#ICD therapy
Text
Guardians of the Heart: Implantable Cardioverter Defibrillators.
Implantable Cardioverter Defibrillators (ICDs) are sophisticated medical devices that have revolutionized the management of life-threatening heart rhythm disorders. This article provides an in-depth look at ICDs, including their purpose, how they work, who may benefit from them, the implantation process, and potential advantages.
Understanding Implantable Cardioverter Defibrillators:
Purpose:
ICDs are primarily designed to treat ventricular tachycardia and ventricular fibrillation, two serious heart rhythm disorders that can lead to sudden cardiac arrest.
They continuously monitor the heart's rhythm and deliver electrical shocks when abnormal rhythms are detected.
How ICDs Work:
Continuous Monitoring:
ICDs use leads (thin wires) placed in the heart to detect electrical signals and monitor heart rhythm.
The device can distinguish between normal and abnormal rhythms.
Intervention:
When a life-threatening rhythm is detected, the ICD delivers precisely timed electrical shocks to restore normal heart rhythm.
This rapid response can prevent sudden cardiac death.
Candidates for ICDs:
High-Risk Patients:
Individuals with a history of ventricular tachycardia, ventricular fibrillation, or sudden cardiac arrest.
Those at risk due to heart conditions like cardiomyopathy or previous heart attacks.
The Implantation Process:
Surgical Procedure:
Implanting an ICD involves a surgical procedure that typically takes 1-2 hours.
The device is placed under the skin, usually near the collarbone.
Lead Placement:
Leads are carefully threaded through blood vessels into the heart's chambers.
Proper lead positioning is crucial for effective monitoring and therapy.
Advantages of ICDs:
Life-Saving Potential:
ICDs can deliver shocks within milliseconds, potentially preventing sudden cardiac death.
They provide peace of mind for individuals at high risk of life-threatening arrhythmias.
Continuous Monitoring:
ICDs offer ongoing heart rhythm monitoring, allowing healthcare providers to assess the patient's condition remotely.
Improved Quality of Life:
Many patients experience reduced anxiety and fear of sudden cardiac events.
Increased confidence to engage in daily activities.
Potential Risks and Considerations:
Possible Risks:
Infection or bleeding at the implantation site.
Lead dislodgment or damage.
Inappropriate shocks in response to non-life-threatening rhythms.
REFERENCE:
TX Hospitals Group, Hyderabad is one of the country’s largest and fastest-growing chains of multi-super specialty hospitals.
CONTACT : 9089489089
Book an appointment now
#Implantable Cardioverter Defibrillators#heart rhythm disorders#ICD therapy#hospitals#health#procedures#surgery
0 notes
Text
just remembered how silly the diagnostic process was on the community centre i did my internship at. we literally sat in a room, someone presented each new patient and then they discussed it all together and agreed on a diagnosis for each person even if they didn't meet all the symptoms. only one of these people had ever seen the patient, exactly once.
#i mean it wasn't official diagnosis and the person usually wasn't told#but everyone had to be categorised based on the icd#which was stupid bc the people working there seemed to actually be fine#and it was free therapy so idk how much more they could do with tbe amount of people they got#just why that protocol in particular idk
5 notes
·
View notes
Text
What Vitamins Help Restless Leg Syndrome?
What Vitamins Help Restless Leg Syndrome? With causes And Codes
Restless Leg Syndrome (RLS) is a neurological disorder that affects millions of people worldwide. The condition is characterized by an irresistible urge to move the legs, particularly during rest or sleep.
RLS can significantly affect the quality of life of individuals who suffer from it, leading to disrupted sleep patterns,…

View On WordPress
#Alternative Therapies#Dopamine Dysfunction#Fatigue#Health Conditions#ICD-10#Insomnia#Iron Deficiency#Lifestyle Changes#Neurological Disorders#Pregnancy#Restless Leg Syndrome#RLS#Sleep Disorders#Vitamins
2 notes
·
View notes
Note
Oh great, everyone is all in on the ~all the kids who think they have DID are wrroooong~ thing.
Im sorry but none of you saying that are helping the community or plural folks as a whole. Even if you are also a system or have a CDD.
For DID *alone* the barrier to diagnosis is very high- arguably as high as Autism and according to one study it takes an average of 10 years in therapy to be diagnosed because so many doctors are ill-informed or refuse to diagnose it/believe it exists despite all the evidence due to the shadow of the satanic panic. The goddamn REASON people are diagnosed in their 30s and 40s isnt because you *need* to wait that long its because they look for horses before zebras and refuse to do anything else most of the time and fuck us over!!! Many of us report symptoms -the same fucking symptoms- since teen&young adult age or earlier!!!
The diagnosis has many of the same drawbacks of any other major diagnosis like autism and schizospec stuff where you can lose custody of children or the ability to adopt, face unofficial discrimination from doctors or employers or people you try to get accommodations from with it, and could even have your drivers license taken away or have to jump through hoops to keep it- and more issues!
Pursuing a paper diagnosis is not for everyone and the plural community for decades has been built on this- even before the exclusion criteria were added to the DSM and ICD that kicked a huge chunk of us of us off even getting one despite being systems (which is a good thing to be clear! If its not impairing or distressing it shouldnt be pathologized!). We have folk therapy and dyi resources and we have a lot of them for a reason.
And thats not even getting into how therapy has historically severely abused our community and how the only accepted treatment path is pursuing the fusion into one person (which has a hilariously low success rate that for anything else wouldnt be accepted as a vaild treatment) and not everyone wants that or is helped by that.
Most of us are never going to be ABLE see useful therapy or a paper dx, so we use the community to find resources and community and it FUCKING WORKS. We built our community with our own blood, sweat, and tears because no one else could or would fucking help us. And it WORKS.
Attacking these people who self-dx ONLY ever causes splash damage on the very people this kind of behavior claims to protect.
And like. If someone reports an autonomous entity that talks in their mind and takes over their body sometimes its... rather obvious they belong in the 'having an autonomous entity that talks in your mind and takes over your body sometimes' community regardless of anything else. NB4 people say psychosis; Schneiderian First-Rank symptoms are actually more indicative of DID than schizophrenia in this manner according to studies- but schizospec people with persistent personlike voices are known to benefit from the same exercises you'd do if they were ''''real'''' alters and are included in the plural community anyway (which btw doesnt require a dx- calling yourself plural or a system is not self diagnosing its an identity label the community created OUTSIDE of diagnosis criteria FOR this very purpose of self-ID).
While yes, we would agree many people say DID For Sure when they might want to hesitate there- we do NOT doubt they are plural. We just wonder if they were told the ONLY way they could be plural/a system is through DID and that is why they are saying they have it. Which... yeah thats not so great. HOWEVER informed self-dx is fine provided they havent been fed that kind of misinformation.
The solution there though is to just spread the real information about the breadth of plural experiences and people will feel less pressured. Simple as that.
Never EVER telling them its really just something else, you dont know yourself- you cant know something that extreme when something that extreme is EASIER to tell tbh because its such a unique and intense experience.
--
59 notes
·
View notes
Text
I briefly want to talk about why "proving your diagnosis" to strangers online is absolutely useless, and especially if you want to prove it to a stranger.
I'll use two documents I was allowed to upload.

