#bpd + ptsd + osdd culture
Note
bpd , ptsd + osdd culture is, "we just failed a social interaction with our mom & our fp is leaving for their 1 month "their partner/fp is visiting them" thingy and now i, the depression holder, have to do Host Things , WHILE JUGGLING our episodes , ddrowning ourrsselves in sstudying AND battling inttrussive habitss of sself harm for a month . i'm going to derail a ffucking train ! into ! the pentagon !!! Kill Me Now ! Please ! Just Strike Me Down with the Force of God ! ( please don't . jusst make me not a wombo combo ssymptom holdder . please )
—⭐🌊🐾 (or well , tthe ssad boy from that anon'ss ssystem. oopss)
.
#i'm sorry op :(#bpd + ptsd + osdd culture is#bpd + ptsd + osdd culture#bpd + ptsd + osdd#borderline culture is#borderline personality disorder#bpd#bpd culture is#bpd culture#bpd safe#actually borderline#actually bpd#bpd fp#fp#fp bpd#ptsd#post traumatic stress disorder#osdd#osdd system#actually osdd#actually ptsd#- ⭐️🌊🐾
15 notes
·
View notes
Text
Alexia's Mental Health Headcanons
Hi! This might go without saying, but I am 100% talking about sources and the thing introjects are based off of. Just a disclaimer!!
MLP
Pinkie Pie - ADHD hyperactive type. She is super hyperactive, has trouble focusing on things without an incentive (which can increase dopamine), etc. I headcanon that she uses baking and party throwing as a way to express the individuality that comes from being ND and having ADHD.
Rainbow Dash - BPD and her fp is her pet Tank. Rainbow Dash, with as much as she loves winter, tried to stop it to keep Tank from hibernating. She's also insanely impulsive and has some self destructive habits that are common with BPD.
Discord - BPD, and his fp is Fluttershy. Okay. Discord is literally the embodiment of BPD, in my opinion /lh Fluttershy invited another friend to the Grand Gallopping Gala and he got super angry and felt like she was leaving him. Similarly, he has self destructive behaviors, an unstable sense of self (in my opinion), is impulsive, and is emotionally unstable.
Glitter Force Doki Doki
Princess Marie Angellica - DID. This is according to the core theory, which we do not believe in due to the reason I headcanon her this way. The core theory doesn't have a reason as to why systems can't form past childhood, to my knowledge. In my headcanon, she split her identity into Natalie, Regina, and Dina. The show said that after King Mercenair took over Splendoris, the Princess was insanely stressed and probably traumatized over having to imprison her father. There was the part that was loyal to him, Regina, and the warrior meant to protect, Natalie. She split them into two and decided fate would decide who would win. Her physical form turned into Dina. Anyways, I think this would represent DID really well because they end up as the actual heroes.
Regina - A persecutor (reformed at the end) of the Princess' system and she has BPD, her fp being Maia. Regina has an unstable identity of who she is, is impulsive, has suicidal idealation, and a severe abandonment fear from Maia. She does also fight against the Glitter Force in the name of King Mercenair, her father and cause of the system, and I think a lot of systems can resonate with having alters who are loyal to the abusers and hold their ideaologies (we do, anyways /lh).
Nathalie - A syskid and protector of the Princess' system, as well as an ageslider. I also like the idea of her being a subsystem with Glitter Ace. Her appearance and age varies greatly when she is transformed vs when she's not, and she was also formed to continue to fight against the King. She is 9 or 10 in the show, I think. I also think her being so mature "for a syskid" could stem from the Princess being a princess and having to be responsible at a young age because of that.
Winx Club
Musa - An OSDD-1b system. She doesn't show any sort of symptoms in source, and it's of course never mentioned, but I still like the idea as if she did show any symptoms because it'd be good representation. She had repetitive childhood trauma that I personally think would better suit OSDD-1b instead of OSDD-1a or DID.
Bloom - PTSD from being targetted specifically so frequently.
Riven - has anger issues.
#did system#osdd system#did alter#did osdd#dissociative system#osdd#osdd community#osdd support#osdd things#trauma#bpd favorite person#bpd feels#bpd tag#ptsd culture is
9 notes
·
View notes
Text
ROTTMNT HEADCANONS BECAUSE I WATCHED AND LOVE THIS SHOW AND AM HYPERFIXATING AGGRESSIVELY ON IT NOW:
They keep the surnames of “Hamato” despite abandoning the strictly traditional practices of the Hamato clan whilst also taking more eclectic inspiration from their arts to their own.
They all brumate btw. Pry this from my cold dead hands. Every time brumation season comes, the Disaster Twins Inc. hog the couch.
Donnie, because he’s autistic and is a softshell turtle, has sensory issues and is very picky about what food he eats and which clothes he wears, as well as what surfaces he touches. He secretly has a casual list catalogued about what sensory things he loves versus what he hates, and there’s a small area in his lab that’s sensory heaven for him.
All the turtles have different eye colours. Leo has natural heterochromia, one eye being cobalt blue and another eye being bright amber. Post-movie Raph has heterochromia from being turned into a Krang zombie for a short amount of time- one eye is emerald green, and another is a bright magenta purple. Donnie has warm brown eyes, and Mikey has baby/cornflower blue-ish grey eyes. April has hazel green eyes.
Teenage Mutant Intersex Turtles, anyone?? They’re all different variations of intersex on the intersex spectrum. Leo was presumed to be a guy and does have some male traits, but is biologically female- he’s both intersex and a trans dude (and I’m all here for it).
Raph is an aroace bigender (both transfem and demiboy), Mikey is genderfluid and greyaroace pansexual and panromantic, Donnie is nonbinary, asexual and greyromantic biromantic, and Leo is FTM trans, demisexual and gay (did I mention they are all intersex).
Yes I do headcanon disaster twins, and that Donatello was taller than Leonardo when they were younger but Leo is 3 and a half minutes older than Donnie and takes every damn opportunity to brag about it.
“We need CaCa and Maggie~!” “JUST SAY CALCIUM AND MAGNESIUM GODDAMNIT-”
In the future, all of the turtles have cloaking brooches and stable jobs that earn them great income. They also have apartments close to the sewers that is their home.
Okay, we all know Donnie’s canonically autistic. But what if all the turtles are on differing parts of the spectrum. More at 5.
Donnie in addition to being autistic has insomnia, BPD and misophonia and does have sight issues and is prone to migraines due to staring at screens and not getting enough sleep, Raph has panic disorder, dyslexia, OSDD-1a and GAD, Leo has ADHD-I, autism, GAD and is bipolar, and Mikey has ADHD-HI, dyscalculia and autism. All of them have some form of PTSD post-movie.
Leo does know how to play chess please and thank you. He just does it for fun and doesn’t really practice.
Splinter has PTSD, is autistic and is bisexual (the most unrealistic thing is young Lou Jitsu/Hamato Yoshi in his 20’s NOT kissing men and enby hoes in addition to women). He’s not a bad father, he just passed some of that generational trauma of everything that’s happened to him, as well as his regrets and grief, down to his kids without even knowing and feels terrible about it once he realizes. He may have made so many mistakes as a father, but he deeply loves his sons beyond what they could ever comprehend, and he’d send anyone to the shadow realm if they laid a finger on his beloved turtle children.
Donnie and Leo (mostly Donnie) bite each other for no reason at all- not enough to hurt or draw blood, but enough for the bitten to yelp and want an apology from the one who did the biting.
April O’Neil is an also autistic lesbian polyamorous demigirl. She’s saving up enough money by working at The Foot shoestore partially for her top surgery. Sunita is her best friend soon-to-be girlfriend. They’re gay disasters your honor.
Cassandra Jones is MTF trans. Fight me on this one.
Sunita, despite being a teenage slime yokai, does celebrate and participate in Indian culture and does consider herself Indian (let me have my rep I’m starved of please). She’s also a lesbian demigirl, and is asexual and autistic. She also has the ability of superhuman bodily elasticity, even in human form (though it is restricted somewhat in human form). Sunita WILL call pilaf ‘biryani that needs therapy’ okay, she’ll fight you if you say they are the same thing.
