#enby gal
Text
Feminamoric Girl Pride Flag

Feminamoric woman/girl: a diamoric orientation describing those who are genderqueer/non-binary and woman/girl while attracted primarily or exclusively to women.
Combining colors from feminamoric flag and non-binary woman flags.
#girlby#xirl#demigirl#female-leaning bigender#nonbinary woman#genderqueer girl#non-binary#feminamoric#mogai#pride flags#mod a-p#femby#enby gal#demiwoman#demifem#fideospec#fiaspec#woman-aligned#pride flag#femaric#lgbt+#fingender#fem-related#women's rights
26 notes
·
View notes
Text
here's to men with big tits, and women with no tits. kissing every one of you on the mouth (if you want)
#transgender#trans#nonbinary#enby#lgbt#lgbtq#queer#transmasculine#transfeminine#trans women#trans woman#mtf#transmasc#transsexual#ftm#trans men#transman#trans man#trans guy#trans gal#transfemme#genderqueer#bigender#polygender#multigender#our writing#intersex
3K notes
·
View notes
Text


"man-bun Dowling years Crowley is the best look" THIS and "S2's cunty turtleneck is the best look" THAT. Stop fighting, girls, they're both gorgeous. Together they're unstoppable.
That fruity black turtleneck better be a recurring character in season 3 or I will lose it. After all the angst, we deserve this.
#good omens#good omens season 2#crowely#that turtleneck really better be there when season 3 drops#and God i hope that he will have longer hair. we deserve this my gals and pals and enbys!#sha's artsies uwu
210 notes
·
View notes
Text
also as a nonbinary myself (a nonbinary man but still) i dont get the idea of "enby" being infantilizing? like okay the -by is like the sound in baby. but the primary image it invokes in my brain is the abreviation "nb" from nonbinary. ive always thought of it as just the spelled out version to avoid confusion with other meanings of nb like non-black. and ive never heard an alternative suggested either like are we just "nonbinaries" then
#og post#somebody mentioned enby in the tags of that poll#though they also mentioned “guys gals and nonbinary pals” and i agree there im not a fan of that one at all
32 notes
·
View notes
Text
My wife said her forum was wondering what trans guys make memes about -- trans gals have Blahaj and stripy socks and all that, so is there a counterpart? And I realized I didn't have a good answer, so I Googled "transmasc memes"
and almost all the results were memes about how there aren't transmasc memes. thanks, Google
#trans tag#my posts#now obviously those stereotypes exclude vast swaths of the trans gal experience etc etc#but they're distinctive#everything i could think of for trans guys also goes for butch lesbians and/or enbies#maybe i'm forgetting something obvious? lol#transmasc
25 notes
·
View notes
Text
Wait what's that she's drawing again?
Oh my Falke it's signalis ocs
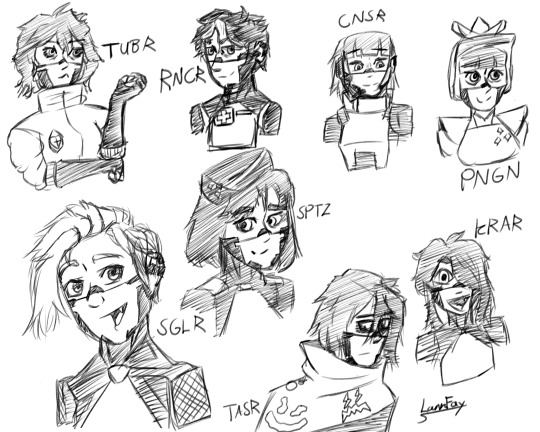
It's signalis OCs from some of my favorite folks who make signalis stuff! Either with a style I can't help but love or lore and vision I can't stop thinking about, these little androids stuck in my head and I had to get em' out
#signalis#signalis oc#signalis fanart#TASR#TUBR#RNCR#CNSR#SGLR#SPTZ#KRAR#PNGN#love seeing these little guys gals and enby pals
132 notes
·
View notes
Text
I kind of hate being a Stereotypical Autistic Person, but it's not my fault, it's just who I am.
I feel like a caricature from a sitcom-- "I'm autistic, my parents got me tested after I tried to memorize an entire tv show and recite it." I alternate my text as I type, and I write my meticulously-planned, 60-plus-character-novel in comic freaking sans. I pronounce things weird as vocal stims, (seriously? Lemned Demoned? What am I, a child?) and I move erratically, oftentimes to my humiliation, since I cannot control my body.
I wear over-ear headphones because I can't think if I hear too much noise. I'm verbalflux, which means I go from yammering my mouth off to hardly being able to formulate a sentence. I communicate via doodles and communication cards.
I really like listening to halloween music and memorize everything about my hyperfixations. I love dying my hair but I hate the way it feels. My sensory needs control my daily life-- I can't wash dishes if the sponge is too wet!
I'm gender non conforming because I don't understand the concept of gender-based societal roles. I also have OCD, and that means people act like I'm either "just picky" or "legitimately going to hurt someone as a tic."
I cry a lot. I'm hyper-empathetic. I have a lot of vocal tics I can't control-- you know my signoff? That's something I do uncontrollably.
I'm torn between loving myself as I am, and being cringe, and hating myself for even existing, because I feel like a hollow stereotype. I can't sit still in churches or temples, so organized religion is a nope, but I feel like I am physically tethered to something greater than myself. I am the stars. I am nobody.
If I could be neurotypical for one day, I would see a concert, because I can't see concerts. They're too loud.
I don't know, I suppose I'm venting.
I'm not unhappy, or happy. I'm just me.
#vent#happy vent#wait no#not happy#unhappy vent#conflicted vent#those are much better tags#autism#actually autistic#autism spectrum#neurodivergent#neurodiversity#actuallyautistic#autistic#ocd#actually ocd#look guys#and gals#and enbys#I have got the mental inless#I don't know anymore#I am sorry
22 notes
·
View notes
Text
i shared a peanut butter cookie with my manager today

