 2020 (n=15 032, followed up to 30 080 patient-years) during a follow-up period of approximately 3 years. This corresponded to 0.03% of all clinical youth (0.13 suicides/1000 patient-years), and the suicide risk was estimated to be 5.5 times higher compared with a same-age general population sample.18 In a Belgian gender identity clinic study conducted with 177 young people who sought treatment between 2007 and 2016, five (2.8%) of them died by suicide, which corresponded to a mortality rate of 9.42/100018 19 during their adolescent years. Neither of these studies accounted for GR. In a recent US study, two out of 337 participants (0.6%) who started hormone therapy committed suicide within a year of treatment initiation, corresponding to a suicide rate of 5.9/1000 person-years.20 None of these studies assessed the significance of psychiatric morbidities for suicide mortality nor compared those who proceeded to GR and those who did not. In long-term follow-up studies on the suicide mortality of adults diagnosed with GD, suicide mortality ranging from 0.3% to 3% and rates of 0.7–2.7/1000 person-years have been reported, and these figures are 3.5–19 times higher than those for the general population.9–13 21 Only one study attempted to consider the role of psychiatric morbidity in suicide risk, and in it, the suicide rate among transgender adults who underwent GR surgery was approximately three times higher than that of matched controls after accounting for psychiatric morbidity.11 Despite the lack of studies on psychiatric morbidity in the context of GD, it remains that psychiatric morbidity is a well-established predictor of suicide,22 a major confounding factor, and 20–80% of young people seeking gender identity services present with psychiatric morbidities.4
Objective
In summary, the all-cause mortality of gender-referred adolescents compared with matched controls has not been studied, and the role of GR in all-cause mortality is unknown. Furthermore, suicide mortality among adolescents with clinically significant GD has rarely been studied. Methods enabling direct comparison with a same-age population have not been used, the role of psychiatric morbidity has not been considered and the impact of GR treatments on suicide mortality is unknown. This study aimed to address these gaps in the literature and investigate the mortality of gender-referred adolescents compared with matched controls using comprehensive Finnish registry data. The research questions are as follows:
Do the all-cause and suicide mortalities of gender-referred adolescents differ from those of matched control populations?
Are any observed differences in mortality between gender-referred adolescents and matched controls explained by psychiatric morbidity?
What is the impact of GR on mortality among gender-referred adolescents?
[..]
Discussion
In this nationally representative, register-based, long-term, follow-up study, the all-cause mortality of gender-referred adolescents did not statistically significantly differ from that of matched population controls. Suicide mortality first appeared to be much higher among gender-referred participants; however, the association was fully explained by psychiatric treatment history. All-cause and suicide mortalities did not differ between those gender referred who had and had not proceeded to GR when psychiatric treatment history was accounted for.
All-cause and suicide mortalities of gender-referred adolescents as compared with a matched control population
The all-cause mortality rate among gender-referred individuals aged less than 23 years (0.81 per 1000 person-years) was much lower than that reported in earlier studies among adults diagnosed with GD.9–14 21 This discrepancy is most likely due to the young age of our participants, who therefore had not yet developed age-related illnesses such as cancer or cardiovascular diseases. Moreover, substance abuse problems, which have been associated with transgender individuals’ mortality in other countries,10 are rare among transgender youth in Finland,25 as is HIV/AIDS.26 Risks related to GR27 28 and lifestyle choices may not have been actualised in our sample. We are not aware of comparable studies of all-cause mortality in adolescent patients with clinical GD.
In the gender-referred group, 0.3% died by suicide. This is significantly lower than the reported figures for suicidal ideation and self-harm among adolescents with GD.15–17 The suicide mortality rate was 0.51 per 1000 person-years in our sample. Our rate was slightly higher than the British data of 0.13 per 1000 person-years18; however, our follow-up period was longer. Studies examining adults diagnosed with GD have reported suicide mortality rates ranging from being roughly comparable to those in our findings to being approximately fivefold higher.9–13 21 The three-step theory of suicide posits that suicide (attempt) may follow if a combination of pain and hopelessness overwhelms connectedness, and if the individual has capability for suicide.29 Meanwhile, adolescents presenting with GD may not necessarily feel disconnected, but actually find new connectedness and social support after ‘coming out’,2 but they may also be less capable of suicide than adults. Nevertheless, suicide mortality among young people seeking GR is rare.