Queerplatonic/non-romantic Apritello where they have a super close relationship greater than best friends but cringe at the idea of being in a romantic relationship together wya <3
April’s African American, we all know, but what about her being of Afro-Iranian Jewish descent and her mother’s Shakshuka and Latkes and Rugelach and Sufganiyot being her absolute favorite among all the stuff she makes. She gets MAJOR hyped by the time Hanukah comes around and tells the Turtle boys and Splinter about it.
And there’s more, but I’ll tell y’all about that later, or we’ll be here all day.
#rottmnt#rise of the tmnt#rise of the teenage mutant ninja turtles#rise donnie#rise leo#rise raph#rise mikey#rise april#rise splinter#rise sunita#rise cassandra#LGBTQIA+#queer#Yoshi Hamato#disaster twins
45 notes
·
View notes
Text
📌
bodily 21, white, ablebodied, perisex/altersex; collectively queer, nonhuman/trans/nonbinary/aspec-heavy. apart from facets we identify as different people
anxiety, depression, autism, ADHD, OCD, (C)PTSD, phobias, delayed sleep-wake phase disorder, psychosis (symptom), BPD; considering other PDs/dissociative disorders
dni
- racist, ableist, misogynistic, etc (obviously)
- harass ppl over fiction
- think kids/animals can consent
- any sort of transX/transID/radqueer. not only dni but seek professional help
- queer exclus
- pro-endo, think DID/OSDD doesn't require trauma (literally just do research on complex dissociative disorders, stop using tumblr as a source for nondisordered plurality & pick up a textbook. yes cultural plurality exists but its still traumagenic and most endos arent part of those cultures)
frequently active (not all active members)
Aspen (they/th3m/thxirs, spi/spider, li/lims/liminalself) host, tied to front (does not have individual memories, only shared)
Oliver (he/sun/fag)
Blue (they/5h3/h3/rawr/XD/ze/paw/plur+etc)
Rye (he/they/vamp)
Wilt (he+gore-themed neos) asocial anger holder
0 notes
Text
Guys, I just had the best idea ever while sitting and eating raw cereal.
TW//mention of mental disorders (not in detail though)
What if there was a game developed, where Neurotypical ppl got to live a day in the life of a person with mental disorder (maybe mental illnesses too). Like maybe they would pick one or multiple and start the game, things such as ADHD, autism, PTSD/ C-PTSD, OSDD/DID, Anxiety, personality disorders, ED's...etc.
And they get to live through a day(maybe mutliple days) where they expirence stuff from the disorders in the game and they also deal with ableists and shit and everything a Neurodivergent person (maybe even ppl struggling with mental health). And the whole thing just shows them how much stuff we go through, esp self-diagnosed ppl or ppl who live amongst way too many ableists.
The game would be developed by ND ppl and therapists and psychiatrists to make it as realistic as possible.
~Elijah
#neurodivergent#adhd#autism#ptsd#complex ptsd#adhd culture#autism culture#anxitey#personality disorder#osdd#osdd1b#osdd 1a#didosdd#bpd stuff#eating disoder mention#random idea#osdd system#did system
135 notes
·
View notes
Text
Me: I feel like shit idk why
My body: get some sleep for once
My body: eating cereal does not suffice for a full meal
My body: take a walk
My body: calm your nerves down
My body: Get some sun
My body: and maybe take showers more often
Me: Welp, guess I'll never know. There are some anomalies that modern medicine cant decode.
My body: OhmygOD
#actually dissociative#did osdd#dissociation#dissociative alters#dissociative identity disorder#dissociative system#ptsd#childhood ptsd#did system#did#autistic experiences#autism#autistic blogger#autistic culture#actually autistic#executive dysfunction#neurodivergent#borderline pd#bpd#bpd feels#bpd thoughts#mental illness#mental health#humor#meme#dark humor
28 notes
·
View notes
Text
New Pinned Time ^^
Eyo, we’re the Controlled Chaos Collective,(perviously known as the bee hive system) we’re a multigenic collective of 100ish known members (system reset set our number waaay back) and we grow pretty frequently! our collective pronouns are ze/zir/zirself, and we all respond to Niv or Nivison ! (pls ignore the varying typing styles, we’re soupy) Please read below for our DNI, more info, request info, and our tagging system!
Request Status: Closed
okay, we in? let’s go!
DNI
Anti-endogenic systems, sysmeds, transmeds, TERFS, Pro-ship, anti-mogai, anti-neopronoun, NSFW/K!NK blogs, make fun of “animesexual”/any other mogai sexualities, anti mspec lesbians/gays, exclusionist of any type, believe in cringe culture, regularly hate on DSMP/MCU (criticism of bigotry is a-okay, harassment towards real people is not.), (NO)MAP, anti-kin (yes, that includes fact-kin), make fun of triggers (no matter what they are), anti-chronosian
More info about us !
System Name: The Controlled Chaos Collective/The CCC
Collective Pronouns: Ze/zir/zirself, they/them aux
System Origin: Multigenic
System Modifiers: OSDD, Mixed, Introject Heavy
Chrono age: Minor, 13+ (we are age dysphoric, please avoid bringing up age related topics)
Intra-age: 19
Date of discovery: Sometime October-January 2019/2020
Headcount: 70+ known members, we usually say infinite due to constant splitting & possible gateway
Frequent fronters: Niv, Adaine, Libby, Brennan, Philza, Kai, Lila, Stormi, Fig
Body conditions: Prof Dx hEDS, PCOS, POTS, PTSD, MDD, GAD, ASD, ADHD, BPD, PNEE, Tic Disorder not otherwise specified
Suspected C-PTSD, OSDD-3, & MCAS (these are subject to change)
Special Interests: Health science, animals/zoology, dungeons & dragons
Current hyperfixations: D20/Fantasy High/Unsleeping City/Misfits & Magic/A Starstruck Odyssey/Dropout TV
General Interests: Video Games (Nintendo, Minecraft, Bugsnax, etc), RTGame, Markiplier, Marvel Cinematic Universe, Atypical, Heartstopper
Requests
We do take requests on occasion! we will make moodboards, coin mogai + plural terminology, make mad pride or plural flags, make user boxes, or do mogai headcanons characters! we are not currently doing stimboards due to an issue with our computer!
Sideblogs
@geos-hive - sideblog for fandom and aesthetic stuff !
@endzonedragon - End’s blog, mostly trendercore + minecraft stuff
@thedaydreamers-cave- Ezzi’s blog, mixed bag of it’s hyperfixs + daydream stuff + mogai
Our Stuff!
Our picrew- https://picrew.me/image_maker/1219235
Our carrd-
System Twitter- @/ControlledCC
System Tiktok- @/bee_hive_sys
System Instagram- https://www.instagram.com/bee_hive_sys/
System Pronoun Card- https://en.pronouns.page/@thebeehivesys
System Carrd- https://controlled-chaos-collective.carrd.co/
Tagging
🐽- Techno’s sign-off (he/they)
🪒- Volt’s sign-off (🔪/🔪s)
🎸- Wilbur’s sign-off (any prns)
🌷- Niki’s sign-off (she/her)
🔷- Ezzi’s sign-off (he/she/it/they)
💜- Kate’s sign-off (she/her)
🔮- Adaine’s sign-off (she/they)
📚- Kristen’s sign-off (they/them)
🪦- Fig’s sign-off (she/rot)
💼- Riz’s sign-off (he/it)
⚔️- Fabian’s sign-off (he/they/it)
☮️- Esther’s sign-off (they/she)
🥁- Gorgug’s sign-off (he/him)
🦎- Delvin’s sign-off (he/she/they)
📝- Libby’s sign-off (she/her)
⚖️- Brennan’s sign-off (he/him)
🏐- Aabria’s sign-off (pronounfluid, they/them default)
6️⃣- Barry Syx’s sign-off (he/him)
🐰- Cinna’s sign-off (he/bun/pup)
🎬- Lou’s sign-off (he/him)
💰- Margaret’s sign-off (she/they)
💧- Riva’s sign-off (they/them)
🏹- Clint’s sign-off (he/they)
🕸- Nat’s sign-off (she/her)
🔬- Peter’s sign-off (he/him)
🚽- Micheal’s sign-off (he/him)
🛡- Yelena’s sign-off (she/it/they)
🌺- Viv’s sign-off (she/it)
❓- Blurry sign-off
🌻 -Niv’s sign-off (ze/zir)
🌧 - Kai’s sign-off (he/it/ghost/monster)
🍎 - Lauren’s sign-off (any prns)
🐁 - Kathryn’s sign-off (pup/toy/hug)
🦄 - Serenity’s sign-off (she/any)
#rb - reblogs, mixed bag of things
#asks - any asks we respond to!