What does this photo say or prove to you? Well, first of all, absolutely nothing if you don't understand German. And all my documents are in German. This is it in English:
"Diagnosis: Motor coordination disorder with dynamic equinus"
I don't even know how to translate this properly. It's not developmental coordination disorder, aka dyspraxia. It doesn't even have an ICD code. Doctors love not to use ICD codes when it comes to the development of disabled people where I live, they rather describe the symptoms. All it means is that I struggle with motor coordination, either due to brain damage or specifically because of my cerebral palsy. And that I limp (equinus).
But does it really prove that? No, all you know is that somebody took a picture of this document and uploaded it. It has no date and no name and you can't even see the name of the institution. Because you always censor that, that's basic internet safety.
Another one:

In English:
"You are applying for coverage of the costs of early intervention at the early intervention centre [redacted] for your above-mentioned child.
According to the medical opinion I have received, your child requires early intervention because of an imminent or significant disability."
If you know German law, you'll realise that this is an older document because they don't say "wesentliche Behinderung" anymore now. Alright. But does it tell you that I'm disabled and was in early intervention? Does it tell you that there are medical documents that prove that I have a significant disability?
No, it tells you that somebody uploaded a medical document. And that sensitive information is redacted. And you always redact sensitive information, that's basic internet safety.
I could be someone who has access to these documents, maybe because a family member is disabled. Or because it's my job and the document belongs to one of my patients.
It would be even easier for autistics who really were in early intervention and group therapies or special education, and therefore know many peers who "have it worse", so to speak. Maybe I'm friends with someone who's severely developmentally delayed, and they once sent me something that proves their significant disability. I could censor and upload that, and I could start roleplaying because 1. I absolutely know what their life is like and 2. I have the "proof" to back it up.
So what would really prove it?
I'd have to take a picture of an identity card or maybe even my disability ID card, and then I'd need to start a video call to show them my face and, again, my ID. That would prove that I am me, and that the documents belong to me.
And you don't do that with strangers, especially not internet strangers.
So you see, there's absolutely no way to reliably prove your disability to internet strangers.
Therefore, whenever somebody asks you to prove your diagnosis, just ignore them. You can't prove it. You just can't.
233 notes
·
View notes
Text
Tony is in his 50s and recently did a rough calculation of how much of his life he has spent looking at pornography. “The result was horrifying,” he says. It was eight years. “I can barely think about it. The sense of failure is intense.”
Tony saw his first “hardcore” film on VHS in the 1980s when he was 12. In his 20s, he connected to the internet for the first time, which turned his habit into a “full-blown addiction”. Over the past 30 years, he has just about managed to maintain a double life: he works in a caring profession, is friends with men and women, has had relationships. But there is a part of him he keeps entirely hidden.
“So far, I’ve only told three people in my life about it – two therapists and now you,” he says. “It’s a complete secret from everyone I have ever known. I’m meticulous about covering my tracks, even when in a relationship. My lack of interest in sex with my partner might be the only thing that would cause her to wonder.”
Tony has tried to stop looking at pornography multiple times, but has never managed more than a month without it. He’s tried cutting down, he’s gone cold-turkey – banning himself from masturbating and blocking porn sites. But “the addict brain is exceptionally devious and adept”, he says. He’s also tried therapy, but has found it hard to keep paying for it long-term.
Still, Tony is grateful for one thing: he was young before the internet. “At least I had a normal youth – parties, gigs, adventures with friends. I had girlfriends and a sex life. Boys like me don’t stand a chance now.”
Every statistic related to pornography use in the UK – and globally – is soaring, driven by the ubiquity of mobile phones. About 13.8 million people – a third of all adults using the internet – viewed porn online in May 2023 alone, according to Ofcom. Two-thirds of these were men. While pornography companies don’t report (or acknowledge) statistics on underage viewers, British children, on average, first watch porn at the age of 12. The children’s commissioner for England found in a recent study that much of what young people see is violent and extreme.
Jack is in his 20s and first saw pornography when he was nine. “I was with a group of friends on a school trip. It was a woman giving a blowjob, something I had never been told about in sex education.”
Like many children and teenagers today, porn found Jack before he went looking for it. “It came up through things friends shared, then on flash gaming websites. I saw really bizarre things which evoked both arousal and curiosity. That gradually turned into just arousal and then compulsion grew along with it.”
Soon, the intense stimulation of the pornography he was watching meant he “lost interest in day-to-day life”. It wasn’t so much the time he spent watching porn, but the “hyper intensity” of the content. “Sometimes in a particularly addicted phase I would spend hours watching it each day,” he says. ‘‘But usually it would just be an occasional binge then less use the rest of the time … In terms of how it was affecting me, though? That was not a normal life. The porn stimulus is intense and it leads to desensitisation to the small everyday pleasures that keep us sane and content.”
When Jack started having real-life sexual experiences, “it was very difficult to maintain an erection. Real sex was less intense than the masturbation of a desensitised addict – which is what I was”. Unlike online, “there was no option to click through many possible videos for something new and more stimulating.”
Both Jack and Tony describe themselves as porn addicts. Unlike other behavioural addictions such as gambling and gaming, pornography addiction is not included in the International Classification of Diseases (ICD), which is compiled by the World Health Organization (WHO). It is instead defined as a compulsive sexual behaviour.
Paula Hall is a psychotherapist who specialises in working with people struggling with their pornography use and has set up a private clinic dedicated to it in London. She has been an addiction therapist for 30 years – and started her career working with people with substance abuse issues. She believes it’s clear that pornography is addictive. “Porn use carries a risk of escalation and that is what hallmarks it for me as an addictive behaviour,” she says. “It’s a condition that causes significant suffering and we desperately need to develop resources for prevention and treatment.”
Peter Waddington is a counsellor with Relate, a charity offering relationship support, who is seeing more people with concerns about their pornography use. “Some people might be masturbating 10 times a day, up to three or four hours a go. They are physically in pain and sleep deprived. I see people who look unwell. The similarities to alcohol [misuse] are very strong … It’s also perceived as more shameful than gambling or alcohol,” he says.
“It’s helpful that it is now recognised as a compulsion by the WHO but we would like to see it classified as an addiction. If it was supported by the NHS, people could ask their GP for help.” As it stands, Waddington believes that shame can be a barrier to accessing help.
“There has been concern that by talking about pornography and sex addiction we are pathologising human sexuality,” says Hall. But, she insists, calling it an addiction is not increasing that sense of shame. “We know that alcohol is linked to violent behaviour, to coercive relationships, to heart disease, but people still enjoy alcohol. So we can acknowledge those potential risks without pathologising recreational porn use.”
Hall is finishing work on a leading study into British pornography habits with Leeds Trinity University. The aim is to help develop an online self-help programme. Out of the 193 people interviewed who felt they could not control their porn use, more than 93% reported struggling with depression. “Very worryingly, more than 40% say that, at times, they feel like ending their life,” says Hall. “In the same way that the gambling industry has been instructed to provide warnings and help problem users, the porn industry needs to do the same.”
Tony says: “I indulge in a compulsive behaviour that I feel totally unable to stop, despite severe negative consequences. I feel like an addict, I emotionally isolate like an addict, and I suffer the consequences like an addict. These websites are specifically designed to target addicts and keep them clicking.”
The algorithms that serve up new content for users “are incredibly powerful”, he says. “They tease out interests and kinks you didn’t know you had … You wouldn’t believe the number of mouse clicks you go through in a session sometimes. It’s not enough to watch the same few videos over again. It’s always more, more, more, new, new, new.”
Tony thinks this has made it impossible for him to commit to a relationship. “Porn tricked my brain into thinking I could have an endless supply of sexual partners. How does one partner compete with that? The version of me that isn’t porn addicted might have made a good husband and devoted father, but I became sexually bored and I always hid my addiction – I was never authentic.”
Pornography is often a factor in relationship breakdown, says Waddington. “For a lot of the guys I see, their partners have brought them in because they found out about secret porn viewing. Or they have become so addicted that they started watching it at work. So they need to change urgently – their world is imploding.” None of the pornography websites I approached for this piece wanted to comment.
Gunter De Win is a urologist who specialises in adolescent and paediatric urology and, each month, travels from his base of Belgium to London, where he is a consultant at University College hospital.
“Three years ago I started seeing more and more young guys coming in with erectile dysfunction related to issues with porn,” he says. “They need pornography to climax with a partner or to maintain an erection during masturbation. And they may have to watch many videos before they find one that turns them on. As a scientist, I wanted to unravel this.”
He is now part of a research group attempting to study the impact of pornography on young men’s sex lives. But, as his most recent report states, it is difficult to assess the impact that porn consumption has had on young men with erectile dysfunction as “it is more or less impossible to find a control group that is not using pornography from a young age and at the same time is not morally against its consumption”.
Teenage boys getting “performance anxiety is absolutely normal”, he says. However, De Win has seen young men concerned that they lose an erection during foreplay – which again, “is all normal”. But by watching porn so young, “they don’t understand the basics”.
De Win believes more research is needed into the impact of widely available pornography in the digital age. “Too much of the research on porn is biased either for or against,” he says.
Cold-turkey approaches such as NoFap, a US-based peer support network that encourages abstinence from pornography and masturbation as a recovery method, can have mixed results for young people, he says. “For some, going cold-turkey can be beneficial, but I see boys who end up with no sexual interest at all, which is also bad for their wellbeing.”
His solution is vastly improved sexual literacy – in sex education in schools and in the medical community – that does not condemn all pornography and masturbation as bad. “Introducing shame and guilt has consequences,” he says. For example, “if someone has a religious background and sees porn as taboo, then maybe this creates shame”. Shame, in turn, means that honest conversations around pornography do not happen.
“What I think might have steered me away from compulsive behaviour around porn might have been frank conversations with my parents,” says Tony. “My mother was extremely kind and caring but with an inability to communicate emotion. So maybe some of my tendency towards emotional isolation is just that I am my mother’s son? It’s hard for me to be sure what is really me and what is me corrupted by porn use.”
For now, nature is stepping in to help. “I’m in my 50s and my testosterone levels are dropping significantly, so that’s been a blessing and I am looking less at porn. I’m thinking now about getting help again,” he says. “But it feels like standing at the foot of Everest looking up at the summit.”
69 notes
·
View notes
Text
Kaiser, narcissistic wound and NPD