#we've been working on a project together this month and I've been getting to see her at her office more ૮ ᴖﻌᴖა#we usually just meet remotely or sometimes at the office in our city but we're setting up a new office so it's just us there#she treated me to lunch yesterday too (〒﹏〒)♡ she got us gyro fries n i had some pepsis 2 share.#chaotic as the project's been it's been rly nice🧍🏾♀️im usually just working from home#when i get there we go to the lil coffee shop together ૮˶• ﻌ •˶ა i like their drinks n their staff r really nicey 2 me 👉🏾👈🏾#the new office is nice too actually... even before the building change i just love talking 2 anyone frm her city. they r all so nice n#friendly and inviting. literally so akskska i am always being invited to stuff when i visit.#after moving into my next place i wanna give this city a fair chance now that i actually have a good one to Experience it for a year#and if it's more of the same imma move to her city fr 🚶🏾♀️i wonder where the queer ppl kick it at..#we have some enbies n real sweet gals from that office around my age I'd love to hang with 👉🏾👈🏾 much 2 think
10 notes
·
View notes
Text
Girls don't want jewelry, girls want VIP tickets to see Bad Omens.
#bad omens#guys gals enby pals#all of us#noah sebastian#nick folio#nicholas ruffilo#joakim karlsson#music
183 notes
·
View notes
Text
Truly impressive how kfam was both woke and offensive at the same time.
#i mean i loved the guys gals and enby pals but then you'd get the racist and homophobic stuff#like wow#kfam#king falls am#slut.txt
128 notes
·
View notes
Note
Hey bruno what do you think of this banger
https://youtu.be/rlQd9qWKjLM