#plural - all things plurality related
#mogai - all things mogai related
#chronic illness - all things chronic illness and cripplepunk related
#ccc rants a lot - various rants, often about random childhood memories that suddenly broke through amnesia or just all of our thoughts
#emoji - emojis, mostly reblogs
#is this a shitpost? - potential shitposting
#our terms - terms we’ve coined!
#dsmp dump - all DSMP things
#nhie posting - all things Never Have I Ever
#mogai headcanons - all the mogai/mad pride headcanons we’ve done!
#posi tag - positivity stuff !
#tw syscourse - filter this is you do not wish to see syscourse. we do not engage in arguments, but we do occasionally post syscourse opinions (we are very pro endogenic and parogenic systems, nothing will be hate directed at these groups)
#tw (insert thing here) - how we trigger tag, we tag most basic triggers, you can ask for anything to be tagged if needed! We cw food instead of tw. we do not tag queer, caps, or any of our special interests (including dsmp and mcyt)
That’s all for today folks, hope you have a good timezone!
81 notes
·
View notes
Note
How do you feel about endos? Just curious.
Oookay, Riku will probably never get around to this, and while Riku wants to “get all the aspects” addressed in a “diplomatic” manner because it is a “complex and multifaceted discussion”, but they are over thinking this and will literally never do it so I’ll go with the really rough outline that they started and fill it in with what I know of our system.
Sorry if I sound really inflammatory, I’m not a diplomatic person lel
Also, for comedy sake, I am going to maintain everything Riku kept in this outline and try my best to fill it out. A lot of this I am completely lost on so, there will be moments where I am clearly confused lel
I may get some of our opinions “wrong” because I’m kind of taking a guess from my access of the brain, so I apologize if Riku looks at any asks or reblogs we might get from this and goes WHY DID ADERIS SAY THAT?! I’m trying my best
===
Overall TLDR Opinion: So as a system, we don’t like to be too involved in it publicly. Its a multilayered complex topic with too much nuance for it to be worth advocating for or against, and with how large of a cultural phenomenon it is, it isn’t going to change with us. We don’t think it is likely that DID can be formed without trauma, but we also don’t write it off fully. We strongly however do not like “intentional” systems and find it really offensive and gross. With that being said, we also recognize issues in being too forward about that, so we don’t bother with it much.
More details below the keep reading.
-Aderis (Local Discourse Alter)
Can I follow if…
Yes. We really don’t limit or care who is following us. If you identify as an endogenic, singlet, fictionkin, a roll of toothpaste, we really don’t mind or care. I mean, we’d prefer if transphobes and homophobes and all those gross things weren’t following us because honestly - G r o s s - but also like, whatever.
I guess the only people we don’t want following are people that are actively going to use our posts to hurt others or to fetishize trauma or anything? I don’t think we have much worry for that but yeah nah. If you are endogenic or whatever, you can still follow. Just know that our writing isn’t written for an endogenic crowd.
====
Stages of Understanding DID and Endogenic Spaces
I don’t FUCKING know what Riku meant this. What the FUCK is “stages of understanding DID”? I’ve been sitting here for like... five minutes trying to understand what that meant, but I *think* they were trying to get at the idea of how people come to terms with DID.
If that is the case, then one reasons we don’t want to bash or actively advocate against endogenics is that identifying as an endogenic / endogenic-parallel concepts or finding concepts put out there by endogenics is kind of a stage / easier way to accept the situation since it doesn’t carry to baggage of having to accept that you were abused / mistreated.
It isn’t necessarily the healthiest and there is a large concern of getting misinformation and feeding the denial or learning really bad coping mechanisms through those environments, so we don’t think it is a **good** purpose or environment to be in, but the last thing we’d want is to force people who are still struggling to understand their mental state and come to terms with the past that they *have* to admit that they were really fucked up and hurt by things that had happened in the past.
We have a lot of mixed feelings and don’t have a firm stance on if that role in coming to terms with DID is good or not so we really don’t know there or have firm opinions. Since we don’t have firm opinions, we default to “we don’t want to rush / control / dictate what other people with DID are doing in their path of healing and we don’t want to rush people’s healing journey with DID” so we refrain from involving or telling people one thing or the next.
====
Intentional Systems / Tulpamancy Systems
We think they are really offensive and problematic. We instantaneously unfollow and block systems that claim to be intentional, and we tend to unfollow people who post about intentional systems. That is the part of the endogenic community we have very little patience for.
We do know there are still probably actual DID / OSDD systems out there that use those terms to write off their condition similar to endogenics mentioned above, but the amount of damage these ones do and the just straight up often horrible thoughts and opinions about DID that they have outweighs our opinion on not budding our head where it doesn’t belong.
Don’t fetishize / make our disorder a fun thing.
====
Median Systems
Uhh.... I think Riku was going to mention something about how we found out that some people have multiple people in their head through median systems and came to understand that as ourselves and learned beyond that???
I don’t really know what stands out in specific about Median Systems though. I think there might be an opinion somewhere about BPD and Median systems? But generally we also put this in the same categroy as “stages of understanding DID”. Maybe if Riku comes around they can explain if they even know.
====
Can you have a system without trauma?
Oooookaaay, this is one Riku would be 10000% better at answering because they have a lot of nerd stuff about this about science and psychology and statistics and research and shit. I’m not that savvy in those topics though? So I guess I’ll give you a quick rundown from the gist.
We don’t think that it is likely that you can have a system - a true dissociative system with dissociated parts - without trauma. That though comes with the key word “likely”. We are very much open to the possibility / idea that other methods could form dissociated parts and are actually a bit keen into maybe some day doing research on it. Science and research has backed that DID is formed due to disorganized attachment to caregivers and repeated trauma at a young age, but DID is very under researched, psychology is a soft science, and very little about the conscious, identity, and dissociation is actually firmly known.
Until the exact neurological structure / reasoning / process to how DID forms and how it differs from those that don’t have it, we really hesitate to put it in any box because that’s really not how mental health works. It might be that the majority of cases are due to trauma, but theoretically other disorders can cause pretty dissociation and if said disorders occurred at a young enough age, then theoretically maybe something like that could happen. There is somewhere in this brain a tab on ADHD or something, but I can’t go into that cause I really wouldn’t do it a service.
The really condensed version is we don’t think so with our current understanding and readings, but we don’t think it is 100% certain and there is a very reasonable possibility that there is something out there, a different path way that can cause the DID we know - or a different condition that looks and appears similar to DID but is fundamentally different.
You rarely ever *know* anything in psych, especially with something so abstract of a disorder with little research on it such as DID and how consciousness / states of consciousness work in the brain to really be claiming anything so certainly.
====
Should endogenics be considered DID?
I don’t care?? Honestly, our system is generally of the consensus that until evidence comes to show that it is possible AND the same disorder, then no. And even then, I think the question Riku meant was “should endogenics and DID be related / equated / in the same space” which is a strong no.
Even if endogenics are real and are possible, the amount of which trauma plays into what we currently know as DID is so ridiculous that there is honestly little overlap other than the “same hat” of having multiple parts in a body. So much of DID is much more about “spicy” C-PTSD with the exclusive DLC of thick dissociative barriers. A lot of our experience is centered around navigating trauma and helping parts grow beyond the trauma that seeded their existence and I really don’t know how much of that would be able to be properly understood and shared with someone who has NO trauma? I also feel as though inherently the dynamics between parts would HAVE to be extremely different without trauma because all of the “roles” in our system are fundamentally absed on how we are because of our trauma and how we cope and manage things.
====
Endogenics on Social Media / Practically Speaking?