Tw: narcissistic personality disorder is mentioned, there is a lot of discussion on the topic of diagnosis. English is not my native language.
!Please take everything described below as my personal reasoning! If you need background information for yourself, then contact a specialist.
Note: This is a small addition to my post, where I discussed exactly what kind of psychological problems Kaiser might have.
In the original post, I mentioned that I consider a narcissistic wound to be more appropriate for Kaiser's background and current character, but did not explain what the difference is between narcissistic wound and narcissistic personality disorder*. So let's fix it. (*Next, I will use the abbreviation NPD.)
In fact, when it comes to psychiatry, everything becomes very complicated, because the correct diagnosis requires a lot of information, especially about the internal processes taking place in the human psyche. And as such, there is no difference in the internal dynamics between NPD and narcissistic wound, BUT.
1. NPD is a personality disorder, whereas narcissistic wound is a trauma of the psyche. The main difference is that NPD is not treatable, that is, a person with NPD can only learn to live with his disorder, but not get rid of it completely. Whereas narcissistic wound can be treated with therapy. (That's why I try to be very careful about the diagnosis of any mental illness, because it's really complex and without experience working directly with people, it can be very difficult to understand all the subtleties of the inner workings of the disease. Not to mention the fact that some mental illnesses are so similar in symptoms and external manifestations that they can be confused even with long experience. In addition, the diagnosis is often not limited to just one disease and it is very easy to get confused in this tangle. As far as I know, this is one of the reasons why there is no clear division into personality disorders in ICD-11* anymore, since they often mix. But this is a very complicated topic, so let's skip the details. In general: it is good to analyze and take information into account, and it is not good to hang labels using psychiatry as an excuse.)
*ICD-11 - International Classification of Diseases.
2. Narcissistic wound , in fact, is a transitional state between the "norm" and pathology, which is NPD. Despite the fact that narcissistic wound has the same internal mechanics as NPD (tossing between self-praise and self-flagellation; in the relationship between "I love you" and "I hate you"), narcissistic wound at the same time leaves a person with at least a relatively healthy psyche. What I'm talking about: having an NPD, a person is hardly aware of what he is doing. Personality disorders are therefore called personality disorders, personality disorder affects a person to such an extent that he does not realize his problem without outside intervention. His psyche is simply not capable of this, as it does not function normally and cannot function normally. Any personality disorder is very serious.
On the other hand, a narcissistic wound still leaves a person at least a little room for reflection, if his intellect allows it. It is easier for people with such a trauma to control themselves than for people with NPD, because their trauma does not hit their psyche so hard and fatally. In Kaiser's case, this is noticeable, because even without proper therapeutic help, he can relatively control himself, only sometimes breaking down to the state of "I'm a complete nothing." NPD makes self-esteem much more unstable, painfully unstable in the sense that almost anything can affect self-esteem in such a situation, no matter how insignificant it may be. Kaiser's self-esteem, while not being healthy, still has some stability and fluctuates only when he encounters something really more serious (a loss against Isagi). Plus, Kaiser is able to eventually accept other people's abilities (Noa, Isagi, Rin), which indicates that everything is not as bad as it could be and he is not alien to critical analysis and at least partially objective perception of reality and himself. (If a person has NPD, this is possible only after therapy and with a very high level of awareness.)
3. I did not find accurate information about this, but based on my knowledge, I can assume that if Kaiser had an NPD, he would hardly be able to "leave" Ness. Despite the fact that narcissists are not interested in the feelings of other people, they cannot give up love and attention so easily (after all, a black hole needs to be fed). A low-functioning narcissist can even commit a crime if the flow of incoming attention is cut off, but Kaiser does not seem to be so paranoid about this, which indicates the absence of pathology in the psyche.
A little off topic: Any personality disorder is very serious and people with such a disease can inflict injuries on others completely unconsciously, because this is how their psyche functions. But I insist that we should not demonize people with mental illness. They all need professional help and a lack of stigma around mental illness. This also doesn't mean that you need to tolerate bad treatment from these people. Anyone who hurts you has no right to do so, so in such situations it is important to understand that the problem is not with you and it is better to stop communicating if possible if it traumatizes you. Not everyone can be saved and you don't have to do it at the cost of your own health, it's not your area of responsibility. It is possible to be in a relationship with people who have any kind of mental illness, but it requires effort from both sides and an understanding that such relationships have their own specifics. You will save a lot of nerve cells if you don't try to reshape another person or yourself.

P. S. Thank you for the kind words under the post with Kaiser's analysis. I'm glad that this post found those who were interested in this information. Take care of yourself and your health, and do not encroach on someone else's. Best regards, your Shine.
#blue lock#bllk#michael kaiser#blue lock kaiser#bllk kaiser#blue lock analysis#bllk analysis#ssstar shine#shine's analysis
41 notes
·
View notes
Text
An Uncommonly Discussed Trauma Symptom

Disclaimer: This is in no way a substitute for therapy: it’s only psychoeducation. Please consult a therapist and/or hotline and get the help you need if you are experiencing mental health difficulties, especially if experiencing distress or issues that feel unmanageable.
Warnings: Mentions and discussion of suicidal ideation, death, abuse and violence.
Special thanks to @ashanimus and @childlikegoblinqueen
Ever heard of "the sense of a foreshortened future"?

If you have suffered trauma over a sustained and long enough period of time, you may find that you can't imagine yourself living long. You can't see yourself reaching milestones, because it hardly makes sense to your mind that you can go on for that long...given how much you have felt like you've escaped danger, given just how many close calls you have had in life.
Yet the sense of a foreshortened future is a separate thing from suicidality.
If you have both of those together though, it really isn't fun because they may feed one another in a cycle, in the way that symptoms under the same mental health condition have the potential to do the same.
It isn't a desire for pain to end (which is what suicidality is), more so a generated expectation that takes root, and a framework which a survivor tries to fit their experiences into, with the goal to get things to make as much sense as can be. Because it's often the easier thing to devise a simple formula, to feel certainty and to manage one's expectations: rather than embrace the grey areas of uncertainty about how life will turn out.
It's almost as if this feeling of a foreshortened future is in a tug-of-war match between what appears to be solid reasoning, and a person's natural survival instinct along with the hunger for a meaningful life.

This symptom isn't on the *official* criteria for a psychiatrist or clinical psychologist to make any diagnoses, it is not listed in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) or International Classification of Diseases, 10th Revision (ICD-10). But informally it is sometimes categorized as an avoidance symptom under both PTSD and Complex PTSD, and also under longer-term depression.
(however, I think it can extend to other conditions. The key criteria is it emerges from repeatedly experiencing horrible things until it makes sense in one's head to expect themselves not to last much longer)
If you hop onto Google Scholar to find proper research about it, the findings are very scarce because it's hard to define it, empirically measure it and quantify it in the first place.
Again, it's not the same as suicidal ideation because a foreshortened-future view is an expectation, while the latter is about a desire.
I wasn't taught about this symptom in any training and supervision before becoming a licensed therapist, nor did any of my own therapists bring it up as psychoeducation when I saw them. It was only through online articles on informal websites that I stumbled upon the phrase and it all clicked for my long-term experiences.
But I feel it is good knowledge for anyone providing psychotherapy to bear in mind.