Hmm...it's not bad! It feels like it gives off...manic energy? Like I'm running around the house and I'm being chased by a monster and I have to hide.
Y'know, I think I've had dreams like that, but instead of it being a monster, it was mi madre.
...P-please don't tell mami I said that...
#[[im alive bros gals and enby pals]]#[[im still probably gonna post sporadically tho]]#[[school life and burnout yknow?]]#[[but thank you all for being patient!]]#bruno madrigal#encanto#ask blog#rp blog
18 notes
·
View notes
Text
Feminizing HRT Overview, Guide & Information for All People Seeking It
we also have a version of this post for testosterone/masculinizing HRT as well. we wanted to write a companion piece as many folks have asked about this. it has take a bit of time, but here we are!
The testosterone HRT post is here.
Getting Your Prescription
To start taking estrogen, you will need to find a general practitioner, family doctor, endocrinologist or informed consent clinic where you can discuss gender affirming care with knowledgeable staff. Planned Parenthood is a good option for many trans people in general. Your mental health may also be evaluated, and your heart health and screening for a few other health conditions, as well as having access to your family health history if possible will be required.
Check to see if you have medical insurance, either through your family, your job, or if you are low income, a program like medicaid. Search for low income insurance plans in your area if it is needed, many places offer insurance plans for those who can't afford care on their own.
Here is a map of informed consent HRT clinics in the US.
You will discuss any gender dysphoria, gender presentation needs, if you have a support network, how you are impacted by your gender in your every day life with your provider and so on before being given a prescription. You will only be given a prescription after you discuss the risks of HRT and are screened for possible health problems and diseases or ways your body could react negatively to HRT. If you have needle trauma or phobias and can't inject hormones, it's best to bring it up before you get your prescription to save time and confusion.
The Medications
Treatment typically starts with spironolactone (aldactone), an anti-androgen that blocks androgen receptors ("male" sex hormones) for a few weeks, and then add estrogen, but many folks start with spiro and estrogen at the same time. Spiro will lower the amount of testosterone your body makes. For some people, spiro isn't necessary at all!
Some forms of spironolactone are reported to make folks pee like crazy, others do not have as bad of a time with it. Your mileage will vary depending on manufacturer. Spironolactone is intended to be a blood pressure medication, meaning it is a diuretic and is intended to help your body flush out fluids + salt. You will need to keep yourself hydrated if you notice this effect, as well as increasing electrolyte intake where possible.
Estrogen also lowers how much testosterone your body makes, and triggers changes in the body that occur during puberty in afab & adjacent people. Estrogen can be taken several ways, and is usually taken daily, and several times a day. You can take it in a pill or shot, and several forms of estrogen that can be applied to the skin like creams, gels and patches.
Make sure you thoroughly sanitize the skin of any injection sites or areas you will be applying gel or patches. If you are given topical estrogen, make sure you wash your hands after application and do not have someone else apply it for you. Make sure you do not go swimming or shower within several hours of application to make sure your skin absorbs the hormone.
You may not need to take anti androgens if you are doing estrogen injections, depending on how effective the estrogen injections are for you. Some people may not end up needing anti-androgens at all, and may be able to skip that entirely as spiro has unwanted side effects. Your natural hormone levels will dictate whether or not it's necessary, but it is not necessary for everyone.
You may end up being recommended to switch from one form of estrogen to another as your transition progresses, depending on how your body responds.
It's recommended to not take estrogen as a pill if you have personal/family history of blood clots in a deep vein or in lungs (venous thrombosis).
Some people also end up taking progesterone as well alongside estrogen. Progesterone is typically taken to encourage breast tissue growth, as this is the most prominent effect of the hormone. If sufficient breast tissue growth isn't seen from estrogen alone, progesterone can be added to your regimen, though this is only done later on into treatment, around a year or so in.
If you choose injectable estrogen, make sure to listen to your provider and ask for instructions about how to use needles and syringes, as well as injection angles, how and where you'll be injecting. Do not inject in the exact same spot every time, this can prevent the issue from healing properly and create scar tissue or cause infections or skin tissue necrosis (death). You also need a sharps container to safely dispose of your needle tips. Never re-use a needle, even if it was used previously on yourself. Always ask the pharmacy if you need more needles. A lot of places let you get them in bulk.
If you are going the injection route, make sure you know whether or not you are instructed to do intramuscular or subcutaneous injections. Intramuscular injections usually taper out of the system more quickly and need to be done more frequently, where as many patients find subcutaneous injections less painful and easier as they can be done less frequently.
For more information on safe intramuscular or subcutaneous injection for estrogen, please read here.
Another option for feminizing HRT is to take gonadotropin-releasing hormone (Gn-RH) analogs. They lower the amount of testosterone your body makes and may allow you to take lower doses of estrogen without using Spiro. Gn-RH analogs are usually more expensive, but are an option if for whatever reason the conventional route can't work for you.