We leave them alone for the most part. If they aren’t being toxic or spreading misinformation, its really not our deal to care about much - and even then it really isn’t. We have a lot of other things in our life to care about and we really don’t have the time or energy to get worked up, heated, stressed, or anything because we see someone claiming to have parts without trauma.
I say let people be people and do things as people do so long as they aren’t harming anyone. We disagree and are technically “sysmeds” or whatever, but like, its not that huge of a thing.
Anyways, that’s all.
13 notes
·
View notes
Text
This is a very long post answering some questions for @nichrage
There is tons of great information and I did my best to break it up so it’s easy to read. Sources so you can do more reading on your own will be linked at the bottom.
In all ages the DSM 5 recommends diagnostic interview to diagnose DID.
During the diagnostic interview (or more often over the course of many therapy sessions) at least one identity (alter) must be identified in addition to the part responsible for living daily life (host), these parts must identify as separate rather than parts of a single personality, and thanks to a change in criteria from the DSM 4 to the DSM 5 the existence of alters may be reported by either someone in the persons life, the therapist or the individual with the experience.
The secondary criteria for the diagnosis of DID is differences in memory not explainable by normal forgetfulness. This happens because of the dissociative barriers between parts and basically means at least one alter cannot remember what happened at least sometimes when another alter was out.
The third criteria for DID is that because it is a disorder it must cause distress or impairment. If something does not cause distress or impairment it is not considered a disorder.
The forth criteria that needs to be met for a DID diagnosis is essentially that it isn’t something else. If symptoms can be better explained by culture, religion, or imaginary play (in children) it is not DID.
The final criteria in the DSM 5 is that drugs, alcohol, or other medical conditions do not explain symptoms. Blacking out when your drunk or losing time due to a head injury, already has an explanation that fits better than DID.
For researching DID many things can be used. The studies I’ve read have all used different methods of studying the disorder but all begin by validating the diagnosis. Some studies rely on self-report inventories, some studies use observations from the individuals therapist and some studies even use brain scans for data.
Environment has a lot of influence of DID because it is a trauma based disorder, however, individual predisposition to dissociation is believed to be important too. In the case of two people living identically, assuming they had the exact same traumas, I imagine if one developed DID the other would too. I can’t know this though. Due to DID’s existence as a disorder caused by trauma it would be unethical to run an experiment to test the probability of developing the disorder based on specific experiences.
It’s believed that predisposition to dissociate is a predictive factor in developing DID, however, DID is a disorder caused by chronic trauma during childhood. Without experiencing childhood trauma current research indicates you cannot develop DID. The current theory of what causes DID is the theory of structural dissociation.
On a basic level this theory assumes that people aren’t born with an integrated personality but rather that we are born with many ego states with different responsibilities relating to a child’s needs, around the age of 6-9 these ego states should integrate into one to create a personality.
Inability to integrate ego states occurs because of incompatible beliefs and world views. For instance if a child is being abused by their parent, the ego state responsible for fulfilling the need of hunger may see their parent as being good because they provide food and the ego state responsible for seeking affection may see their parent as being bad because they do not provide affection, in this case the too parts have incompatible world views and may be unable to integrate.
When no trauma occurs structural dissociation does not occur and the personality fully integrates at the appropriate age.
When only one trauma or one type of trauma occurs one part of the personality may remain separate (or if occurring later in life become separate) from the rest. This is called primary structural dissociation and it is responsible for PTSD.
When multiple traumas happen multiple parts may remain separate from the rest. This is secondary or tertiary structural dissociation. In secondary structural dissociation there is one ANP and multiple EPs, in tertiary structural dissociation there are multiple ANPs and multiple EPs. ANP stands for apparently normal part (also called normal life focused part) and EP stands for emotional part (also called trauma focused part).
Secondary structural dissociation can cause complex PTSD or borderline personality disorder (BPD) in which case EPs are much less complex and will not have a feeling of being distinct individuals that are separate from the ANP. Secondary structural dissociation can also cause OSDD, I do not know enough about other types of OSDD well enough to cover them but in the case of OSDD1 the structural dissociation must occur during childhood just like DID. In OSDD1 EPs feel separate from the ANP but are either not sufficiently distinct or there is a lack of amnesia barriers.
Tertiary structural dissociation can only occur before personality integration in childhood. Tertiary structural dissociation causes DID.
Studies looking at the neurological profile of people with DID in comparison to people in the general population have found significant differences.
One study showed attention to be increased on the unconscious level and decreased on the conscious level; in other words, people with DID were shown to have more dramatic startle reflexes due to increased vigilance that does not reach the conscious level. This is to say people with DID are jumpier because their unconscious picks up on what it believes may be a sign of danger and doesn’t bother to send the message to the conscious mind which could make a logical evaluation of the supposed threat.
Neurological differences have also been seen in memory. For people with DID it was seen that emotionally neutral memories, like word definitions were more likely to be shared across multiple alters, but emotional and associative memories, like ones first date or the ability to trigger a memory from a smell, were more likely to belong to one part.
Finally, the most concrete neurological difference was the size of the parts of the brain responsible for memory, emotional regulation and the fight or fight reflex. For people with DID these parts of the brain are significantly smaller.
In this post I’ve already explained the theory of structural dissociation which explains how parts end up separate. The reason for differing self concepts for different alters is predominately different experiences. As each part accumulates differing experiences they become more differentiated and well rounded; think about twins for instance, their biology is identical and often they are raised in the same environment, attending the same schools, and potentially even sharing a friend group, yet they are not the same people, they do not have identical experiences, and they do not have identical personalities.
Sources
This page explains what the DSM 5 says about DID
Explanations of Structural dissociation 1 2
A study looking at differences between ANP and EP brain activity
This study explains what DID is, how it is diagnosed and how neurology differs for people with DID
2 notes
·
View notes
Note
GAH... BPD + OSDD symptom holder culture is knowing you guys' fp sys (and ttherefore your qpp (she's one of the members IN SAID SYSTEM) is gonna be gone for 42 days and being put in charge because everyone's going through a depressive episode because of it (you're a depression + anxiety + ptsd holder) , and you try and pep yourself up , going "i can do this ... ! i CAN do this !" ...
only to catch a HORRIBLE anxiety attack seconds later and break down . i CAN'T do this !!! not without her !! pplease ccome bback ;; i mmiss yyou sso mmuchh waaahhuugu,uahhg,,hhg
— ⭐🌊🐾 , from resident sad boy in said system sspecifically
We wish you luck 🫡 that sounds rlly tough /g
Hug if it helps? 🫂 /nf
#bpd + osdd holder culture is#bpd + osdd culture is#bpd + osdd culture#bpd + osdd#borderline culture is#borderline personality disorder#bpd#bpd culture is#bpd culture#bpd safe#actually borderline#actually bpd#bpd fp#fp#fp bpd#osdd#osdd system#osddid#cdd#actually osdd#- ⭐️🌊🐾
13 notes
·
View notes
Text
Sander Sides and Dissociative Identity Disorder
This is a topic that wanders in and out of the sphere of focus amongst the Thomas Sanders and Sanders Sides fandoms (the Fanders). I feel inclined to give our input as well as a thorough explanation, because I’m long winded like that.
For the purposes of credibility and clarity, we are officially and unofficially diagnosed with Dissociative Identity Disorder (which used to be called multiple personality disorder). By this, I mean more than one therapist and a psychiatric nurse have told us it’s highly likely we have this disorder. However, our various institutions of mental treatment do not provide the primary diagnostic tools used to diagnose DID. We are having a hard time finding someone who can administer either the Structured Clinical Interview for Dissociative Disorders (the SCID-D) for either the DSM IV or the DSM V, or the Multidimensional Inventory for Dissociation (the MID) who also accepts our insurance. So according to medical professionals, we’re diagnosed. However, there are people in the community who will say you can’t be diagnosed without one of those two tools. My sibling is also diagnosed with Dissociative Identity Disorder.