In The Owl House, the grimwalker lore weaved into Hunter's arc, can shockingly be linked with this symptom, symbolically and thematically.
But the show's age rating means it would likely be too dark for the writing team to explicitly incorporate it into Hunter's dialogue.
Hunter was a lamb marked for the slaughter early on.
He has questioned his survival and ability to thrive.
The following article on Psychology Today describes Belos's long-term influence on Hunter pretty well and provides info that strengthens the points I'm making in this whole post:
Link
It's bad enough that before Hunter and Luz found Belos's mindscape, he struggled with the fear of failure to the extent that there was already the raging inner battle between his primal survival instinct and the already knackered part of him that sought eternal rest from his suffering (showing up as suicidal thoughts):


Fast forward a number of episodes...and we see the looming horrors in Hollow Mind that culminated in Hunter's discovery of what his predecessors went through:

followed by permanent rejection by his parental figure:


The power held by a foreshortened-future view, and its potential to isolate you - to make you feel like you're invisible, or a ghost - can be strong.
What Hunter said to Gus in the following screencaps sums up what it feels like pretty well:


In the context of having an abuser, it emerges from the negative beliefs they impose on you. It gets tricky if those beliefs are internalized, and which may remain internalized even after you get to safety and away from said abuser. Internalized until they become what you expect of your life.
It's about those thoughts which you know in your rational mind are lies, but you feel their apparent truth. They go more silent when you practice self-care but they return to try and reel you in again, and to a degree, they succeed in getting you to believe them all over again, before you renounce them once more.
Being in the C-PTSD Club along with Hunter, I personally experience the feeling of a foreshortened future as a voice deep down which almost always says that life feels too long and it therefore feels absolutely weird, like it doesn't make sense. Life feels too long, contrary to that commonly heard cheesy quote, "Life is too short to blah blah blah".
When I reached milestone birthdays like my 21st, it was confusing and made me irritable, feeling an itch deep down that I could not scratch.
The voice asks me why the heck I'm still around when it apparently doesn't make sense. It's a pervading feeling which can be pretty annoying, though I have it far enough in the background that it's like noise instead of being a source of distress.
It's not the easiest thing to explain this, but Hunter may have confusing thoughts creeping into his head like "Caleb didn't last long, why would I?" whereby such thoughts have a strange feel to them. They aren't exactly hard rules, nor are they distant enough that they can be easily brushed aside. Brain hurty, emotions spooky.
After the horror of this night:


I can definitely see Hunter wrestling with this symptom from time to time. No doubt. It was a major loss of autonomy and control that would significantly aggravate what was already brewing deep down.
I'm doubtful that the crew even established this on purpose (unless they actually consulted trauma experts and/or experienced mental health practitioners), but...this one symptom ties in with grimwalker lore so perfectly...it's hella fascinating that all Hunter's predecessors' lives (including Caleb's) were cut short. Prematurely.

They came with an expiry date set by their abuser: something very characteristic of this foreshortened future feeling, though not unique to survivors of abusive home environments (e.g. if you experienced natural disasters over many years, yet had a loving family, you could also feel like you may not live long). And Hunter's experience of seeing the grimwalker graveyard in Hollow Mind is a shockingly visceral and visual metaphor to symbolize a concept like this, which matches perfectly with his symptomology as a Complex PTSD survivor.
The battle for inner peace has a high price: it is ongoing, and extends beyond him being physically free from Belos. Because Hunter can't just trim away the Belos-related memories from his earliest years and formative years. He can't forget, but he can choose to give those memories less attention, and choose not to let them take the steering wheel in the long-term.

In my opinion, the possession scenes don't just portray the physical experience of an abuser returning to try regaining control or restoring the status quo of having the survivor in their grasp.
The scenes also represent the abuser's imprint upon the survivor that lasts beyond the duration for which Belos is present in Hunter's life. Belos is the kind of abuser that is so insidious that he knows he could leave some marks that outlast his directly physical presence, in the event that he meets his own end. He would have definitely thought about this. Leaving the kind of grisly reminders that won't ever technically fade away (not to be confused with how they can certainly "fade further into the background" via therapy, new positive experiences and the support of loved ones).
For example, the patterns of the permanent scars on Hunter look so much like the patterns on Philip's own face and body. When possessed, the markings were dark green, later faded to the colour of scar tissue once Belos leaves his body.
As we all know, it's hella sad to imagine Hunter having to look at himself in mirrors throughout the rest of his life. It was awful enough that he had the haircut-related panic attack.
If we tie all that back to the symptom of a foreshortened-future view: Hunter might be left with a spooky nebulous feeling (that will alternate between coming back to haunt him, and subsiding) that he too has some expiry date that is different from how the people around him naturally and confidently expect to live a substantially long life. As a cult survivor with C-PTSD, Hunter can't afford the luxury of those natural expectations.
I don't mean that he might plan a day in the future to end his own life, not at all. But he may have a strange ghostly expectation of how long more he has till his life may come to an end, and he wouldn't be sure of how this subconscious expectation came about.
The darker days of navigating the confusing mess of his complex trauma may feel like exhaustion from paddling and swimming to keep your head above water to breathe.

Speaking of water and drowning, plus the theme of sinking down vs. rising back up above the water surface...the fact that Camila jumped in to bring him back up, his friends helped to pull him out, and Flapjack passes new life to him...this is also some crazy powerful symbolism for surviving complex trauma.

Falling back on a support network, your "tribe", that won't abandon you.
My other Hunter analyses (link) go into more detail about his support network and why he needs it.
I was talking to a friend about all this: she has relevant lived experience and mentioned that poor Hunter would reach a milestone birthday and perhaps cry at least a bit on that day, maybe even during the birthday party: out of sheer confusion. The confusion would be silently screaming "But...this doesn't...make sense?". And he might feel confusing waves of darker emotions along with a strange sense of joy.
He may make a decision to start a family with Willow, and a confused questioning voice will bother him now and then with "How are you still here, doing this and living to see this?".
(...also, when is his birthday...? Is it documented in some Emperor's Coven records that they will find..? Even the mere concept of having a birthday is messed up for him to think about, given the purpose behind his creation)

Complex trauma changes its survivors' relationships with the world, not just with people, and this can even apply to their relationships with things like joy and how joy is experienced.
Flapjack's absence would have bred survivor's guilt. It might translate into Hunter questioning whether he is worth the love and effort his friends put in for him. This feeling could emerge at random moments over the years in his life.
Visually, I feel that these two frames - the lighting (which I'd say is unique among all his scenes because they are parts of his arc that stand out so much), his pose, his expression - somehow capture the experience of how complex trauma is chronic and long-term:


The currently most known C-PTSD memoir out there, What My Bones Know by journalist Stephanie Foo, has some content that I feel matches nicely with what Hunter is experiencing in the two separate scenes above.
The author describes something she calls "the dread" (if you get the book, it's first mentioned on page 51). I would call it the amalgamation of multiple things such as shame, the fear of impending harm, self-doubt where you question whether you did something wrong, fearing that someone hates you, etc.
And basically, good lord my poor boy in the first screenshot..with that expression of suspecting what he thought was Belos's presence in the room: something about it fits the book author's words, feeling like she was "on the precipice of fucking everything up".
That's certainly something that would cross Hunter's mind multiple times as he processes the worst night of his life. That he could have done something to prevent all that.
With so much pre-existing worry that his friends and family might actually hate him, the possession scenes and Flapjack's death would definitely shake his foundation and I'm sure he isn't past this kind of ingrained thought pattern at all:

Second, the book author calls C-PTSD a shapeshifting "beast" (page 316). And when she fights it, she must use a different strategy depending on what form it takes, and that it will keep coming back from time to time in another form. Which is why there is a particular exhaustion one feels from having to adapt to each battle.
For Hunter, the second screencap of him fighting Belos's coercion in a direct physical manner is the first of many battles he has to win in his mind, even after Belos is gone for good. Outlasting whatever invisible assailant is trying to get him, as he faces inevitable episodes of being retraumatized in the future: these are called emotional flashbacks (one of the symptoms of C-PTSD).
Being a survivor of complex trauma who experiences a weird sense of time via a foreshortened-future view, can feel like being on the outside looking in.
But! To end this meta on a hopeful note, I should reiterate something from my most recent long meta about Retraumatization vs. Self-Soothing, the first part of Hunter's important speech in Thanks to Them touches on wild magic and palisman. Wild magic represents freedom, while palismen (quoting the Bat Queen) represent close bonds in relationships, emotion, and conviction.