DON'T GIVE UP IF YOU DON'T SEE THE EFFECTS YOU WANT TO SEE RIGHT AWAY! Many of them can take a long time to develop, often times patience is the key. If you wait it out and still don't see the results you'd like, you can try another route. Don't give up, a lot of people get deterred in the early stage of transition, you'll get there with patience and communication.
Stay patient, stay positive!
What to Expect from Feminizing HRT
Less facial and body hair growth: typically happens 6 - 12 months after treatment starts. Full effects within ~3 years on average.
Slower scalp hair loss: begins 1 - 3 moths after treatment begins. Full effect between 1 - 2 years on average.
Softer, less oily skin, and changes in general skin texture: 3 - 6 months after treatment starts, full effects within 2 - 3 years on average
Rounder, softer features including face and body, and more body fat: 3 - 6 months after treatment starts, full effects in 2 - 5 years.
Breast development: begins 3 - 6 months after treatment starts, full effects within 2 - 5 years on average or more, according to medical studies, but it can vary wildly from person to person, give dosage and hormones taken. If desired effects are not seen, progesterone can be taken alongside estrogen to help after around one year on estrogen. When breast growth begins, it starts with hard lumps under the nipples along with some soreness and itchiness. Some have sore breasts for a long time, and some may get scared and think they have cancer during this stage. Breasts will be swollen and tender for good while, and nipples may be especially sensitive to even light touch.
Reduced muscle mass/density: 3 - 6 months after treatment starts, full effect in 1 - 2 years on average
Potential decrease in libido if on estrogen alone, though not guaranteed: If it happens, it's generally within 1 - 3 months in and can last a while, but may even out over time
Fewer erections, decreased ejaculate volume, and erections that can become painful or uncomfortable if frequent erections are not maintained. This begins 1 - 3 months after treatment starts, and the full effect is within 3 - 6 months. Regularly maintaining erections and frequent ejaculation can ease some of these uncomfortable feelings in some people.
Changes in how orgasms feel, changes in texture and degree of sensation of penis and scrotum skin as well as changes in body odor: typically begins within 3 - 6 months, though it varies from person to person. Often times the way one's body responds to orgasms completely changes, many people find themselves experiencing full-body orgasms and more intense erogenous zones elsewhere in the body other than the genitals.
Smaller testicles, or testicular atrophy happens within 3 - 6 months and the full effects are usually seen within 2 - 3 years.
Increase in size of bladder and decrease in size of prostate over time which can lead to making one's gspot harder to find, and make prostate examinations more difficult, though they are still vital, as prostate cancer is still a possible factor.
Potential mood fluctuations while adjusting to the hormones, many report increased crying and sadness during the first 3 - 6 months with this tapering off after a full year at most.
Increased fatigue while adjusting to the hormones, sleepiness and becoming easily exhausted are common reports. This can vary drastically from person to person, ymmv.
If you have testicles and choose to have them removed, you may need to take testosterone as well as estrogen in order to have a healthy endocrine system. You will need to discuss the effects of this with your specialists if you want to go this route. If your androgen levels get too low because your body cannot synthesize enough testosterone after bottom surgery, you may need additional medication.
Potential infertility, though this is not a guarantee, and safe sex should still be practiced at all times. No timeline projected though the longer one is on E the more likely it becomes.
Monthly cycles akin to menstrual cycles: these are not present in everyone, but many people report entering a cycle of extreme fatigue, body aches, abdominal cramping in the approximate area where a uterus would sit, headaches, and more for around the duration of a menstrual cycle (4 - 10 days on average).
Progesterone inversely to estrogen can cause an increase in libido in most who take it, and is the primary hormone used for breast growth. Lactation may also occur while taking prog, if this happens, talk to your doctor right away.
Keep track of your progress when and where you are able, and don't be afraid to bring up any concerns you may have with your professionals or trans friends, or any other trans resource. Your transition is in your hands and you're allowed to modify it as you see fit. If you do not see the effects you want from traditional HRT, you may be able to seek the Gn-RH route, and if you aren't seeing the results you want from just estrogen, progesterone might be of use to you.
You will need to keep an eye on your bone health as high levels of estrogens can increase your chance to develop osteoporosis, and potential new cancers like breast cancer may arise, as well as heart problems. Getting checkups as frequently as possible and communicating with your doctor/s will be of great use when and where possible
Either way, we hope this helps in some way! We will add to it as we find/think of more information. Good luck to everyone seeking feminizing HRT, you deserve to look and feel like yourselves!
#transfem#transfeminine#transgender#trans#lgbt#lgbtq#queer#transfemme#trans girl#trans woman#trans women#trans lady#trans girls#trans gal#nonbinary#enby#genderqueer#genderfluid#drag queen#estrogen#progesterone#spironolactone#feminizing hrt#hrt#hormone replacement therapy#estrogen hrt#e hrt#e#our writing#resources
1K notes
·
View notes
Text