Since I plan on tagging multiple tags outside of the Fanders, I will very briefly summarize Sanders Sides. This is a youtube series starring a singlet by the name of Thomas (Thomas Sanders being the owner of the channel and actor, but he has made it clear that the Thomas in the series is a character and not himself). In it, he talks to different “sides�� of his personality, exploring all sorts of issues while doing so. These sides are logic, creativity and morality with a fourth side of anxiety being added later (for those in the fandom, I know I’m leaving information out. Shhhhh. I am specifically doing so in case anyone outside the Fanders decides to go watch it). Later on, these four sides reveal their names of Logan, Roman, Patton and Virgil respectively. For those amongst multiplicity cultures, you should already be able to see why this might cause controversy.
Dissociative Identity Disorder is an extreme on a spectrum of multiplicity. For the purposes of this discussion, let’s give a quick run down of the typical names and types of multiplicity across this spectrum. (Using gender neutral pronouns because I cannot be bothered to type himself/herself/themself repeatedly)
1. Singleton
This is the average individual you will run into. This type of person is whole in and of themselves. They might have different ways of behaving with friends versus family versus work versus alone, but that is typically accepted behavior for a singleton.
2. Median System
This is someone who’s behavior implies more than one person. They may or may not consciously recognize this vague division with themselves, or they might have consciously or unconsciously created more extreme modalities of behaving for the purposes of getting things done. They are neither singlet nor multiple.
3. Tulpamancy
Originally a monk practice, this is when someone consciously personifies different aspects themselves. This can be either to sharpen skills or to learn about themself. An example would be someone who pushes their sadness into a box and talks to it in an attempt to understand their sadness. Eventually, this box is supposed to evolve into an independent being inside their head. Once fully developed, they are officially called a Tulpa, thus tulpamancy being the practice of creating them. They may or may not have a name or gender. They are neither singlet nor multiple.
4. Borderline Personality Disorder
I hesitantly place this on this list, but I feel it’s worth discussing for the purposes of this discussion. On the spectrum, BPD could arguably be placed anywhere on the spectrum below OSDD. There are 9 symptoms to diagnose this illness, and there are entire books written on it. I am not going to dig into that here, but suffice it to say that BPD could be argued to be on this spectrum. This is someone who is characterized by a distinct instability of self. They may or may not go by multiple names, but what defines them as a person swings wildly around. They feel or act unstable. They might change behavior, clothing style, or friend groups rapidly. This is a MENTAL ILLNESS and not something to be pursued. If you think you might have BPD, please seek professional help. They are typically considered an extremely unstable singlet or perhaps median at most. However, it is not uncommon for someone with BPD to pursue tulpamancy to help understand themselves or become an endogenic system to help define their unstable state of being. (However, if this person developed BPD as a result of trauma, they could arguably be placed within the traumagenic area of this spectrum)
5. Endogenic System
This is a broad term. Technically speaking, an endogenic system is strictly a system that came to exist naturally (essentially, trauma did not cause their identity split). As a result, this could include Median, Tulpamancy, BPD splitting their different ways of behaving to understand themself, or anything and everything in between. Some claim they just grew up this way. Due to the broad nature of the definition of endogenic, there is a lot of controversy surrounding it. I’ll touch a bit on that controversy later. Within endogenic culture, they are considered multiple.
6. Quiogenic System
This is a system who has no idea why they’re multiple. They don’t know if they’re traumagenic or endogenic, if its caused by childhood trauma, if they grew up this way, if they accidentally created their multiplicity, or any combination of the above. They might be singleton, they might be endogenic, or they might be traumagenic (Worth noting is a lot of traumagenic systems are amnesiac of their trauma. Something could have traumatically happened, but they have no recollection of what happened. Some are even amnesiac of their own amnesia. Meaning, they don’t know what memories they don’t know, and/or they don’t even realize they’re missing significant portions of their life where trauma occurred. This naturally causes a lot of concern and confusion). If you don’t know why you’re multiple, you deserve professional psychiatric help if it is something you struggle with.
7. Imitative Dissociative Identity Disorder
This is where we lean into the multiplicity debate heavily. Imitative DID is not an officially DSM recognized illness (DSM stands for the Diagnostic and Statistical Manual of Mental Disorders and is the accepted standard for diagnosing mental illnesses). However, it is gaining recognition within professional psychiatric fields and multiple articles have been written on it. This is someone who either deliberately or unconsciously created their multiplicity. Believers in Imitative DID would argue everything discussed thus far would be Imitative. You can easily see how this causes strife, as this essentially states anyone who isn’t traumagenic is making up their multiplicity for whatever reason. Since multiplicity is so closely tied to how someone understands themself or themselves, this is like a slap to the face. It is not uncommon for traumagenic systems to call anyone else fake and incapable of understanding true multiplicity. Which traumagenic multiplicity comes with a LOT of problems that makes life terribly difficult or hellish. They get angry because they feel like endogenic systems are encroaching on their clinical terminology and stealing/redefining it. This in turn is considered to be devaluing their mental illness and struggles, ruining the official credibility of a set of illnesses that is already extremely stigmatized culturally and professionally. They also feel like endogenics are stealing/overwhelming/corrupting their admittedly few areas of clinical support. Knowing all this, it should be pretty obvious why there’s so much controversy here and why it can get so vicious.
8. Complex Post Traumatic Stress Disorder
This is not yet a DSM recognized mental illness. This is a form of PTSD created for the purposes of better encompassing chronic abuse symptoms such as childhood abuse. However, this could also include trauma caused later in life such as war. There are other examples, but these are the most common cases. In that case, C-PTSD would be diagnosed instead of PTSD if it presents with what appears to be multiplicity, such as severe emotional dysregulation (inability to control emotions) and emotional black outs. This person can present with one or two other supposedly different identities. The difference in personality is usually very obvious, and the individual does not typically remember what happened in this alternate state. It is unclear if they are truly multiple or not, although most will argue not. If you think you have PTSD or C-PTSD, you deserve help and should seek it out as best you can.
9. Traumagenic System
These are systems that are created due to trauma. Clinically speaking, the large majority of professionals state this can only be caused by chronic childhood physical, sexual or emotional abuse. PTSD is almost always diagnosed comorbidly (comorbid illnesses simply meaning illnesses that are frequently diagnosed together on the same person). All traumagenic symptoms are defined by two or more distinct personalities/personality states/alternate personalities/or simply put: alters. These alters can be completely different ages, genders, or even ethnicities. Alter don’t even have to be human, presenting as animals, fairies or even rocks. This becomes terribly difficult to live with when say… a 5 year old, a wolf, or a rock alter ends up taking control (the clinical term being “fronting”) around family, friends, or even at work. Functioning independently can easily become impossible, although plenty of people manage it with treatment. If you think you might have DID or OSDD, you deserve professional help and should seek it out as best you can.
9a. Other Specified Dissociative Disorder
There are several different types of OSDD, but for the purposes of multiplicity only type 1 applies. Subtype 1a includes alters without clear boundaries between each personality. Subtype 1b is essentially DID without “lost time” (time during which the body was doing something but one or more alters do not remember what).
- I will add the caveat that OSDD 2 might apply depending on your POV. This is someone who has become convinced they are multiple via severe coercion/abuse.
9b. Dissociative Identity Disorder
This is a single body with two or more alters. In some cases, none of the alters will remember what anyone else has done. They might only be able to communicate via leaving each other letters. Other times, some alters might share memories and others might not. In order for DID to be diagnosed, there has to be lost time somewhere between the alters (as in, alter 1 might remember what alter 2 did but alter 3 might not). Whether or not this lost time has to be something that occurs in recent times or only something that occurred in childhood is a decision left to individual professionals.
Now back to Sander Sides. Knowing all of the information above, it should become obvious why there might be controversy surrounding the Sanders Sides. If you watch the series, it quickly becomes obvious that Thomas is a tulpamancer. Outside of the show, people have argued that Thomas Sanders himself might be median. Thomas Sanders himself has strictly denied any similarities between Sander Sides and Dissociative Identity Disorder.
This obviously puts Sander Sides dead center of the Imitative DID debate (endogenic versus traumagenic). Aside from that, there is the fact that tumblr in general has a gatekeeping culture inside it especially concerning any and all mental illnesses.
As for our personal opinion?