Applying this to how we can navigate the swampy waters of a foreshortened-future view, Hunter can use his newfound freedom and sense of agency to create the story he'd like to tell about his life. It is pretty much impossible to avoid bringing beliefs from our young formative years into adulthood. But expectations (which have a direct link with emotions we end up feeling) of ourselves and of life can be altered over time, so they become less rigid and instead more open to new possibilities.
He has an inquisitive mind which is a big plus point in understanding the impact of what he has been through, and I have full faith that he'll do just fine in that regard because of the courage we have seen in him.
Among the hobbies he explores in the future, flyer derby will be one example of an excellent outlet for him because of its physicality: trauma and grief are not only emotional battlegrounds but also highly physical ones. The body is also very much involved e.g. feeling the lead-like weight of depressive moods in one's body, feeling the physical tension of hypervigilance, etc.
It's fantastic that he has Luz, Willow, Gus and company, he will have a very meaningful career, and he'll have everyone else in his large found family.

His story...his heart...his resilience and vitality...it's all truly inspirational.
We might learn even more about the grimwalkers in the finale and that would undoubtedly prompt me to do a shorter Part 2 on top of this meta.
554 notes
·
View notes
Text
A Deep Dive Into Antisocial Mindsets
how does the mind of a person with aspd work?
First off, it's important to understand what ASPD is, so let's get a few things cleared up before we really dive into it.
Antisocial Personality Disorder is classified in the DSM-5 as a cluster B personality disorder, and in the ICD-11 as a "personality disorder with dissociality".
(Since I live in a country that typically uses the DSM-5 as a guideline and it has a set classification for ASPD, I will be referring mainly to that.)
It's described as "pattern of disregard for, and violation of, the rights of others", and characterized as a maladaptive* practice of antisocial* behaviours.
*Maladaptive: Behaviours that cause issues in someones ability to adapt normally to daily situations
*Antisocial: Behaviours that are antagonistic to social practices, rules, and/or expectations
A personality disorder is
characterized by deeply ingrained maladaptive patterns of behavior, thoughts, and emotions that deviate from the cultural norms and cause distress or impair functioning in various areas of life
The current criteria for diagnosing ASPD involves a reoccurring, ingrained pattern of three or more of the following (occurring from at least age 15):
failure to conform to social norms, as indicated by repeatedly performing acts that are grounds for arrest.
repeated lying, deceitfulness, conning others for personal pleasure or profit
impulsivity or failure to plan ahead
irritability and aggressiveness
reckless disregard for safety of self or others
consistent irresponsibility
lack of remorse, being indifferent to or rationalizing having mistreated another
To understand ASPD, we need to dig a little bit deeper than a set of symptoms. It is important to note also that antisocial traits and beliefs are not necessarily an indication of antisocial personality disorder.
"only when antisocial personality traits are inflexible, maladaptive, and persistent and cause significant functional impairment or subjective distress do they constitute antisocial personality disorder." - DSM5
Antisocial beliefs in ASPD are views about themselves, others, and the world that are heavily engrained into their thoughts, perceptions, and behaviours. Most importantly, these traits negatively impact the individuals life on a regular basis. They are dysfunctional and reoccuring. In the criteria for ASPD, these harmful behavioural issues must have been present in the individuals life from at least 15 years old.
Looking into what causes ASPD can help us further gain insight into the condition as well.
"child abuse or neglect, unstable or erratic parenting. or inconsistent parental discipline may increase the likelihood that conduct disorder will evolve into antisocial personality disorder." -DSM5
"...in the absence of a parent or other caring, involved adult, a child cannot internalize his parent's values, a necessary factor in the development of morality."
"in homes where no adult takes an interest in or expresses love to a child, the conscience does not develop and the individual fails to be socialized in this very critical way. It seems likely that this is at least one possible cause of antisocial personality. Another possibility is that highly inconsistent discipline and attention, even from the same person, prevents the child from forming normal values."
"This form of child rearing allows the child to grow up without a clear understanding of what is right and what is wrong. Behaviorists believe that individuals learn their behavior by testing behaviors to see which is successful. Studies have shown that people with antisocial personality disorder frequently have fathers with the same disorder, and the child often observes and mimics the father's behavior." - Drug Therapy & Personality Disorders
A very important factor in early years of development is being taught about the "social contract". Like any other animal, children learn by seeing, and doing. They are highly impressionable, coming into the world as a blank slate. Children look to their peers and primary caregivers for guidance on how to respond to situations, and how to view the world.
(It is believed that there is commonly a genetic component to ASPD, and the environment may either worsen the antisocial traits or teach the child how to cope/adapt in positive ways)
If a child develops in an unstable situation, they may internalize maladaptive behaviours as a way to adapt, or because they don't have any healthy guidance to challenge these beliefs and behaviours towards the world.
Studies show that people with ASPD are highly likely to have grown up in neglectful and/or physically abusive households. There is also a correlation with children growing up witnessing criminal activity and the development of ASPD.
This is a very important factor to consider when looking into the mindsets of somebody with dysfunctional antisocial traits.
If a child comes into the world with no clue how anything works, or what anything means, and the only information they're given about the world is harmful, they will uncritically learn and adapt to that information.
A key element of ASPD beliefs is self-preservation. This heavily connects to a history of neglect, as the child who had no stable caregiver will grow to not trust that others will be reliable. They may also grow to not know what a healthy, trusting, caring connection with others looks like.
Personality Disorders are often thought to be something of a defence mechanism. A maladaptive defence mechanism as a response to a stressful environment in childhood that remained unchallenged and unsoothed.
Another key feature of this is that antisocial beliefs are related to justification. This is directly mentioned in the DSM-5 criterion A.7
"being indifferent to or rationalizing having mistreated another"
It is important to note, however, only 51% of those with ASPD will match this criteria. This doesn't necessarily take away from the general idea that antisocial beliefs include a rampant chain of excuses and justification to brush off their behaviours.
"individuals with personality disorders often view their symptoms as consistent with their own self-image, or ego-syntonic, and not as problems that need treatment." - Drug Therapy & Personality Disorders
ASPD is characterized by a disregard for others, rules, and norms. A common belief in people with ASPD is that they are above consequences, and never in the wrong. They refuse to put themselves in a submissive position to others, which often manifests as refusal to follow rules, responsibilities, and expectations.
At their core, they fear being controlled, weak, and losing power/dominance in a situation. They often lack the care, self-control, and forethought needed to healthily adapt to situations that threaten them. To them, it is a dog eat dog world, every man for themselves, survival of the fittest.
If we view ASPD as a maladaptive defense mechanism, then we can understand better how and why they respond to situations this way.
Studies show that reactive aggression* and hostile interpretation* is heavily prominent in those with antisocial behavioural patterns.
*Reactive Aggression: Aggressive behaviour in reaction to a perceived threat
*Hostile interpretation: Interpreting something as hostile or threatening to them
This means that people with ASPD are more likely than the average person to view an ambiguous comment, situation, etc as hostile (regardless of whether or not it actually was), and more likely to respond to that percieved threat with aggression.