Woman + Man =

(Please read pinned post before interacting! <3)
Woman - Anyone who is a woman in some way.
Man - Anyone who is a man in some way.
#woman pride flag#man pride flag#trans woman#trans man#trans girl#trans boy#trans gal#trans guy#transfem#transmasc#bigender#genderfluid#multigender#lesboy#turigirl#nonbinary#enby#NB#polygender#omnigender#trigender#pangender#agender#flag combo#flag mashup
48 notes
·
View notes
Text

🥥🌊🌺🌴Tropical🌸🐬🌼🧜🏾♀️
Day 2 of Cute girltober done! I love how cute this piece is!!!
#kiggu mew#digital art#art#illistration#artists on tumblr#digital artist#digital drawing#cute#doodle#digital atist#artist of tumblr#enby artist#gal#gyaru fashion#gyaru#gyaru gal#gyaru makeup#inktober#art challenge
12 notes
·
View notes
Text

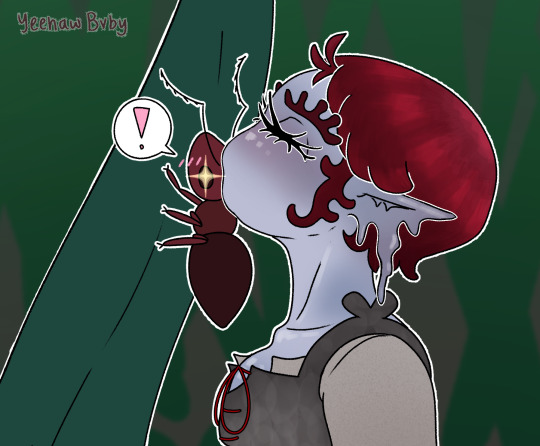

Funguary week 3 (pt 2) | Ophiocordyceps
What kinda fungus will the little ant become? 👀 Find out here, in part 3/Week 4!!
Part 1
#yes the ant is trans#yes they will fall in love and live happily ever after#devils fingers is a she/they gal and the ant is becoming a they/them enbie uwu#princess and the frog#????#funguary#crisart#fungus#mushroom#character concept art#character design#original character#oc#art challenge#february art challenge#concept art#devils fingers#clathrus archeri#ophiocordyceps#comic#feefal funguary#funguary 2023
22 notes
·
View notes
Text
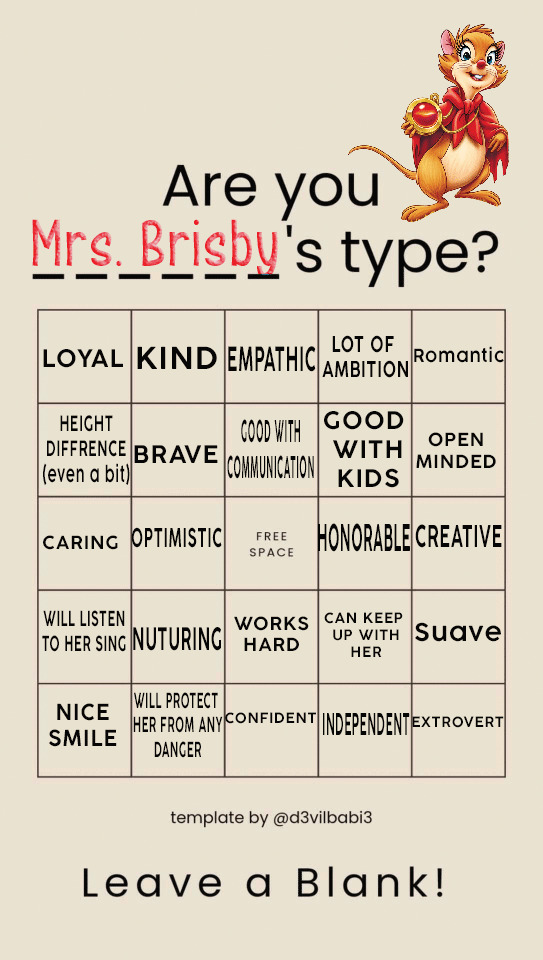

"What's this? Who put this here? Not me! Never!"

"Listen this momma needs to get back into the dating scene."
#(m; nimh mother)#meme#memes#dash games#dash game#(Again I haven't used her alot and I love her pls feel free to throw anyone at her guys gals enbys lets go!)#(last for tonight I swear)#(bingo cards)
4 notes
·
View notes
Last Seen Blogs

foxlecter
Foxlecter

spw-art
Also Bugs

ultimate-world-war-ii
World War II

heeheetag
gughg

mariyav
it's britney, bitch