By all means, promote Sander Sides. We don’t even care if you present or consider Sander Sides to be representative of multiplicity, although I would generally discourage saying it is DID specifically, only similar in some ways. In the face of movies like Split and Sybil, multiplicity and DID especially needs better cultural representation. The fact that DID only ever makes the news when a criminal has revealed themselves (Like Billy Milligan, Billy Joe Harris, and Dwayne Wilson) makes this representation particularly important. As someone with DID, I would die for more media presenting DID as something other than dangerous. In fact, someone with DID or OSDD is far more likely to be victims than to create victims.
-On a side note: If you’re curious about multiplicity and how this may or may not apply to singletons in general, I highly recommend reading The Myth of Sanity: Divided Consciousness and the Promise of Awareness by Martha Stout. The DSM V is also a great resource for obvious reasons. For DID specifically, I recommend did-research.org . If more resources are desired, I can add them. I’d also encourage someone to reblog this with resources for these various mental illnesses, but I’m a bit too spent to attach that right now after typing all this.
Aside from all the debates, Sander Sides has helped multiple people come to accept their DID or OSDD. For some, it’s brought awareness to those mental illnesses. I know for multiple people with DID or OSDD, Sander Sides has been a huge relief. Finally, we get to see something that shows debates similar to the arguments that happen in our heads every single day. It’s a breath of fresh air.
Is Sander Sides DID? No.
Do I promote it anyway? Yes.
Do I think comparing it can do more good than harm? Yes.
Do I think it’s possible for it to cause harm? Certainly, but there is far more good that can come out of it. It’s worth the risk.
Editing real quick to say that I'm more than willing to answer any questions, related or no. Comment, reblog, Ask, PM or whatever else you can think of.
(tagging @aromantic-asshole cause he asked)
(Also tagging a few big name Fander blogs, because we would really like this to make the rounds)
@tinysidestrashcaptain @treblesanders @randomslasher @sanders-sides-thuri @princelogical @milomeepit @theonlyjelly-iwillput-inmybelly @2queer2deer @ironwoman359 I know for a fact I’m forgetting people, I’m so sorry. I also don’t personally know over half of you and if this is unwanted, I apologize for that too. This just means a great deal to us, and we finally worked up the courage to say something. Also screw it, let’s tag @thatsthat24 and @thejoanglebook
#sanders sides#thomas sanders#sander sides#actuallydid#dissociative identity disorder#median#tulpa#tulpamancy#borderline personality disorder#bpd#endogenic#traumagenic#quiogenic#imitative did#ptsd#cptsd#c-ptsd#osdd#osdd1#osdd1a#osdd1b
539 notes
·
View notes
Text
Trigger warning: Suicide, rape, poop and child molestation.
My Facebook is almost entirely meme pages these days, so my feed is 90% jokes about killing yourself and chronic alcoholism, 5% puns, 1% each for gore, porn, poop and anime, and finally 1% articles (news and opinion alike). And before you ask, yes I have unfollowed the majority of my friends to make room for the aforementioned "It's time to put the I in suicide!" posts - I just relate to those more.
So imagine my shock when my pleasant scroll was interrupted by a post from a page that I shall not name but that can be summarized with "I smoke lots of weed, hate the government, and am likely to engage in revolutionary suicide so that even my death is virtue signaling" - said post being an article about "Pedophile culture". I've seen the article shared on here before (long story short: men like hairless legs, how can we use this to make men look evil? children have hairless legs... aha! lets claim men like children!), but this time I decided to look for some spicy reactions in the Facebook comments, maybe a good "this is bait" picture I could steal... oh how I came to regret that decision.
First I found a comment thread in which a person with Link (some Twilight Princess artwork, to be precise) as their profile picture very calmly and respectfully explained that liking hairless legs could be a number of things - simply not liking the texture of hair, or even being victim to the same brainwashing that the article claims the media inflicts upon women. To which the page responded "^ dude stop fucking kids" (and got 38 likes compared to Link's 18... kill me, just right now, end my suffering, please). Want to convince people that pedophilia is an incredibly prevalent problem caused by sexism? Well don't forget to fire off baseless, albeit jokey, accusations of child molestation at everyone who disagrees with you! That'll really hammer home the severity of the situation!
There was also a comment saying that people who use the term "SWERF" to describe certain feminists are "rape apologists", and some pretty gnarly stuff calling every guy on there who commented about his own preferences towards body hair a pedophile, and then blah blah patriarchy, blah blah women are oppressed, blah blah beautiful hairy pussy - suffice to say, most of the comments were the generic trash that I am used to scrolling past to get to that sweet sweet reaction pic.
But then... well, I'll let these two direct quotes speak for themselves:
[After someone else mentioned the "I'm a pedophile but not a monster" article] "I wholeheartedly agree with you. You're not a monster - you're a man. A rather common man. A microcosmic representation of patriarchy's most prevalent perversions."
"I and every other woman I know has a story of being sexually abused or taken advantage of by an older man when still a child or teenager. It's an epidemic."
Earlier I saw a video in which a man walked into a bathroom stall, did a handstand, and projectile pooped over the wall of the stall. That soaring turd made more sense than whatever twisted logic led these two people to claim that it's common, normal for men to be child molesters, that being a pedophile is simply part of being a man, and that society accepts- no, encourages child molestation... and on top of that, to imply with anecdotal "evidence" that 100% of women were raped by men as children.
Unlike the article, these two people are not simply trying to attribute bad intentions to a perfectly normal occurrence because of their own bias; they're literally claiming that men, en masse, are raping female children to enforce patriarchy (enough female children to be called "common", an "epidemic", the "most prevalent").
There are actual victims of child molestation, sexual assault, rape and child abuse - we get disorders that stick with us for the rest of our lives: PTSD, DID, OSDD, BPD, NPD, AVPD, depersonalisation/derealization, depression, anxiety, agoraphobia, eating disorders, fuck I could go on and on and on. It isn't a normal human experience. It's not common, prevalent, an epidemic, it's not something that every woman goes through or that every man wants to do/actually does. It isn't "Oh, there goes Bobby down the road, probably raping kids again, how quaint."
There's something extra sickening about people claiming that child molestation is just what men do all the time to enforce patriarchy. That's not why abusers do what they do. Even if you believe in patriarchy, surely you understand that individual people still do awful things without doing those things specifically to further patriarchy, and that by implying that raping children is some orchestrated global conspiracy amongst men and not the actions of a terrible individual you're fucking with victims and not only how they view their abusers, but how they view men as a whole; not to mention that you're invalidating male victims and victims of female abusers.
It's important to realise that there may well be actual victims reading these comments, and when you say that all men are as dangerous and cruel as their abusers... well, from where I'm sitting, that just looks like you're trying to incite paranoia and mistrust of an entire gender, in people who've already been through enough.
And I haven't even gone into the long rant about how this crime shouldn't be gendered or used to further gender-focused ideologies - about how many boys are victims of child molestation, about female teachers raping male students, about the cultures around the world that include being raped as a part of a boy's "becoming a man" journey, about the number of female abusers especially when you include cases in which there were multiple abusers (Spoiler alert: it's a fuck tonne higher than zero). I haven't even begun ranting about the article itself or the rest of the comments - I haven't talked about how there isn't a pedophile culture, about how it is literally seen as the single most disgusting thing a human being can be.
But I can't put all of my problems with these comments into words right now - fearmongering, lies, gendering child abuse/molestation, belittling the severity of abuse by claiming that it's an accepted everyday tactic that "the system" inflicts upon everyone within it, and more - I'm tired and the world sucks and people suck. It's like they got done diluting the word rape and they had to move on to something worse.
Next week on The Feminism Show: Is patriarchy gang-raping all babies and then feeding them to pigs? The answer may surprise you.
~ Vape
#Tw rape#tw suicide#tw child molestation#tw really shitty post full of bad jokes#Mod Vaporeon#your regular alter was unavailable so this post was brought to you by me
11 notes
·
View notes
Text
Dissociative Disorders 101
In this post, I'm going to give an outline of Dissociative identity disorder (DID) and Other Specified Dissociative disorder (OSDD).