The child who grew up in a hostile environment may have developed a brain that scans for the tiniest sign of an attack, and responds as it sees fit. It bites back.
As stated before, self-preservation is a very prominent trait in those with ASPD, and it is associated with a justification of their actions. People with ASPD think and act based on a worldview that everything is a matter of power and control, being on top or being hurt, dog eat dog.
In those who have ASPD, they commonly find themselves unwilling to, or unable to, care for anything but themselves. They often lack an empathetic response to others. "Not my life, not my problem". They are typically very defensive and protective of themselves, and protective towards things they value, but wont experience or express any care, compassion, or empathy towards anything they deem 'unworthy'.
It is the persistent irrationality and the ingrained lack of healthy adaptations and reponses to situations that makes ASPD a disorder. And it's the aggressive/dominating responses to threats, and justification of their responses, that makes the disorder antisocial.
#info#aspd#cluster b#psychology#actually aspd#antisocial personality disorder#aspd things#cluster b pds#personality disorder#aspd awareness#aspd positivity
67 notes
·
View notes
Text
Reminder: System has been a shared community term since the 90s.
System has a broad usage in the field of psychology for referring to parts of a person, such as in internal family systems therapy. There is no solid medical definition that only applies to people DID and OSDD. Psychologists and psychiatrists studying endogenic and non-disordered systems are calling also calling them systems.
The World Health Organization's ICD-11 affirms the existence of non-disordered and endogenic plurality. Transgender Mental Health, written by Dr Eric Yarbrough and published by the American Psychiatric Association states that you can be plural without trauma. Endogenic systems have also been supported by experts like Dr. Colin Ross. Numerous studies into these other forms of plurality have been conducted and are being conducted as we speak. This includes an fMRI study into tulpa systems showing neurological changes during possession.
Relying on institutions to determine if you should support people's identities and believe their experiences isn't very "punk" of you, and you should respect people's right to self-determination regardless.
But if anti-endos do want to have this discussion, they should know that the doctors don't support them either.
The existence of endogenic and non-disordered systems is not up for debate.
The anti-endo position is not rooted in science or psychology. It's rooted in hate, bigotry, and internalized ableism.
And will be no safe spaces for hate and bigotry.
#syscourse#systempunk#syspunk#pro endogenic#pro endo#anti endogenic#anti endo#sysblr#multiplicity#psychology#psychiatry
49 notes
·
View notes
Note
Hey we've been thinking about that "OSDD was a temporary diagnosis" post for a while and. it makes complete sense what you guys said but like. we can't get ANYONE to diagnose us as anything CDD, let alone anything that isn't going to give us the treatment equivalent of slapping a bandaid on a stab wound. Is there like, anywhere we could look further into P-DID/DID research on the subject? We're not comfortable moving off of the self diagnosis of OSDD-1b yet so we wanna be triple sure to get as much information as possible.
Thankies 💕💕💕
- 🐑 & 🌸 of the Constellation Collective
There's places all over to find that info, but I want to encourage you not to overthink it. You can dig deeper, you absolutely should, but the label... it doesn't matter. It's really, truly okay to get this one wrong and switch around between the labels or use them interchangeably. I promise. You don't need to be right, because you're right regardless (unless it's a misdiagnosis, but I'm going to talk about that at the end of this, because it's important).
I am diagnosed OSDD, but I call myself DID. It's easy, I understand that there's not that big of a difference, no one is going to yell at us (me or you) if it turns out that we have the other one. We're not misrepresenting ourselves. If it turns out I would only ever be diagnosed with OSDD, that doesn't mean I was wrong using the DID label, or that I was even mislabelling myself.
Whether you're diagnosed with DID or OSDD largely depends on where you live. I made a post about this a while back but I can't find it. The US is more likely to diagnose OSDD with minor amnesia than the UK. They're more likely to call minor amnesia DID (as they should). It's literally a dice throw, and not that important.
To quote my BFF, Colin Ross,
The dividing line between DID and most cases of dissociative disorder not otherwise specified is arbitrary [or OSDD]. Most cases of DDNOS are partial forms of DID which lack either clear switching of executive control, full amnesia barriers between identity states, or clear differentiation and structure of identity states. They are partial forms of DID with the same patterns of childhood trauma and co-morbidity.
Also this quote.
So on the one hand we have a vast swathe of people who are, or would be, diagnosed with OSDD as opposed to dissociative identity disorder but who show almost all of the symptoms of DID. Many people therefore see DID and OSDD as appearing on a spectrum, and prefer to conflate the two conditions so that DID/OSDD represents a range of dissociative experiences with more or less amnesia and greater or less elaboration and distinctive identity states or parts of the personality.
It is also what happens in practice: very few people would realistically distinguish between DID and OSDD.
And,
Both OSDD and DID are the result of the spontaneous action of the brain in response to trauma. Both contain different self-states, holding shards of memory and ‘unformulated experience’ (Stern, 1997). Both can be helped by similar approaches to therapy which encourage neuronal repair and result in brain growth such as increased hippocampal volume. Above all, all forms of dissociation need to be validated for their unique contribution to survival.
P-DID is a bit of a new one. Here's the ICD link to it, if you want to read more, but it's going to be the same as above. It's really not that important. Its main difference is that the system doesn't really switch, it's mostly intrusion (like feelings bleeding between alters and host).
These are really only useful for describing how your system generally functions.
Finally, misdiagnosis.
It's okay to be wrong completely. Maybe it's just BPD or OCD, autism, any of the number of disorders that come with identity confusion.
When someone self DX something like BPD and they finally get to therapy and find out it's literally ANYTHING else, we celebrate with them. Good job, you found answers! You're on the right path! You can get the right kind of help now. You did what you had to do in order to get by, and you did your best to try to understand yourself with the tools you had. The use of the first label wasn't malicious, you didn't hurt anyone by using it, and you probably got yourself pretty knowledgeable on the topic.
You are now a resource for those who are also trying to figure themselves out.
Who knows better what the difference between BPD and OSDD is than someone who tried out both and found the answer?
Being wrong doesn't mean you're bad, I don't know why we don't celebrate a misdiagnosis of DID like we do some others. We're all just trying to understand ourselves, and sometimes we're wrong. The point is that eventually we figure it out, and the journey there... recognizing a misdiagnosis is a GOOD part of your story, and it's an important story to share. You were still struggling, regardless of what label you used and what you're being diagnosed with.
Use the label that feels right to you. If you want to keep using OSDD, that's fine. You're describing how your system works right now, and that's perfect. Using DID or OSDD, you'll end up in the same place regardless-- hopefully this means with a good therapist who's going to take your symptoms seriously, but you're going to end up in that same chair no matter what label you're using.
I really hope this helped.
Also, I didn't really touch on it, but I'm sorry you're struggling to get a diagnosis. That must be incredibly frustrating. Don't give up. Unfortunately, the average is about 5 years for most. Keep advocating for yourself.
#not syscourse#did#osdd#osddid#actually dissociative#actually traumagenic#actually did#actually osdd#pro system#system safe#CDDs first#pro endo#plurality#actually plural
33 notes
·
View notes
Text
How psychiatrists actually diagnose DID because the DSM is a manual not a diagnostic tool
Excerpts written by Paul Dell from Dissociation and the Dissociative Disorders: DSM-V and Beyond