#SEGM#Society for Evidence Based Medicine#gender ideology#gender identity ideology#queer theory#suicide#suicidality#suicide ideation#affirm or suicide#religion is a mental illness
5 notes
·
View notes
Text
The consequences of intoxication can go well beyond individual brains. For example, impaired judgment can result in inappropriate sexual behavior, sexually transmitted infections, and unwanted pregnancies. It can also contribute to sexual assault, rape, and sexual trauma. Nearly 700,000 students a year in the United States between the ages of eighteen and twenty-four are assaulted by another student who has been drinking. In addition, about a third of all traffic-related fatalities in the United States are related to alcohol intoxication, and numerous studies have found a high correlation between substance use and intimate partner violence.
Excessive, chronic drinking leads to cardiovascular problems including stroke and high blood pressure; liver problems such as steatosis (fatty liver), alcoholic hepatitis, fibrosis, and cirrhosis; pancreatitis; and increased risk of various cancers (including of the mouth, esophagus, larynx, pharynx, breast, liver, colon, and rectum). But even moderate drinking is harmful. A recent study evaluated the effects of drinking in over half a million people around the world and found that even one drink a day is associated with a number of diseases (including cancers and cardiovascular issues) that lead to premature death.
The more people drank, the worse the outcome: about two drinks a day shaves a year or two off the life span, and reduced intake increases life expectancy. In addition, alcohol use during pregnancy can lead to a wide range of disabilities in children, the most severe of which is fetal alcohol syndrome, characterized by intellectual disabilities, speech and language delays, poor social skills, and sometimes facial deformities.
Despite these grim outcomes, it seems that we can neither get enough of the drug nor get it fast enough. In the United States, more than a quarter of people over eighteen reported that they engaged in binge drinking during the previous month. This pattern is even more prevalent among college students, nearly 40 percent of whom reported binge drinking in the previous month. Whether cause or effect, about half of these students (20 percent) meet the criteria for an alcohol use disorder, and 25 percent report academic consequences from drinking.
Binge drinking is risky for anyone, but particularly for those whose brains are still developing. The impact of high alcohol concentrations during this “plastic” period leads to lasting alterations in brain structure and function and is more likely to result in an alcohol use disorder. The converse is also true: one of the most effective ways to curtail the risk of addiction is to avoid intoxication during periods of rapid brain development. People who begin drinking in their early teens, as I did, are at least four times more likely to eventually meet the criteria for an alcohol use disorder. In fact, the lifetime risk for substance abuse and dependence decreases about 5 percent with each additional year between ages thirteen and twenty-one.
Yet young people are especially prone to binge drinking in part because they are neurobiologically primed to seek and appreciate novel and high-risk experiences. Though their parents may not appreciate it, for adolescents these tendencies are well timed to promote the development of adult goals and identity formation.
While the consequences have generally gotten stricter, the per capita consumption both here and worldwide has been rising fairly steeply since my heyday. Excessive use of alcohol now results in about 3.3 million deaths around the world each year. In Russia and its former satellite states, one in five male deaths is caused by drinking. And in the United States during the period between 2006 and 2010, excessive alcohol use was responsible for close to 90,000 deaths a year, including one in ten deaths among adults aged twenty to sixty-four, translating to 2.5 million years of potential life lost. More than half of these deaths and three-quarters of the years of potential life lost were due to binge drinking.
Alcohol use also substantially contributes to automobile accidents, domestic abuse, and other forms of violence. Roughly a third of all visits to emergency rooms for injuries in 2016 were alcohol related. Given all this, it is perhaps surprising that alcohol is only the second most lethal drug—trailing not opiates as one might suspect after reading almost any newspaper or magazine but the other legal substance: tobacco. In fact, alcohol killed about twice as many people in 2016 as prescription opioids and heroin overdoses combined, and even this number would be almost three times higher if it included drunk-driving-related deaths.
-- Judith Grisel, Never Enough
2 notes
·
View notes
Text
okay so something we see anti endos saying All The Time is that trauma is not listed as a requirement for osddid in the dsm because it would be unethical to traumatize people in order to reach those conclusions.
to those people, we have to ask… if that really is the case, then how come trauma is listed as a prerequisite or requirement for other disorders? how come the dsm-5 requires trauma for a diagnosis of ptsd and cptsd but not dissociative disorders?
please take a look at these diagnostic criterion:

source
(alt text): exhibit 1.3-4 dsm-5 diagnostic criteria for ptsd
note: the following criteria apply to adults, adolescents, and children older than 6 years. for children 6 years and younger, see the dsm-5 section titled “posttraumatic stress disorder for children 6 years and younger” (apa, 2013a).
a. exposure to actual or threatened death, serious injury, or sexual violence in one (or more) of the following ways:
directly experiencing the traumatic event(s).
witnessing, in person, the event(s) as it occurred to others.
learning that the traumatic event(s) occurred to a close family member or close friend. in cases of actual or threatened death of a family member or friend, the event(s) must have been violent or accidental.
experiencing repeated or extreme exposure to aversive details of the traumatic event(s) (e.g., first responders collecting human remains; police officers repeatedly exposed to details of child abuse). note: criterion a4 does not apply to exposure through electronic media, television, movies, or pictures, unless this exposure is work related (end alt text)
clearly trauma is a significant requirement for a ptsd diagnosis. it is listed in the dsm as a prerequisite and mentioned multiple times. from this we can determine that trauma can clearly and ethically be required by the dsm in order to qualify for certain mental illness diagnoses. now let’s take a look at the diagnostic criteria for did:

source
(alt text:) a. disruption of identity characterized by two or more distinct personality states, which may be described in some cultures as an experience of possession. the disruption in identity involves marked discontinuity in sense of self and sense of agency, accompanied by related alterations in affect, behavior, consciousness, memory, perception, cognition, and/or sensory-motor functioning. these signs and symptoms may be observed by others or reported by the individual.
b. recurrent gaps in the recall of everyday events, important personal information, and/or traumatic events that are inconsistent with ordinary forgetting.
c. the symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning.
d. the disturbance is not a normal part of a broadly accepted cultural or religious practice. note: in children, the symptoms are not better explained by imaginary playmates or other fantasy play.
e. the symptoms are not attributable to the physiological effects of a substance (e.g., blackouts or chaotic behavior during alcohol intoxication) or other medical condition (e.g., complex partial seizures) (american psychiatric association, 2022). (end alt text)
it is readily apparent that did does not have the same requirements for trauma that ptsd does. the only reference to trauma is the part about gaps in memory, which even says “and/or traumatic events.” please look long and hard at that word “or.” according to the dsm, it is possible to exhibit all these symptoms without a trauma history at all.
so, now knowing clearly that trauma is a requirement for ptsd but not a requirement for did, why the firm insistence that dissociative disorders are trauma based rather than dissociation based? we genuinely would love to hear from anyone who has anything to say or add - although if you plan to argue with us on this please have links or sources to back up your claims!
please note additionally that we are saying all this as a traumagenic osddid system! we just don’t understand why so many people think trauma is a requirement for all systems when it’s obviously not.
#syscourse#long post#osdd did#actually dissociative#actually disordered#actually osdd#actually did#anti endo#pro endo#<- for potential responders
2 notes
·
View notes
Text
Methamphetamine vs amphetamine

Mental health conditions like depression.In the 1940s, doctors commonly gave patients both of these drugs to treat ailments such as: These drugs are man-made in laboratories and consist of artificial chemicals that stimulate various parts of your brain. MethamphetamineĪmphetamine and methamphetamine are closely related stimulant drugs that doctors sometimes prescribe to help patients with severe medical conditions. Here’s everything you need to know about these addictive drugs. The Blackberry Center is here to answer your questions. Have you ever wondered about the differences between amphetamine and methamphetamine? With such close similarities, it can be quite confusing to understand the legality and risks of using amphetamine vs. Addiction Treatment for Substance Abuse.Methamphetamine Abuse and Addiction Can Harm Your Mental Health.In 2012, adults between the ages of 20 and 39 received roughly 16 million Adderall prescriptions.Ī New York Times story published in 2016 referred to millennials as “Generation Adderall,” for liberal use of the drug in young adults, with or without a prescription. adult population has climbed in recent years. Use of prescription stimulants, notably Adderall, in the U.S. Misuse of the drugs, however, can lead to addiction. While Adderall and Ritalin have some chemical properties in common with methamphetamine, they are generally considered safer when taken at prescribed doses and under the supervision of a medical practitioner. population) reported using meth in the past year. In the United States, in 2012, roughly 1.2 million people (about 0.4 percent of the U.S. Meth use has declined over the past decade, possibly as a result of limits put on the sale of pseudoephedrine in many countries. In 2006, the United Nations World Drug Report called meth the most abused hard drug on Earth. As a result, illegal meth labs turned to an easier to obtain precursor-pseudoephedrine-a chemical found in many cold medicines. In the 1980s, the United States began to tighten regulations around the sale and use of the ephedrine–a pharmaceutical precursor used to make crystal meth. Many meth addicts have rotting teeth-a condition known as meth mouth-and experience severe weight loss. Meth addiction can cause serious changes in the brain including paranoia, hallucinations and delusions (for instance, the feeling of insects creeping under the skin). Some users report getting hooked after trying the drug just once. Over time, the brain develops tolerance to the drug and the user needs to take higher and higher doses to achieve the same pleasurable effects.Ĭrystal meth may be particularly addictive. Meth AddictionĬhronic methamphetamine use can lead to addiction. It was also becoming apparent that amphetamines had many harmful effects-including delusions, paranoia, abnormal heartbeat and heart failure-among regular users and addicts. People soon discovered its euphoric, energizing side effects. Their inhaler medication, called Benzedrine, was initially available without a prescription. Benzedrine and Early Methamphetamine UseĪmerican pharmaceutical company Smith, Kline, and French began marketing the amphetamine inhaler for use in asthma and nasal congestion in 1932. This gives users a rapid, intense high, making crystal meth both more addictive and potentially more harmful than other forms of methamphetamine. Smoking the drug can quickly elevate levels of methamphetamine in the brain. It may look like shards of glass or clear-white rocks. Other, illegal forms of methamphetamine-usually in the form of a white powder-can be recreationally snorted or dissolved in water and injected.Ĭrystal meth is a solid, crystalline form of the drug. Adderall (amphetamine) and Ritalin (methylphenidate) are related FDA-approved drugs that have typically been used to treat ADHD in adolescents.
2 notes
·
View notes
Last Seen Blogs

lhyrihcah
Lowkie Fanart Reposter

zaian777
樂旬堂・坐唯杏<RakushunDining-Zaian>

twinpinestwinpeaks
Calvin “Ace” Klein

yev-atl
Visual Communication

anythingforn
Life sucks, then you die