These two disorders are terribly misunderstood due to horrible representation in media, a lack of education on the topic. Many people still refer DID as Multiple Personality Disorder (MPD) an outdated term from when DID was classified as a personality disorder, we now know the disorder is better seen as a dissociative disorder. I hope this post will help clear up misunderstandings about these topics.
[CW: Mentions of abuse, medical trauma, war, human tracking, suicide, self-harm, and addiction. All of these are briefly mention and not discussed in detail. Ableism is the only cw discussed in detail]
[Note: This post is not to be used as a diagnostic tool.]
DID & OSDD Glossary:
Alter: Shorthand for alternate personality or alternate identity. The most common language to refer to the multiple identities in the system. You may also see the terms "parts" & "headmates".
Alter jobs: also called “Alter types” or “Alter Roles”. This refers to the common occurrence of certain alters taking on specific roles. This often happens because to some extent DID & OSDD acts as extreme involuntary coping skills. Examples of this are protectors who deal with danger, caretakers who help keep the alters in the system comforted, or trauma holders who retain memories of trauma.
Co-Consciousness: often shortened to co-con. When two or more alter are aware of the outside together. Thoughts of both alters can often blend together. Even at times alters may have split control of the body.
Depersonalization and Derealization: Often shortened to DR/DP. DR/DP disorder is its own diagnosis but those with other dissociative disorders experience it as well. Depersonalization the feeling of oneself is not real or is heavily disconnected from the body. This can even result in one of feeling in control of limbs at all. Derealization is the feeling of the outside world not being real, or a simulation.
Fronting: The act of being the alter conscious at the time and ability to interact with the outside world.
Host: Either the person believed to be the “first” personality (sometimes called the core or original) or the latter who fronts the most.
Splitting: In this case, it refers to when new alters form.
System: A word used to reference all of the alters as a whole. Used like "I am an alter in a system" or sometimes “ I am a system”. Rather someone uses this term is a matter of personal preference, and if they see themselves as part of a system or collectively are a system.
What is Dissociation?
Dissociation refers to the mechanism our brain has to disconnect us from our surroundings sometimes as a benign reaction but severe dissociation is associated with trauma and other mental illnesses.
Every Person has the capacity for dissociation and many experiences some degree of the skill like when you drive home but don’t remember it. However daydreaming in class, spacing out every now again is healthy, there is a huge difference between those experiences and those of people with dissociative disorders.
Dissociation is primarily associated with DID but can also be a symptom of C-PTSD, Borderline Personality Disorder (BPD) and some forms of psychosis. There are also physiological conditions that cause and/or mimic dissociation. Like seizures and migraines.
What are the symptoms of DID & OSDD?
[Disclaimer: I’m aware that the DSM is a flawed way to look at mental health, but it is the best way we have to ensure all parties are working with the same definition of terms]
DID:
DID diagnostic criteria are as follows:
1)Two distinct identity states are present. They have to be separate and able to act autonomy. It isn’t “feeling” like another person.
2)Amnesia must occur, defined as gaps in the recall of everyday events, important personal information and/or traumatic events
3)The person must be distressed by the disorder or have trouble functioning in one or more major life areas because of the disorder. This criterion is common among all serious mental illness diagnoses as a diagnosis is not appropriate where the symptoms do not create distress and/or trouble functioning.
4)The disturbance is not part of normal cultural or religious practices.
This DID criterion is to eliminate diagnosis in cultures or situations where multiplicity is appropriate. An example of this is in children where an imaginary friend is not necessarily indicative of mental illness.
5) The symptoms are not due to the direct physiological effects of a substance
So what does that mean? It means that those who have the disorder have at least one alter the hallmark of DID. Alter come in all kinds of varied types and versions. The amnesia criterion does refer to forgetting traumatic events, but also incidents in normal life.
Alters themselves are a complex they aren’t "alter egos or" made up people. Alters can be almost anything, children (younger than the body) adult alters (older than the body), alters based on fiction called Fictional introjects (fictives for short), alters who are angels or spirits, ghost alters, animal alters, alters of varying race and sexualities. This is because alters form to ensure the survival of the child, this includes alters to comfort, protect, soothe and hold trauma away from the wider consciousness. This means that anything that can fill that role can be put into an alter. There is no control over alters, they are not imaginary friends or malleable they are the best way the mind had to survive.
In day to day life DID might look like having missing time, experience dissociation even when in control, a sense of not having an identity, hearing voices within their heads (not auditory hallucinations), meeting people you feel like you should know, having actions you took but have no recollection of, overlapping emotions and trouble focusing.
People with DID have high rates of self-harm, suicidal behaviour, addiction, disordered eating and other behaviours that cause damage to oneself. This is often even more distressing as one might hurt themselves and not remember it because an alter did it.
Those with DID will also often have what is referred to as “Inner worlds” or “headspace” this refers to in the mind of the person there is a mental world within. This is a place where alters have a form, body and voice within the mind. It is often a combination of a coping skill used as a kid to escape and a way to be able to interact with others alters. Headspaces often are where alters feel they are when not fronting. It also provides a way of seeing where alters who are not in communication with others are, and can sometimes serve as a visual connection to understanding the others in the system and understand trauma.
Somatic symptoms are really common, Including: Headaches, nausea and vomiting, Non-epileptic seizure/psychogenic seizures, blurred vision, muscle aches, nerve dysfunction (like dysautonomia), fatigue, other feelings of illness. This is sometimes part of conversion disorder.
People with DID & OSDD almost always also have (C-)PTSD. So symptoms like hypervigilance, nightmares, and flashbacks. As they have DID & OSDD and have experienced trauma they likely have symptoms from that other than dissociation, even if they do not meet PTSD criteria.
BPD has high comorbidity with DID, many people with DID or OSDD are misdiagnosed with BPD. Other common comorbid conditions include Anxiety Disorders, Depression, Eating Disorders, and Conversion Disorder.
OSDD:
So the thing about OSDD is a category of conditions that don’t fit another diagnosis. With this post, we are mostly concerned with OSDD-1a and OSDD-1b because those disorders are most similar to DID and form systems.
The DSM Description is as follows:
This category applies to presentations in which symptoms characteristic of a dissociative disorder that cause clinically significant distress or impairment in social, occupational, or other important areas of functioning predominate but do not meet the full criteria for any of the disorders in the dissociative disorders diagnostic class. The other specified dissociative disorder category is used in situations in which the clinician chooses to specify the reason that the presentation does not meet the criteria for any specific dissociative disorder. This is done by recording "other specified dissociative disorder" followed by the specific reason (e.g., "dissociative trance"). Example presentations that can be specified using the "other specified" designation include the following:
1. Chronic and recurrent syndromes of mixed dissociative symptoms. This category includes identity disturbance associated with less than marked discontinuities in sense of self and agency, or alterations of identity or episodes of possession in an individual who reports no dissociative amnesia.
2. Identity disturbance due to prolonged and intense coercive persuasion: Individuals who have been subjected to intense coercive persuasion (e.g., brainwashing, thought reform, indoctrination while captive, torture, long-term political imprisonment, recruitment by sects/cults or by terror organizations) may present with prolonged changes in, or conscious questions of, their identity.
3. Acute dissociative reactions to stressful events: This category is for acute, transient conditions that typically last less than 1 month, and sometimes only a few hours or days. These conditions are characterized by constriction of consciousness; depersonalization; derealization; perceptual disturbances (e.g., time slowing, macropsia); micro-amnesias; transient stupor; and/or alterations in sensory-motor functioning (e.g., analgesia, paralysis).
4. Dissociative trance: This condition is characterized by an acute narrowing or complete loss of awareness of immediate surroundings that manifest as profound unresponsiveness or insensitivity to environmental stimuli. May be accompanied by minor stereotyped behaviours of which the individual is unaware and/or that he or she cannot control, as well as transient paralysis or loss of consciousness. The dissociative trance is not a normal part of a broadly accepted collective cultural or religious practice.
Those with OSDD-1a&b meet most but not all of DID criterion. They are considered Complex Dissociative Disorders along with DID.
OSDD-1a is either identity disturbance with less distinct alters than DID (they cannot physically take executive control over the person's body, but strongly influence the person's thoughts and actions with this type there is amnesia.