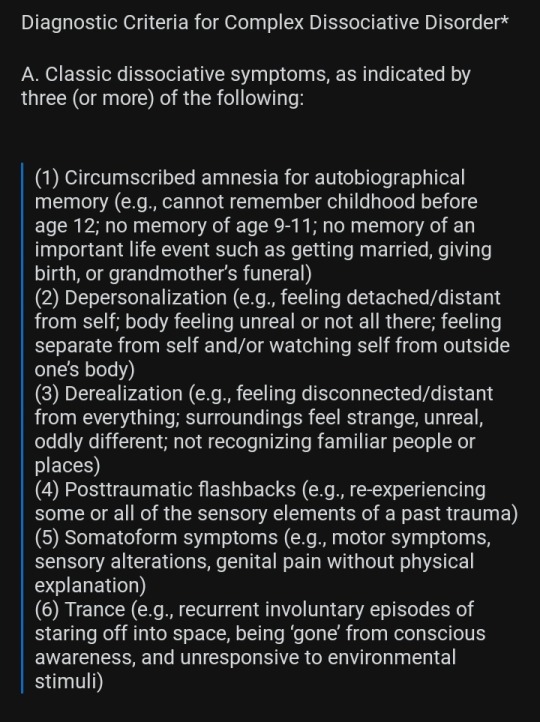
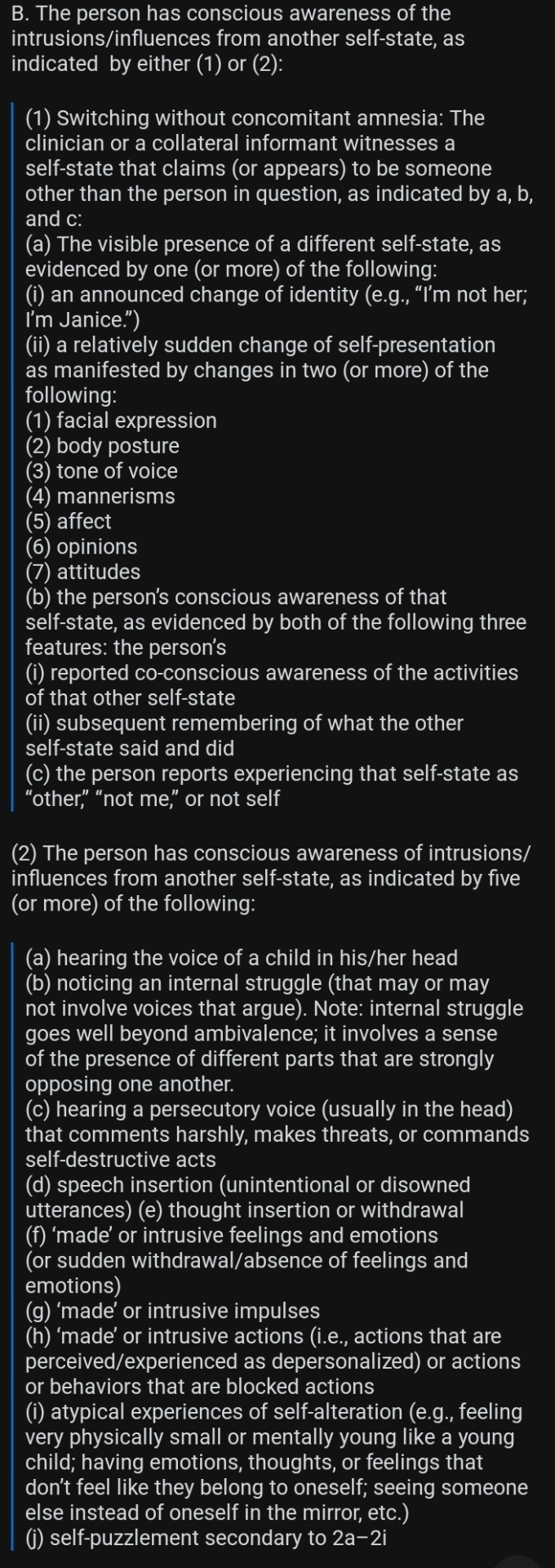
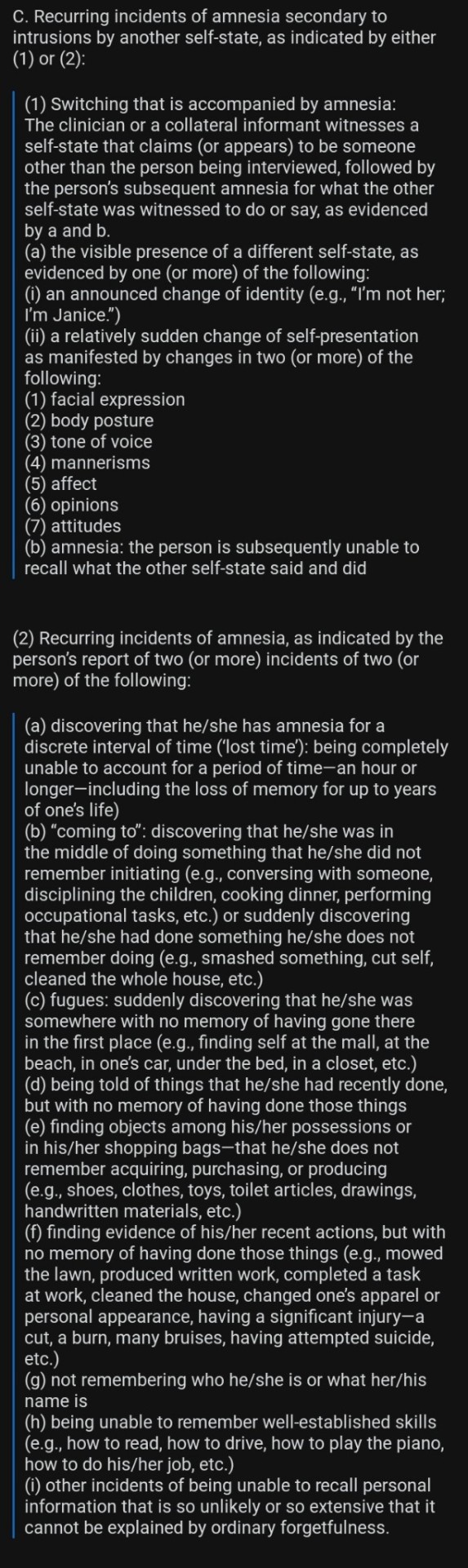
I am begging y'all to understand that "E. The symptoms cause clinically significant distress or impairment" applies to ALL of the symptoms listed. Not distress over being a system itself.
The DSM and ICD are not suitable diagnostic tools because they're a list of all the currently accepted disorders, for brevity's sake everything is condensed. Diagnostic tools that focus on a smaller subset of disorders are able to get into much more precise symptomology and phenomenology.
A successful diagnostic tool:
a) Can satisfy the criteria set out in the DSM and ICD
2) Is able to detect as many people with the disorder as possible (doesn't under diagnose)
iii) Is able to exclude as many people without the disorder as possible (doesn't misdiagnose)
And most importantly for DID) Is able to capture and identify the full range of patient experience (doesn't diagnose you with depression and calls it a day)

For instance, I know for a fact that my local psychiatric team use a tool that includes a possible diagnosis of BPD but not DID, so if I went through that assessment process I would get a diagnosis of BPD, whereas the MID can diagnose both (plus the other Dissociative disorders and PTSD).
DID is a really tricky thing to diagnose because it's designed to hide itself. The DSM criteria really only focus on the main most obvious and blatant symptoms and are therefore only useful in a minority of cases, the DSM-IV criteria used to require a switch being witnessed by a therapist for fuck sake lmao. Now I might switch in therapy a lot but my alters do their damned best to hide it when it happens. The disorder was hidden from me for a whole 25+ years, did I not have DID when I didn't know? I was just depressed and anxious right? How could I be distressed by alters I didn't know I had? I was absolutely distressed by my symptoms and damn was I relieved to find out I had alters to help with them but I still have DID, I always had DID.
And look, this isn't to tell anyone they're wrong about themselves or their own experiences, but the diagnostic criteria are not for US to interpret. They're for professionals to interpret and discuss and debate and refine to make sure they're actually doing their job properly.
So much of the bullshit in syscourse is just arrogant pedantry over ambiguity in definitions and for a lot of it, other much more qualified people have done it for us
54 notes
·
View notes
Text
Medical stuff I wish cisgender people knew
Medical transition does not make someone a man or a woman. A trans woman is a woman, and a trans man is a man, regardless of what medical treatment they have or have not had. Medical treatment just makes life a hell of a lot easier for a lot of people
It is not true that 40% of trans people commit suicide. The infamous 40% statistic refers specifically to rates of suicide attempts which occur before transition. Most of these attempts fail and the person survives.
Transition vastly reduces risk of suicide attempts from 40% down to around the national average, while dramatically improving mental health, social functionality, and quality of life for those who need it.
Being trans is not classified as a mental illness by either the American Psychological Association or the World Health Organization. Gender dysphoria (in the DSM) or incongruence (in the ICD) is recognized by both as a medical condition, and transition is the only treatment recognized as effective and appropriate medical response to this condition
When able to transition young, with access to appropriate medical care, and spared abuse and discrimination, trans people are as psychologically healthy as the general public
Transition-related medical treatment is not new or experimental; it has existed for over a century
Transition-related medical care is recognized as necessary, frequently life saving medical treatment by every major US and world medical authority
Transition is the only treatment for dysphoria that has proven to be effective. Attempts to "cure" trans people, alleviating dysphoria by changing the patient victims' gender identity to match their appearance at birth (aka "conversion therapy" or "gender identity change efforts"), are such utterly worthless and actively destructive train wrecks that this "therapy" is condemned as pseudo-scientific abuse by all major medical authorities
Transition is a very individual process; not everyone needs or wants the same things
"Regret" rates among trans surgical patients are vanishingly rare, consistently found to be about 1% and falling. This 1% includes people who are very happy they transitioned, and often are still glad they got reconstructive surgery, but regret only that medical error or shitty luck led to sub-optimal surgical results. That's a risk in any medical treatment, and a success rate of about 99% is astonishingly good. And only about 6% of trans people have had reconstructive surgery, so rates of surgical regret among trans people as a whole are about 0.06%.
Transition "regret" is vanishingly rare. Of everyone who starts even the preliminary steps of transition, like trying a new name or pronouns socially, only about 0.4% eventually realize it is not right for them (see p108-111). Most realize this soon after starting transition, when physical changes are minimal or nonexistent. Many do not regret exploring transition as an option, even if ultimately it wasn't what they needed.
Hormone therapy is pretty cheap, is generally the first line of treatment most trans people get, and dramatically impacts one's appearance
Most trans people socially transition long before they get reconstructive genital surgery, if they ever get it at all. Not everyone needs or wants surgery, and even those who do need it are often unable to afford it. Genital surgery for trans women costs tens of thousands of dollars out of pocket. Surgery for trans men can cost between tens of thousands to over $100k, depending on the procedure one is getting.
25 US states currently have laws prohibiting health insurance companies from having "trans exclusion" policies, where they categorically refuse to cover medically necessary transition-related treatment. This means that a small but growing number of people are able to get treatment, including surgery, covered by insurance
When a child or adolescent transitions that does not mean they are being rushed into irreversible surgery
Transition for predolescent children is 100% social; changing hair, clothes, name, pronouns, and/or the gender they are recognized as by their family and community. No medical treatment is necessary or provided before the start of puberty
The first line of medical care for trans adolescence is puberty-delaying treatment. It is gentle, fully reversible, and has been used for decades to delay puberty in kids who would otherwise have started it too young. It does nothing but buy time, and has no long term effects
Transition-related hormone supplements do not cause serious long term health problems
Reconstructive genital surgery for both trans women and trans men can provide excellent results
#gender equality#gender roles#gender bender#genderqueer#gender#gender stuff#queer stuff#trans stuff#pronouns#trans tag#thepinprick#pride#trans#pin#lgbt pride#pride flags#lgbt#queer#gay pride#pride edit#pride icons#ace pride#lesbian pride#mogai pride
390 notes
·
View notes
Text
Little disclaimer about endo “syscourse”. Mild TW!for brief mentions of $H and Su1cid3
Okay, as an anti-endo system one thing we feel the need to address about “syscourse” is that when people say they’re anti endo or try to educate someone, that is not anyone trying to invalidate anyone’s experience. It’s just when you claim a trauma disorder can form without trauma and then go around spreading misinformation it creates a stigma around the disorder that impacts so many people with dissociative disorders, even if they’re not part of a system.
Your lived experience ARE valid, HOWEVER, there are other explanations for what you’re experiencing, a lot of which don’t require trauma. It’s okay to be wrong but it’s not okay to create a stigma around already heavily stigmatized disorders and mental health conditions. Even when it comes to things like IFS therapy, there’s an important distinction that it’s not the same as an actual system, yes the parts are valid and real, but nowhere near the same, and in all honesty just because the s stands for systems, doesn’t mean using that terminology and other terms created for/by systems doesn’t do genuine harm.
The first people to popularize the concept of having this disorder without trauma were not professionals, one of which had the disorder but denied it and refused to take any treatments, and the other didn’t have it but claimed he did because he had some dissociative symptoms, even though you can dissociate without trauma and have some other dissociative disorders without trauma(some require trauma, some don’t, but for all o them it’s more likely to be developed with it). Both of these people created very dangerous stereotypes about systemhood, both encouraging the stereotypes we are dangerous, and just spreading a lot of misinformation and even encouraging su1cid3 and $H. Additionally, tulpamancy and religious beliefs are not the same as being a system. The DSM (and I believe the ICD as well) specifies that. So please stop using system terminology or claiming to be one without trauma, your experiences are valid, but that doesn’t automatically make you a system. Please do some research.
With that said, any repeated or prolonged trauma is “enough” to form the disorder, and it doesn’t need to be super severe on the brink of death abuse or anything like that. Medical trauma is a valid, emotional abuse/neglect is valid, sibling trauma is valid, your trauma is valid even if it “wasn’t that bad”. It does need to be during formative years to form a system, but what you went through, no matter how old you were is still valid, and no one is trying to say it isn’t. It IS possible you don’t remember your trauma, but dont force yourself to remember it without professional help, and don’t claim to have a trauma based disorder until you’re sure you have trauma.Thank you for your time reading this.
also this is the one post we’re not putting anti endo tags, outside of this post and conversations that may stem from this Endos please DNI.
#autistic system#system stuff#system#osddid#did osdd#osdd system#actually traumagenic#disclaimer#psa#feel free to add on#feel free to ask questions#information#this has been a psa#important psa#thank you#thank you for your time#thank you for reading#unsure what to tag this as#syscourse#traumagenic system#actually a system#systempunk#education#educate yourself#educación
33 notes
·
View notes
Note
Please note I have only taken a few psych classes cause I was required to in college, but I have always seen disorders in the DSM like adjustment disorder or prolonged grief disorder as something to get insurance to pay for therapy because at least my insurance in the US will only cover my therapy if I have a diagnosis... is that wrong though? Are they actually trying to make greif a pathology?
it's the other way around- the dsm (or diagnostics in general) does not exist/modify itself because of insurance, insurance bills based on the widespread belief in psychiatric research + practice that there is a meaningful split between "normal" and "pathological" behavior which can be categorized into illnesses which are meaningfully distinct both from one another + from "normality" (exemplified by the dsm).
even if some therapists no longer abide by this belief, it is still the dominant narrative in psychiatric research. insurance requiring you to medicalize your own pain in order to be given access to healing is a problem that should be addressed directly, not by inventing more and broader ways to be 'sick'. if we're literally inventing disorders now just to get people access to therapy- that's a huge problem + not something we should settle back into + accept. to its credit, even the icd (medical dx book for insurance) has codes that essentially mean "no illness or disease here, just a need to speak with a physician".
to be clear (which i think ppl were not getting from the post i made)- there is no grand conspiracy to like... cover up grief or delegitimize pp due to covid. i do think that researchers for prolonged grief disorder do genuinely believe that they are helping increase access to healing (which may be true but at the cost of medicalizing grief) + that identifying a 'disordered' form of grief is somehow empowering or healing for ppl. what it does is further construct a cold (western-based) narrative that there are 'normal' + 'abnormal' ways to experience grief, that there are forms or intensities of grief which are a sickness (that is, a problem within to be solved or cured), that there are right and wrong ways to grieve. it stems from such a myopic, medicalized, neoliberal view of the world that someone whose life is permanently altered by a devastating loss is seen as a disordered object to shift onto the 'proper' track of grieving.
at the risk of getting too personal, because i've been thinking abt this a lot since losing my brother- criterion for this disorder include identity disruption, intense emotional pain, loneliness, and difficulty reintegrating into life. one of the worst parts of grieving in the US is the culture's rabid obsession with you getting over it as soon as possible w/o letting it affect you in any meaningful way. you have to get out of the house, get back to normal, don't let it drag you down! my dad said to me the day after my brother died "we can't let this change the course of our lives". the absolute arrogance + cruelty of implying that it hasn't already changed. that my identity isn't forever changed because i was a sibling + now i am not. now i am something different. of course i am lonely. of course i am having difficulty reintegrating into life. of course i am in intense emotional pain. i wrote that post before losing my brother + now it just feels like another manifestation of the unspoken cultural mandate that grief be contained, efficient, unimpactful.
tl;dr the insurance benefits may or may not be there, but this misses the larger issue of how insurance functions this way due to psychiatry's obsession with diagnostics + will ultimately serve to draw even stricter boundaries around acceptable/unacceptable grief, isolating grievers + severing their pain from a communal context
222 notes
·
View notes
Note
Google isn't talking to me so you're the only person I can ask, I'm so sorry-
Is it possible to have NPD, APD, BPD AND HPD at the same time?-
It's honestly complicated. You know, personality disorders, particularly those within the same cluster, often share multiple traits at the behavioral level, such as attention-seeking, unstable personal relationships, and violent outbursts. However, similar behaviors can stem from very different motivations. For example NPD might act aggressively to dominate their partner and maintain their ego, while someone with BPD might exhibit the same behavior out of a fear of abandonment. What should technically allow for differentiation between disorders is their core mechanisms that underlie everything going wrong. However, in my opinion, this is largely a theoretical concept because the core of the psyche is interpreted differently across psychological paradigms. That's partially what makes diagnostic procedure so difficult. Also there are for example multiple studies about "BPD in men" or "APD in woman" which only showcases that classification is not carved in stone as symptoms can differ across other categories like gender. At the group therapy I encountered very few people with a single diagnosis. In the majority of cases, it was "XPD with traits of YPD" because fitting neatly into one prototype is not easy. Also DSM V is only one of available classifications, ICD lists like 5 more specific personality disorders.
What I'm saying is that the labels we use are the flawed results of statistical cluster analysis, and it's not uncommon for someone to exhibit traits that span across multiple clusters. In cases of someone showing traits from three or more personality disorders I would just describe it as mixed personality disorder or unspecified personality disorder, ICD style.
21 notes
·
View notes
Last Seen Blogs

pingobeshifting
Penguin Master


raffe242
Raffe FKA Jeffery

dmnaveen
dmnaveen

faketypefan
✮❀The Simp❀✮