OSDD-1b does have distinct alter do exist and can take executive control with the type there is no amnesia.
How does DID or OSDD Develop?
DID & OSDD comes from long term childhood trauma. When a child is exposed to long term trauma and the identity of the child cannot properly integrate. This means your brain put up amnesic barriers to memories and perception forming the separate identity states.
DID is highly correlated with sexual abuse, physical abuse, medical trauma, living in a war zone, child trafficking, and Ritual abuse. Another key factor in a child developing these disorder is the lack of healthy attachment (more info here) You can not develop this disorder after age 9, you can't develop it from a single trauma.
The most current theory used to understand how these disorders works are Structural Dissociation. It refers to the way our brain changes the usual structure to compensate for traumatic experiences. It also posits that a child is not born with an integrated personality, to begin with, and this what allows the extreme dissociative symptoms of DID to manifest.
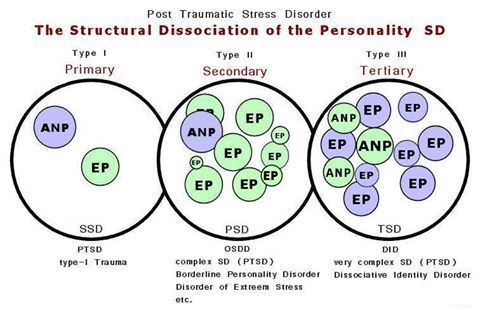
(Image Source)
ANP refers to “Apparently Normal Part” (someone who takes care of daily life)
EP refers to “Emotional part” (someone who holds trauma memories, reactions, and/or sensations).
Primary SD: is found among those with PTSD. The EP holds all trauma associated things such as fight or flight, feelings, sensations, etc, and is not a fully differentiated being (such as alters are/can be in DID and OSDD-1)
Secondary SD is OSDD, complex PTSD, and BPD. OSDD-1 has the most developed EPs out of the secondary SD disorders. BPD and C-PTSD EPs are less developed than OSDD-1 and are fragments (less fragmented than fragments found in OSDD-1 and DID). Secondary SD emotional parts hold less trauma-related material than the single EP found in PTSD. While the EP in PTSD will hold all of the trauma, there may be an EP in the secondary SD category for an emotion related to the traumas, another for body memories, another for visual memories and auditory memories in some of the traumas, and so on.
Secondary SD is OSDD, PTSD, and BPD. OSDD-1 has the most developed EPs out of the secondary SD disorders. BPD and C-PTSD EPs are less developed than OSDD-1 and are fragments (less fragmented than fragments found in OSDD-1 and DID). Secondary SD emotional parts hold less trauma-related material than the single EP found in PTSD. While the EP in PTSD will hold all of the trauma, there may be an EP in the secondary SD category for an emotion related to the traumas, another for body memories, another for visual memories and auditory memories in some of the traumas, and so on.
Tertiary SD refers to DID. There are multiple ANP and multiple EP. They are more developed than the ANP and the EPs in Secondary structural dissociation (though DID parts can have the same degree of development as OSDD-1 parts and vice versa). EPs can be “small”, as in less developed and would be considered fragments, as they hold limited trauma material such as a single feeling or one or two of the senses in a few trauma memories (or just one or two of the senses in one trauma memory). EPs can also be a fully developed part, such as an ANP would be, but hold trauma material. Multiple ANPs exist and can have various jobs associated with daily life such as a school part, a work part, a caretaker part, etc.
This theory is one of the most widely accepted concepts of how alters form and best matches most people's experience. It does contradict the idea that alters are split pieces of one cohesive identity being split the old model.
Another thing to keep in mind about this theory is it shows the structure and function of the brain are altered from a young age. Brains conditioned to dissociate during stress and trauma will continue to split during stress. This means alters can continue to form in those with DID & OSDD past age 9.
This Video explains further how this relates to alters splitting
Treatment:
DID & OSDD can be treated and worked on so the person is no longer experiencing the adverse effects or usually lessen them. Treating DID works mostly the same way as any other trauma survivor. Most kinds of trauma therapy can be used, EMDR being the exception. Certain kinds of meditation and visualisation also prove to be not as effective.
Medication can be used to treat comorbid disorders like depression or anxiety but there are no pharmacological treatments for DID on its own.
What is unique about DID is there is the aspect of how the alters affect you. With DID & OSDD time spent with, alters is crucial. Helping alters who are struggling with trauma becomes deeply important in healing.
The two main options with alters are integration or communication.
Integration refers to a process of when two identity states fuse together. This means you have less altered consciousness states, it also relates to them both being able to handle their trauma. The goal here is to end up with the patient having a singular integrated identity.
The other treatment focuses on forming functional working relationships with the altar and helping them process trauma individually, integration might still happen but a singular identity is not the end goal.
Mythbusting:
“People with DID are just psychotic or delusional” False, psychosis is not a feature of DID or OSDD and has been shown to act completely differently for the person and in the brain than psychosis. This is also offensive as it denigrates people with psychosis.
“DID is fake/made up by a therapist/ social contagion/the person only believes they have alters” False: DID has been observed in multiple studies and social contagion, malingering and therapist coercion are no longer prime theories. People saying this often bring up the false memory scare and Sybil. Both of those have been proven to be wildly overstated and are not the only evidence we have. There are cases dating back to the 1500s with the first psychiatric observations in the 1800s.
“Aren’t they dangerous?” or “they're so scary and crazy!” or “Don’t they need to be locked up” False, The real facts are people with dissociative disorders don’t commit violence at a higher rate than anyone else. They are much more likely to be the victims of violence. Starting with the fact they faced violence as a child to even have the disorder.
“Isn't that possession?” or any other spiritual concepts. False, There is nothing supernatural reasons for DID. Some people have spiritual or religious beliefs that change how they personally perceive their condition, but there is nothing supernatural about DID or OSDD.
“It’s super rare” Not actually the estimate for DID is about 1% of the population. Might sound small but with the number of people in the US alone who have, it means you're likely to meet someone with it.
“I would know if you had it” Not likely. Most people with DID present with covert DID. These people do not have alters who act wildly different from the host. Generally alters will attempt to not show obvious signs as well as being n the same mind with similar physiological aspects and upbringing influence things like mannerisms. Only 5-6% of people with DID have an overt presentation. Even these people are unlikely to be able to wildly change the way they dress and the like as it’s impractical.
“Bad alters/evil alters/violent alters/murder alters” False. There are often alters who might feel aggressive or be persecutors who hurt the other alters. But they are not going to commit murder or rape. They are usually more dangerous to the person with the disorder than anyone outside. And this anger usually stems from trauma.
“You can’t have the disorder you wouldn’t know” and other variations on “Crazy people don't know their cray”. False usually people with DID reach out to help themselves they don’t get forced into it. Because the symptoms of DID disrupt life and the usual comorbid PTSD or other mental health conditions. People with DID are also often aware to some extent of their alters. Rather this is voices, time gaps, or passive influence. And people who have known about the disorder and are in treatment often have good communication between alters in the mind, they are definitely aware of their health.
I Hope this is helpful for those with and without the disorder to better understand these conditions. My personal experience with DID does mean I’m particularly passionate about education on this topic even more as it intersects with education about trauma in general. I hope this didn’t come off as adversarial and helps people learn.
-Admin 1
{Resources: Structural Dissociation Explained, OSDD Diagnostic Material, The Fantasy Theory of DID, New Models of DID, DID Literature Review, DID Research.org, DSM Library, Webermann, A. R. & Brand, B. L. (2017). Mental illness and violent behaviour: The role of dissociation. Borderline Personality Disorder and Emotion Dysregulation}
#blog post#mental illness#mental health resources#mental health education#mental illness education#dissociative identity disorder#did#other specified dissociative disorder#osdd#osdd1#multiple personality disorder#mpd#dissociative disorder#dissociatvie disorders#dissociation#childhood trauma#structural dissociation#bpd#cptsd#ptsd#disordered eating#long post
39 notes
·
View notes
Last Seen Blogs
bisnankz
Untitled

napoli1961potenza
Senza titolo
several-almost-score
Untitled

zenkonto
Zenkonto
spacestrap
i top my f/os and they like it